

Abstract
Since the initiation of national healthcare reform in 2009, China’s hospital market has witnessed significant change. To provide a brief description about its evolving process, China Health Statistical Yearbook data and Sichuan administrative data from 2009 to 2017 were used in this article. An overall upward trend of hospital delivery capacity was found in this study, which increased from 3.12 million beds and 1.09 million doctors in 2009 to 6.12 million and 1.80 million in 2017, respectively, while the primary healthcare institutions presented fairly slow development pace. Growing proportion of medical resources and patients gathered in hospitals, especially tertiary hospitals. While private hospitals demonstrated an increasingly important role in hospital market with growing share of capacity and service, their average capacity, especially the human resource, was found to be much lower than that of public hospitals and the gaps are still widening. The competition among hospitals grouped by homogeneous ownership types has predominated the increasingly intensified hospital market competition in China. In order to adapt to the raising demand of health care in China, it is highly recommended that strategies forged at governmental levels be focused on primary care promotion, guiding the development of private hospitals as well as on promoting orderly competition in the hospital market.
Keywords: capacity, medical service, market share, hospital competition, China
What do we already know about this topic?
After the national healthcare reform, multi-dimensional policies have been implemented which might have changed the hospital market.
How does your research contribute to the field?
As previous literature merely provided scarce evidences on investigating the impacts of healthcare reform in China on its nationwide hospital market since 2009, our study was expected to contribute to relevant literature in this field via demonstrating the evolving process of China’s hospital market from multiple aspects including hospital capacity, market share and market concentration, which further provided evidence-based implications for policy-making procedures in order to optimize the nationwide healthcare system.
What are your research’s implications toward theory, practice, or policy?
Hospital market in China was still dominated by the public and tertiary hospitals, the promotion of healthcare at primary levels should be emphasized as an essential strategy during future policy-making procedures. Instructions regarding to the development of private hospitals should also be provided at governmental levels in order to achieve the optimization of nationwide hospital market via constant promotion of orderly competition performances among various hospitals.
Introduction
The healthcare system in China has demonstrated deficiency in meeting the rapidly raising demands of high-quality medical services in parallel with the prospering economy. In attempt to find a solution for the nationwide issue summarized as “kan bing nan, kan bing gui” (the access to medical service is hard to obtain while unaffordable medical cost remains a ubiquitous problem), the Chinese government initiated a new phase for national healthcare reform in 2009. Based on the implementation of multi-dimensional policies, the healthcare reform had been expected to bring about significant impact on the hospital market structure in China, which would be reflected in 3 aspects including hospitals’ delivery capacity, the development pace of private hospitals as well as competitions among various hospitals.
As a considerable amount of key strategies designed for the new healthcare reform had been focused on the development of primary care institutions,1-4 it was not surprising to assume that the growth rate of primary healthcare institutions would exceed that of the overall hospitals’ delivery capacity with an increasing tendency expected to be seen in both areas. Specifically, half of the national budget planned in promoting the healthcare delivery and financing system, which reached CN¥850 billion, was spent on improving this aspect at primary healthcare level.5 Putting restriction on the expansion of public hospitals (mainly tertiary hospitals) had been proposed as another strategy to encourage the development of primary healthcare institutions.6,7 In terms of improving the quality and efficiency of healthcare delivery at primary care level, abundant medical resources of high quality had been planned for allocation in primary healthcare institutions8 as an incentive for attracting healthcare professionals to work in primary healthcare institutions and realize their “gate keeping” roles, managing referrals to specialist care in hospitals.9
Private hospitals, which are believed to be indispensable supplements to public hospitals in order to enhance healthcare quality and efficiency across the nation as well as meeting rapidly rising demand of diversified health care, had been expected to present satisfactory participation and development throughout the healthcare reform phase. Policies and strategies forged at governmental level in order to achieve this desired outcome had been focused on the abolishment of some previous regulatory limitations which had posed entry barriers for private hospitals into the healthcare delivery system.10-13 In an attempt to provide a friendlier hospital market for private hospitals, a policy called “guan ban fen kai” (making the operational system within public hospitals administratively independent from the surveillance of governmental regulatory divisions), had also been proposed and implemented in order to mitigate the negative impact of executive committee and stakeholders from public healthcare organizations on private hospitals.14,15
The optimization of hospital market structure in China, as a desired outcome achieved by the healthcare reform, had been on the other hand predicted to intensify the competition between public and private hospitals as well as among different public/private hospitals. Based on the experiences of and lessons learned from multiple countries around the world such as the United States and United Kingdom, in which market mechanism had all been used to induce positive competitions within healthcare markets,16 it had been anticipated that the future hospital market in China would be benefit from the positive competitions among hospitals as the result of an optimized hospital market structure.17,18 The implementation of the “guan ban fen kai” policy, as previously discussed, would very much likely to stimulate the engagement of public hospitals in this competition by giving them more independency in terms of administrative and financial management. The penetration of private hospitals would intensify competition between public and private hospitals, and that within private hospitals.
Based on the expected outcomes as discussed above, this study, therefore, had been designed to evaluate the evolving process of the healthcare market from the 3 aspects. Data collected on national, provincial, and hospital levels from 2009 to 2017 were used in this study in order to investigate the evolving process of hospital market in China after the new round of national healthcare reform in 2009. Health service capacity, hospital market shares and concentration were used as key indicators for assessing the consistency of hospital market change with the desired outcomes. As the traditional Structure Conduct Performance (SCP) model in the field of industrial organization has addressed on the impact of market structure on institutional behavior and performance,19-21 the changing trend of hospital market would also influence hospital performance, which needs to be highlighted as an aspect for constant analysis. As previous literature merely provided scarce evidences on investigating the impacts of healthcare reform in China on its nationwide hospital market since 2009, our study was expected to contribute to relevant literature by demonstrating the evolvement process of nationwide hospital market in China during the study period from a list of novel perspectives including hospital capacity, market share and market concentration. A brief introduction to healthcare delivery system in China was provided in the following section. Statistical analysis and methods used were discussed in section 3 and the outcomes were reported in section 4. Discussion and recommendations based on the study were also provided in the last sections.
