

ABSTRACT
Background:
Immediate loading of dental implants is an obvious advantage. A long treatment period that involves the wearing of a temporary prosthesis may be of great inconvenience, and is sometimes the reason for not choosing implant-supported restorations at all.
Aim:
In our study, an attempt was made to immediately load single tooth implants in the aesthetic zone of the dentition.
Materials and Methods:
Patients were selected from Government Dental College, Patna. Twenty-four single tooth implants were placed in 24 patients; 12 male and 12 female patients desiring replacement of one or more missing teeth in anterior region were selected. Surgery for the placement of the implant was carried out, and implants of the Uniti Implant System were placed. The abutment was then attached and the flap was sutured. A temporary acrylic resin crown was fabricated and cemented on the same day. Permanent prosthesis was inserted on sixth month after implant placement.
Results:
A clinical study was performed to evaluate the treatment outcomes of dental implants installed according to a one-stage surgical procedure followed by immediate loading with prosthesis. Of the 24 implants, 23 showed signs of successful osseointegration over a 1-year follow-up.
Conclusion:
Within limits of the evaluated data, it was observed that immediately loaded implants osseointegrate, so this alternative was used over conventional procedures that take 6 months for osseointegration. This has advantages, both for patient and practitioner.
KEYWORDS: Dental implant, immediate loading, osseointegration
INTRODUCTION
Missing teeth in aesthetic region has affected psychology of mankind. Contemporary dentistry today offers two distinct solutions to address the problem of partial edentulous state in the form of removable and fixed partial dentures. A removable prosthesis is one that can be removed and inserted by the user at his will and discretion. Though it is flexible, it has its own inherent drawbacks, such as difficulty in speech, altered taste perception, and irritation to denture supporting tissues.[1]
Fixed prosthesis overcomes several problems posed by removable prosthesis, but they too are accompanied by several drawbacks, the principal drawbacks being, for replacement of particular tooth/teeth, the crowns of adjacent teeth have to be cut and prepared to serve as abutments. In this way, healthy tooth structure is sacrificed for the sake of replacing a missing tooth.
In view of all these problems, a third modality of tooth replacement called the dental implant was brought into existence, after the serendipitous discovery of the phenomenon of osseointegration by Professor Branemark in 1952. With the better understanding of biocompatibility of titanium and effective osseointegration achieved by hydroxyapatite plasma coated surface, implant therapy has reached new frontiers. The science of dental implantology today has become highly evolved, and today it is regarded as a highly effective and predictable modality of tooth replacement.[2]
By traditional protocols, the dental implant, once placed in bone, was submerged under the mucosa and left for 3–6 months to allow the implant to osseointegrate into the surrounding bone. During this phase, the patient was advised to wear an interim partial denture in the existing space. Later in the second stage of surgery, the abutment was attached to the implant, and only after adequate healing of soft tissues, the final prosthesis was placed. For many individuals, this way of working may be a psychologically traumatic experience.
A need has been felt to develop the routine “implant protocols,” decreasing or even eliminating the healing periods before loading inserted implants.Consequently, creation of fixed implant supported prostheses via protocols for either immediate (within 72 hrs) and early implant loading (within one to a few weeks of healing) have gradually become available during later years as additional concepts, aiming at reducing the treatment time and treatment costs. This is a totally new way of working in comparison to routine “protocols.” The new technique offers several advantages, including increased masticatory function, minimized uncontrolled transmucosal loading through cross-arch stabilization, improvement of psychological well-being, and reduction in treatment time. The new immediate loading approach, therefore, seems to be a good alternative for treatment of the aforementioned group of patients.[3]
Therefore, this study was conducted to evaluate the performance of implants subjected to load immediately after placement. This is accomplished under the following headings:
To assess osseointegration at regular interval to assess implant stability
To assess soft tissue changes surrounding implant after immediate loading
To assess marginal bone level changes in the follow-up examinations
MATERIALS AND METHODS
A total of 24 partially edentulous patients reporting to Government Dental College, Patna, Bihar, India, desiring replacement of missing teeth were selected for the study, if they satisfied the sampling criteria. In this study, 24 single tooth implants were placed in 24 partially edentulous patients. For the study, the edentulous spaces in the aesthetic zone (i.e., the anterior maxilla, consisting of the maxillary incisors, canines, and premolars) are considered.
Patient selection is carried out based on age and sex.
