

Abstract
The emergence of COVID-19 across the globe prompted many countries to institute total lockdown or other models of mobility restrictions to mitigate the spread of the disease. On March 29th, Nigeria instituted a nationwide lockdown. It is pertinent to understand the pattern created by this lockdown. This could offer insights into how people perceive the hazard and the level of compliance across the States in Nigeria. Mobile phone-based mobility data and the number of new cases from the beginning to the end of the lockdown were utilised. The study examines space-time trends across different place categories at the state level. Place categories witnessed mobility reduction as high as 56%, 57%, 65%, 75%, 38% for retail and recreation (RtRc), Grocery and Pharmacy (GrPh), Park, and Transport Hubs (Trst) respectively. Most States recorded mobility uptrend towards workplace, retail and recreational areas. Multiple correspondence analysis (MCA) identified two dimensions from the Space-time trends. The first dimension (D1) accounted for 66% of the variance. Examination of the Object Scores from the MCA showed that there are two classes–two risk perception groups. The pattern of mobility recorded shows that there is a variation in mobility restriction compliance across the States. The trend groupings identified captured an aspect of risk perception within each State. Thus, pointing to difference in levels of risk acceptance. With the level of misinformation currently being experienced worldwide, concerted efforts should be made on improving risk perception to prevent the re-emergence of the disease.
Keywords: Community mobility, Risk acceptance, Space-time trend, Risk perception, Mitigation planning
Introduction
In December 2019, the news of the outbreak of an emerging viral infection broke in the city of Wuhan, China. The World Health Organisation (WHO) initially declared the outbreak a public health emergency of international concern and later upgraded it to a global pandemic, following its rapid diffusion to several countries. Currently, the number of global COVID-19 cases has surpassed the 9 million mark while deaths arising from these cases are over 800,000. This has never been seen in contemporary times. It is in fact unlike, the previous outbreak of Severe Acute Respiratory Syndrome (SARS) of 2003 and Ebola in West Africa of 2014. COVID-19, within a short period, grew from a local event to a pandemic affecting many people and places. This prompted many countries to institute total lockdown or other models of mobility restrictions to mitigate the spread of the disease. On March 29th the Federal Government of Nigeria instituted a nationwide lockdown to mitigate the spread of COVID-19. This lockdown offers one of the most potent tools at mitigating the spread, however, it also presents a serious problem. With the instituted restriction and the induced mobility reduction due to fear and apprehension, the effect on various aspects of the society is going to be disparate over space and across people. Thus, it is important to examine the pattern of this mobility restriction across the country, thereby offering insights into the potential impact across the country. In this context, the study examined variation in human mobility during the lockdown period across the country. Therefore, providing an understanding of the pattern of mobility restriction compliance and the indication this provides for risk perception during this period. This understanding can provide baseline information for the management of future infectious disease emergencies, response and recovery (social and economic) planning, and evidence to support post-pandemic social and economic development.
Devastating pandemics have existed since 541 A.D when the world experienced the bubonic plague that wiped out 25–50 million people in one year (Morony 2007). It was one of the worst outbreaks the world experienced, and it lasted for another 225 years, sweeping throughout the Mediterranean world until 750 CE. In the year of 1347–1351, the Black Plague killed more than 75 million people in the Middle Eastern lands of China, India, as well as Europe (Cohn 2002). The Spanish Flu pandemic, caused by an H1N1 virus with genes of avian origin, killed over 50 million people in one year in 1918 (Cohn 2002). In America, 675,000 deaths were recorded; 2,000,000 in Sub-Saharan Africa, and 500,000 in Nigeria, out of a population of 18 million in less than 6 months (Ohadike 1991).
Human mobility facilitates infectious disease transmission. For COVID-19, rapid diffusion has been attributed to domestic and international travel within China and other countries. For instance, domestic and international travelers from Wuhan, China facilitated the spread, particularly during the annual Lunar New Year celebrations. As travel restrictions were implemented, this effectively slowed down the spread in the early days of the outbreak (Chinazzi et al. 2020; Kraemer et al. 2020). The recent cases in New Zealand where 2 travelers from the UK were implicated in new cases recorded in New Zealand with no new cases for 24 days (Graham-McLay, 2020) highlight the importance of human mobility for infectious disease spread.
From the foregoing, the relevance of mobility in the spread of infectious diseases is apparent. There is a clear indication that there is going to be another EID in the future, therefore, there is a need to gather insights from the current pandemic on what worked, failed, or need to be improved upon in managing the pandemic. Most especially, the compliance of the mobility restriction and potentially the perception it can indicate needs to be thoroughly explored.
Analyses of spatial patterns and distribution of human activities and natural phenomena are often leveraged for understanding spatial interaction and consequently spread of ideas knowledge and in this context, disease. Identification of the pattern of human mobility and the number of new COVID-19 cases is important. This offers an opportunity to examine the effect of the mobility restrictions and thereby design ways to ensure the effectiveness of measures to curtail the spread of COVID-19. Human activities and habitation are directly impacted by location and the opportunity offered by transportation—human mobility. This interrelationship and dependencies often lead to the increasing agglomeration of businesses, industries, and infections/diseases at specific locations (e.g., established urban centres). Similarly, there is a tendency for the segregation of people with a similar culture, tradition, behavior, social class, etc. across different regions and locations.
Literature review
COVID-19 found its way into Nigeria through an infected Italian national who has work engagements in the country when he touched down in Lagos State on February 27, 2020 (NCDC 2020). Being the third zoonotic coronavirus outbreak of this century (Xie and Chen 2020) with infection and mortality rate seemingly higher than those of the other two–MERS and SARS, its perilous nature cannot be disregarded (Kang et al. 2020). This necessitated the nationwide lockdown that was declared by the Federal Government as a precautionary measure done by countries world over. Nigeria took cognizance of the lockdown's effectiveness when the third confirmed case, who was duly notified by the contact tracing team, self-quarantined and later became symptomatic, was cautiously isolated and successfully treated (Chia and Oyeniran 2020) thereby mitigating community transmission. By and large, the hardiness of public health systems of countries plagued by the virus can have a significant influence on the case and fatality figures (Paintsil 2020). Despite this, the restriction of movement remains imperative in curtailing the spread of the virus.
