

Abstract
Purpose
To determine the utility of chest radiography in aiding clinical diagnosis of coronavirus disease 2019 (COVID-19) utilizing reverse-transcription polymerase chain reaction (RT-PCR) as the standard of comparison.
Materials and Methods
A retrospective study was performed of persons under investigation for COVID-19 presenting to this institution during the exponential growth phase of the COVID-19 outbreak in New Orleans (March 13–25, 2020). Three hundred seventy-six in-hospital chest radiographic examinations for 366 individual patients were reviewed along with concurrent RT-PCR tests. Two experienced radiologists categorized each chest radiograph as characteristic, nonspecific, or negative in appearance for COVID-19, utilizing well-documented COVID-19 imaging patterns. Chest radiograph categorization was compared against RT-PCR results to determine the utility of chest radiography in diagnosing COVID-19.
Results
Of the 366 patients, the study consisted of 178 male (49%) and 188 female (51%) patients with a mean age of 52.7 years (range, 17 to 98 years). Of the 376 chest radiographic examinations, 37 (10%) exhibited the characteristic COVID-19 appearance; 215 (57%) exhibited the nonspecific appearance; and 124 (33%) were considered negative for a pulmonary abnormality. Of the 376 RT-PCR tests evaluated, 200 (53%) were positive and 176 (47%) were negative. RT-PCR tests took an average of 2.5 days ± 0.7 to provide results. Sensitivity and specificity for correctly identifying COVID-19 with a characteristic chest radiographic pattern was 15.5% (31/200) and 96.6% (170/176), with a positive predictive value and negative predictive value of 83.8% (31/37) and 50.1% (170/339), respectively.
Conclusion
The presence of patchy and/or confluent, bandlike ground-glass opacity or consolidation in a peripheral and mid to lower lung zone distribution on a chest radiograph obtained in the setting of pandemic COVID-19 was highly suggestive of severe acute respiratory syndrome coronavirus 2 infection and should be used in conjunction with clinical judgment to make a diagnosis.
© RSNA, 2020
Summary
A characteristic chest radiographic appearance with high specificity and positive predictive value for COVID-19 infection in the setting of pandemic spread is described.
Key Point
■ A characteristic chest radiographic appearance as defined in this article is highly specific (96.6%) and has a high positive predictive value (83.8%) for severe acute respiratory syndrome coronavirus 2 infection in the setting of a pandemic.
Introduction
To date, severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), also known as 2019 novel coronavirus, has infected millions of patients and claimed over 200,000 lives globally, and these numbers continue to grow rapidly (1). The utility of thoracic CT for diagnosing pneumonia associated with coronavirus disease 2019 (COVID-19), the disease caused by SARS-CoV-2, has been a focus worldwide with ample literature originating in particular from experts in China, the United States, and Europe, where specific CT patterns have been recognized in affected patients (2–12). Nonetheless, leading radiologic societies have discouraged the use of CT as a screening tool (5,6,13) with reverse-transcription polymerase chain reaction (RT-PCR) testing considered to be the reference standard for COVID-19 diagnostic screening (14–16). Rather, these societies recommend CT use be reserved for management of patients with COVID-19 with worsening and/or severe respiratory symptoms, in particular for those in a hospital setting or those having special indications for CT (6,13). These recommendations, coupled with additional concerns regarding CT, including risks associated with patient transport and scanner decontamination, have undoubtedly led to fewer CT examinations for persons under investigation for COVID-19 (13,17). Conversely, chest radiography has been widely used in these patients who usually present with respiratory symptoms (18); yet, much less has been written about chest radiography with respect to COVID-19. We have observed a chest radiographic pattern in patients during the exponential growth phase of the COVID-19 outbreak in New Orleans (19) which is in accordance with the most commonly recognized CT features of COVID-19 in recent literature (2,7,9,10,12,20–27). These observations may be useful for patient triage or may assist in discharge and quarantine planning in which rapid and highly sensitive and specific testing is lacking.