Inclusion criteria consisted of the following:
One or more missing teeth in the aesthetic zone (upper and lower incisors, canines and premolars) were included
After extraction, adequately healed and remodeled ridge included
Patients with absence of any periodontal problems in adjacent teeth
Patients with supra-eruption of opposite tooth
Exclusion criteria included the following:
Patients with a habit of smoking
Patients with a medically compromising conditions, which prohibit implant surgery, such as stroke, recent infarction, severe bleeding disorders, diabetes, osteoporosis, and cancer
Patients with a history of bruxism
Patients with implant with a torque of more than 35 Nm was not attained; that implant was not selected for immediate loading, and they were excluded from the study
Pre- and postoperative were assessed by clinical and radiographic means. It included clinical photographs, study models, orthopantomograph (OPG), and intraoral periapical (IOPA) radiographs. A 1-year follow-up was carried out for 1 year for all subjects.
Titanium plasma coated root form dental implant
Implants belonging to the Uniti, manufactured by Equinox Medical Technologies B.V., Zeist, Holland, were used in the study. Corticocancellous design implants were used. The shape of the implants was based on the biologic root form concept. Available in various size configurations of diameters 3.3, 3.7, 4.3, 5.3, and 6.0 mm and lengths 10, 13, and 15 mm, the size selection was done according to the manufacturer’s recommendations.
The design of the threads of the implant provided the property of self tapping to the implant. These threads have two different shapes (cortical, with a depth of 0.1 mm, and cancellous, with a depth of 0.35 mm), to one continuous pitch of 0.9 mm. The surface of the implant was produced using a water-soluble blast medium that is completely dissolved and removed. This surface has been described by the manufacturer as an osteoconductive, high porosity surface with micropores of 1–5 microns.
The transition from the roughened surface to the prosthetic table is a 1-mm highly polished collar. This is said to allow for predictable soft tissue integration by means of a hemidesmosomal attachment, and facilitates oral hygiene. The implant is secured to the abutment by means of a screw, locking the abutment to the implant with a twin hexagon internal connection.
The surgical tray is laid out in an autoclavable container, and sequenced with all color-coded drills and stoppers. The standard diameters of the system are D.3.3, D3.7, and D4.3 mm.
The manufacturer claims this implant system as suitable for use in delayed loading, immediate placement, and immediate loading situations.[4]
A complete case history was taken making use of a standard case history form, and subjects were selected who meet inclusion criteria.
Local examination was done to rule out healing status of extraction socket, presence of periodontal problems, jaw opening, and presence of any pathology at the proposed implant site.
Preoperative and postoperative photographic records of the edentulous space were maintained [Figure 1].
Figure 1.

Preoperative photograph and radiograph
Radiological investigations such as OPG and IOPA
The preoperative OPG was used for evaluation of surgical site, and to decide the length of the implant to be used, based on regional anatomy. IOPA radiographs were taken preoperatively and immediately postoperatively, and subsequently at every follow-up appointment, to assess response to immediate loading. Besides, routine blood investigations and urine examination were done, as in all cases in which any surgical procedure is to be performed.
Oral prophylaxis was performed before surgery. Any restorative work was addressed to next. An irreversible hydrocolloid impression was made, and a diagnostic cast was poured in dental stone. Using caliper/dividers, the available mesiodistal width available for the implant was measured. The diameter of the implant was decided based on Misch’s recommendation[5] that an implant placed adjacent to a natural tooth should remain 1.5–2 mm away from the crown in the aesthetic regions. Guidance was also taken from the manufacturer’s recommendations. The length of the implant to be used was decided based on regional anatomical considerations as evident in the OPG.
The approximate location of the implant pilot osteotomy was marked on the cast. A hole was drilled at that spot, analogous to the pilot drill, in an angulation, which would facilitate the abutment to take the crown in the most favorable position. A paralleling pin was used to check and correct the angulation.
Once the correct angulation was attained, the pin was sealed in the hole with wax. Separating media was applied to the cast. Self curing acrylic was molded over the coronal portion of the pin and labial surfaces of adjacent teeth (as they would provide a stable landmark) and allowed to cure. It was made sure that diameter of the pin was equivalent to the diameter of the pilot drill of the implant surgical kit.