Human mobility has been known to be very important in spreading infectious diseases. Balcan et al. (2009) studied the interplay between short-scale commuting flows and long-range air traffic in shaping the spatiotemporal pattern of the global epidemic. Their model showed that despite commuting flow being one order of magnitude larger than long-range air traffic, the spatiotemporal pattern of infectious disease spread was mainly determined by airline network and traffic. Furthermore, short-range movements were found to be more important for synchronization of the spreading across subpopulations which are weakly connected by air transportation. They found that short-range mobility has an impact on the definition of the subpopulation infection hierarchy.
Riley (2007) reviewed studies on four different diseases (measles, foot and mouth disease, pandemic influenza, and smallpox). The work showed that the major determinant of the geographic spread and emergence of infectious diseases (and reoccurrence) are disease-relevant human interactions (contact with infected surfaces and person-to-person interaction) and mobility across multiple spatial scales. Thus, at the onset of the outbreak, or re-emergence of the pathogen, disease incidence will most likely occur in spatial clusters, as such if containment is activated, it is possible to predict the spread of disease.
Jones et al. (2008) showed that from 1940 to 2004, 335 Emerging infectious diseases, showed a non-random global pattern, most dominated by zoonoses (60% of the EID and notable increases between 1990 and 2000) while about 72% of these originates from wildlife. By controlling for spatial reporting bias within countries, the study found that human population density and wildlife host species richness are significant predictors of the emergence of zoonotic EIDs. In the case of Zoonotic EIDs from the non-wildlife hosts, human population density, growth rate, latitude, and rainfall were found to be significant predictors. EID emergence caused by drug resistance has population density and growth as well as latitude and rainfall as significant predictors. The population density was the only significant predictor of vector-borne EID emergence. The origins EID were found to be significantly correlated with socio-economic, environmental, and ecological factors. Contrary to previous analyses indicating pathogen species richness increase towards the equator, the study indicated that EID events are mostly concentrated around 30° and 60° north and 30–40° south.
Adepoju and Soladoye (2020) held the view that for a vivid comprehension of the epidemic's transmission patterns, geographical perspective must be considered. Moreover, being that social sciences provide comprehensive and robust insights when researching the effects of infectious disease outbreaks on communities and populations socially, contextually, and behaviorally (La et al. 2020), it is crucial to incorporate them in epidemiology. Based on this, the perception of the disease's threats and the compliance level by the populace can be scientifically deduced. For COVID-19 pandemic awareness measures, Olapegba et al. (2020) utilized descriptive statistics to depict the risk perception and precautionary health behaviors as observed by Nigerians. The results of their findings showed that out of 1357 respondents, 66.91% believed there is a high chance of them contracting the virus in Nigeria, 17.46% think they cannot get infected while 15.62% were undecided. On some of the precautionary health behaviors, up to 84.75% indicated their readiness to self-isolate when required to, 10.10% think otherwise while 5.16% were indifferent. Also, 79% abstained from going to public places, 12.16% opposed to it while 8.84% were on either side. However, on the use of face mask, 52.98% were willing to comply, 33.31% found it discomforting and 13.71% were undecided.
Anchored on perception and impact of the pandemic in Nigeria, Akintuyi et al. (2020) in their work revealed that of the 303 respondents, 87% acknowledged the presence of the COVID-19 virus in Nigeria while 13% thought it was a hoax. On the other hand, the movement restriction order hugely affected 80.5% of the respondents and their livelihood while 19.5% did not feel the effect. In their paper, Taiwo and Olumoyegun (2020) demonstrated how distance played a role in the transmission of the virus in Nigeria—from Lagos to other State Capitals. Categorizing the States with International airports, domestic airports, and no airports accordingly, the results showed high variations in the reported case figures for States with International airports as against those States with domestic or no airports. Also, they noted that there was a statistically significant difference between the three groups. Abdullahi and Abdulkadir (2020) analyzed the role of temperature in the dispersion of the COVID-19 virus across geopolitical regions and States in Nigeria with the aid of Linear Trend Surface analytical tools. Their research further established that no significant relationship exists between varying temperatures across States and COVID-19 spread.
In assessing compliance with the mandatory stay-home order and its attendant socio-economic effects on the populace, Olabamiji and Ajala (2020) employed online questionnaires in acquiring data. With 177 respondents, while 68.9% could neither go to work nor do anything productive from home, 13% were not fully engaged in their work and 18.1% did not disclose their work status during the lockdown. On the part of its effects, 68.9% lived on their savings, 13% borrowed funds, 7.3% on salary, 5.7% depended on farm produce, 2.3% each on gifts from relatives and palliatives respectively while 0.6% benefitted from their businesses. Addie et al. (2020) portrayed States ranked in order of their vulnerability to COVID-19 in Nigeria. With the aid of select population-based indicators, they performed a stepwise regression analysis on their data to point out different vulnerability levels. Results obtained showed Kebbi State was the most vulnerable with 39.82 points followed by Zamfara at 39.27 points and then Sokoto at 39.24 points. Based on Geopolitical Zones, North West ranked as the most vulnerable with North East in second place and North Central in third place. In a similar vein, Fasona (2020) utilized some core transmission drivers to analyze and create maps, at the State level, to show their respective vulnerability level to the virus. The results indicated that 7 States (Lagos, FCT, Kaduna, Katsina, Kano, Rivers, and Oyo) had very high vulnerability, 17 States had high vulnerability while that of 13 States stood at medium vulnerability.
In modeling COVID-19 transmission predictively in Nigeria as was influenced by traveling history and contacts, Ogundokun et al. (2020), using the number of cases data from the NCDC, applied the ordinary least squares estimator in generating a regression analysis model which showed both the daily effects in travel history and contact rates on confirmed cases. Between the months of March and May 2020, the results indicated a 4.8% reduction in COVID-19 cases in comparison to the expected figures as a result of the travel ban on both local and international flights. They also noted that the populace chances of contracting the virus due to their travel history and contacts they made increased by 85% and 88% respectively.