Context
In China, a Three Tier Healthcare Delivery System has provided the framework for healthcare delivery across the nation. Specifically, the rural 3 tire system consists of village clinics, Township Health Centers (THCs) and county hospitals, while its counterpart in the urban areas consists of Community Health Centers/Stations (CHCs) and city hospitals, which can be further graded based on different districts.22 Hospitals in China are graded as primary, secondary, and tertiary hospitals with increasing quality based on a list of evaluation criteria including the quality and safety of healthcare delivery, the quality of clinical facilities and hospital management, as well as clinical skills of healthcare professionals and their research abilities. As village clinics are managed by THCs, THCs in rural area and CHCs in urban area are called primary healthcare institutions. Unlike developed countries such as the US and UK, primary healthcare institutions in China are equipped with beds. These primary healthcare institutions have been expected to provide outpatient and inpatient services, medical and public health services at primary care levels, thus mitigating the workload of superior healthcare organizations, namely secondary and tertiary hospitals.
Despite the gatekeeping roles that primary healthcare institutions have been expected to contribute to the society, the lack of a well-developed referral system, however, has laid tremendous hinderance for them for achieving their goals. In sharp contrast with developed countries such as UK and Denmark, where residents have easy access to well-developed primary healthcare institutions, this situation in China has posed immense workload on secondary and tertiary hospitals by allowing a daunting amount of patients to seek medical service in secondary and tertiary hospitals without obtaining referrals from THCs and CHCs in advance. Striving to find a solution for this unneglectable healthcare issue under such adverse circumstances, the enhancement of primary healthcare institutions had been addressed as an essential target throughout the healthcare reform, with a series of strategies proposed targeting at the improvement of healthcare delivery quality and efficiency in primary healthcare institutions through reallocation of medical resources. It had been anticipated that the implementation of those strategies were likely to improve the efficiency of healthcare delivery as well as reducing medical cost for the integrated healthcare system.
Methods
Datasets
The 2009 to 2017 nationwide and provincial-level aggregate data was extracted from China Health Statistical Yearbook 2010 to 2018,23 and was used to evaluate hospitals’ healthcare delivery capacity and medical service, and that based on different hospital ownership types and levels. As the publicly available national dataset provided province as the lowest level of administrative unit, which was considered unreasonable for evaluating the hospital market concentration in China due to its inconsistency with the definition of hospital market, the 2009 to 2017 hospital administrative data retrieved from Sichuan province, was used as a prototype for assessing the hospital market concentration in China. Specifically, the data provided by Health Commission of Sichuan Province served as an ideal resource for evaluating the hospital market concentration within nationwide range as Sichuan Province has a list of similarities with the nation in terms of various aspects including geographic environment, population distribution as well as the distribution of economic development. In addition, Hu Line which runs from Heihe in Heilongjiang Province to Tengchong in Yunnan Province and has been considered as the geographic/demographic demarcation line of the eastern and western parts of China,24-26 has also divided Sichuan into 2 zones by geographic/demographic characteristic: the west (sparsely populated, mountainous with poor economic development) and the east (densely populated, flat with prosperous economic development).Such geographic feature is roughly consistent with the overall situation in China. The provincial administrative data provided county as the lowest level of administrative unit for evaluating the hospital market concentration across the province.
Measurements and Data Analysis
According to the related literature, the total hospital beds and licensed doctors were used to measure the delivery capacity of hospital market,27 the annual outpatient and inpatient visits for the actual services provided, and the 4-firm concentration ratio (CR4) and Herfindahl-Hirschman Index (HHI) for hospital market concentration.21,28-31
CR4 was the combined market share of the 4 largest hospitals in the market and was calculated as:
| (1) |
where m denotes the hospital which is among the 4 largest hospitals in market i. t is the year. Xmit is the medical service provided by hospital m in market i and year t. Xit indicates the total medical service provided by hospitals market i in year t. It shows the extent of market control by the largest hospitals in the hospital market.32
HHI measured market concentration by aggregating the squared volume shares (from each firm) of a market. Higher HHI values represent markets with fewer participants and/or medical uneven volume shares, indicating that the market is more consolidated (less competitive).33 It was calculated as:
| (2) |
where h denotes hospital, N is the total number of hospitals in local market i and year t. Xhit is the medical service provided by hospital h in hospital market i and year t. Xit indicates the total medical service of all hospitals in market i and year t.
All data were analyzed descriptively, and no hypotheses were formulated.
Results
The Overall Hospital Capacity and Service Provided
Since 2009, hospitals’ delivery capacity showed an upward trend. The number of bed and doctor nearly doubled during the sampling years, growing from 3.12 million and 1.09 million in 2009 to 6.12 million and 2.82 million in 2017, respectively (Figure 1a). The average growth rate of bed was higher than that of doctor at 10.68% (0.33 million) per year compared with7.24% (0.08 million) per year. The changing trend is likely to continue in the following years.
Figure 1.

The hospital capacity and service, China, 2009 to 2017.
In order to eliminate the influence of the growing number of hospitals on the results of hospital capacity (see Supplemental Appendix Figure A1a), we further displayed the quantity of bed and doctor each hospital owned, and found a similar evolving process which started at 153.80 and 53.90 in 2009, and reached 197.08 and 57.97 in 2017, respectively (Figure 1b). Taking the growing demand population into consideration, we found that the number of bed and doctor per thousand people also demonstrated a constant rise (see Supplemental Appendix Figure A1b).
With increased capacity, services provided by hospitals also increased during the sample years, with an annual growth rate of 8.77% (189.63 million per year) for outpatient visits and 13.65% (13 034 thousand per year) for inpatient visits. In 2017, the total number of outpatient and inpatient service hospital provided reached 3438.92 million and 1891.54 million, respectively (Figure 1c). The average number of service hospital provided was also rising, in spite of some fluctuation.