The stent was removed from the cast and the pin was removed. It was trimmed of all excesses and smoothened. A preoperative trial was carried out for easy insertion and removal, and pilot drill was passed smoothly, yet snugly through its path. After all necessary adjustments, the stent was sterilized using 2% glutaraldehyde (Cidex) solution.
All implant surgeries were performed under local anesthesia. All patients were instructed to a chlorhexidine 2% mouth rinse immediately before surgery. The patient’s face was disinfected with 7.5% povidone–iodine. The oral cavity was prepared with 5% povidone–iodine. Local anesthesia was administered to block regional nerve supply and aid hemostasis.
A crestal incision was then placed with two releasing incisions, and a flap was elevated with a No. 9 Molts periosteal elevator, taking care to prevent flap tearing. After adequate exposure of crestal bone, the surgical stent was placed [Figure 2].
Figure 2.

Incision and flap elevation
The process of implant osteotomy is begun with the punch cut of the pilot drill being made through the hole in the stent, to accurately reproduce the angulation. The stent is removed and the osteotomy is carried to the desired depth. The angulation is checked once again with the paralleling pin, both clinically and radiographically, and any discrepancy found can be corrected subsequently. The osteotomy is then diametrically enlarged to desired width. Continuous internal and external irrigation was done.
After osteotomy, the implant was screwed in and tightened using the hardware provided in the surgical kit. It is made sure that a minimum torque of 35 Nm is obtained while screwing in the implant (which is ascertained by the slip of the Ratchet), as this is a prerequisite for immediate loading [Figure 3]. The abutment was attached to the implant with screw provided. The flap was reapproximated and sutured [Figure 4]. The screw hole in the abutment was then blocked with wax. Meanwhile, an irreversible hydrocolloid impression was made and cast poured in die stone. The cast was sent to the prosthodontist who fabricated an immediate acrylic temporary crown, which was cemented onto the abutment on the next day of implant placement. It was made sure that the crown was relieved of occlusal contacts. All patients were prescribed medication and were instructed not to bite hard on the prosthesis. Suture was removed on the seventh postoperative day. The procedures for fabricating the permanent prosthesis were performed in the sixth month following placement [Figure 5]. The patients were given a choice of a full ceramic or metal fused to ceramic crown.
Figure 3.
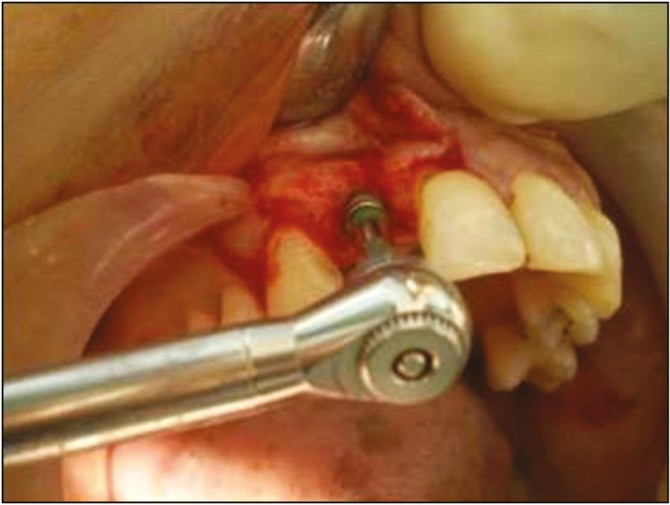
Implant placement
Figure 4.

Wound closure
Figure 5.

6th month—permanent crown placement
The response of the patient to the implant and its loading, before osseointegration, was then monitored over a follow-up period of 12 months. The parameters included in the study were recorded four times, that is, in 1st, 3rd, 6th, and 12th month.
Our postoperative evaluation of the immediately loaded implants included three parameters to assess the objectives of the study.
Implant mobility
-
Soft tissue changes:
-
a.
Peri-implant probing depth
-
b.
Bleeding index
-
a.
Height of marginal bone loss
Implant mobility was assessed in similar way as tooth mobility. With two rigid instruments, a force of approx 500g was applied in the labiolingual direction. The amplitude of implant mobility was scored 0–4, according to as given in Table 1.
Table 1.
