

Abstract
Long-term exposures to the stress and stimulation of different work, parenting, and partnership combinations might influence later life cognition. We investigated the relationship between women’s work-family life histories and cognitive functioning in later life. Analyses were based on data from women born between 1930 and 1957 in 14 European countries, from the Survey of Health, Ageing and Retirement in Europe (2004–2009) (n = 11,908). Multichannel sequence analysis identified 5 distinct work-family typologies based on women’s work, partnership, and childrearing statuses between ages 12 and 50 years. Multilevel regressions were used to test the association between work-family histories and later-life cognition. Partnered mothers who mainly worked part-time had the best cognitive function in later life, scoring approximately 0.63 (95% confidence interval (CI): 0.18, 1.07) points higher than mothers who worked full-time on a 19-point scale. Partnered mothers who were mainly unpaid caregivers or who did other unpaid activities had cognitive scores that were 1.19 (95% CI: 0.49, 1.89) and 0.93 (95% CI: 0.20, 1.66) points lower than full-time working mothers. The findings are robust to adjustment for childhood advantage and educational credentials. This study provides new evidence that long-term exposures to certain social role combinations after childhood and schooling are linked to later-life cognition.
Keywords: cognition, life course, sequence analysis, work-family balance
Abbreviations
- AME
average marginal effect
- CI
confidence interval
- SHARE
Survey of Health, Ageing and Retirement in Europe
Recent decades have seen dramatic changes in work and family life courses, especially among women. Paid work is increasingly normative for women, and a formerly widespread pattern of working for pay until marrying and having children has become just one of many diverse work and family trajectories. Across Europe, female labor-force participation increased by approximately 10–20 percentage points over the course of 1970–2010, and marked variation emerged in schedules (full- vs. part-time) (1). Since the 1960s, a growing fraction of women have not married or raised children, further increasing heterogeneity in work-family histories (2).
Diverging life-course work-family histories contribute to variation in women’s health. Researchers have debated whether combining work and family responsibilities threatens health, due to the strain involved in juggling these demanding roles, or promotes it, given that parenting, work, and marriage have individually been linked to better health (3–5). Combining paid work with marriage and childrearing has been linked to lower risks of mortality (3, 6), cardiovascular problems (7), and later-life frailty (8), although psychosocial impacts might be contingent on the type of work (full- vs. part-time or professional vs. blue-collar) (4, 9). However, while work and family role combinations might provide physical health benefits, they could also be linked to psychosocial strain. Here we extend research on the link between work-family role combinations and health by studying cognitive health, shown to be harmed by long-term exposure to stress (10–12) but benefitted by long-term exposure to cognitive stimulation (13, 14), 2 key features of work-family role combinations. Cognitive capacity develops over the life course and thus is best studied as a product of long-term exposure to certain contexts, such as work and family experiences (15).
Complex work tasks or stimulating work environments (14, 16, 17) and social engagement (16, 18, 19) have been linked with delayed onset of cognitive decline, although we know that some jobs and work-life role combinations are very stressful (4, 20). Marriage might be beneficial (21); researchers hypothesize that social stimulation, even from marital conflict, might be associated with better cognitive health (21, 22). There is scarce research on the topic, but raising children plausibly could provide cognitive stimulation through intensive social interaction; it might also be stressful. Caring for other dependents, particularly when caregivers become socially isolated and less stimulated, could be riskier, and has been linked to higher stress and poorer physical health (23). Thus, the evolving and diverging compositions of women’s days, including their differential exposure to work lives and social relationships, could be linked with varying cognitive health in later life. Past research suggests that stimulating environments and relationships might predict better cognitive functioning in later life.
Because cognition is shaped by long-term exposures, it is important to analyze the accumulation of work-family role experiences across the life course, instead of considering a single point in time, as much past research has done. One recent study of US adults found that longer durations of stimulating paid work were associated with better cognitive health (17). Similar to that study, we used sequence analysis to capture the long-term ordering, duration, and volatility of work histories from ages 12–50 years, but we go beyond, by mapping co-occurring partnership and parenting experiences that further differentiate European women’s lives. Because family life could be a key site of social stimulation, family trajectories, in addition to work trajectories, could importantly shape cognition.
We assessed whether distinctive combinations of long-term exposure to key social roles were associated with cognitive functioning in later life for a contemporary cohort of aging European women. Building on past research, we captured more heterogeneity in role combinations by distinguishing between part- and full-time work and exploring variation in time spent outside the formal labor market in unpaid caregiving versus other activities. We also considered the parenting and partnership experiences interwoven with decisions about work, another novel contribution. We hypothesized that women who combined paid work with partnership and parenting would have better cognitive functioning in later life, and we expected that greater total exposure, via full-time work and/or a longer duration of employment, would be associated with better cognitive function. We hypothesized that spending long periods performing unpaid caregiving work would not afford the same benefits as working for pay and might be associated with poorer cognitive function than being out of the paid labor force for other reasons.