Additionally, we compared the delivery capacity and service of hospitals with that of primary healthcare institutions. As shown in Figure 2a, in China’s healthcare delivery system, more than half of beds and doctors gathered in hospitals, and the share of beds and doctors. hospital owned was ever-rising. By 2017, hospitals owned 80.02% beds and 68.77% doctors. During the sample years, the growth in hospital capacity was found to be 7 times ((6.12−3.12)/((6.12/80.02%−6.12)−(3.12/73.94%−3.12))) faster than that of primary care institutions in terms of beds, and was found to be 4 times ((1.80−1.09)/((1.80/68.77%−1.80)−(1.09/63.04%−1.09))) faster in terms of the increase of doctors. Meanwhile, the percentages of service supplied by hospitals which were 36.17% and 67.37% in 2009, increased to 43.71% and 80.95% by 2017, implying that an increased proportion of patients were attracted to hospitals (Figure 2b).
Figure 2.
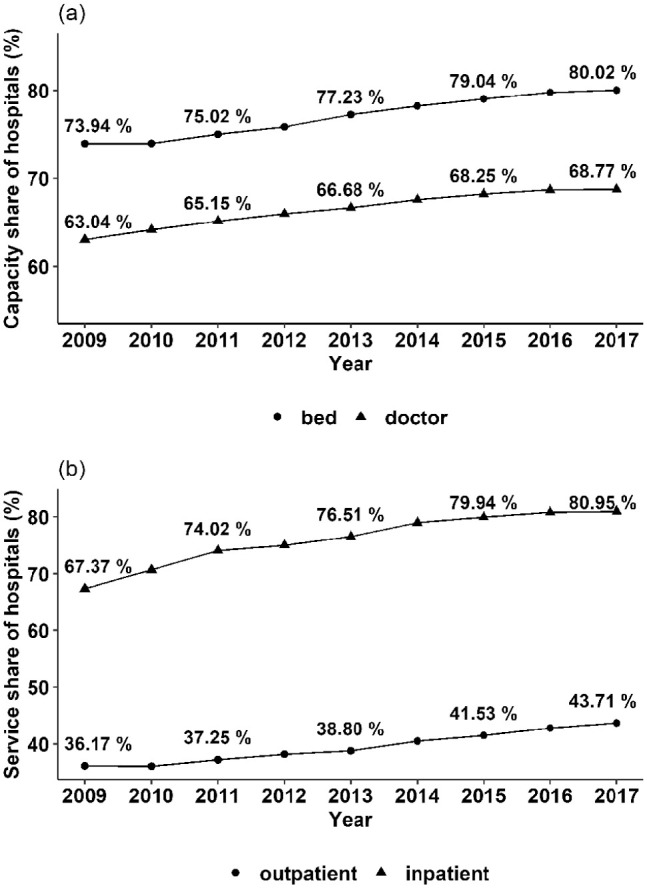
Capacity and service share owned by hospitals in the whole healthcare system, China, 2009 to 2017.
Hospital Capacity and Service by Levels, Ownership
Figure 3 illustrated hospital capacity and service by levels during the sampling years. Tertiary hospital possessed an increasing share of beds and doctors, while that occupied by secondary hospitals were declining (Figure 3a and 3b). The relative delivery capacities of unassigned and primary hospitals were small and had hardly changed in the past 9 years. Specifically, in 2017, tertiary, secondary, primary and unassigned hospitals owned 38.56%, 40.04%, 9.56%, and 11.84% of beds, 47.65%, 37.75%, 6.94%, and 7.66% of doctors, respectively. The changing pattern for share of hospital medical service by levels was found to be similar with that for share of hospital capacity by levels, and tertiary, secondary, primary, and unassigned hospitals offered 50.20%, 36.87%, 6.46%, and 6.47% outpatient service, and 44.39%, 42.32%, 6.18%, and 7.11% inpatient service in 2017, respectively (Figure 3c and 3d). This indicated that tertiary hospital owned more medical resources, while supplied more service. However, a constantly existed asymmetry between the hospital capacity and hospital service was found for tertiary hospitals, since the proportion of hospital resources they possessed was not equal to the proportion of hospital service they provided.
Figure 3.

Hospital capacity and service by levels, China, 2009 to 2017.
Note. The number of doctors by hospital levels in 2009 was not available.
Figure 4a described the share of delivery capacity and service private hospitals owned. After the nationwide healthcare reform, the number of private hospitals increased dramatically, which ultimately exceeded the number of public hospitals with growing proportion of medical resources in the hospital market (see Supplemental Appendix Figure A1). The share of bed and doctor were 24.33% and 17.24% in 2017, compared with merely 11.03% and 9.22% in 2010, respectively. Meanwhile, the proportion of medical service supplied by private hospital was also growing over time. During 2009 to 2017, the proportion of outpatient and inpatient service private hospital provided accounted for 7.69% and 7.99% in 2017, compared with 14.16% and 17.56%, respectively in 2009. It is not difficult to conclude that the evolving process of the percentage of service private hospitals provided is similar to that of proportion of doctors they have.
Figure 4.
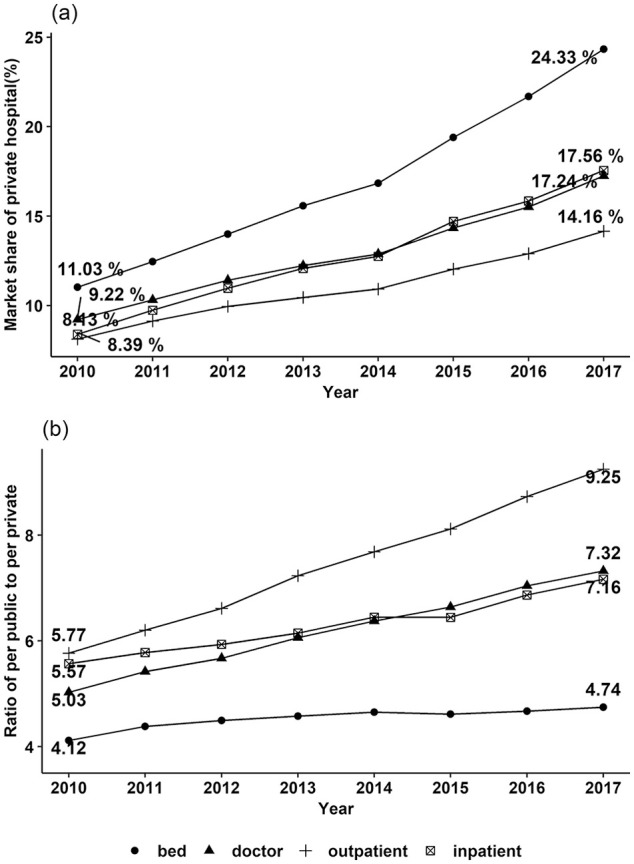
Hospital capacity and service by ownership types, China, 2010 to 2017.