Materials and Methods
Our institutional review board approved this study (IRB# 20–838) and deemed it to be compliant with the Health Insurance Portability and Accountability Act. We performed a retrospective database query within our institution’s electronic medical record system for all patients who had undergone COVID-19 RT-PCR testing utilizing the United States Centers for Disease Control and Prevention (CDC) assay between March 13 and March 26, 2020. These dates represent the period of upswing and exponential growth of COVID-19 incidence in New Orleans. The query returned 383 RT-PCR tests performed in 373 patients, with 10 patients with repeat RT-PCR and chest radiography (which were treated as unique entries for the purpose of data analysis). Six cases were excluded for lack of a corresponding chest radiography and one case was excluded for an inconclusive RT-PCR result, with a final total of 376 coincident chest radiographic examinations and PCR tests evaluated for 366 individual patients. Therefore, our case count represented 366 chest radiographic examinations and PCR tests acquired on presentation at our institution (one set of tests for each of the patients in our study) plus 10 sets of chest radiography/PCR for patients counted above but who also underwent repeat tests later in their hospital course. Sex, age, chief complaint (Table 1), and body mass index were also collected for the cohort.
Table 1:
Clinical Reason for Examination, by Chest Radiographic Pattern

Data Interpretation
Two board-certified radiologists with greater than 10 years’ experience interpreting chest radiographs, blinded to RT-PCR results, independently assessed 376 portable anteroposterior or upright posteroanterior chest radiographs in 366 patients (Fig 1) obtained on the day of testing or immediately prior to that date. Patients with radiographs obtained more than 2 days prior to RT-PCR testing were excluded. Readers assigned one of three patterns: characteristic, nonspecific, and negative (Table 2). A subsequent consensus read was performed to address discrepancies between the two readers. The characteristic COVID-19 pattern (Figs 2–4) was defined in accordance with the prevailingly accepted chest imaging findings of COVID-19 in recent literature (2,12,20,24,25,27–29), including the presence of bilateral patchy or confluent, bandlike ground-glass opacity or consolidation in a peripheral and mid to lower lung zone distribution. If the chest radiograph showed a pleuropulmonary abnormality other than the previously mentioned description, it was assigned to the nonspecific category. Nonspecific radiographs were grouped according to type of abnormality (masslike, upper lung zone predominant, diffuse, ill-defined bibasilar, focal/unilateral, effusion). A radiograph without any perceived pleuropulmonary abnormality was labeled negative (Table 3).
Figure 1:

Methods flowchart. CXR = chest radiography, PCR = polymerase chain reaction.
Table 2:
Chest Radiograph Characterization by Findings

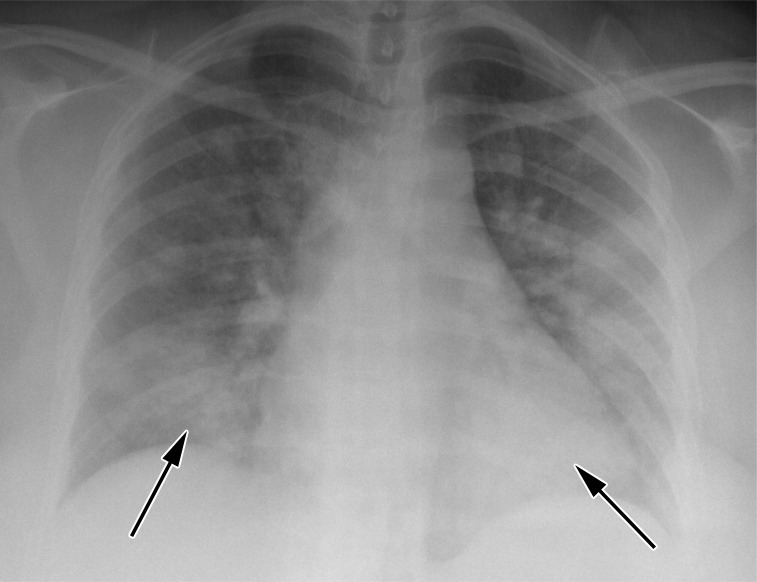
Figure 2:

Characteristic chest radiograph in a 63-year-old woman presenting with dyspnea and fever. Chest radiographic findings include bilateral patchy and confluent, bandlike ground-glass and consolidative opacity in a peripheral, mid to lower lung zone distribution (arrows).