METHODS
Data
This study used nationally representative data from the Survey of Health, Ageing and Retirement in Europe (SHARE), a panel study of adults aged 50 years or older from 27 European countries and Israel (24). Wave 1 was fielded in 2004 and wave 2 in 2006–2007. Wave 3, called SHARELIFE and fielded in 2008–2009, asked respondents to recount their life histories, including partner, parenting, and job histories. We studied respondents born after 1930, the cohorts that experienced the most variation in work and family life histories. We used pooled data from the 14 countries that participated in SHARELIFE (Austria, Belgium, Czech Republic, Denmark, France, Germany, Greece, Ireland, Italy, Netherlands, Poland, Spain, Sweden, and Switzerland) to reconstruct work-family histories for each respondent, the key independent variable. We used information from waves 1 and 2 for other covariates and cognitive function. Data from SHARELIFE and variables drawn from waves 1 or 2 were available for 11,908 respondents.
Measures
The dependent variable, capturing cognitive function, was from a SHARE-adapted scale based on DemTect and the Mini-Mental State Examination (25–29). The measure, ranging from 0–19, combines scaled responses to 5 items: delayed word recall (0–4), immediate word recall (0–4), verbal fluency (0–3), numeracy (0–4), and orientation (0–4). Higher scores indicate better cognitive functioning. If the respondent responded to the wave 2 interview, we used their cognitive and covariate data from wave 2, otherwise we used cognitive and covariate data from wave 1.
We used wave-3 retrospective accounts of work and family status at each age to construct work-family history types. Because the work-family history types incorporated so many indicators, we adjusted for only a small set of additional covariates: year of age (centered at the mean of 62) and a quadratic term for age, given research showing a curvilinear relationship between age and cognitive function (30).
To assess alternative explanations for an association between work-family history type and cognitive function, we further adjusted for potential confounders: 1) level of socioeconomic advantage at age 10 years, and 2) highest educational degree (see Web Appendix, available at https://academic.oup.com/aje, for measure details). In additional analyses (not shown), adjustment for potential mediators—wealth, current employment, and current physical disabilities—did not substantively alter our conclusions.
Work-family histories
To construct work-family life histories, we conducted sequence analysis based on retrospective accounts from SHARELIFE and the SHARE project–generated Job Episodes Panel, which supplemented SHARELIFE with prospectively gathered reports from waves 1 and 2 to improve reliability (31). We coded work status into 5 mutually exclusive states at each age: full-time paid work, part-time paid work, unpaid caregiving (i.e., “looking after home or family,” which could include childcare, adult care, or household management), full-time education, or in another situation (such as unemployed, retired, sick, or disabled). A working spell was reported if the job lasted for more than 6 months. To capture commonly studied family statuses, we used information on marital/cohabiting status and presence of children younger than 7 years of age in the household, before typical school attendance begins, and when care needs might inhibit paid work participation (9). At each age, respondents were in one of 4 states: partnered with young child, partnered without young child, not partnered with young child, and not partnered without young child.
Two separate sequences were created for each respondent, one for work and another for relationship and parental statuses in each year, spanning ages 12 through 50. We constructed a total of 13,588 sequences from women who participated in SHARELIFE, excluding respondents whose sequences were missing more than 5 years of data on work or family status (n = 550, 4%), resulting in sequence data for 13,038 women. When we included women missing more than 5 years of sequence data in the analysis, results (not shown) were substantively similar. Not unexpectedly, women missing large portions of sequence data had poorer cognitive functioning than those included in the analysis.
We used multichannel sequence analysis to consider these work and family sequences simultaneously, constructing a between-individual distance matrix, on which we performed cluster analysis to classify respondents into groups with similar histories (31). Distances were computed using a variant of the optimal matching procedure, based only on “substitution” costs (changing one sequence element into another) (32, 33). Specifically, we used “dynamic Hamming matching”; the substitution costs used here are inversely proportional to observed transition rates at that point in the life course. Dynamic Hamming matching tends to fare better than other types of optimal matching procedures in producing interpretable outcomes, because temporal ordering is preserved (32).
Finally, we applied hierarchical clustering on the resultant distance matrix using Ward’s method (34) to reveal clusters of work-family histories. We executed the clustering algorithm iteratively, specifying 2–8 clusters, and found that the 5-cluster solution best fit the data (Figure 1).
Figure 1.
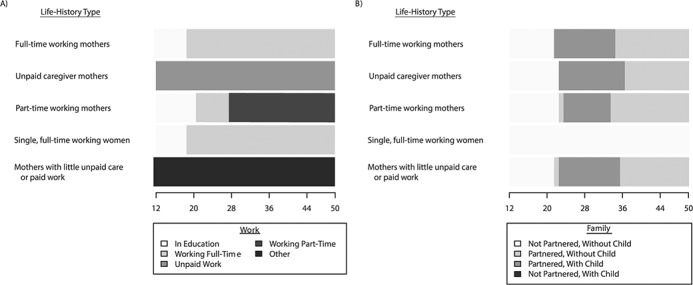
Visual depiction of prototypical work and family trajectories from age 12 to age 50 years among women aged 50–77 years, Survey of Health, Ageing and Retirement in Europe, 2004–2009. Full-time working mother was the most common trajectory (50%), followed by unpaid caregiver mother (25%), part-time working mother (12%), single, full-time working woman (9%), and mother with little unpaid care or paid work (4%).