Data and methods
Study area
Nigeria as a federation has 36 states and Abuja as the Federal Capital Territory (FCT)—Fig. 1. The States are further divided into 774 LGA spread over an area of 923,768 square kilometres, including about 13,000 Km2 of water. The work of Lawal and Anyiam (2019) provides more details about the study area.
Fig. 1.

The Nigerian States and the neighbouring countries
Data sources
Mobility data were sourced from the Google COVID-19 mobility report (Google LLC 2020). The dataset represents the percentage change in mobility around six place categories from their baseline. The period under consideration for this study spans the lockdown period i.e. between March 29 and June 30, 2020. The places categories captured are:
-
I.
Grocery and pharmacy: grocery markets, food warehouses, farmers markets, specialty food shops, drug stores, and pharmacies. (GrPh)
-
II.
Parks: local parks, national parks, public beaches, marinas, dog parks, plazas, and public gardens. (Park)
-
III.
Transit stations: public transport hubs such as subway, bus, and train stations. (Trst)
-
IV.
Retail and recreation: restaurants, cafes, shopping centres, theme parks, museums, libraries, and movie theatres. (RtRc)
-
V.
Residential: places of residence. (Resd)
-
VI.
Workplaces: places of work. (Wkpl)
Furthermore, the sum of the place categories except the Residential were summed and explored.
Data for the new cases were collated from the Humanitarian Data Exchange website, under the COVID-19 Pandemic initiative (Backup Rural 2020).
Methods
To capture the distribution of mobility across the study area, choropleths of median mobility were produced. These were produced using SPSS (IBM 2015), for each of the place categories as well as the aggregate of all the place categories (except the residential categories).
Space-time analyses of aggregated mobility values were carried out within a Geographic Information System (GIS)—ArcGIS (ESRI 2019). This was done to identify the Spatio-temporal clusters of mobility across the lockdown period. Trends were discerned across the study area over time using the Mann-Kendal Test (Kendall and Gibbons 1990; Mann 1945). This approach is a rank correlation analysis for the bin count (sum of value) and their respective time sequence. Each period is compared to the one before it and an increase results in a value of + 1 (an increase over time) while a decrease results in 1 (a decrease over time) and a tie result in zero (no trend over time). This was computed for each time slice (day) and the sum of this was computed for each of the spatial units (States). These sums were compared to the expected sum of zero (no trend over time) and using the variance of the values, as well as number of ties and the number of time slices, as the observed is compared to the expected to deduce the z score and a p-value. The trends across each sector were examined at weekly (14) intervals for each State.
Trend categories identified from the Space-time analysis were subjected to Multiple Correspondence Analysis. This was carried out to group quantify the nominal categories by assigning numerical values to each State and grouping them. This analysis does maximise intergroup differences and minimise intragroup differences, thus creating homogenous groups based on the trend of mobility across each State. The trend of mobility for the six place categories was utilised for this analysis. The initial analysis assumed there are two dimensions. An equal weight of 1 was given to each of the variables as there was no scientific justification to assign unequal weight. For discretisation, the multiplication approach was adopted. This comprises of standardisation of values, multiplication by 10, rounding off, the addition of constant value (to ensure the lowest value is 1). Object principal normalisation method was applied as this optimises for the distance between objects thus, ensuring that within group similarity are minimise and between group are maximised. The results of this analysis would provide insight into the potential grouping of risk perception based on the mobility trend.
Results and discussion
Place category aggregated mobility trend
Retail and recreation
For the retail and recreation category (Fig. 2a), Sokoto showed median mobility of zero while some States experienced an increase (compared to baseline) mobility for this place category. Zamfara showed a very high increase in mobility (median 51%). Kebbi, Borno, Yobe, Gombe, and Ebonyi represents a group of State with relative median mobility decline of less than 10% (relative to baseline). The greatest decline (ranging between 45 and 56%) in mobility were recorded across various States (Ekiti, Kaduna, Lagos, FCT, and Edo) spanning various regions of the country. The largest decline was recorded for Edo State. Generally, most of the States recorded median mobility decline ranging between 44% and 10%.
Fig. 2.

Median of aggregated mobility across States for place categories a Retail and recreation; b Parks; c Grocery and pharmacy; d Transit stations; e Workplaces; and f Residential
Parks
In the Parks place category (Fig. 2b), Gombe State is the only State with the increased median mobility across the country during the period under investigation. Abia, Adamawa, Jigawa, Ebonyi, Bayelsa, and Bauchi State showed a slight decline in mobility (relative to baseline) ranging between 7% and 1%. FCT, Benue, Ekiti, and Lagos witnessed the highest decline ranging between 65% and 45%. While the remaining States recorded declines between 39% and 10%.
Grocery and pharmacy
For this place category, all the States witnessed a decline relative to their baselines for the period under consideration (Fig. 2c). The lowest decline was recorded for Yobe State (3%) and the greatest was recorded for Zamfara State (57%), this was followed by Ekiti (51%), and Kano (41%). Most of the States (67%) recorded a relative decline ranging between 39% and 10%.
Transport stations
This place category witnessed a relatively high mobility decline ranging between 75 and 3 (Fig. 2d). Three States namely Ebonyi, Nasarawa, and Niger recorded a median mobility value indicating a slight increase relative to their baseline values (3%–4%). Kebbi and Kogi showed a slight decline of 3% while 70% of the geographic units considered recorded decline ranging between 44% and 14%. Six States (including the FCT) showed a considerably high level of decrease in mobility with a median change from baseline ranging between 75% for the FCT and 44% for Rivers State.
Workplaces
Zamfara recorded a median increase of 5% relative to the baseline mobility for the Workplaces category (Fig. 2e). This is the only outlier State for this category (i.e. it bucks the trend of declining mobility for this category). States like Yobe, Bauchi, Katsina, Kogi, and Adamawa recorded a slight decline median values raging between 9% and 2%. Most of the States recorded a decline ≥ 10% while four geographic units—Kwara, FCT, Kano, and Lagos recorded a decline above 30%.