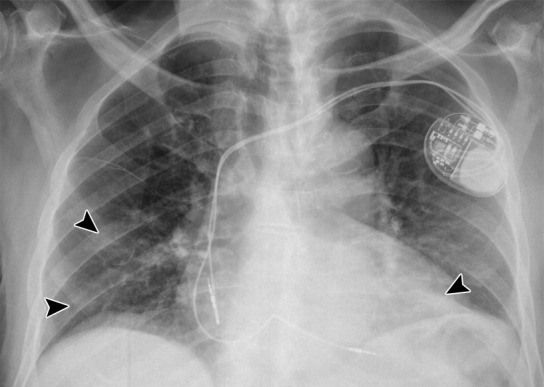
Figure 4:

A more subtle characteristic radiograph in a 41-year-old man presenting with dyspnea and chest pain. Patchy ground-glass opacities are limited to the peripheral portions of the mid lung zones (arrows).
Table 3:
Summary of Radiographic Findings

Figure 3:

Characteristic chest radiograph in a 41-year-old woman presenting with cough and fever. Chest radiographic findings include bilateral patchy and confluent, bandlike ground-glass and consolidative opacity in a peripheral, mid to lower lung zone distribution (arrows).
Statistical Analysis
Statistical analysis was performed using Microsoft Excel software (Microsoft [2018]). Chest radiograph characterizations were compared with RT-PCR tests, considered the reference standard. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated on consensus reads. Interreader agreement was assessed using Cohen κ coefficient.
Results
Patient and Clinical Characteristics
The clinical characteristics of the 366 patients at the time of RT-PCR testing included: 178 male (49%) and 188 female (51%) patients, with a mean age of 52.7 years (range, 17 to 98 years). Average patient body mass index was 32.0 kg/m2 ± 9.7 (standard deviation). Various clinical indications for the examinations in question are listed in Table 3. Of the 376 chest radiographic examinations, 37 (10%) exhibited the characteristic COVID-19 appearance, 215 (57%) exhibited the nonspecific appearance, and 124 (33%) were considered negative for pleuropulmonary abnormality. The two readers had almost perfect agreement (30) on evaluation of chest radiographic examinations for COVID-19 (κ = 0.8627), agreeing on 346 (92.02%) total chest radiographic examinations. Of the 376 RT-PCR tests evaluated, 200 (53%) were positive and 176 (47%) were negative. One was inconclusive. RT-PCR tests took an average of 2.5 days ± 0.7 to provide results.
Chest Radiographic Correlation with RT-PCR
Sensitivity and specificity were calculated to be 15.5% (31/200) and 96.6% (170/176), respectively, with P < .000001 as determined by a McNemar χ2 test. PPV and NPV were 83.8% (31/37) and 50.1% (170/339), respectively. True-positive findings consisted of patients having both a characteristic chest radiographic appearance and a positive RT-PCR result for COVID-19 (true positive = 31). A true negative was a patient who had a negative RT-PCR result with either a negative or nonspecific chest radiograph. A false positive therefore was a patient considered to have a characteristic appearance on a chest radiograph but had a negative RT-PCR result. False negatives were patients considered to be either nonspecific or normal in appearance on chest radiograph but had a positive RT-PCR (false negative = 169). The achieved high specificity (96.6%) of this study was attributed to the high number of true negatives (n = 170) and relatively few false positives (n = 6). We attributed these numbers to a very strict definition of a positive, characteristic radiographic appearance for COVID-19. Given this narrow classification, our study had few false positives as well as few true positives, six and 31, respectively. As a result, the specificity of our study should be considered in conjunction with our PPV (83.8%).