Statistical analysis
We used the categorical indicator of work-family history types to predict cognitive function using linear and ordinal logistic multilevel models containing individuals nested within countries. We adjusted for age and age-squared and allowed the age-related decline of cognition to vary between countries by including a random slope for the linear age term, because evidence suggests that age-related declines in cognition vary nationally (35). Linear regression with clustered standard errors for country showed substantively similar results (not shown) but does not allow for country-specific age slopes. In age-stratified models (not shown), the direction and magnitude of the associations are similar across age groups. To account for survey design, we scaled the individual-level probability weights provided by SHARE such that the new weights sum to the cluster sample size (36). Proper inclusion of design weights in multilevel models requires scaling them in order to reduce bias in the parameter estimates. As recommended (36), we compared unweighted and weighted results and found them similar, so we present weighted results. To compare all work-family history types with one another, we used pairwise contrasts after estimating the regression models.
RESULTS
European women who were older, were more disadvantaged as children, and who had had less education had lower average cognitive scores (Table 1). Figure 1 depicts a common trajectory for work (Figure 1A) and family (Figure 1B) for one respondent in each work-family history type (Web Figure 1 shows sequences for the full analytical sample). Web Figure 2 presents the distribution of work and family states at each age for each work-family history type.
Table 1.
Characteristics of the Study Sample (n = 11,908), Survey of Health, Ageing and Retirement in Europe, 2004–2009a
| Characteristic | Total Sample | Total Cognition Score | |||
|---|---|---|---|---|---|
| Mean | % | SE | Mean | SE | |
| Cognition scores | |||||
| Total cognition (0–19) | 15.39 | 0.03 | |||
| Orientation (0–4) | 3.89 | 0.00 | |||
| Verbal fluency (0–3) | 2.38 | 0.01 | |||
| Numeracy (0–4) | 2.34 | 0.01 | |||
| Immediate recall (0–4) | 3.52 | 0.01 | |||
| Delayed recall (0–4) | 3.26 | 0.01 | |||
| Age category, years | |||||
| 50–59 | 0.48 | 0.01 | 16.14 | 0.04 | |
| 60–69 | 0.33 | 0.00 | 15.29 | 0.05 | |
| 70–79 | 0.19 | 0.00 | 13.63 | 0.09 | |
| Childhood advantage scaleb | |||||
| 0 | 0.30 | 0.00 | 13.88 | 0.06 | |
| 1 | 0.30 | 0.00 | 15.25 | 0.06 | |
| 2 | 0.24 | 0.00 | 16.38 | 0.05 | |
| 3 | 0.13 | 0.00 | 16.92 | 0.06 | |
| 4 | 0.04 | 0.00 | 17.15 | 0.10 | |
| Education | |||||
| No education | 0.03 | 0.00 | 11.50 | 0.19 | |
| Primary | 0.25 | 0.00 | 13.33 | 0.07 | |
| Lower secondary | 0.18 | 0.00 | 15.46 | 0.06 | |
| Upper secondary | 0.30 | 0.00 | 16.30 | 0.04 | |
| Postsecondary, nontertiary | 0.03 | 0.00 | 16.48 | 0.12 | |
| First stage of tertiary | 0.18 | 0.00 | 17.16 | 0.04 | |
| Second stage of tertiary | 0.00 | 0.00 | 17.19 | 0.22 | |
Abbreviation: SE, standard error.
a Results adjusted for complex survey design.
b Higher values indicate more advantaged childhood.
The most common work-family history was working full-time after leaving education, in conjunction with raising a young child with a partner (50%). The second most common history was spending nearly all of midlife looking after home and family while raising a child with a partner (25%). The 3 other history types captured women who predominately worked part-time while raising a child with a partner (12%), worked full-time but were largely not partnered or raising a child (9%), or were not working for pay for most of midlife and did not report looking after home or family, but were raising a child with a partner (4%). Figure 1 and Web Figure 2 demonstrate more heterogeneity in work than family histories: There were 4 distinct work histories, but only one prototypical family history does not feature partnership and childrearing. The distribution of work-family history types varied by sociodemographic characteristics (Table 2). Women without long durations of paid work were older, had less advantaged childhoods, and had less formal education than women with other work-family histories.
Table 2.