Note. The number of doctors by ownership in 2009 was not available, hence the line graph only showed data from 2010 to 2017. Subfigure (b) illustrated the ratio of the delivery capacity and service per public hospital owned to that of per private hospital owned respectively.
There was an upward trend in the average delivery capacity of both public and private hospital (see Supplemental Appendix Figure A2). However, compared with public hospitals, the average delivery capacity for private hospital was still very small, and the average delivery capacity gap between different ownerships was expected to widen in the next few years. Illustrated by Figure 4b, the number of beds and doctors per public hospital were 4.12 times and 5.03 times of those per private hospital respectively in 2010, which raised up to 4.74 times and 7.16 times in 2017. In other words, the quantity gap of doctor between public and private hospitals was much larger than that gap of bed between the 2 ownership types. Correspondingly, the total number of service each private hospital supplied was found to be smaller than that provided by each public hospital. Moreover, the evolving averaged service gap between the 2 ownership types was similar to the evolving averaged number of doctors owned by both ownership types.
Hospital Market Concentration
During the past 9 years, an increased number of new hospitals entered hospital markets in China. Averagely, there were 350 new hospitals per province (the amount of hospital grew from 654.55 hospitals per province to 1001.81) and 3 per county (the amount of hospital rose from 7.12 hospitals per county to 10.89) (see Table 1). With the increase of competitors in each hospital market, the market competition was expected to be constantly intensified.
Table 1.
The Average Number of Hospitals in Each Province and County, China, 2009 to 2017.
| Year | Number of hospitals | |
|---|---|---|
| Per province | Per county | |
| 2009 | 654.55 | 7.12 |
| 2010 | 674.77 | 7.34 |
| 2011 | 709.00 | 7.71 |
| 2012 | 747.42 | 8.13 |
| 2013 | 797.06 | 8.67 |
| 2014 | 834.19 | 9.07 |
| 2015 | 889.90 | 9.68 |
| 2016 | 940.00 | 10.22 |
| 2017 | 1001.81 | 10.89 |
Figure 5 showed the CR4 for hospital markets in Sichuan province during 2009 to 2017. The CR4 for both outpatient and inpatient service were decreasing, which change from 84.64% (95% CI: 83.89%-85.40%) to 82.21% (95% CI: 81.73%-82.69%) for outpatient service and 85.76% (95% CI: 85.04%-86.49%) to 76.52% (95% CI: 75.96%-77.07%) for inpatient service implying a less concentrated hospital market. As CR4 represents the market share of the 4 largest hospitals in each market, the downward trend suggests that large hospitals are also confronted with more intensive hospital competition, and their market advantage is weakening.
Figure 5.
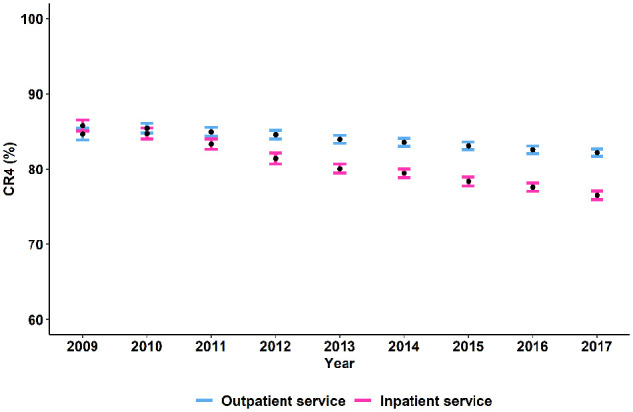
Four-firm concentration ratio (CR4) for hospital markets in Sichuan, China, 2009 to 2017.
Note. Point estimates of CR4 with 95% confidence interval were presented in this figure.
Figure 6 illustrated the HHI for outpatient (Figure 6a) and inpatient service (Figure 6b). Similar with what showed in Figure 5, the hospital market competition for both outpatient service and inpatient service were increasing over time, and the HHI for outpatient service were averagely higher than that for inpatient service, suggesting that hospital competition was more intense in inpatient service market. Specifically, HHI for outpatient and inpatient service decreased from 0.35 (95% CI: 0.34-0.36) and 0.40 (95% CI: 0.39-0.41) in 2009 to 0.31 (95% CI: 0.30-0.32) and 0.26 (95% CI: 0.25-0.27) in 2017, respectively.
Figure 6.