Discussion
The chest radiograph, while low in sensitivity, can be highly suggestive of COVID-19 in patients whose radiographs exhibit characteristic COVID-19 findings, when used in concert with clinical factors. While not a substitute for RT-PCR or chest CT, chest radiography could provide rapid, cost-effective diagnosis of COVID-19 in a subset of infected patients (estimated at 15 out of 100 in our cohort), during the COVID-19 pandemic. The utility of this technique is described in the context of known disadvantages of RT-PCR, considered the reference standard in COVID-19 diagnosis, and chest CT, which is currently not recommended for diagnosis of COVID-19 (13). Moreover, it is important to note that the observed specificity of radiographic findings in this study was significantly influenced by the prevalence of COVID-19 in the community and would only serve to guide management in the context of a pandemic.
Variable RT-PCR sensitivities have been reported, ranging from 30% to 91% (28,31). This may be the result of relatively lower viral loads in individuals who are asymptomatic or experience only mild symptoms. Furthermore, tests performed when symptoms were resolving also resulted in false negatives (14,32,33). These low sensitivities result in false-negative tests, potentially leading to patient discharge without appropriate planning and creating the potential of community transmission of disease by patients incorrectly cleared by the health care system. Also, RT-PCR testing has been difficult to obtain, especially in the earliest days of the COVID-19 outbreak in New Orleans. Because of a dearth of tests and testing supplies, only patients at the highest pretest probability were tested, while others were diagnosed clinically. As we know now and suspected then, many more patients were infected than tested (19). Initially, RT-PCR assays and kits from the United States CDC were utilized. Later, other tests with varying sensitivities and specificities became available. In this study we relied solely on the CDC assay by way of the nasopharyngeal swab, which was collected and processed in accordance with CDC guidelines (34,35). Finally, RT-PCR results can take time. Within our population, RT-PCR tests took an average of 2.5 days to provide results. During this time, patients and health care providers had to make important decisions relying almost solely on clinical data and interpretations of chest radiographs. These deficiencies lead to clinical problems, including uncertainty in decisions regarding admission (to the floor or to an isolation room/unit) and discharge planning (routine discharge home or to quarantine). Similar challenges in health care have been reported in the United States and elsewhere (36–39). Early in the pandemic in Wuhan, this led to some physicians relying upon CT as a correlate to clinical suspicion for COVID-19 in an effort to guide decision making for quarantine efforts and attempts to limit disease spread (39).
With CT usage in persons under investigation for COVID-19 being largely dissuaded (6,13), there is an opportunity for the ubiquitous chest radiograph to be useful. While chest radiographs of most persons under investigation are either negative or reveal nonspecific abnormalities (Fig 5), there is a characteristic pattern of opacity that can aid in diagnosis. That pattern corresponds to a subset of patients with the typical pattern discussed in the joint statement on reporting by the American College of Radiology, the Radiological Society of North America, and the Society of Thoracic Radiology (5). The characteristic pattern, therefore, indicates an idiosyncratic distribution of acute lung injury and/or organizing pneumonia which is more clearly illustrated with CT.
Figure 5a:
Three anteroposterior radiographs demonstrate nonspecific findings. A, Diffuse bilateral opacities including ground glass and bibasilar consolidation (arrows), in a more central distribution than in the characteristic pattern. B, Ill-defined, bibasilar opacities (arrowheads). C, Focal, unilateral airspace disease (arrows).
Figure 5b:
Three anteroposterior radiographs demonstrate nonspecific findings. A, Diffuse bilateral opacities including ground glass and bibasilar consolidation (arrows), in a more central distribution than in the characteristic pattern. B, Ill-defined, bibasilar opacities (arrowheads). C, Focal, unilateral airspace disease (arrows).
Figure 5c:

Three anteroposterior radiographs demonstrate nonspecific findings. A, Diffuse bilateral opacities including ground glass and bibasilar consolidation (arrows), in a more central distribution than in the characteristic pattern. B, Ill-defined, bibasilar opacities (arrowheads). C, Focal, unilateral airspace disease (arrows).