Descriptive Statistics of Work-Family History Types, Expressed as Means and Standard Deviations, Survey of Health, Ageing and Retirement in Europe, 2004–2009
| Characteristic | Full-Time Working Mothers (n = 5,947) | Unpaid Caregiver Mothers(n = 3,011) | Part-Time Working Mothers(n = 1,444) | Single, Full-Time Working Women (n = 1,054) | Mothers With Little Unpaid Care or Paid Work (n = 452) |
|---|---|---|---|---|---|
| Total cognition score (0–19) | 15.69 (2.92) | 14.26 (3.51) | 16.29 (2.56) | 15.77 (2.99) | 14.40 (3.56) |
| Age | 60.85 (7.21) | 63.32 (7.32) | 61.08 (7.15) | 60.59 (7.05) | 63.30 (7.70) |
| Childhood advantage score (0–4)a | 1.34 (1.14) | 0.96 (1.03) | 1.52 (1.13) | 1.59 (1.13) | 1.00 (1.10) |
| Educational attainment (0–6)b | 2.83 (1.50) | 1.95 (1.24) | 2.76 (1.39) | 3.07 (1.49) | 2.01 (1.32) |
Abbreviation: SD, standard deviation.
a Higher scores indicate more advantage.
b Higher scores indicate higher levels of educational attainment based on 1997 International Standard Classification of Education.
We modeled the association between the 5 work-family trajectory types and cognitive functioning, using full-time working and partnered mothers as the reference category. Table 3 shows the multilevel linear regression results for the overall cognition score and multilevel ordinal logistic regressions for individual components of the cognition scale. Compared with full-time working mothers, single women who worked full-time had similar cognitive health in later life. Part-time working mothers had better cognitive scores (β = 0.61, 95% confidence interval (CI): 0.17, 1.06) than full-time mothers (and better verbal fluency, immediate recall, and delayed recall). Pairwise contrasts show that women who spent long periods not in paid work had significantly lower cognitive scores, verbal fluency, numeracy, immediate recall, and delayed recall scores compared with women who worked for pay, regardless of family trajectory. Single women had poorer overall cognitive scores, verbal fluency, immediate recall, and delayed recall scores than part-time working mothers.
Table 3.
Hierarchical Regression of Cognition Score on Work-Family Types Among Women Aged 50–77 Years (n = 11,908), Survey of Health, Ageing and Retirement in Europe, 2004–2009a
| Total Cognition Score (0–19) b | Orientation Score (0–4) c | Verbal Fluency Score (0–3) c | Numeracy Score (0–4) c | Immediate Recall Score (0–4) c | Delayed Recall Score (0–4) c | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI | β | 95% CI |
| Life-history typed | ||||||||||||
| Unpaid caregiver mothers | −1.16 | −1.84, −0.49 | −0.22 | −0.49, 0.06 | −0.69 | −1.07, −0.32 | −0.50 | −0.84, −0.16 | −0.58 | −0.91, −0.24 | −0.49 | −0.81, −0.17 |
| Part-time working mothers | 0.61 | 0.17, 1.06 | 0.00 | −0.23, 0.23 | 0.58 | 0.22, 0.94 | 0.19 | −0.08, 0.46 | 0.42 | 0.13, 0.71 | 0.38 | 0.13, 0.62 |
| Single, full-time working women | 0.13 | −0.14, 0.41 | −0.11 | −0.35, 0.14 | 0.16 | −0.07, 0.40 | 0.10 | −0.06, 0.26 | 0.06 | −0.15, 0.28 | 0.10 | −0.08, 0.27 |
| Mothers with little unpaid care or paid work | −0.92 | −1.65, −0.20 | −0.06 | −0.52, 0.40 | −0.54 | −0.90, −0.19 | −0.48 | −0.88, −0.09 | −0.38 | −0.76, 0.01 | −0.39 | −0.78, −0.01 |
| Agee | −0.77 | −0.95, −0.58 | −0.30 | −0.38, −0.22 | −0.32 | −0.38, −0.25 | −0.30 | −0.38, −0.22 | −0.44 | −0.51, −0.38 | −0.44 | −0.50, −0.39 |
| Age squarede | −0.31 | −0.41, −0.20 | −0.10 | −0.16, −0.04 | −0.10 | −0.15, −0.04 | −0.10 | −0.16, −0.04 | −0.10 | −0.18, −0.02 | −0.09 | −0.14, −0.05 |
Abbreviation: CI, confidence interval.
a All models included random intercept for country and random slope for age. Estimates adjusted for complex survey design.
b Multilevel linear regression.
c Multilevel ordinal logistic regression.
d Reference group is full-time working mothers.
e Age is centered at sample mean of 62 years and standardized.
We calculated the average marginal effect (AME) of each life-history type on the cognitive score for the main model and alternative models that adjusted for childhood advantage and educational attainment. Figure 2 shows AME estimates relative to full-time partnered mothers. Negative values left of the reference line at zero reflect worse cognitive functioning. Results show that partnered mothers who worked part-time had better overall cognitive function (AME = 0.63, 95% CI: 0.18, 1.07). Mothers who did not participate in paid work showed significantly poorer cognitive functioning, whether they were unpaid caregivers (AME = −1.19, 95% CI: −1.89, −0.49) or were otherwise not working for pay (AME = −0.93, 95% CI: −1.66, −0.20). In comparison, a 1-year increase in age is associated with an AME of −0.10 (results not shown); thus, compared with mothers who mainly worked full-time, mothers who did not work for pay had average cognitive scores equivalent to those of women 9–12 years older. Results for models that adjusted for childhood socioeconomic advantage were similar. After adjusting for educational credentials, mothers who predominately did not work for pay or did not spend time as unpaid caregivers were not significantly different than mothers who worked full-time.