Residential
This place category witnessed a high mobility increase, with a relative percentage increase ranging between 0 and 28% (Fig. 2f). The largest increase is recorded for Lagos (the epicentre of the COVID-19 infection in Nigeria) while the lowest (no change in mobility) is recorded for Kogi (one of the last State to record a COVID-19 case). This is a wide variation in the increase across different States and regions, with about 65% of the State recording 10% or more median mobility increase for this place category.
Summed mobility across unsafe place categories
Mobility values for all the place categories except Residential were summed to indicate mobility across places where infection may be spreading (unsafe). This term unsafe is relative in this context since there is a possibility that mobility towards residential areas could also spread the disease (Community spread). The median mobility (Fig. 3) for these unsafe categories showed a general reduction in mobility with the lowest mobility decline recorded for Ebonyi State (34.5) while the greatest decline was recorded for FCT (237). This computation gave a cumulative overview of how mobility varied for these place categories across States. 21 out of the 37 States and FCT showed a cumulative decline above 100, while only three States (Ebonyi, Kebbi, and Zamfara) recorded a cumulative decline of less than 50. From the values, four major hotspots for the decline could be identified around Lagos, Ekiti, FCT (Kaduna, Kano) as well as Akwa-Ibom State.
Fig. 3.
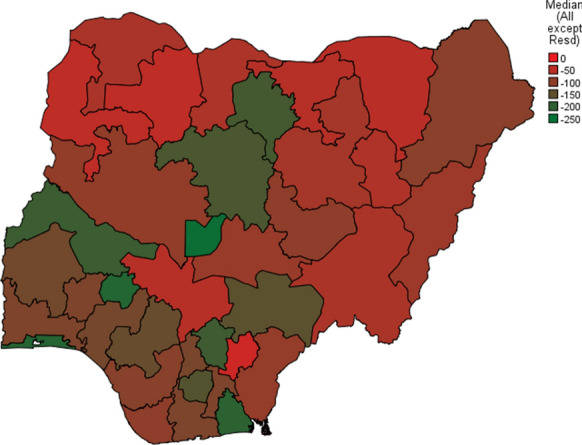
Cumulative mobility across unsafe place categories
Space-time trend of mobility
Mobility trend for retail and recreation
Examination of the weekly aggregated mobility for the retail and recreation category showed that 7 states exhibited no statistically significant trend (Fig. 4a). Five of these States spanned across the north–west and north-eastern part of the country while the other two can be found in the south (Bayelsa) and the middle belt (Taraba). Three States showed a statistically significant downtrend for mobility for this place category, with all of them in the northern part of the country. All other States displayed an uptrend in mobility for this place category.
Fig. 4.

Space-time trend (weekly) of State-level aggregated mobility for place categories a Retail and recreation; b Parks; c Grocery and pharmacy; d Transit stations; e Workplaces; and f Residential
Mobility trend for parks
For Parks, most of the States showed no statistically significant trend (Fig. 4b). However, Bayelsa and Abia States showed a downward trend in mobility for the category. All the other States (in the Southern part and the middle belt of the country) showed an upward trend in mobility.
Trend mobility for grocery and pharmacy
Yobe and Gombe States recorded a declining trend for mobility in the Grocery and Pharmacy place category (Fig. 4c). Twelve States across the north-western, north-eastern, middle belt, and southern (Bayelsa and Cross River) parts of the country displayed no statistically significant trend in mobility for this place category. The remaining States spread across different parts of the country—mostly in the southern part displayed a statistically significant upward trend of mobility for this place categories.
Trend mobility towards transportation hubs
For this place category, the trend of mobility revealed that there are three contiguous regions across the country (Fig. 4d). Kaduna, Plateau, and FCT formed a region of uptrend across the central part of the country, while the States from Kwara to Lagos down to Delta and Abia formed another contiguous region with a statistically significant uptrend in mobility. A contiguous region of no statistically significant trend surrounds Kaduna, FCT, and Plateau uptrend region. This region of no discernible trend extends down to Ebonyi, Cross River, Akwa-Ibom, Rivers, and Bayelsa State.
Trend mobility towards workplaces
Only a handful of States (Borno, Jigawa, Kano, Katsina, and Sokoto) showed no statistically significant trend in mobility for workplaces. Most States showed an upward trend in mobility during the period under consideration.
Trend mobility toward residential areass
For the residential place category, two States–(Benue and Kogi) showed an upward trend in mobility. This could be attributed to a late onset of infection recorded in these States. Most of the States across the north-eastern and north-western regions of the country showed no discernible trend of mobility. However, from Kano down to Abuja and Nasarawa, Niger to Lagos, Ondo through Imo to Cross River, there is an upward trend of mobility. Ebonyi, Rivers, and Bayelsa are outliers with no definite mobility trend while being surrounded by States with a clear trend.
Space-time trend of new cases
A look at the new cases of COVID-19 diagnosed during this same period (Fig. 5) revealed that there is a statistically significant uptrend across many States of the federation. Osun, Cross River, and Taraba States represent a group of outliers, as they have no statistically significant trend and are surrounded by other States with an upward trend in the number of (weekly) new cases. Sokoto, Zamfara, Kano, Jigawa, and Yobe State also have no discernible trend, however, they have neighbours with an upward trend in the number of new cases (Fig. 5).
Fig. 5.

Space-time trend of new cases (weekly) for the period under study across States
Grouping of mobility trend categories
The multiple correspondence analysis identified two dimensions within the mobility trend designation recorded for each State for the six place categories (Table 1). The first dimension (D1), showed as high internal consistency (Cronbach's Alpha = 0.898) with an explained variance of 66%. The second dimension (D2) has explained a lesser proportion of the variance across the variables and has a lower level of internal consistency.
Table 1.