Clinical implant mobility scale[6]
| Score | Inference |
|---|---|
| 0 | Absence of any clinical mobility with 500g in any direction |
| 1 | Slight detectable horizontal movement |
| 2 | Moderate visible horizontal mobility |
| 3 | Severe horizontal mobility >0.5 mm |
| 4 | Visible moderate to severe horizontal movement |
Peri-implant probing depths
It was measured in the same way as for a natural tooth, using a William’s periodontal probe. Probing depths are recorded for each of the four surfaces, and averaged to yield a mean peri-implant probing depth for each implant.
Bleeding index
The bleeding index used for evaluating our implants was the Silness and Loe Gingival index.[6] This index scores gingival inflammation from 0 to 3 on the facial, palatal, mesial, and distal surfaces of the implant. The scores are based on the presence or absence of bleeding on probing and are scored as follow:
Score 0 – normal gingiva;
Score 1 – mild inflammation, slight change in colour, slight oedema, no bleeding on probing;
Score 2 – moderate inflammation, redness, oedema, and glazing, bleeding on probing;
Score 3 – severe inflammation, marked redness and oedema, ulceration tendency to spontaneous bleeding
Mean marginal bone levels
Mean marginal bone levels were assessed radiographically using the standard IOPA radiographs. The distance between the observed crestal bone level and implant–abutment interface was measured at the mesial and distal implant surfaces and averaged to yield the mean marginal bone loss level for that implant.
The actual implant length is known based on manufacturing standards. To adjust the measurements for magnification error, the following equation was used to determine the corrected crestal bone levels:[7]
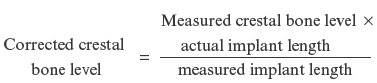
The measurements were classified into groups of 0.5 mm.
RESULTS
A total of 24 patients, reporting to Government Dental College, desiring replacement of missing teeth in the aesthetic zone of the anterior maxilla were selected, if they satisfied the specified inclusion and exclusion criteria. Also, 24 single tooth implants were placed totally in 24 patients. In all the patients, the implants were loaded with the prosthesis on the same day of placement.
Among the 24 patients, 50% (n = 12) were male and 50% (n = 12) were female. The mean age of the patients was 29.91 years (range, 19–42 years). The period of edentulousness ranged from 2 to 24 months, the mean duration being 11.4 months.
In all the cases, implants of dimensions 3.7 × 13 mm were used, except in two cases, where the central incisor had to be replaced, wherein we have used implants of dimensions 4.3 × 13 mm. As aforementioned, the prosthesis was fabricated immediately and placed on the first postoperative day, that is, within 24h of implant placement.
To assess the outcomes of the immediately loaded implant, we have focused our follow-up on three clinical and one radiographic parameters, namely implant mobility, peri-implant probing depths, bleeding index, and mean marginal bone levels, respectively. The values were recorded over follow-up appointments scheduled at 1st, 3rd, 6th, and 12th month of implant placement surgery.
Implant mobility was represented according to the implant mobility scale as described in “Materials and Methods.” In the first month, 95.8% (n = 23) of the implants showed absence of any clinical mobility with 500g force in any direction. One implant showed the presence of a slight detectable horizontal movement, 4.16 (n = 1). In the third and sixth month, the implant mobility scores remained rather alike, with 79.16 (n = 19) of implants showing no clinical mobility, 16.66% (n = 4) implants showing the presence of a slight detectable horizontal movement, and one implant (4.16%, n = 1) showed a moderately visible horizontal mobility. In the 12th month also, the scores were quite similar, the only difference being that the condition of the implant (n = 1, i.e. 6.67%) showing moderate horizontal mobility in the third and sixth month, deteriorated to show severe horizontal mobility, more than 0.5 mm depicted in Table 2.
Table 2.
Implant mobility scores
| Score | 1st month | 3rd month | 6th month | 12th month | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| 0 | 23 | 95.84 | 19 | 79.16 | 19 | 79.16 | 19 | 79.16 |
| 1 | 1 | 4.16 | 4 | 16.16 | 4 | 16.16 | 5 | 16.6 |
| 2 | 0 | 0% | 1 | 4.16% | 1 | 4.16% | 0 | 0% |
| 3 | 0 | 0% | 0 | 0% | 0 | 0% | 1 | 4.16% |
William’s periodontal probe was used to check peri-implant probing depth. Four values were recorded for each implant, each value corresponding to a surface, and then averaged, to yield a mean probing depth for each implant. In the first month, 29.16% (n = 7) implants showed a probing depth in the range of 1–1.5 mm, 37.5% (n = 9) showed a probing depth in the range of 1.5–2 mm, and 53.3% (n = 8) had a probing depth in the range of 2–2.5 mm. Meanwhile at every interval of 3 and 6 months, probing depth was measured. And at 12th month, only one implant (4.16%) showed a probing depth beyond 3 mm as depicted in Table 3. The median probing depth recorded for these 24 implants was calculated. The values were found to be 1.88, 1.69, 1.88, and 1.85 mm in the 1st, 3rd, 6th, and 12th month, respectively.