Figure 2.
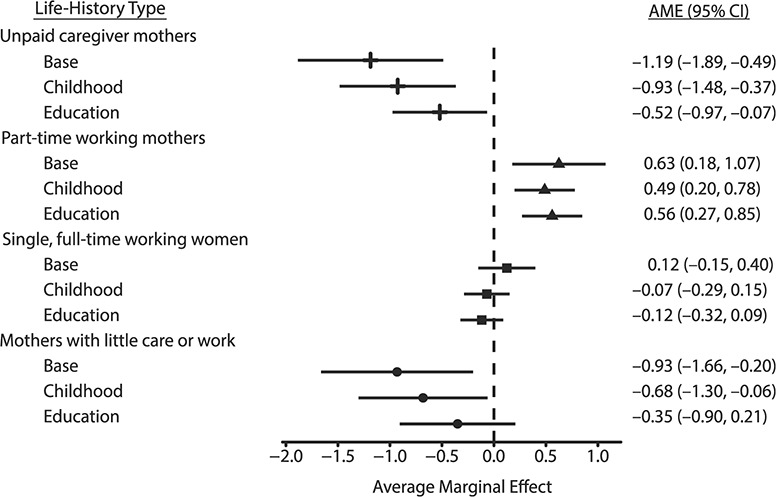
Average marginal effect (AME) and 95% confidence interval (CI) of work-family type on total cognition score relative to full-time working mothers, ages 50–77 years, Survey of Health, Ageing and Retirement in Europe, 2004–2009. Base is total cognition in Table 1. Childhood advantage builds on base to adjust for childhood advantage scale. Education adjusts for 7 categories of educational attainment based on the 1997 International Standard Classification of Education.
DISCUSSION
We identified 5 common and distinct work-family life histories and assessed their association with cognition scores among European women 50–77 years old. The evidence linking work-family histories to physical health is growing, but there has been minimal research on links with cognitive functioning. Because cognition is shaped by long-term exposures, we used multichannel sequence analysis to capture ordering and duration of paid and unpaid work combined with partnership and parenting, to understand how these interdependent life-course processes shape later-life cognition. We found that women who combined part-time paid work with childbearing and partnership for long spans had the best cognitive functioning in later life. Women who spent most of their life not working for pay had the poorest cognitive function.
Previous research suggests that women who combine multiple roles—partnership, child rearing, and paid work—have better physical health outcomes (3, 7). We found that working for pay across midlife, regardless of partnership or parenting experiences, was associated with the best cognitive functioning. While literature to date has identified a favorable association of paid work with cognitive function (17), we provide new evidence by exploring the possibility of heterogeneous associations among working women (part- vs. full-time) and among nonworking women (unpaid caregivers vs. others not steadily working for pay). This is the first investigation, to our knowledge, to distinguish between full- and part-time work in work trajectories, and a key finding is that women who worked part-time for much of midlife had better cognitive health than women who worked full-time, even after adjusting for childhood advantage and educational credentials. These women might benefit from the cognitive stimulation of paid work with less exposure to the stress of paid work or work-family conflict. For these cohorts, part-time working women might also have less financial need to work full-time, exposing them to less daily stress. We also found that spending long periods of midlife taking care of home and family was associated with poorer cognition, building on previous evidence that time out of paid work for homemaking is associated with poorer cognitive health (37). Women not steadily working for pay but who did not report caring for home or family showed outcomes similar to caregivers, pointing toward future research targeting the mechanisms that link labor-force participation to cognitive health.
Life-course work-family exposures might influence cognition for multiple reasons. Cognition experts hypothesize that long exposure to stimulating social environments is protective for cognitive health (13, 16, 18, 19). Cognitive stimulation can come in the form of social interaction, complex tasks, or confronting and solving challenges. Women who spend much of midlife away from paid work might not benefit from the cognitive stimulation of diverse, non-kin social connections (38) and problem-solving opportunities.
Additionally, persistent exposure to work and family role stress, or the strain of managing both, might have consequences for cognitive health. Acute and chronic stress have been linked to cognitive health in prior research (10, 11, 39). Exposure can lead to negative physiological changes and dementia onset by triggering increased levels of glucocorticoids and neuroinflammation (11). Chronic midlife stress is also associated with decreased gray matter volume in certain regions of the brain, with potential maladaptive consequences for cognitive functioning (12). Our findings suggest that for these cohorts of European women, working part-time might be the optimum balance between the stress and stimulation of paid work. While paid work and work-family conflicts might be stressful, women who spend many years at home often act as informal caregivers for children and other kin. Some unpaid responsibilities might involve more exposure to chronic stress (23) and fewer compensating rewards than paid work.