Model summary of the multiple correspondence analysis
| Dimension | Cronbach's alpha | Variance accounted for | |
|---|---|---|---|
| Total (Eigenvalue) | % of Variance | ||
| 1 | 0.898 | 3.977 | 66.279 |
| 2 | 0.607 | 2.024 | 33.729 |
| Total | 6.000 | ||
| Mean | 0.800a | 3.000 | 50.004 |
aMean Cronbach's Alpha is based on the mean Eigenvalue
The summary from Table 2 shows how correlated each of the quantified variables is related to the dimensions. Most (4) of the variables loaded highly (measures ≥ 0.700) into D1 while none have similar attributes for D2. This explained why D1 has a lower percentage of explained variance and lower internal consistency.
Table 2.
Discriminant measures summary for identified dimensions
| Variables | Dimension | |
|---|---|---|
| 1 | 2 | |
| Trend_Grph | 0.687 | 0.436 |
| Trend_Park | 0.702 | 0.050 |
| Trend_Resd | 0.773 | 0.423 |
| Trend_RtRc | 0.566 | 0.522 |
| Trend_Wkpl | 0.536 | 0.502 |
| Trend_Trst | 0.712 | 0.091 |
| Active Total | 3.977 | 2.024 |
| % of Variance | 66.279 | 33.729 |
From the result (Table 2), there is an indication that D1 is the most relevant dimension for subsequent discussion. Hence, the distribution of the Object Scores for D1 for each State was represented in Fig. 6. From Fig. 6, there are some contiguous regions with similar characteristics across the northern and southern regions of the country. While there is an element of a divide across the two regions, the difference is pronounced along the south-west and spanned across the south–east with distinct characteristics for Rivers, Bayelsa, Cross River, and Ebonyi States. Across the central part of the country, Niger and Kogi exhibited distinct characteristics (Object Score for D1) compared to their neighbors. Similarly, Kaduna and FCT also showed distinction in D1 object score when compared to their neighbors.
Fig. 6.

Distribution of D1 object scores across the States
Two-step cluster analysis (IBM 2016) was carried out to examine the natural groupings that may exist within D1 Object Scores. The internal consistency of the members within the groups identified was examined using the Silhouette measure of cohesion and separation (Rousseeuw 1987). For this measure, cluster set with Silhouette measure value > 0.5 is considered to have a good cluster quality while < 0.5 but > 0.2 is considered fair.
The summary of the auto-clustering operation presented in Table 3, indicated that two clusters are the optimal number of clusters from the D1 object scores. The identification of two clusters is because the highest ratio of distance measure (Table 3) is greatest at 4.690 when the number of clusters is 3 compared to 4.453 for 3 clusters and 2.708 for 6 clusters.
Table 3.
Summary of the auto-clustering diagnostic for the two-step clustering analysis
| Number of clusters | Schwarz's Bayesian criterion (BIC) | BIC changea | Ratio of BIC changesb | Ratio of distance measuresc |
|---|---|---|---|---|
| 1 | 32.365 | |||
| 2 | 20.920 | 11.444 | 1.000 | 4.690 |
| 3 | 24.163 | 3.242 | 283 | 4.453 |
| 4 | 30.491 | 6.328 | 553 | 1.106 |
| 5 | 36.905 | 6.414 | 560 | 2.340 |
| 6 | 43.781 | 6.877 | 601 | 2.708 |
| 7 | 50.876 | 7.094 | 620 | 1.001 |
| 8 | 57.970 | 7.094 | 620 | 2.155 |
| 9 | 65.133 | 7.163 | 626 | 1.385 |
| 10 | 72.312 | 7.179 | 627 | 2.090 |
| 11 | 79.514 | 7.201 | 629 | 1.183 |
| 12 | 86.718 | 7.205 | 630 | 1.294 |
| 13 | 93.927 | 7.208 | 630 | 1.385 |
| 14 | 101.139 | 7.212 | 630 | 1.398 |
| 15 | 108.354 | 7.215 | 630 | 1.381 |
aThe changes are from the previous number of clusters in the table
bThe ratios of changes are relative to the change for the two-cluster solution
cThe ratios of distance measures are based on the current number of clusters against the previous number of clusters
Based on this result, the cluster distribution showed that 18 States (51.4%) belong to Cluster 1 while the remaining belong to Cluster 2 (Fig. 7). This clustering exhibited a good cluster quality (internal consistency) with a silhouette measure of 0.8. The object score utilised is a multidimensional index quantify the trend of mobility across six place categories during the national lockdown period. As such the groups identified could give a reflection of the perception of risk of infection among people of each group of States.
Fig. 7.

Distribution of D1 Object Scores cluster across the States
Examining the cluster membership against the trend categories depicted in Fig. 4a–f, the association can be identified (Table 4). Cluster 2 members are mostly showing uptrend for Grph Park, and Trst while most of them recorded a downtrend for Resd. The mobility trend for RtRc and Wkpl could not distinguish between the two clusters. However, for Resd, Cluster 2 is quite distinct with most members having a downtrend in mobility, while most members of Cluster show no discernible trend. Most members of Cluster 1 also showed no discernible trend for Grph, Park, and Trst.
Table 4.