Table 3.
Peri-implant probing depth
| Score | 1st month | 3rd month | 6th month | 12th month | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| <0.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 0.5–1.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 1.0–1.5 | 7 | 29.6 | 11 | 45.8 | 7 | 29.6 | 7 | 29.6 |
| 1.5–2.0 | 9 | 37.5 | 9 | 37.5 | 11 | 45.8 | 12 | 50 |
| 2.0–2.5 | 8 | 33.3 | 4 | 16.6 | 5 | 20.8 | 4 | 16.6 |
| 2.5–3.0 | 0 | 0 | 0 | 0 | 1 | 4.16 | 0 | 0 |
| >3.0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 4.16 |
The bleeding index was evaluated by Silness and Loe method. On the basis of clinical findings obtained, scores of 0, 1, 2, and 3 were awarded to each of the four surfaces, and the mean value was calculated. The interpretation of the values obtained is given in Table 4. In the first month, 20% of the implants yielded a bleeding index of 0.1–1.0, which indicated the presence of a mild inflammation surrounding the implant. In 67% of the cases, a score of 1.0–2.0 was obtained, correlating to a moderate inflammation surrounding the implant. In the third and sixth month, the bleeding index scores were similar. The mean of the bleeding scores of all the implants, recorded at each follow-up visit, was calculated, the values of which were 1.31, 1.24, 1.13, and 0.93 in the 1st, 3rd, 6th, and 12th month, respectively.
Table 4.
Bleeding index score
| Score | 1st month | 3rd month | 6th month | 12th month | ||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | n | % | |
| 0.1–1.0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2.0–3.0 | 3 | 12.50 | 4 | 16.67 | 3 | 12.50 | 19 | 79.17 |
| 1.0 | 21 | 87.50 | 20 | 83.34 | 20 | 83.34 | 4 | 16.16 |
| 2.0 | 0 | 0 | 0 | 0 | 1 | 4.16 | 1 | 4.16 |
The marginal bone levels were assessed radiographically, using the IOPA radiograph. The height was measured on the radiograph. After eliminating the elongation caused by angulation errors, the level of bone loss was classified into groups of 0.5 mm. The resultant data were classified and depicted in Table 5. It was found that in the first month, all the implants (100%, n = 24) showed a negligible bone loss, that is, within 0.5 mm. In the third month, 20% of the implants showed bone loss below 0.5 mm, and 73% showed bone loss of 0.5–1 mm. In the sixth month, 93.34% of implants showed a mild loss of bone height of 0.5–1 mm. By the 12th month, 26.67% had bone loss levels below 1 mm, and 66.67% implants had bone loss levels between 1 and 1.5 mm.
Table 5.
Marginal bone loss level
| Score | Follow up (month) | |||||||
|---|---|---|---|---|---|---|---|---|
| 1st | 3rd | 6th | 12th | |||||
| n | % | n | % | n | % | n | % | |
| <0.5 | 24 | 100 | 3 | 12.5 | 0 | 0 | 0 | 0 |
| 0.5–1.0 | 0 | 0 | 20 | 83.3 | 23 | 95.83 | 4 | 16.6 |
| 1.0–1.5 | 0 | 0 | 0 | 0 | 0 | 0 | 19 | 79.6 |
| 1.5–2.0 | 0 | 0 | 1 | 4.16 | 0 | 0 | 0 | 0 |
| 2.0–2.5 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 2.5–3.0 | 0 | 0 | 0 | 0 | 1 | 4.16 | 0 | 0 |
| >3.0 | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 4.16 |
The overall results of our study show a success rate of 93.34%, with 23 of the 24 immediately loaded implants successfully osseointegrating. On the basis of these data, the inferences and conclusions have been derived.