Due to the aforementioned limitations of RT-PCR and current recommendations against routine use of CT, recognition of the characteristic chest radiographic pattern used in conjunction with clinical judgment may allow clinicians to diagnose COVID-19. However, the main hurdle in using our approach to the characteristic COVID-19 chest radiograph is the associated low sensitivity. Wong et al reported a sensitivity, as it pertains to the diagnostic ability of a baseline chest radiograph compared with RT-PCR in detecting COVID-19, to be 69% and 91%, respectively (28). Our calculated sensitivity was 15.3%. We attribute this discordance to stark differences in image evaluation between our studies. The image evaluation in the work of Wong et al (28) was based upon a scoring system for the evaluation of pulmonary edema, the radiographic assessment of lung edema (RALE) score (40). As such, readers identified areas of lung consolidation/opacity and rendered a severity score. The study’s baseline chest radiographic sensitivity was then calculated based on a score of greater than “zero” which was denoted as an absence of pulmonary opacification or consolidation, such that any opacification/consolidation (even if singular in one lung) was considered positive (28). In our design, a chest radiograph was considered positive only if a characteristic pattern was seen, necessitating the presence of bilateral opacity/consolidation in a peripheral and mid to lower lung zone distribution. This stricter inclusion criterion resulted in far fewer true positives and a high number of false negatives for our study, yielding a low sensitivity but a higher specificity. It cannot be overstated that calculated specificity was undoubtedly shaped by the plenitude of COVID-19 in our patient population at the time of this study and therefore should be used for guidance of patient management only in the setting of such a pandemic.
Statistical analysis of our data also revealed six false-positive chest radiographic results. A few issues may generate false-positive results while utilizing our approach. First, false-positive chest radiographic interpretations may be a reflection of the variability of RT-PCR sensitivities, as discussed previously. These RT-PCR false-negative cases should proportionally manifest as false-positive results in our study. In fact, in two of our six false-positive cases, at least one clinical service determined a clinical diagnosis of COVID-19 with presumptive false-negative PCR results. Other scenarios might produce false-positive results as well. Abundant soft tissue of the chest wall (as may be seen in obesity or breast tissue) may result in inadequate penetration of the x-ray beam, simulating peripheral, basilar airspace opacity as the tissue lateralizes in the supine patient (41). These simulated pulmonary opacities may manifest as false-positive radiographs. Furthermore, the pattern of disease we have labeled as characteristic of COVID-19 can be seen in other pathologic conditions. The differential diagnosis list includes chronic eosinophilic pneumonia, nonspecific interstitial pneumonia, organizing pneumonia, and acute lung injury, including diffuse alveolar damage, among others (42,43). These histologic diagnoses, in turn, may result from any number of insults, including autoimmune disease, drug toxicity, and viruses other than SARS-CoV-2. We do not propose, therefore, that the characteristic pattern herein should always suggest COVID-19 positivity—the pattern may be seen in other conditions. Nevertheless, this pattern is quite uncommon outside of the setting of pandemic; the corresponding author appreciated several characteristic cases per day in late March and early April 2020 and could only recall a few such cases in the previous 10 years of his career. With the particulars of recall bias set aside, we believe it is fair to say that in the setting of pandemic COVID-19, the characteristic pattern notable on chest radiographs should be highly suggestive of SARS CoV-2 infection, and that patient triage and disposition should be informed by that suggestion. At times when serologic testing is deficient in number or quality, or when result wait times are inconveniently long, chest radiography provides a useful diagnostic tool.