Finally, different work-family histories lead to varied accumulation of material resources. Dual-earner households might have more money to spend on health-promoting lifestyles in midlife and accumulate more resources to spend during retirement. This might lead to more physical exercise, better preventive health care, and less stress in the transition to retirement, which might been linked to better late-life cognition (40). Resources have also been shown to mitigate some of the negative cognitive impact of midlife stressors (10). Moreover, as captured in the work sequences used here, women in the paid work trajectories were more highly educated, and formal education has been shown in a range of studies to have an independent association with cognitive health (41–43). Our results show that after adjusting for educational attainment, women who were out of the labor force no longer had significantly poorer cognition compared with full-time mothers. However, the same pattern was not observed for other work-family types, suggesting that after adjusting for education, exposure to different work-family histories has an independent relationship with cognitive health.
The associations between work-family histories and cognitive health were generally robust to adjustment for a measure of childhood socioeconomic circumstances. Thus, while a large body of literature has shown the cognitive health consequences of early-life contexts (44, 45), we find that women’s mid-life work-family circumstances remain an independent predictor.
Limitations
This study also has limitations. We cannot conclude that there is a causal relationship between work-family trajectories and cognition because of multiple co-occurring endogenous processes in these domains. Moreover, the typologies do not perfectly capture distinct experiences, given that there is variation in life histories within each type, limiting causal identification. These data do not allow us to adjust for early-life cognitive functioning that could influence unfolding work-family histories. However, recognizing that cognitive decline typically occurs later in life and adjusting for early-life advantage bolsters a causal interpretation.
We also rely on retrospective life-history data; respondents can misreport the end date of spells and underestimate the number of spell changes (46, 47). Our trajectories likely reflect less volatility than the true life histories. Survey-recall theory asserts that more salient events will be better recalled, so while specific transition dates or frequency might not accurately be recalled, we expect better recall of salient histories of employment, childbearing, and marriage (46). Comparisons between SHARELIFE retrospective reports and wave-1 and -2 reports on marital status, children living, and employment status show consistency (48). There is also likely a higher amount of recall bias among the cognitively impaired. We found a strong association between missing life-history data and cognitive health (not shown). Because we did not analyze those with large swaths of missing sequence data, we likely captured a conservative estimate of the relationship between life-history trajectories and cognition.
Finally, these associations were found for women born between 1930 and 1957 in certain European nations, and their experiences might not be fully generalizable to other contexts and periods with different distributions of work-family histories or governmental programs to support combining work and childrearing. Additionally, more recent cohorts are more highly educated (49), face more precarious and unstable employment careers (20, 50), and have more varied family lives. Future research should consider whether the stress of precarious work, higher levels of formal education, or changes in partnering and fertility alter the apparent cognitive benefit that we observe for working mothers.
Conclusion and implications
In a large and representative sample of contemporary older European women, we found a robust association between work-family life histories and cognition, regardless of early-life circumstances or educational credentials. The cohorts analyzed here were at the leading edge of radical changes in women’s work and family life histories. Future analyses of more recent cohorts will likely find increasingly varied work and family life experiences, implying additional variation in accumulated stress and cognitive stimulation. The accumulation of experiences in paid and unpaid work, childrearing, and partnership across the life course deserve deeper assessment as social determinants of cognitive health.
Supplementary Material
ACKNOWLEDGMENTS
Author affiliations: Population Studies Center, Institute for Social Research, University of Michigan, Ann Arbor, Michigan (Erin Ice, Shannon Ang, Karra Greenberg, Sarah Burgard); Department of Sociology, College of Literature, Sciences, and the Arts, University of Michigan, Ann Arbor, Michigan (Erin Ice, Shannon Ang, Sarah Burgard); School of Social Sciences, Nanyang Technological University, Singapore, Singapore (Shannon Ang); and the Institute for Research on Women and Gender, University of Michigan, Ann Arbor, Michigan (Karra Greenberg).
This work was supported by the National Institute on Aging and Eunice Kennedy Shriver National Institute of Child Health and Human Development (grants T32AG000221 and P2CHD041028).
The authors gratefully acknowledge the technical help from Dr. Morten Wahrendorf.
The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Conflict of interest: none declared.
REFERENCES
- 1. Ortiz-Ospina E, Tzvetkova S Working women: key facts and trends in female labor force participation. https://ourworldindata.org/female-labor-force-participation-key-facts. Accessed February 19, 2020.
- 2. Eurostat Fertility statistics. https://ec.europa.eu/eurostat/statistics-explained/index.php?title=Fertility_statistics. Accessed February 19, 2020.