DISCUSSION
Dental implants today have become a highly predictable mode of replacement of missing teeth. The ultimate goal is to achieve comfort, function, and aesthetics, and a last parameter, being reduction of treatment time.[3]
Initially a 3–6 month stress-free healing period was recommended by Mortonet al.[8] to achieve optimum bone healing and osseointegration before loading. This undue waiting period was always a source of inconvenience, both to the patient and clinician, and many a time, the reason for opting against implant therapy.[2]
The previously stipulated healing time that is necessary before the implants can be loaded has been proposed as a result of clinical observations rather than biological documentation.[2] Moreover, early trials faced demanding conditions, such as non-optimized patient selection with poor bone quantity and quality, non-optimized implant design, short implants, non-optimized surgical protocols, and biomechanically non-optimized prosthesis.[9]
Immediate loading of endosseous root form implants has been described in the literature for eliminating the 3- to 6-month healing period. Earlier, it was thought that micromotion resulting from early implant loading can result in fibrous encapsulation of the implant. In fact, Barone et al.[10] have found that the density of bone around immediately loaded implants to be higher than around those loaded after a delay. Histological evaluation in animals has shown osseointegration when implants were immediately loaded.[11,12] Histological evaluation from human beings regarding implants that received immediate loading has shown evidence of osseointegration.[13,14,15]
The need to develop routine implant protocols has been felt, particularly for decreasing or even eliminating the healing periods before loading inserted implants.[16] With better understanding of biomaterials, improvements in implant design, and surgical protocols, creation of fixed implant supported prostheses via protocols for either immediate (same day) and early implant loading (within one to a few weeks of healing) has gradually become available during later years as additional concepts, aiming at reducing the treatment time and treatment costs. This is totally a new way of working—a new paradigm—as compared to routine “protocols.” In the words of Ganeles et al.,[17] once immediately loaded implants have clinically osseointegrated, they appear to take on the long-term predictability characteristics of conventionally healed and loaded implants. Furthermore, as stated by Kinsel et al.,[18] the new techniques may even offer several advantages, including increased masticatory function, minimized uncontrolled transmucosal loading through cross-arch stabilization, improvement of psychological well-being, and reduction in treatment time.
We have conducted a prospective clinical study with the purpose of evaluating the treatment outcomes of 24 immediately loaded implants in the anterior maxilla, that is, the aesthetic zone.
For this study 24 patients were selected, based on their inclusion and exclusion criteria. Molars were not included in the study, as implants in the posterior region must withstand relatively high forces and loading moments in function.[19] The difference in stress patterns for anterior and posterior teeth would naturally alter the results, and hence to maintain standardization of the results, we have excluded molars. Patients were excluded if they provided a positive history of smoking, bruxism, or the presence of any medically compromising conditions, which prohibit implant surgery, such as stroke, recent infarction, severe bleeding disorders, diabetes, osteoporosis, and cancer. Intraoperatively, those patients in whom a minimum torque of 35–40 Nm was not achieved were also excluded from the study, as that amount is a prerequisite for immediate loading.[20,21,22] These criteria of patient selection were in accordance to those given by Nkenke and Fenner[1] and Lekholm.[16]
Several implant manufacturers have come forth claiming that their implant system can be effectively used in immediately loading systems. However, we have selected the Uniti System, from Equinox Medical Technologies B.V., considering its simplicity of surgical technique.[4] The cost factor also played an important role in the selection of the implant system. However, due attention was paid to avoid any compromise on quality.
After being loaded immediately with the temporary prosthesis, the implant was closely followed up for six months, after which it was replaced with a permanent porcelain fused to metal restoration, which would be in physiologic/functional occlusion with its opposite tooth. The 6-month gap between the temporary and permanent prosthesis carried significance as:
It played vital role in the reduction of micromotion over the freshly placed and loaded implant during its osseointegration period, as it was made sure that the provisional restoration would be out of occlusal contact.
The temporary prosthesis would also allow any minor adjustments to be made post-insertion, which would be unbecoming of a permanent ceramic prosthesis.
It would allow sufficient remodeling of the peri-implant soft tissue architecture.
A temporary restoration would allow easy removal for any clinical examination, if the need arises.
The radiolucency of the material (acrylic) would facilitate convenience and clarity in radiological assessments.