Our study had limitations as discussed in detail previously. These limitations included variability in timing between chest radiography and RT-PCR; the broad scope of the nonspecific category and narrow scope of the characteristic category; uncertainty in RT-PCR sensitivity; and variability in image quality and technique. Future work would address many of these limitations. Sensitivity and specificity of chest radiography results could be correlated with body mass index, breast tissue, and technique, to address the potential confounder of inconsistent image quality. Reanalysis of chest radiographic images utilizing either a scoring system or a four-tiered rather than a three-tiered categorization system may offer improved sensitivity in an “intermediate” category defined between characteristic and nonspecific. Finally, as more information regarding the CDC RT-PCR test emerges and RT-PCR sensitivities and specificities become better known, and as RT-PCR tests continue to improve, chest radiography results could be correlated with newer and more sensitive RT-PCR tests which could decrease false-positive chest radiography results and increase true-negative chest radiography results.
Interpretation
The presence of bilateral patchy and/or confluent, bandlike ground-glass opacity or consolidation in a peripheral and mid to lower lung zone distribution on a chest radiograph obtained in the setting of pandemic COVID-19 is highly suggestive of SARS-CoV-2 infection and should be used in conjunction with clinical judgment to make a diagnosis, especially when rapid and reliable serologic testing is lacking.
Acknowledgments
Acknowledgments
The authors thank the health care workers of New Orleans for their strength and dedication and the citizens of New Orleans for their cooperation and good will during the COVID-19 pandemic of 2020.
Disclosures of Conflicts of Interest: D.L.S. Activities related to the present article: disclosed no relevant relationships. Activities not related to the present article: author provides expert testimony for Hall Booth Smith on a matter unrelated to this article; author is paid by Genentech for speakers bureau giving nonbranded lectures on interstitial lung disease (unrelated to this article). Other relationships: disclosed no relevant relationships. J.P.G. disclosed no relevant relationships. C.B. disclosed no relevant relationships. B.S. disclosed no relevant relationships.
Abbreviations:
- CDC
- Centers for Disease Control and Prevention
- COVID-19
- coronavirus disease 2019
- NPV
- negative predictive value
- PPV
- positive predictive value
- RT-PCR
- reverse-transcription polymerase chain reaction
- SARS-CoV-2
- severe acute respiratory syndrome coronavirus 2
References
- 1.COVID-19 Dashboard by the Center for Systems Science and Engineering (CSSE). https://coronavirus.jhu.edu/map.html. Accessed April 21, 2020.
- 2.Zhou S, Wang Y, Zhu T, Xia L. CT Features of Coronavirus Disease 2019 (COVID-19) Pneumonia in 62 Patients in Wuhan, China. AJR Am J Roentgenol 2020;214(6):1287–1294. [DOI] [PubMed] [Google Scholar]
- 3.Li M, Lei P, Zeng B, et al. Coronavirus Disease (COVID-19): Spectrum of CT Findings and Temporal Progression of the Disease. Acad Radiol 2020;27(5):603–608. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Cheng Z, Lu Y, Cao Q, et al. Clinical Features and Chest CT Manifestations of Coronavirus Disease 2019 (COVID-19) in a Single-Center Study in Shanghai, China. AJR Am J Roentgenol 2020;215(1):121–126. [DOI] [PubMed] [Google Scholar]