Crosstabulation of trend category and cluster designation
| Place category | Cluster | Downtrend confidence | Not significant | Uptrend confidence | Total | ||||
|---|---|---|---|---|---|---|---|---|---|
| 99% | 95% | 90% | 90% | 95% | 99% | ||||
| Trend_Grph | 1 | 0 | 1 | 1 | 12 | 1 | 3 | 1 | 19 |
| 2 | 0 | 0 | 0 | 0 | 1 | 5 | 12 | 18 | |
| Trend_Park | 1 | 0 | 1 | 0 | 18 | 0 | 0 | 0 | 19 |
| 2 | 0 | 0 | 1 | 3 | 3 | 5 | 6 | 18 | |
| Trend_Resd | 1 | 1 | 2 | 1 | 14 | 0 | 1 | 0 | 19 |
| 2 | 14 | 2 | 1 | 0 | 0 | 0 | 1 | 18 | |
| Trend_RtRc | 1 | 3 | 1 | 0 | 3 | 0 | 2 | 10 | 19 |
| 2 | 0 | 0 | 0 | 0 | 0 | 0 | 18 | 18 | |
| Trend_Wkpl | 1 | 0 | 0 | 0 | 6 | 0 | 2 | 11 | 19 |
| 2 | 0 | 0 | 0 | 0 | 0 | 0 | 18 | 18 | |
| Trend_Trst | 1 | 0 | 0 | 0 | 18 | 0 | 1 | 0 | 19 |
| 2 | 0 | 0 | 0 | 3 | 0 | 5 | 10 | 18 | |
Discussion
State median mobility
There is a wide variation in changes from baseline mobility for this period across the country. Residential witnessed an overwhelming increase towards it while all the other place categories witnessed a decline relative to baseline. Moreover, there is no clear-cut regional pattern discernible from the median mobility values for all the place categories. Furthermore, while cumulative mobility for the unsafe place categories identified some hotspots of decline, a north–south divide is evident from the pattern. However, highly populated States such as Kaduna and Kano in the northern part of the country bucked that trend.
Space-time pattern/trend
As the lockdown draws longer, mobility toward retails and recreation facilities is ticking upwards. This is an indication that people need to get necessities and earn a living, movement cannot be effective if there are no alternatives to earn and secure daily needs. For Parks, there seems to be a North–South divide in the mobility trend. While mobility is picking up in the south, there is no clear trend recorded in the north. This could be attributed to the spread of the disease from the south towards the north. Many groceries and pharmacies in most States are allowed to open, albeit, some restrictions, this place category is expected to witness increased mobility. This is partly due to the need to meet daily necessities and the need to take care of other existing or new ailments.
Mobility towards transportation hubs indicated that across States where infections were discovered earlier and States around them, people are beginning to accept the risk and travel more. In essence, people are making decisions (to travel) despite the constraints (Zsolnai 1998)—the risk of exposure, potentially lack of full understanding of the disease, and their chances of survival. The mobility trend for the workplaces indicated that fatigue is taking hold, and more people are moving towards their workplaces. This could be as a result of the overwhelming population of people who need to earn daily to survive despite the risk. Thus, as more people gravitate toward their workplace the mobility trend recorded for residential areas is not surprising. Across most States, people are venturing out more as the fatigue of staying at home gets overwhelming, and the need to earn a living is becoming more dominant on their mind.
For reported new cases, the upward trend during the lockdown could be partly attributed to the varying level of enforcement of the mobility restriction, coupled with the need for many people to seek their daily income. This may have increased people's exposure and consequently infections. The ‘infodemic’ of misinformation—many conspiracies and fake news about the virus circulating on social media and the internet (Zarocostas 2020) may also be partly responsible for this trend as there is a lot of scepticism across many parts of the country. Write-ups and messages about instant remedies for the virus and several race targeted news were being propagated on various platforms (Rathore and Farooq 2020). This surely will impact how seriously people considered the need to respect the mobility restriction orders.
From the trend, there is an indication that mobility decision is being guided across most States by the risk acceptance principle. Mobility is picking up with people likely considering COVID-19 as just one of those ailments they are likely to get, as such they are willing to take the risk. With many States also having a few cases, there is also the tendency for people to underestimate the risk. Most significantly, the need to earn a living is a more dominant driver of mobility as evident in the uptick in mobility towards transportation hubs, workplaces, and downward mobility trends for residential areas. Recent studies showed that in the United States of America, COVID-19 infection rates increased with city size (Stier et al. 2020). Thus, the spread is effectively aided by mobility and proximity to urban landscapes as the quantum of cases is considerably higher for highly urbanised and densely populated States. Therefore, the increase in mobility across most States, is an indication of either poor perception of the risk posed by increased mobility and/or adoption of risk avoidance (non-pharmaceuticals) measures.
While some can afford to stay at home, many cannot as they must earn their living every single day evidently, the mobility restriction is a luxury for some and a severe cost for others. It is thus evident that the mitigation measures taken by each country will determine the course of the pandemic (Anderson et al. 2020). For example, there is evidence showing that as travel restrictions were implemented, this effectively slowed down the spread in the early days of the outbreak (Chinazzi et al. 2020; Kraemer et al. 2020). While this may be the case, prolonged lockdown without adequate provision to manage the individual challenges such posed to many households (especially in Nigeria where many required daily income to survive) will likely witness the waning of compliance as observed. This category of households as well as the rural dwellers were least compliant to the measures (Carlitz and Makhura 2020). It is well established that vulnerability and extent of the impact of disaster or hazard are a function of location as well as the socio-economic circumstances of the people affected (Lawal and Arokoyu 2015).
From the mobility trend during the pandemic, some indications of risk perception could be deduced. For example, the level of risk acceptance is almost similar across most States especially considering their mobility towards retail, recreation, and workplaces. However, from the mobility around residential area Cluster 2 States are venturing out (more acceptance) while Cluster 1 States are neither here nor there about venturing out—an indication of uncertainty about the risk. This uncertainty was also indicated in their mobility towards Parks, grocery, and pharmacy as well as transport hubs. The result indicated how knowledge, experience, values, attitudes, and feelings influence the judgement and decision about the acceptability and seriousness of risk–risk perception (Slovic 1987). There are differences between voluntary (knowingly taken risk) and involuntary (risk we are unable to control or not aware of) risk perception and the public willingness to accept voluntary risk is several folds greater than that of involuntary risks (Smith 2013). The way people view risk or perceived it is a major problem for mitigation. This was evident from the way varied mobility across the different Cluster of States. Therefore, actions taken by people (prevention and avoidance) is a function of their perception of the hazard (Coppola 2011). This perception also skews how they view the consequences and the likelihood of them getting infected. In essence, the actions captured by mobility gave a general indication of some aspects of peoples’ perception of the risk, consequences and likelihood them getting infected.