This protocol followed in the study is in strict accordance with the protocols followed by Andersen et al.,[2] Lorenzoni et al.,[23] Proussaefs and Lozada,[24] Ericsson et al.,[25] Lorenzoni et al.,[26] and Morton et al.[8]
The results of our short-term clinical study have shown that implants in the anterior maxilla may be immediately loaded following their insertion. The success rate achieved was 92% after 12 months post-loading. The clinical and radiologic parameters of evaluation of implant success included in our study were implant mobility, peri-implant probing depths, bleeding index, and mean marginal bone levels. All the four parameters appeared to be in healthy limits in 23 of 24 implants placed, which is in agreement with the findings of other studies, which have prospectively evaluated immediately loaded implants.
Of special interest are the findings pertaining to the bleeding index, which decreases significantly after the sixth month, or in other words, after delivery of the permanent crown. We attribute this to the favorable anatomy of the permanent prosthesis, when compared to the temporary prosthesis.
CONCLUSION
An analysis of the data obtained in the course of this study, coupled and compared with data obtained while reviewing literature, directs us to the conclusion that immediate loading of dental implants in the aesthetic zone of the maxilla is a highly predictable modality for replacing single missing teeth. It must however be noted that patient selection plays a pivotal role in the success of immediately loaded dental implants. However, further trials involving a larger sample size and longer follow-up period are necessary before this implant placement protocol can be decisively declared superior to the conventional loading protocols.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Nkenke E, Fenner M. Indications for immediate loading of implants and implant success. Clin Oral Implants Res. 2006;17:19–34. doi: 10.1111/j.1600-0501.2006.01348.x. [DOI] [PubMed] [Google Scholar]
- 2.Andersen E, Haanaes HR, Knutsen BM. Immediate loading of single-tooth ITI implants in the anterior maxilla: a prospective 5-year pilot study. Clin Oral Implants Res. 2002;13:281–7. doi: 10.1034/j.1600-0501.2002.130307.x. [DOI] [PubMed] [Google Scholar]
- 3.Laney WR. Editorial: After 40 years: the mission is possible. Int J Oral Maxillofac Implants. 2005;20:505. [PubMed] [Google Scholar]
- 4.Uniti Implant System Surgical Kit and Implants. Information brochure. Zeist, Holland: Equinox Medical Technologies B.V.; 2005. [Google Scholar]
- 5.Misch CE. Contemporary implant dentistry. 2nd ed. Maryland Heights, MO: Mosby; 1999. p. 148. [Google Scholar]
- 6.Misch CE. Contemporary implant dentistry. 2nd ed. Maryland Heights, MO: Mosby; 1999. p. 23. [Google Scholar]
- 7.Yoo RH, Chuang SK, Erakat MS, Weed M, Dodson TB. Changes in crestal bone levels for immediately loaded implants. Int J Oral Maxillofac Implants. 2006;21:253–61. [PubMed] [Google Scholar]
- 8.Morton D, Jaffin R, Weber HP. Immediate restoration and loading of dental implants: clinical considerations and protocols. Int J Oral Maxillofac Implants. 2004;19:103–8. [PubMed] [Google Scholar]
- 9.Szmukler-Moncler S, Piattelli A, Favero GA, Dubruille JH. Considerations preliminary to the application of early and immediate loading protocols in dental implantology. Clin Oral Implants Res. 2000;11:12–25. doi: 10.1034/j.1600-0501.2000.011001012.x. [DOI] [PubMed] [Google Scholar]
- 10.Barone A, Covani U, Cornelini R, Gherlone E. Radiographic bone density around immediately loaded oral implants. Clin Oral Implants Res. 2003;14:610–5. doi: 10.1034/j.1600-0501.2003.00878.x. [DOI] [PubMed] [Google Scholar]
- 11.Chiapasco M, Gatti C, Gatti F. Immediate loading of dental implants placed in severely resorbed edentulous mandibles reconstructed with autogenous calvarial grafts. Clin Oral Impl Res. 2008;18:13–20. doi: 10.1111/j.1600-0501.2006.01293.x. [DOI] [PubMed] [Google Scholar]