- 5.Simpson S, Kay FU, Abbara S, et al. Radiological Society of North America Expert Consensus Statement on Reporting Chest CT Findings Related to COVID-19. Endorsed by the Society of Thoracic Radiology, the American College of Radiology, and RSNA - Secondary Publication. J Thorac Imaging 2020;35(4):219–227. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Rubin GD, Ryerson CJ, Haramati LB, et al. The Role of Chest Imaging in Patient Management During the COVID-19 Pandemic: A Multinational Consensus Statement From the Fleischner Society. Chest 2020;158(1):106–116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Ye Z, Zhang Y, Wang Y, Huang Z, Song B. Chest CT manifestations of new coronavirus disease 2019 (COVID-19): a pictorial review. Eur Radiol 2020;30(8):4381–4389. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Wei J, Xu H, Xiong J, et al. 2019 Novel Coronavirus (COVID-19) Pneumonia: Serial Computed Tomography Findings. Korean J Radiol 2020;21(4):501–504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Guan W, Liu J, Yu C. CT Findings of Coronavirus Disease (COVID-19) Severe Pneumonia. AJR Am J Roentgenol 2020;214(5):W85–W86. [DOI] [PubMed] [Google Scholar]
- 10.Han R, Huang L, Jiang H, Dong J, Peng H, Zhang D. Early Clinical and CT Manifestations of Coronavirus Disease 2019 (COVID-19) Pneumonia. AJR Am J Roentgenol 2020;215(2):338–343. [DOI] [PubMed] [Google Scholar]
- 11.Chung M, Bernheim A, Mei X, et al. CT imaging features of 2019 novel coronavirus (2019-nCoV). Radiology 2020;295(1):202–207. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Zhao W, Zhong Z, Xie X, Yu Q, Liu J. Relation Between Chest CT Findings and Clinical Conditions of Coronavirus Disease (COVID-19) Pneumonia: A Multicenter Study. AJR Am J Roentgenol 2020;214(5):1072–1077. [DOI] [PubMed] [Google Scholar]
- 13.American College of Radiology . ACR recommendations for the use of chest radiography and computed tomography (CT) for suspected COVID-19 infection. Reston, Va: American College of Radiology, 2020. [Google Scholar]
- 14.Tahamtan A, Ardebili A. Real-time RT-PCR in COVID-19 detection: issues affecting the results. Expert Rev Mol Diagn 2020;20(5):453–454. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Noh JY, Yoon SW, Kim DJ, et al. Simultaneous detection of severe acute respiratory syndrome, Middle East respiratory syndrome, and related bat coronaviruses by real-time reverse transcription PCR. Arch Virol 2017;162(6):1617–1623 [Published correction appears in Arch Virol 2018;163(3):819.]. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Shen M, Zhou Y, Ye J, et al. Recent advances and perspectives of nucleic acid detection for coronavirus. J Pharm Anal 2020;10(2):97–101. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mossa-Basha M, Medverd J, Linnau K, et al. Policies and Guidelines for COVID-19 Preparedness: Experiences from the University of Washington. Radiology: 2020. 10.1148/radiol.202020132. Published online April 8, 2020. [DOI] [PubMed] [Google Scholar]
- 18.Tu YF, Chien CS, Yarmishyn AA, et al. A Review of SARS-CoV-2 and the Ongoing Clinical Trials. Int J Mol Sci 2020;21(7):E2657. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.COVID-19 Projections . https://covid19.healthdata.org/united-states-of-america/louisiana. Accessed April 21, 2020.
- 20.Kong W, Agarwal PP. Chest Imaging Appearance of COVID-19 Infection. Radiol Cardiothorac Imaging 2020;2(1):e200028. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Feng H, Liu Y, Lv M, Zhong J. A case report of COVID-19 with false negative RT-PCR test: necessity of chest CT. Jpn J Radiol 2020;38(5):409–410. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Shi F, Yu Q, Huang W, Tan C. 2019 Novel Coronavirus (COVID-19) Pneumonia with Hemoptysis as the Initial Symptom: CT and Clinical Features. Korean J Radiol 2020;21(5):537–540. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Chen Z, Fan H, Cai J, et al. High-resolution computed tomography manifestations of COVID-19 infections in patients of different ages. Eur J Radiol 2020;126:108972. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Bai HX, Hsieh B, Xiong Z, et al. Performance of Radiologists in Differentiating COVID-19 from Non-COVID-19 Viral Pneumonia at Chest CT. Radiology 2020;296(2):E46–E54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Salehi S, Abedi A, Balakrishnan S, Gholamrezanezhad A. Coronavirus Disease 2019 (COVID-19): A Systematic Review of Imaging Findings in 919 Patients. AJR Am J Roentgenol 2020;215(1):87–93. [DOI] [PubMed] [Google Scholar]