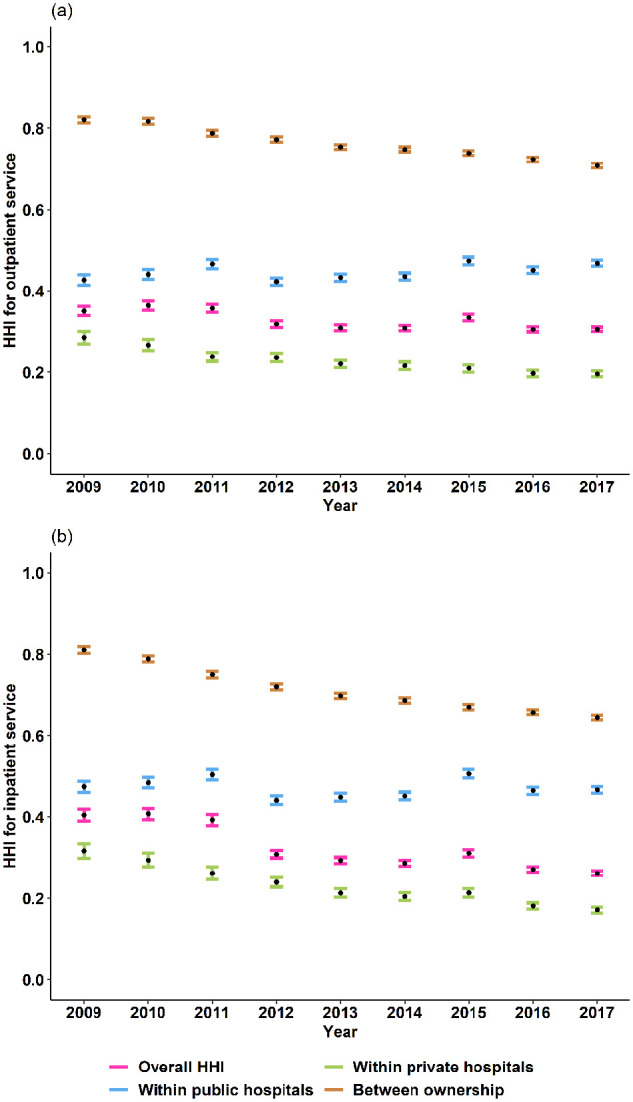
Herfindahl-Hirschman Index (HHI) for hospital markets in Sichuan, China, 2009 to 2017.
Note. Point estimates of HHI with 95% confidence interval were presented in this picture. When calculating HHI within public (private) hospitals, we just included public (private) hospitals and ignored private (public) hospitals; when calculated HHI between ownership, we regarded all the private or public hospitals in the seam hospital market as a whole.
As the Chinese healthcare market has long been a mixed ownership system since 1980s, we further decomposed HHI by ownership types, to explore how hospital competition changed between ownership types (public and private) and within public or private hospitals. We found that hospital market competition mainly existed within public and private hospitals, since the HHI between ownerships was higher than that within public and private hospitals for both outpatient and inpatient service. Besides, during 2009 to 2017, HHI between ownerships and that within private hospitals were ever-decreasing, which decreased from 0.82 (95% CI: 0.81-0.83) and 0.29 (95% CI: 0.27-0.30) to 0.71 (95% CI: 0.81-0.83) and 0.20 (95%CI: 0.19-0.20) for outpatient service, and from 0.81 (95% CI: 0.80-0.82) and 0.32 (95% CI: 0.30-0.33) to 0.64 (95% CI: 0.63-0.65) and 0.17 (95% CI: 0.16-0.18) for inpatient service, respectively. However, the HHI within public hospital fluctuated in the sample years, and changed slightly.
Discussion
China’s new healthcare reform initiated in 2009 has stimulated rapid development of nationwide hospital market in terms of supply capacity and deliveries, with increasing market competition. However, hospital market in China was still dominated by the public and tertiary hospitals, the promotion of healthcare at primary levels should be emphasized as an essential strategy during future policy-making procedures. Instructions regarding to the development of private hospitals should also be provided at governmental levels in order to achieve the optimization of nationwide hospital market via constant promotion of orderly competition performances among various hospitals.
Healthcare Capacity and Deliveries
This study found that, after 2009, Chinese patients’ demand for medical service increased greatly, which might have resulted from the fact that the development of economy and the expanded range of social insurance coverage had alleviated patients’ financial burden,34 thus making medical service gained from healthcare institutions affordable for Chinese residents. However, over the past decade, outpatient and inpatient services offered by hospitals both demonstrated up-going tendencies, which increased to 43.71% and 80.95% in 2017, respectively. In addition, about half of all hospital services were provided by tertiary hospitals which owned the most advanced clinical skills and supplied high-tech medical service22 and thus had been expected to merely offer service for patients with complex and intractable disease that cannot be treated in primary healthcare institutions or inferior hospitals (primary or secondary hospitals). This indicated that primary healthcare institutions still did not achieve their gatekeeping roles after the healthcare reform. The factors leading to such undesirable circumstances can be analyzed both from suppliers’ and demanders’ perspectives in healthcare market.
In China, hospitals tend to have more motivation for providing healthcare for patients as they have been given financial autonomy and therefore have discretionary power for disposing their revenues. The fee-for-service reimbursement method in China is considered as another factor that stimulates hospital owners’ motivation for increasing the quantity of medical care.35 In sharp contrast with hospitals, primary healthcare institutions are state owned and are required to provide cheap basic healthcare service at the sacrifice of their own benefits,36 thus lacking the motivation for attracting patients for health care. From demanders’ perspective, primary healthcare institutions have relatively untrustworthy reputations for their health care quality among patients compared with hospitals. Compromised by the lack of a well-developed referral system in China, this enabled a daunting number of patients to seek health care at hospitals without obtaining referrals from primary healthcare institutions in advance. As the result, most of Chinese residents tend to visit tertiary hospitals for even easily treatable diseases, which has posed immense workload on tertiary hospitals.
Despite the fact that the promotion of primary healthcare systems has been addressed as an urgent task for healthcare system in China, most of the resources were still allocated to hospitals after the national healthcare reform, which is opposite to the situation in most Organization for Economic and Cooperation and Development (OECD) countries. During the past few years, the number of hospital beds per 1000 residents owned declined in most OECD countries such as the UK, Denmark, Finland, the Netherlands, and Spain where well-developed primary healthcare systems had been established (see Supplemental Appendix Figure A3). In contrast, such index was found to demonstrate a rising tendency in China, which is similar to Korea where primary healthcare system was still in an undeveloped stage.37,38
A well-developed primary healthcare system has been addressed as the key to promoting population health, reducing medical cost as well as improving residents’ overall satisfaction towards the holistic healthcare delivery system.39,40 As the result, an increased amount of medical resources, especially well-trained healthcare professionals, should be allocated at primary healthcare levels in order to improve China’s nationwide primary healthcare system via the adoption of policy-making strategies as well as ensuring residents’ basic needs for health care can be met in primary healthcare institutions. However, in China, low compensation has been the main obstacle for attracting well-trained healthcare professionals to work in primary healthcare institutions. Under such circumstances, medical alliance could be proposed as an effective strategy for improving service capacity of primary healthcare institutions, which enables tertiary hospitals or county hospitals to become the leaders of unions while their inferior institutions as members. Primary healthcare institutions are very much likely to substantially benefit from the medical resources, technique support and professional training programs provided by the leading hospitals, thus improving the healthcare quality for patients with common diseases. It is predictable that via the adoption of medical alliance, primary healthcare institutions are expected to obtain a good reputation for enhanced healthcare quality thus becoming more trustworthy and attractive to patients.