- 12.Romanos GE, Toh CG, Siar CH, Swaminathan D. Histologic and histomorphometric evaluation of peri-implant bone subjected to immediate loading: an experimental study with Macaca fascicularis. Int J Oral Maxillofac Implants. 2002;17:44–51. [PubMed] [Google Scholar]
- 13.Meyer U, Joos U, Mythili J, Stamm T, Hohoff A, Fillies T, et al. Ultrastructural characterization of the implant/bone interface of immediately loaded dental implants. Biomaterials. 2004;25:1959–67. doi: 10.1016/j.biomaterials.2003.08.070. [DOI] [PubMed] [Google Scholar]
- 14.Duyck J, Vandamme K, Geris L, Van Oosterwyck H, De Cooman M, Vandersloten J, et al. The influence of micro-motion on the tissue differentiation around immediately loaded cylindrical turned titanium implants. Arch Oral Biol. 2006;51:1–9. doi: 10.1016/j.archoralbio.2005.04.003. [DOI] [PubMed] [Google Scholar]
- 15.Nkenke E, Fenner M, Vairaktaris EG, Neukam FW, Radespiel-Tröger M. Immediate versus delayed loading of dental implants in the maxillae of minipigs. Part II: histomorphometric analysis. Int J Oral Maxillofac Implants. 2005;20:540–6. [PubMed] [Google Scholar]
- 16.Lekholm U. Immediate/early loading of oral implants in compromised patients. Periodontol 2000. 2003;33:194–203. doi: 10.1046/j.0906-6713.2003.03316.x. [DOI] [PubMed] [Google Scholar]
- 17.Ganeles J, Rosenberg MM, Holt RL, Reichman LH. Immediate loading of implants with fixed restorations in the completely edentulous mandible: report of 27 patients from a private practice. Int J Oral Maxillofac Implants. 2001;16:418–26. [PubMed] [Google Scholar]
- 18.Kinsel RP, Lamb RE, Moneim A. Development of gingival esthetics in the edentulous patient with immediately loaded, single-stage, implant-supported fixed prostheses: a clinical report. Int J Oral Maxillofac Implants. 2000;15:711–21. [PubMed] [Google Scholar]
- 19.Abboud M, Koeck B, Stark H, Wahl G, Paillon R. Immediate loading of single-tooth implants in the posterior region. Int J Oral Maxillofac Implants. 2005;20:61–8. [PubMed] [Google Scholar]
- 20.Galli F, Capelli M, Zuffetti F, Testori T, Esposito M. Immediate non-occlusal vs. early loading of dental implants in partially edentulous patients: a multicentre randomized clinical trial. Peri-implant bone and soft-tissue levels. Clin Oral Implants Res. 2008;19:546–52. doi: 10.1111/j.1600-0501.2008.01530.x. [DOI] [PubMed] [Google Scholar]
- 21.Cornelini R, Cangini F, Covani U, Barone A, Buser D. Immediate restoration of single-tooth implants in mandibular molar sites: a 12-month preliminary report. Int J Oral Maxillofac Implants. 2004;19:855–60. [PubMed] [Google Scholar]
- 22.Neugebauer J, Traini T, Thams U, Piattelli A, Zöller JE. Peri-implant bone organization under immediate loading state. Circularly polarized light analyses: a minipig study. J Periodontol. 2006;77:152–60. doi: 10.1902/jop.2006.040360. [DOI] [PubMed] [Google Scholar]
- 23.Lorenzoni M, Pertl C, Zhang K, Wimmer G, Wegscheider WA. Immediate loading of single-tooth implants in the anterior maxilla. Preliminary results after one year. Clin Oral Impl Res. 2003;14:180–7. doi: 10.1034/j.1600-0501.2003.140207.x. [DOI] [PubMed] [Google Scholar]
- 24.Proussaefs P, Lozada J. Immediate loading of hydroxyapatite-coated implants in the maxillary premolar area: three-year results of a pilot study. J Prosthet Dent. 2004;91:228–33. doi: 10.1016/j.prosdent.2003.12.016. [DOI] [PubMed] [Google Scholar]
- 25.Ericsson I, Nilson H, Lindh T, Nilner K, Randow K. Immediate functional loading of Brånemark single tooth implants. An 18 months’ clinical pilot follow-up study. Clin Oral Implants Res. 2000;11:26–33. doi: 10.1034/j.1600-0501.2000.011001026.x. [DOI] [PubMed] [Google Scholar]
- 26.Lorenzoni M, Pertl C, Zhang K, Wegscheider WA. Inpatient comparison of immediately loaded and nonloaded implants within 6 months. Clin Oral Impl Res. 2003;14:273–9. doi: 10.1034/j.1600-0501.2003.140304.x. [DOI] [PubMed] [Google Scholar]