- 26.Li X, Zeng X, Liu B, Yu Y. COVID-19 infection presenting with CT halo sign. Radiol Cardiothorac Imaging 2020;2(1):e200026. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Guan CS, Lv ZB, Yan S, et al. Imaging Features of Coronavirus disease 2019 (COVID-19): Evaluation on Thin-Section CT. Acad Radiol 2020;27(5):609–613. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Wong HYF, Lam HYS, Fong AH, et al. Frequency and Distribution of Chest Radiographic Findings in Patients Positive for COVID-19. Radiology 2020;296(2):E72–E78. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 29.Hosseiny M, Kooraki S, Gholamrezanezhad A, Reddy S, Myers L. Radiology Perspective of Coronavirus Disease 2019 (COVID-19): Lessons From Severe Acute Respiratory Syndrome and Middle East Respiratory Syndrome. AJR Am J Roentgenol 2020;214(5):1078–1082. [DOI] [PubMed] [Google Scholar]
- 30.Landis JR, Koch GG. The measurement of observer agreement for categorical data. Biometrics 1977;33(1):159–174. [PubMed] [Google Scholar]
- 31.Ai T, Yang Z, Hou H, et al. Correlation of Chest CT and RT-PCR Testing for Coronavirus Disease 2019 (COVID-19) in China: A Report of 1014 Cases. Radiology 2020;296(2):E32–E40. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Lippi G, Simundic AM, Plebani M. Potential preanalytical and analytical vulnerabilities in the laboratory diagnosis of coronavirus disease 2019 (COVID-19). Clin Chem Lab Med 2020;58(7):1070–1076. [DOI] [PubMed] [Google Scholar]
- 33.Sheridan C. Coronavirus and the race to distribute reliable diagnostics. Nat Biotechnol 2020;38(4):382–384. [DOI] [PubMed] [Google Scholar]
- 34.Nalla AK, Casto AM, Huang MW, et al. Comparative Performance of SARS-CoV-2 Detection Assays Using Seven Different Primer-Probe Sets and One Assay Kit. J Clin Microbiol 2020;58(6):e00557–e00520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Carter LJ, Garner LV, Smoot JW, et al. Assay Techniques and Test Development for COVID-19 Diagnosis. ACS Cent Sci 2020;6(5):591–605. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Gozansky EK, Moore WH. SARS-CoV-2 From the Trenches: A Perspective From New York City. AJR Am J Roentgenol 2020;215(1):27–28. [DOI] [PubMed] [Google Scholar]
- 37.Lessons from the frontline of the covid-19 outbreak . The BMJ. https://blogs.bmj.com/bmj/2020/03/20/lessons-from-the-frontline-of-the-covid-19-outbreak/. Accessed April 21, 2020.
- 38.Imaging the coronavirus disease COVID-19 . https://healthcare-in-europe.com/en/news/imaging-the-coronavirus-disease-covid-19.html. Accessed April 21, 2020.
- 39.Yu J, Ding N, Chen H, et al. Infection Control against COVID-19 in Departments of Radiology. Acad Radiol 2020;27(5):614–617. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40.Warren MA, Zhao Z, Koyama T, et al. Severity scoring of lung oedema on the chest radiograph is associated with clinical outcomes in ARDS. Thorax 2018;73(9):840–846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Uppot RN, Sahani DV, Hahn PF, Gervais D, Mueller PR. Impact of obesity on medical imaging and image-guided intervention. AJR Am J Roentgenol 2007;188(2):433–440. [DOI] [PubMed] [Google Scholar]
- 42.Jeong YJ, Kim KI, Seo IJ, et al. Eosinophilic lung diseases: a clinical, radiologic, and pathologic overview. RadioGraphics 2007;27(3):617–637; discussion 637–639. [DOI] [PubMed] [Google Scholar]
- 43.Kligerman SJ, Franks TJ, Galvin JR. From the radiologic pathology archives: organization and fibrosis as a response to lung injury in diffuse alveolar damage, organizing pneumonia, and acute fibrinous and organizing pneumonia. RadioGraphics 2013;33(7):1951–1975. [DOI] [PubMed] [Google Scholar]