Development of Private Hospitals
Boosted by governmental strategies, private hospitals achieved prosperous development over the past few years with their quantity exceeding the total number of public hospitals. Previous studies also showed that the share of private hospital’s quantity in the nationwide hospital market surpassed that in many OECD countries.41 This study found that both the delivery capacity and delivered service of private hospitals have increased after the national healthcare reform, while the averaged delivery capacity of private hospitals remained much lower than that of public hospitals. These findings suggested that future policies and strategies forged at governmental levels should be switched from merely increasing the number of private hospitals to improving their service capacity and quality.
In addition, we also found that the medical resource gap between private and public hospitals mainly resided in human resources, while the evolving tendency of human resource gap proved to be consistent with that of the medical service gap. This phenomenon indicated that the lack of human resources, especially well-trained medical experts, might be the leading factor that restricted private hospitals from improving their quantity and quality of health care. Therefore, it is highly recommended that the future promotion strategies for private hospitals should be emphasized on the recruitment of medical professionals instead of accumulating material resources aimlessly. However, this can hardly be achieved as healthcare workers, especially new and experienced medical workers in China tend to choose public hospitals as their ideal workplace which can provide them stable positions by giving them job guarantees. As the result, multiple ways should be adopted by private hospitals in the process of recruiting healthcare professionals. Apart from several currently existing strategies such as improving the compensation for medical staffs and comfortableness of work environment, incentives for stimulating health professionals’ motivation for working in private hospitals might also include the provision of future study opportunities such as professional training programs in tertiary hospitals and even in overseas hospitals if possible. As the well-trained healthcare workers are rare, encouraging professionals from public hospitals to work part-time in private hospitals could also be a solution for labor shortage and undesirable health care quality in private hospitals.
Hospital Competition
An increasingly intensified hospital market competition was found in our study in the past decade, which was opposite to that in the US.28,42 In 2017, the competition level in China was even more intense than that in the US, with an HHI of 0.26 as measured by inpatient services, compared with 0.58 in the US.43 During the study period, competition within public hospitals changed very little, while competition within private hospitals and the overall degree of competition in hospital market increased dramatically. It can be concluded that the increased amount of private hospitals had induced the reduction of hospital market concentration in China over the past decade. However, the immense capacity and service gap had made it extremely difficult for private hospitals to compete with public hospitals. The competitions among various hospitals was found to be mainly exist among hospitals of homogeneous ownership types while the competition between private and public hospitals was found to be much less intensive. In addition, hospital competition among private hospitals was found to be more intensive than that among public hospitals, which was similar with the situation in Australia where HHI of public hospitals was 0.57 and 0.40 of private hospitals.44 A constantly intensified trend of hospital competition in China is very much likely to be seen as a trend in the future.
From demanders’ perspective, the decreased market concentration over the past decade indicates that the nationwide healthcare issue “kan bing nan” (obtaining access to medical service is difficult) has been partly alleviated as the distribution of patients became more even in the hospital market. In other words, patients became more likely to seek medical service from various hospitals instead of gathering in several specific hospitals, despite that most of residents in China still tend to seek medical service from tertiary hospitals. As the economic development in China has entered a new phase with a relatively stable development pace, it is not unreasonable to predict that the growth rate of Chinese residents’ income will slow down. Consequently, Chinese residents’ investment and consumption capacity for medical service will likely to be stable. Meanwhile, the implementation of the universal health coverage (UHC) strategy in China has substantially alleviated the financial burden imposed by unaffordable medical cost for Chinese residents,34 thus essentially reducing the amount of unmet medical demands in China. As the result of combined factors, the growth rate of medical demand obtained from hospitals will very much likely to slow down in the new development phase. The constant medical demand in China is expected to stimulate the intensification of hospital competition among various suppliers.
However, whether hospital competitions will bring about positive impact on health care delivery remains a worldwide controversy. While multiple studies indicated that intensified hospital competition would improve hospital quality,16,21,45 reduce medical expense46 as well as promoting the overall hospital performance,47 some other studies presented mixed outcomes48 or even opposite results.43,49-51 Under such circumstances, the constantly intensified hospital competitions in a nationwide range has made it a critical need to encourage well-managed and orderly competition performances among hospitals via the adoption of policies and strategies forged at governmental levels in order to facilitate quality-based competitions among healthcare organizations as well as avoiding malicious competitions.
While the adoption of market mechanism has been proposed to facilitate the promotion of health care quality, to date no guidelines for achieving orderly competition in China has been published accordingly. As the result, how to make how to guide hospital competition beneficial for promotion of health care delivery remains an urgent issue that needs to be solved. In China, it has been concerned that the information asymmetry in healthcare system might be the leading cause of market failure,52 which implies that most of the patients are not able to evaluate the quality of health care due to their insufficient medical knowledge compared with healthcare providers. As a strategy for reducing information asymmetry in the healthcare market, the establishment of a reliable auditing system is therefore highly recommended which provides access to patients for obtaining real-time and comprehensive information about healthcare quality and efficiency in hospitals prior to their visits.
Limitations
Several limitations should be noted in this study. First, as our study merely described the evolving process of China’s hospital market in the past decade which failed to further investigate the impacts of these changes on the quality of healthcare in China, it is highly recommended that the evaluation of this aspect be addressed in future studies. Another limitation inherent in this study was that hospital administrative data in Sichuan province was adopted as a prototype in the process of accessing hospital market concentration via the evaluation of HHI and CR4. However, it should be noted that hospital markets would differ among different regions in China due to large disparity in terms of both geographical features and socioeconomic development status. As the result, our findings based on the adoption of CR4 and HHI in Sichuan province should only be considered as indicative of the situation in western China instead of representing the whole nationwide situation due to data availability issues. Scholars and policy makers should be cautious when citing our results.