- 3. Sabbath EL, Guevara IM, Glymour MM, et al. Use of life course work–family profiles to predict mortality risk among US women. Am J Public Health. 2015;105(4):e96–e102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Lippert AM, Damaske S. Finding jobs, forming families, and stressing out? Work, family, and stress among young adult women in the United States. Soc Forces. 2019;98(2):885–914. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Martikainen P. Women’s employment, marriage, motherhood and mortality: a test of the multiple role and role accumulation hypotheses. Soc Sci Med. 1995;40(2):199–212. [DOI] [PubMed] [Google Scholar]
- 6. Sabbath EL, Mejía-Guevara I, Noelke C, et al. The long-term mortality impact of combined job strain and family circumstances: a life course analysis of working American mothers. Soc Sci Med. 2015;146(suppl C):111–119. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. van Hedel K, Mejía-Guevara I, Avendaño M, et al. Work–family trajectories and the higher cardiovascular risk of American women relative to women in 13 European countries. Am J Public Health. 2016;106(8):1449–1456. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Lu W, Benson R, Glaser K, et al. Relationship between employment histories and frailty trajectories in later life: evidence from the English Longitudinal Study of Ageing. J Epidemiol Community Health. 2017;71(5):439–445. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Engels M, Weyers S, Moebus S, et al. Gendered work-family trajectories and depression at older age. Aging Ment Health. 2019;23(11):1478–1486. [DOI] [PubMed] [Google Scholar]
- 10. Gilsanz P, Quesenberry CPJ, Mayeda ER, et al. Stressors in midlife and risk of dementia: the role of race and education. Alzheimer Dis Assoc Disord. 2019;33(3):200–205. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Greenberg MS, Tanev K, Marin M-F, et al. Stress, PTSD, and dementia. Alzheimers Dement. 2014;10(3 suppl):S155–S165. [DOI] [PubMed] [Google Scholar]
- 12. Gianaros PJ, Jennings JR, Sheu LK, et al. Prospective reports of chronic life stress predict decreased grey matter volume in the hippocampus. Neuroimage. 2007;35(2):795–803. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Vemuri P, Lesnick TG, Przybelski SA, et al. Association of lifetime intellectual enrichment with cognitive decline in the older population. JAMA Neurol. 2014;71(8):1017–1024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Smart EL, Gow AJ, Deary IJ. Occupational complexity and lifetime cognitive abilities. Neurology. 2014;83(24):2285. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Whalley LJ, Dick FD, McNeill G. A life-course approach to the aetiology of late-onset dementias. Lancet Neurol. 2006;5(1):87–96. [DOI] [PubMed] [Google Scholar]
- 16. Fratiglioni L, Wang H-X. Brain reserve hypothesis in dementia. J Alzheimers Dis. 2007;12(1):11–22. [DOI] [PubMed] [Google Scholar]
- 17. Kobayashi LC, Feldman JM. Employment trajectories in midlife and cognitive performance in later life: longitudinal study of older American men and women. J Epidemiol Community Health. 2019;73(3):232–238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18. Zunzunegui M-V, Alvarado BE, Del Ser T, et al. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J Gerontol B Psychol Sci Soc Sci. 2003;58(2):S93–S100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Liao J, Scholes S. Association of social support and cognitive aging modified by sex and relationship type: a prospective investigation in the English Longitudinal Study of Ageing. Am J Epidemiol. 2017;186(7):787–795. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Burgard SA, Brand JE, House JS. Perceived job insecurity and worker health in the United States. Soc Sci Med. 2009;69(5):777–785. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Håkansson K, Rovio S, Helkala E-L, et al. Association between mid-life marital status and cognitive function in later life: population based cohort study. BMJ. 2009;339:b2462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Xu M, Thomas PA, Umberson D. Marital quality and cognitive limitations in late life. J Gerontol B Psychol Sci Soc Sci. 2015;71(1):165–176. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Vitaliano PP, Zhang J, Scanlan JM. Is caregiving hazardous to one’s physical health? A meta-analysis. Psychol Bull. 2003;129(6):946–972. [DOI] [PubMed] [Google Scholar]
- 24. Börsch-Supan A, Brandt M, Hunkler C, et al. Data resource profile: the Survey of Health, Ageing and Retirement in Europe (SHARE). Int J Epidemiol. 2013;42(4):992–1001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Kessler J, Calabrese P, Kalbe E, et al. DemTect: a new screening method to support diagnosis of dementia. Neurobiol Aging. 2000;21(suppl 1):30. [Google Scholar]
- 26. Scheurich A, Müller MJ, Siessmeier T, et al. Validating the DemTect with 18-fluoro-2-deoxy-glucose positron emission tomography as a sensitive neuropsychological screening test for early Alzheimer disease in patients of a memory clinic. Dement Geriatr Cogn Disord. 2005;20(5):271–277. [DOI] [PubMed] [Google Scholar]
- 27. Ziegler U, Doblhammer G. Dementia in Germany—Past Trends and Future Developments [dissertation] Rostock, Germany: University of Rostock; 2010. [Google Scholar]
- 28. Kalbe E, Kessler J, Calabrese P, et al. DemTect: a new, sensitive cognitive screening test to support the diagnosis of mild cognitive impairment and early dementia. Int J Geriatr Psychiatry. 2004;19(2):136–143. [DOI] [PubMed] [Google Scholar]
- 29. Arevalo-Rodriguez I, Smailagic N, Roqué I Figuls M, et al. Mini-Mental State Examination (MMSE) for the detection of Alzheimer’s disease and other dementias in people with mild cognitive impairment (MCI). Cochrane Database Syst Rev. 2015;2015(3):CD010783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30. Verhaeghen P, Salthouse TA. Meta-analyses of age–cognition relations in adulthood: estimates of linear and nonlinear age effects and structural models. Psychol Bull. 1997;122(3):231–249. [DOI] [PubMed] [Google Scholar]
- 31. Brugiavini A, Cavapozzi D, Pasini G, Trevisan E Working life histories from SHARELIFE: a retrospective panel. Working Paper Series 11-2013 http://www.share-project.org/uploads/tx_sharepublications/WP_Series_11_2013_Brugiavini_Cavapozzi_Pasini_Trevisan_01.pdf. Accessed February 19, 2020.