Conclusions
While it might be too early to conclude on the effect of the mobility restriction on the COVID-19 spread and cases, it is noteworthy that the extent of compliance varies from State to State as evidenced by the findings from this study. Thus, we might expect the evolution of the spread of the disease to follow the pattern of compliance with non-pharmaceutical measures e.g. mobility restrictions, use of face mask, hand washing, restriction of large number gatherings, etc.
From the space-time analyses, we can conclude that mobility evolved along the line of necessities for each of the place categories i.e. high decline for most and concurrent increased for residential at the beginning of the lockdown followed by gradual increase for all others except residential towards the end of the lockdown.
As mobility started an uptrend even during the lockdown period, there is an indication that generally, peoples' perception of the disease is to consider the pandemic as a voluntary risk. Thus, the need to earn a living is much more overwhelming than to stay at home and be safe. Higher resolution and multidimensional data would be required to ascertain how this plays out among different groups of people. But it could be expected that the perception may differ from person to person.
There was an increase in number of cases during the lockdown, it is possible to conclude that this is as a result of the non-compliance with the lockdown protocols and potentially in the increase in testing—leading to quicker identification of infected persons. The changes in compliance over time as indicated by mobility changes gave an indication of changes in risk perception and acceptance aggregated at the State level. Thus, the conclusion is that mobility, could indicate how people perceive the risk they are exposed to and the level of risk they are willing to take. However, further research on risk perception and risk compensation during the pandemic is pertinent to examine this in more detail.
The study utilised smartphone-based location data, thus, the mobility of people without GPS enabled smartphone is not captured and people with phones without google location history enabled are not captured. Thus, the data is incomplete but in the absence of mobility data for this period, there are no other alternatives. However, the data can indicate mobility during this period which is critical in tracking the distribution pattern as well as in predicting the number of cases in the various States.
From the foregoing, it is pertinent that risk perception and risk acceptance should be tracked and understanding from such be incorporated in the management of the pandemic. As restriction and information fatigue sets in, there is need to device means to change behaviour and stimulate actions and attitude that will ensure people stay safe and prevent the spread and resurgence of COVID-19 across various communities.
Funding
The authors did not receive any funding from any Organisation/Institution for this study (study was not funded by any grant).
Compliance with ethical standards
Conflict of interest
The authors declare that they have no conflict of interest.
Human or animal rights
This article does not contain any studies involving human or animals performed by any of the authors.
Footnotes
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Olanrewaju Lawal, Email: olanrewaju.lawal@uniport.edu.ng.
Chidozie Nwegbu, Email: dozienwegbu@gmail.com.
References
- Abdullahi, A.H. & Abdulkadir, M. (2020). An analysis of coronavirus disease transmission in relation to temperature variability in Nigeria. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511
- Addie, O., Taiwo, O., & Seun-Addie, K. (2020). Determining the vulnerability of states in Nigeria to COVID-19. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511.
- Adepoju, O., & Soladoye, O. (2020). Geospatial enabling strategies for timely containment of COVID-19 Pandemic in Lagos state. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511.
- Akintuyi, A., Badru, G., Fashoto, B., Sobanke, D., & Oladipo, R. (2020). Perception, impact and coping strategies to COVID-19 pandemic in Nigeria. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511.
- Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country-based mitigation measures influence the course of the COVID-19 epidemic? The Lancet. 2020;395(10228):931–934. doi: 10.1016/S0140-6736(20)30567-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Backup Rural. (2020). Nigeria: Coronavirus (Covid-19) subnational. Retrieved from: https://data.humdata.org/dataset/nigeria_covid19_subnational.
- Balcan D, Colizza V, Gonçalves B, Hu H, Ramasco JJ, Vespignani A. Multiscale mobility networks and the spatial spreading of infectious diseases. Proceedings of the National Academy of Sciences. 2009;106(51):21484–21489. doi: 10.1073/pnas.0906910106. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlitz RD, Makhura MN. Life under lockdown: Illustrating tradeoffs in South Africa’s response to COVID-19. World Development. 2020;137:105168. doi: 10.1016/j.worlddev.2020.105168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chia T, Oyeniran O. Will Africa experience a spike in COVID-19. Asian Pacific Journal of Tropical Medicine. 2020;13(7):285. doi: 10.4103/1995-7645.282560. [DOI] [Google Scholar]
- Chinazzi M, Davis JT, Ajelli M, Gioannini C, Litvinova M, Merler S, Vespignani A. The effect of travel restrictions on the spread of the 2019 novel coronavirus (COVID-19) outbreak. Science. 2020;368(6489):395–400. doi: 10.1126/science.aba9757. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohn SK., Jr The black death: End of a paradigm. The American Historical Review. 2002;107(3):703–738. doi: 10.1086/ahr/107.3.703. [DOI] [PubMed] [Google Scholar]
- Coppola, D. P. (2011). Risk and Vulnerability. In Introduction to International Disaster Management (2nd ed., pp. 138 - 207). Burlington: Butterworth-Heinemann.
- ESRI. (2019). ArcGIS Desktop (Version 10.7). Redlands, CA: Environmental Systems Research Institute.
- Fasona, M. (2020). COVID-19 vulnerability and pathways in Nigeria. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511.
- Google LLC. (2020). COVID-19 Community Mobility Report. Retrieved from https://www.google.com/covid19/mobility/index.html?hl=en.
- Graham-McLay, C. (2020, 2020/06/16/). New Zealand ends Covid-free run with two cases from UK. the Guardian. Retrieved from https://www.theguardian.com/world/2020/jun/16/new-zealand-records-first-new-covid-19-cases-after-women-arrive-from-uk-carrying-virus.
- IBM . IBM SPSS statistics (Version 23) Armonk, New York: IBM Corporation; 2015. [Google Scholar]
- IBM. (2016). Knowledge Centre -Two Step Cluster Analysis. Retrieved from https://www.ibm.com/support/knowledgecenter/SSLVMB_21.0.0/com.ibm.spss.statistics.help/idh_twostep_main.htm.