Supplemental Material
Supplemental material, Appendix_0826 for The Evolving Hospital Market in China After the 2009 Healthcare Reform by Qingling Jiang and Jay Pan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding: The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was founded by National Natural Science Foundation of China (grant no. 71874116 and 72074163), Ministry of Education of China (grant no. 18YJA790062), Sichuan Science and Technology Program (grant no. 2019JDR0159), Chengdu Federation of Social Science Association (grant no. ZZ05), Sichuan University (grant no. 2018hhf-27 and SKSYL201811), and China Medical Board (grant no. 17-276).
ORCID iD: Jay Pan  https://orcid.org/0000-0001-9501-1535
https://orcid.org/0000-0001-9501-1535
Supplemental Material: Supplemental material for this article is available online.
References
- 1. State Council. The performance direction of the health care reform of the programs from 2009 to 2011 (in Chinese). State Council. http://www.gov.cn/test/2009-04/08/content_1280057.htm. Accessed October 13, 2019.
- 2. State Council. The state council issued a notice on the work arrangements for the five major reforms of the medical and health care system in 2009. State Council. http://www.gov.cn/zhengce/content/2009-07/23/content_6221.htm. Accessed August 31, 2019.
- 3. State Council. Opinions of the state council on establishing and improving the compensation mechanism for primary health care institutions. State Council. http://www.gov.cn/zhengce/content/2010-12/14/content_6178.htm. Accessed December 1, 2019.
- 4. Liu X, Wang Q, Sara B, Yang W, Dong S, Li H. The technical efficiency of community health service centers in Wuhan, China: estimation and policy implications. Inquiry: J Health Care Org Provis Financ. 2018;55:0046958018812972. [Google Scholar]
- 5. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in Universal Health Coverage. Lancet. 2019;394(10204):1192-1204. [DOI] [PubMed] [Google Scholar]
- 6. State Council. Notice of the general office of the state council on issuing the 2011 pilot reform of public hospitals. State Council. http://www.gov.cn/zhengce/content/2011-03/07/content_6131.htm. Accessed August 31, 2019.
- 7. State Development and Reform Commission. Notice on the preparation of the proposed plan for the central investment plan for the health sector in 2019. State Development and Reform Commission. http://www.gov.cn/xinwen/2018-10/26/content_5334626.htm. Accessed August 31, 2019.
- 8. State Council. Guiding opinions of the general office of the state council on promoting the construction of a hierarchical diagnosis and treatment system. State Council. http://www.gov.cn/zhengce/content/2015-09/11/content_10158.htm. Accessed September 22, 2019.
- 9. State Council. Guidelines of the state council on the establishment of a system of general practitioners. State Council. http://www.gov.cn/zhengce/content/2011-07/06/content_6123.htm. Accessed December 1, 2019.
- 10. Chen Z, Barros CP, Hou X. Has the medical reform improved the cost efficiency of Chinese hospitals? Soc Sci J. 2016; 53(4):510-520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. State Council. Several opinions of the state council on promoting the development of health service industry. State Council. http://www.gov.cn/zhengce/content/2013-10/18/content_6067.htm. Accessed August 31, 2019.
- 12. The State Council Information Office. The white paper of “Development rights: China’s concept, practice and contribution”. The State Council Information Office. http://www.scio.gov.cn/zfbps/32832/Document/1532315/1532315_1.htm. Accessed May 21, 2017.
- 13. State Council. Notice of the general office of the state council on issuing the last half of 2018 major task list on deepening the medical and health care system reform. State Council. http://www.gov.cn/zhengce/content/2018-08/28/content_5317165.htm. Accessed August 31, 2019.
- 14. Ministry of Health, National Development and Reform Commission, Ministry of Finance, Ministry of Commerce, Human Resources and Social Security Department. Ministry of Health. Guidance on pilot project of public hospital reform; http://www.china.com.cn/policy/txt/2010-02/24/content_19464497.htm. Accessed May 21, 2017. [Google Scholar]
- 15. Pan J, Liu GG, Gao C. How does separating government regulatory and operational control of public hospitals matter to healthcare supply? China Econ Rev. 2013;27:1-14. [Google Scholar]
- 16. Cooper Z, Gibbons S, Jones S, Mcguire A. Does hospital competition save lives? Evidence from the English NHS patient choice reforms. Econ J. 2011;121(554):F228-F260. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. State Council. Opinions of the CPC Central Committee and the State Council on deepening the health care system reform. State Council. http://www.gov.cn/jrzg/2009-04/06/content_1278721.htm. Accessed August 31, 2019.