- 32. Killewald A, Zhuo X. U.S. mothers’ long-term employment patterns. Demography. 2019;56(1):285–320. [DOI] [PubMed] [Google Scholar]
- 33. Lesnard L. Setting cost in optimal matching to uncover contemporaneous socio-temporal patterns. Sociol Methods Res. 2010;38(3):389–419. [Google Scholar]
- 34. Ward JH. Hierarchical grouping to optimize an objective function. J Am Stat Assoc. 1963;58(301):236–244. [Google Scholar]
- 35. Formanek T, Kagstrom A, Winkler P, et al. Differences in cognitive performance and cognitive decline across European regions: a population-based prospective cohort study. Eur Psychiatry. 2019;58:80–86. [DOI] [PubMed] [Google Scholar]
- 36. Carle AC. Fitting multilevel models in complex survey data with design weights: recommendations. BMC Med Res Methodol. 2009;9(1):49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Leist AK, Glymour MM, Mackenbach JP, et al. Time away from work predicts later cognitive function: differences by activity during leave. Ann Epidemiol. 2013;23(8):455–462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Ellwardt L, Aartsen M, van Tilburg T. Types of non-kin networks and their association with survival in late adulthood: a latent class approach. J Gerontol Ser B. 2017;72(4):694–705. [DOI] [PubMed] [Google Scholar]
- 39. Sabia S, Nabi H, Kivimaki M, et al. Health behaviors from early to late midlife as predictors of cognitive function: the Whitehall II study. Am J Epidemiol. 2009;170(4):428–437. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Leggett A, Clarke P, Zivin K, et al. Recent improvements in cognitive functioning among older U.S. adults: how much does increasing educational attainment explain? J Gerontol B Psychol Sci Soc Sci. 2017;74(3):536–545. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Beydoun MA, Beydoun HA, Gamaldo AA, et al. Epidemiologic studies of modifiable factors associated with cognition and dementia: systematic review and meta-analysis. BMC Public Health. 2014;14(1):643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Marden JR, Tchetgen Tchetgen EJ, Kawachi I, et al. Contribution of socioeconomic status at 3 life-course periods to late-life memory function and decline: early and late predictors of dementia risk. Am J Epidemiol. 2017;186(7):805–814. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Foverskov E, Glymour MM, Mortensen EL, et al. Education and cognitive aging: accounting for selection and confounding in linkage of data from the Danish registry and Survey of Health, Ageing and Retirement in Europe. Am J Epidemiol. 2018;187(11):2423–2430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Haan MN, Zeki Al-Hazzouri A, Aiello AE. Life-span socioeconomic trajectory, nativity, and cognitive aging in Mexican Americans: the Sacramento Area Latino Study on Aging. J Gerontol Ser B. 2011;66(suppl 1):i102–i110. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Kaplan GA, Turrell G, Lynch JW, et al. Childhood socioeconomic position and cognitive function in adulthood. Int J Epidemiol. 2001;30(2):256–263. [DOI] [PubMed] [Google Scholar]
- 46. Shattuck RM, Rendall MS. Retrospective reporting of first employment in the life-courses of U.S. women. Sociol Methodol. 2017;47(1):307–344. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 47. Pina-Sánchez J, Koskinen J, Plewis I. Measurement error in retrospective work histories. Survey Research Methods. 2014;8(1):43–55. [Google Scholar]
- 48. Garroutse C, Paccagnella O. Data Quality: three examples of consistency across SHARE and SHARELIFE data In: Schroder M, ed. Retrospective Data Collection in the Survey of Health, Ageing and Retirement in Europe. Mannheim, Germany: Mannheim Research Institute for the Economics of Ageing; 2011. [Google Scholar]
- 49. Buchmann C, DiPrete TA. The growing female advantage in college completion: the role of family background and academic achievement. Am Sociol Rev. 2006;71(4):515–541. [Google Scholar]
- 50. Kalleberg AL. Nonstandard employment relations: part-time, temporary and contract work. Annu Rev Sociol. 2000;26:341–365. [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.