

Abstract
The use of laparoscopic surgery is widespread worldwide and is becoming the standard procedure. Postoperative adhesion, which is one of the typical postoperative complications, is considered to be less likely to occur compared with open surgery. However, once complications, such as small bowel obstruction or chronic abdominal pain, occur due to adhesion, the minimal invasiveness can be greatly impaired, and it can also become costly from a medical economics perspective. In the past, anti-adhesion absorption barrier films have been used to prevent adhesion, but there are many cases in which laparoscopic techniques are required, depending on the site of intraperitoneal attachment. Herein, we report a device that can easily attach an absorbent barrier preparation.
Keywords: Anti-adhesion–absorption barrier, attaching device, colorectal surgery, laparoscopic surgery
INTRODUCTION
It has been reported that adhesions occur in more than 90% of patients who have undergone abdominal surgery, and small bowel obstruction is one of the postoperative complications.[1] Postoperative small bowel obstruction may be impaired by laparoscopic surgery, and its prevention is important. Herein, we report a device that can easily be used to apply an anti-adhesion–absorbing barrier film, regardless of the site.
PROCEDURE
Endo Roll™ (Hope Denshi, Chiba, Japan) is a device for inserting Seprafilm™ (Kaken Pharmaceutical, Tokyo, Japan), an anti-adhesion–absorbing barrier film preparation, into the abdominal cavity and applying it to the appropriate site. A slit is inserted so that the film can be sandwiched between the long cylinder and the take-up rod, and a cap is attached to maintain the intraperitoneal pressure [Figure 1a]. The length of the inner cylinder is 320 mm while the outer cylinder is 200 mm long and can be inserted from a 5-mm port. The film is stored in the outer cylinder by pinching and rotating the take-up bar [Figure 1b]. The film is inserted from the port into the abdominal cavity in that state, and the inner cylinder is removed from the outer cylinder in the vicinity of the site of attachment. The spread film is held with forceps and attached to the intended site [Figure 2].
Figure 1.
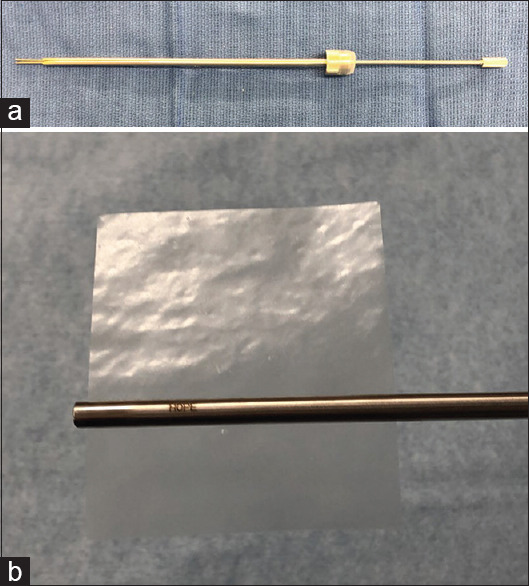
Endo Roll™. (a) The device consists of an outer cylinder and an inner cylinder for hoisting, and both cylinders have slits to allow the film to be sandwiched between them. (b) How to store, insert the film into the slits of the inner and outer cylinders, rotate the inner cylinder for winding and store it in the outer cylinder
Figure 2.
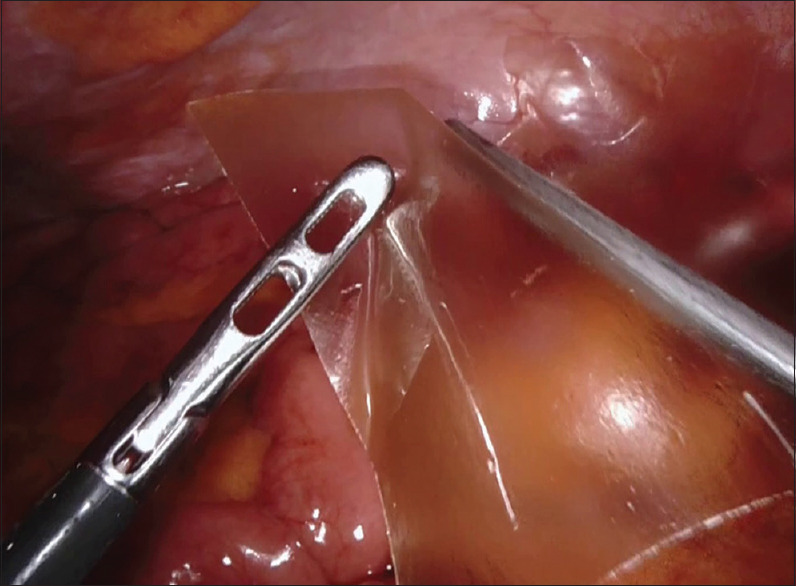
The film expands by removing the inner cylinder from the outer cylinder within the abdominal cavity. The spread film is gripped with forceps and attached to the intended site
DISCUSSION
There are film-, sheet- and spray-type anti-adhesion–absorbing barriers that can be used today. Film-type anti-adhesion–absorbing barriers have the longest history among the three types, and their usefulness has been reported in many papers.[2] However, as a disadvantage, in the case of using an anti-adhesion–absorbing barrier at the peritoneal injury site in the abdominal cavity, during laparoscopic surgery, in the case of a conventional anti-adhesion–absorbing barrier film, a specialised technique may be required for application. Various households have reported the methods/approaches for the insertion of fire-place inserts.[3] The Endo Roll™ used in this report is a device that can be used for easy insertion and affixation of a film-type anti-adhesion–absorbing barrier preparation into the abdominal cavity. Furthermore, its operation is easy and does not require skilled techniques. However, if there is excessive moisture on the Seprafilm™, the file will worsen and may become difficult to attach. Thus, it is better to operate the device and attach the film as soon as possible. In addition, if the film does not spread into the abdominal cavity, it can be widened by shifting the pinching position slightly, rather than in the middle. Similarly, there are products for attaching Seprafilm™ to the abdominal cavity, but there is a drawback, i.e., the cost is high for single use. The device used currently has a price cap of two dollars and seventy-eight cents for maintaining the pressure in the abdominal cavity, but the device for application to the main body is reusable; thus, it is considered to be beneficial from a medical economic point of view. We believe that a device that simply attaches the Seprafilm™ to the abdominal cavity during laparoscopic surgery is useful.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Becker JM, Dayton MT, Fazio VW, Beck DE, Stryker SJ, Wexner SD, et al. Prevention of postoperative abdominal adhesions by a sodium hyaluronate-based bioresorbable membrane: A prospective, randomized, double-blind multicenter study. J Am Coll Surg. 1996;183:297–306. [PubMed] [Google Scholar]
- 2.Hayashi S, Takayama T, Masuda H, Kochi M, Ishii Y, Matsuda M, et al. Bioresorbable membrane to reduce postoperative small bowel obstruction in patients with gastric cancer a randomized clinical trial. Surg Today. 2015;45:1352–9. doi: 10.1097/SLA.0b013e3181656d4e. [DOI] [PubMed] [Google Scholar]
- 3.Nakase Y, Nakamura K, Sougawa A, Nagata T, Mochizuki S, Kitai S, et al. Anovel procedure for introducing large sheet-type surgical material with a self-expanding origami structure using a slim trocar (chevron pleats procedure) Surg Endosc. 2017;31:3749–54. doi: 10.1007/s00464-016-5389-5. [DOI] [PubMed] [Google Scholar]