- 18. Allen P, Cao Q, Wang H. Public hospital autonomy in China in an international context. Int J Health Plann Manag. 2014;29(2):141-159. [DOI] [PubMed] [Google Scholar]
- 19. Andreosso O’Callaghan B, Jacobson D. Industrial Economics & Organization: A European Perspective. Beijing: Economic Science Press; 2009. [Google Scholar]
- 20. Kenneth WC. Industrial Organization: Theory, Evidence and Public Policy. Beijing: Sanlian Bookstore; 1989. [Google Scholar]
- 21. Pan J, Qin X, Li Q, Messina JP, Delamater PL. Does hospital competition improve health care delivery in China? China Econ Rev. 2015;33:179-199. [Google Scholar]
- 22. Wang X, Yang H, Duan Z, Pan J. Spatial accessibility of primary health care in China: a case study in Sichuan Province. Soc Sci Med. 2018;209:S0277953618302582. [DOI] [PubMed] [Google Scholar]
- 23. Zhang X, Zhou G, Liu W, Yu S. China health statistical yearbook. In: National Health Commission, ed. Statistical Database on China’s Economic and Social Development. 2010-2018 ed. Beijing: Peking Union Medical College Press; 2019. http://tongji.cnki.net/kns55/Navi/HomePage.aspx?id=N2019030282&name=YSIFE&floor=1. Accessed August 31, 2019. [Google Scholar]
- 24. Huanyong H. The distribution, regionalization and prospect of Chinese population (in Chinese). Acta Geogr Sin. 1990;45(2):139-145. [PubMed] [Google Scholar]
- 25. Huanyong H. Population distribution in China with statistical tables and density maps (in Chinese). Acta Geogr Sin. 1935; 2:33-74. [Google Scholar]
- 26. Hu Z, Wang Y, Liu Y, Long H, Jian P. Spatio-temporal patterns of urban-rural development and transformation in east of the “Hu Huanyong Line”, China. Int J Geo-Inform. 2016;5(3):24. [Google Scholar]
- 27. Wang X, Pan J. Assessing the disparity in spatial access to hospital care in ethnic minority region in Sichuan Province, China. BMC Health Serv Res. 2016;16(1):399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Gaynor M, Town RJ. Chapter nine – Competition in health care markets. In: Pauly MV, McGuire TG, Barros PP, eds. Handbook of Health Economics. Vol. 2 Amsterdam: Elsevier; 2011:138. [Google Scholar]
- 29. Luo Y, Pan J. Competition and hospital efficiency: an empirical study based on panel data. Work paper, 2016. [Google Scholar]
- 30. Lamm RM. Prices and concentration in the food retailing industry. J Ind Econ. 1981;30(1):67-78. [Google Scholar]
- 31. Shaik S, Allen AJ, Edwards S, Harris J. Market structure conduct performance hypothesis revisited using stochastic frontier efficiency analysis. J Transport Res Forum. 2009;48:24. [Google Scholar]
- 32. Delorme CD, Jr, Kamerschen DR, Klein PG, Voeks LF. Structure, conduct and performance: a simultaneous equations approach. Appl Econ. 2002;34(17):2135-2141. [Google Scholar]
- 33. Cerullo M, Chen SY, Dillhoff M, Schmidt C, Canner JK, Pawlik TM. Association of hospital market concentration with costs of complex hepatopancreaticobiliary surgery. J Am Med Assoc Surg. 2017;152(9):e172158. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34. Li K. Deepen health care reform continuously and promote the establishment of the health care system that suits China’s national conditions and benefits all people. http://www.gov.cn/ldhd/2011-11/17/content_1995480.htm. Accessed October 13, 2019.
- 35. Zhao C, Wang C, Shen C, Wang Q. Diagnosis-related group (DRG)-based case-mix funding system, a promising alternative for fee for service payment in China. Biosci Trends. 2018;12(2):109-115. [DOI] [PubMed] [Google Scholar]
- 36. Yip WC-M, Hsiao WC, Chen W, Hu S, Ma J, Maynard A. Early appraisal of China’s huge and complex health-care reforms. Lancet. 2012;379(9818):833-842. [DOI] [PubMed] [Google Scholar]
- 37. Sung NJ, Suh S-Y, Lee DW, Ahn H-Y, Choi Y-J, Lee JH. Patient’s assessment of primary care of medical institutions in South Korea by structural type. Int J Qual Health Care. 22(6):493-499. [DOI] [PubMed] [Google Scholar]
- 38. Aoki T, Inoue M, Nakayama T. Development and validation of the Japanese version of Primary Care Assessment Tool. Family Pract. 2015;33(1):112-117. [DOI] [PubMed] [Google Scholar]
- 39. Shi L. Primary care, specialty care, and life chances. Int J Health Serv Plann Admin Eval. 1994;24(3):431-458. [DOI] [PubMed] [Google Scholar]
- 40. Starfield B. Is primary care essential? Lancet 1994;344(8930): 1129-1133. [DOI] [PubMed] [Google Scholar]
- 41. Deng C, Li X, Pan J. Private hospital expansion in China: a global perspective. Global Health J. 2018;2(2):33-46. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Johnson G, Frakt A. Hospital markets in the United States, 2007–2017. Healthcare. 2020;8(3):100445. [DOI] [PubMed] [Google Scholar]
- 43. Gautam G, Town RJ. Competition, payers, and hospital quality. Health Serv Res. 2010;38(6 pt 1):1403-1422. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Palangkaraya A, Yong J. Effects of competition on hospital quality: an examination using hospital administrative data. Eur J Health Econ Hepac Health Econ Prevent Care. 2013; 14(3):415-429. [DOI] [PubMed] [Google Scholar]
- 45. Leleu H, Al-Amin M, Rosko M, Valdmanis VG. A robust analysis of hospital efficiency and factors affecting variability. Health Serv Manag Res. 2018;31(1):33-42. [DOI] [PubMed] [Google Scholar]
- 46. Lu L, Pan J. The association of hospital competition with inpatient costs of stroke: evidence from China. Soc Sci Med. 2019;230:234-245. [DOI] [PubMed] [Google Scholar]
- 47. Hu H, Qi Q, Yang C. Analysis of hospital technical efficiency in China: effect of health insurance reform. China Econ Rev. 2012;23(4):865-877. [Google Scholar]
- 48. Longo F, Siciliani L, Moscelli G, Gravelle H. Does hospital competition improve efficiency? The effect of the patient choice reform in England. Working papers, 2017. [DOI] [PubMed]
- 49. Shortell SM, Hughes EF. The effects of regulation, competition, and ownership on mortality rates among hospital inpatients. New Engl J Med. 1988;319(20):1354. [DOI] [PubMed] [Google Scholar]
- 50. Propper C, Gossage D. Competition and quality: evidence from the NHS internal market 1991-9. Econ J. 2010;118(525):138-170. [Google Scholar]
- 51. Mukamel DB, Zwanziger J, Tomaszewski KJ. HMO penetration, competition, and risk-adjusted hospital mortality. Health Serv Res. 2001;36(6 pt 1):1019-1035. [PMC free article] [PubMed] [Google Scholar]
- 52. Deng C, Pan J. Hospital competition and the expenses for treatments of acute and non-acute common diseases: evidence from China. BMC Health Serv Res. 2019;19(1):739. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supplemental material, Appendix_0826 for The Evolving Hospital Market in China After the 2009 Healthcare Reform by Qingling Jiang and Jay Pan in INQUIRY: The Journal of Health Care Organization, Provision, and Financing