- Jones KE, Patel NG, Levy MA, Storeygard A, Balk D, Gittleman JL, Daszak P. Global trends in emerging infectious diseases. Nature. 2008;451(7181):990–993. doi: 10.1038/nature06536. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kang S, Peng W, Zhu Y, Lu S, Zhou M, Lin W, Wu W, Huang S, Jiang L, Luo X, Deng M. Recent progress in understanding 2019 novel coronavirus (SARS-CoV-2) associated with human respiratory disease: detection, mechanisms and treatment. International Journal of Antimicrobial Agents. 2020;55(5):105950. doi: 10.1016/j.ijantimicag.2020.105950. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kendall MG, Gibbons JD. Rank correlation methods. UK: Oxford University Press; 1990. [Google Scholar]
- Kraemer MUG, Yang C-H, Gutierrez B, Wu C-H, Klein B, Pigott DM, Scarpino SV. The effect of human mobility and control measures on the COVID-19 epidemic in China. Science. 2020;368(6490):493–497. doi: 10.1126/science.abb4218. [DOI] [PMC free article] [PubMed] [Google Scholar]
- La V, Pham T, Ho M, Nguyen M, Nguyen K, Vuong T, Vuong Q. Policy response, social media and science journalism for the sustainability of the public health system amid the COVID-19 outbreak: The Vietnam Lessons. Sustainability. 2020;12(7):2931. doi: 10.3390/su12072931. [DOI] [Google Scholar]
- Lawal O, Anyiam FE. Modelling geographic accessibility to primary health care facilities: Combining open data and geospatial analysis. Geo-spatial Information Science. 2019;22(3):174–184. doi: 10.1080/10095020.2019.1645508. [DOI] [Google Scholar]
- Lawal O, Arokoyu SB. Modelling social vulnerability in sub-Saharan West Africa using a geographical information system. Jàmbá: Journal of Disaster Risk Studies. 2015 doi: 10.4102/jamba.v7i1.155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mann HB. Nonparametric tests against trend. Econometrica: Journal of the Econometric Society. 1945;13(3):245–259. doi: 10.2307/1907187. [DOI] [Google Scholar]
- Morony MG. ‘For whom does the writer write?’: The first bubonic plague pandemic according to syriac sources. In: Little LK, editor. Plague and the end of antiquity : The pandemic of 541–750. Reprint. New York: Cambridge University Press; 2007. pp. 59–86. [Google Scholar]
- Nigeria Centre for Disease Control (NCDC). (2020). COVID-19 Outbreak in Nigeria: Situation Report. Retrieved from Abuja: https://ncdc.gov.ng/diseases/sitreps.
- Ogundokun RO, Lukman AF, Kibria GB, Awotunde JB, Aladeitan BB. Predictive modelling of COVID-19 confirmed cases in Nigeria. Infectious Diseases Modelling. 2020;5:543–548. doi: 10.1016/j.idm.2020.08.003. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ohadike DC. Diffusion and physiological responses to the influenza pandemic of 1918–19 in Nigeria. Social Science and Medicine. 1991;32(12):1393–1399. doi: 10.1016/0277-9536(91)90200-V. [DOI] [PubMed] [Google Scholar]
- Olabamiji, A. & Ajala, O. (2020). COVID-19 Lockdown effects, resilience, adaptation and coping strategies in Nigeria. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511.
- Olapegba, P. O., Iorfa, S. K., Kolawole, S. O., Oguntayo, R., Gandi, J. C., Ottu, I. F., & Ayandele, O. J. D. i. b. (2020). Survey data of COVID-19-related Knowledge, risk perceptions and precautionary behavior among Nigerians. 30, 105685. 10.1016/j.dib.2020.105685. [DOI] [PMC free article] [PubMed]
- Paintsil E. COVID-19 threatens health systems in sub-Saharan Africa: the eye of the crocodile. Journal of Clinical Investigation. 2020;130(6):2741–2744. doi: 10.1172/JCI138493. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rathore FA, Farooq FJ. Information Overload and Infodemic in the COVID-19 Pandemic. The Journal of the Medical Association. 2020;70(5):S162–S165. doi: 10.5455/JPMA.38. [DOI] [PubMed] [Google Scholar]
- Riley S. Large-scale spatial-transmission models of infectious disease. Science. 2007;316(5829):1298–1301. doi: 10.1126/science.1134695. [DOI] [PubMed] [Google Scholar]
- Rousseeuw PJ. Silhouettes: A graphical aid to the interpretation and validation of cluster analysis. Journal of Computational and Applied Mathematics. 1987;20:53–65. doi: 10.1016/0377-0427(87)90125-7. [DOI] [Google Scholar]
- Slovic P. Perception of risk. Science. 1987;236(4799):280–285. doi: 10.1126/science.3563507. [DOI] [PubMed] [Google Scholar]
- Smith K. Environmental hazards: Assessing risk and reducing disaster. 6. Abingdon: Routledge; 2013. [Google Scholar]
- Stier, A., Berman, M., & Bettencourt, L. (2020). COVID-19 attack rate increases with city size. Mansueto Institute for Urban Innovation Research Paper. Retrieved from https://ssrn.com/abstract=3564464.
- Taiwo, O. J. & Olumoyegun, J. M. (2020). Distant decay analysis of airports and the number of confirmed COVID-19 in Nigeria. Proceedings of a special virtual conference on COVID-19 of the association of Nigerian geographers (southwest zone). https://ssrn.com/abstract=3683511.
- Xie M, Chen Q. Insight into 2019 novel coronavirus—an updated intrim review and lessons from SARS-CoV and MERS-CoV. International Journal of Infectious Diseases. 2020;94:119. doi: 10.1016/j.ijid.2020.03.071. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zarocostas J. How to fight an infodemic. The Lancet. 2020;395(10225):676. doi: 10.1016/S0140-6736(20)30461-X. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zsolnai L. Rational choice and the diversity of choices. The Journal of Socio-Economics. 1998;27(5):613–622. doi: 10.1016/S1053-5357(99)80114-0. [DOI] [Google Scholar]