

Abstract
Background
Rape remains a controversial issue with a few victims reporting experience because of the myriad of societal perception, prolonged steps in pursuing a case to logical conclusion of securing conviction, as well as psychological and physical residuals of the experience. Data in Nigeria is therefore hard to come by as it is diminished and often not available.
Objectives
To assess the pattern and trend of rape cases in a State in Nigeria.
Methods
A descriptive and retrospective study where data records on socio-demographics and case specifics was collected on victims of sexual assault that reported to DFID/ PATHS 2 supported Tamar Sexual Assault Centre between 2014 and 2016 after which it was analysed and presented in bar charts.
Result
The yearly prevalence varied for the different age groups studied with the highest prevalence noted for 13 years and above (175,200,255) over the 3 years of 2014, 2015 and 2016 studied. The reported cases also improved over the studied years with rates of 0.47, 0.96 and 0.5 respectively.
Conclusion
The yearly comparison and baseline data show that the centre's establishment caused an improvement in rape case reporting and follow-up.
Keywords: Rape, trends, Nigerian, State
Introduction
Rape occurs globally. It has far reaching physical, psychological, social and otherwise effect on the victims which is longstanding.1 Rape is defined medically as unlawful sexual activity and usually sexual intercourse carried out forcibly or under threat of injury against the will usually of a female or with a person who is beneath a certain age or incapable of valid consent.2 In most African societies, women are not in a position to control their sexual lives because of their poor socio-economic status. There is a general agreement that sexual violence against women is rooted in gender power inequalities prevalent in society and in hierarchical gender relations.3 Most women get lured into sex because of financial difficulties. A supposedly financially beneficial friendship cum relationship transcends the confines of a safe inter-relationship as the party financially poised in the situation exploits the prevalent exposure offered by the physical presence/ availability of the dependent fellow. A naive, deprived, helpless, and expectant female becomes a victim of a fellow looked-up-to for succour, financial help and psychological uplift.
In Nigeria as in many other countries there are limited researches on rape. However, more of such studies are needed for further insight into this grave societal vice as rape typifies. In Nigeria, there have been rising newspaper reported cases of rise in rape incidences. Despite this, the issue of rape has been one bereft of in-depth studies in this environment.4,5,6,7,8,9
The increase in reportage of rape cases could however be attributed to an increased awareness, total increase in number of rape cases or both.10,11,12 It is worthy of note however that the reported cases represent the tip of the iceberg; with estimated eight out of every nine cases remaining unreported.13 It is disappointing that a search for articles or publications on rape in Nigeria on the internet will reveal essentially newspaper articles or reportage of isolated cases or incidences but little or no defined informative study or data. This reveals a yelling and a yearning gap.
A community based survey of rape estimated the rate of such incidents at 1300 per 100,000 women a year, which is likely to be more accurate.14 A very worrying dimension of rape has increasingly gained prominence in the recent past in our environment. This is sexual abuse of minors. There have been repeated reports of abuse of children as young as 3 years of age even in sub Saharan Africa.15,16
So many reasons could be called to question and they are varied. The internet has been misused by the youths and the elderly such that what people see on their phones might trigger the animalistic evil of fornication. 17 Some parents would leave their children to travel long distance to stay with cousins or aunts that they have no idea what he or she is capable of.18 It could sometimes be due to undue or avoidable exposure; for instance in a situation the rapists were able to perpetrate their criminal act because the victim's mother had sent her on an errand to the accused residence at a late hour in the night.19
Part of control to these situations is for government to empower the justice system so that stringent punishment would be meted out to those found guilty of rape.20
This paper aims to estimate the trend of rape in the Nigerian state of Enugu. Enugu State is actually one of the 36 States that make up the country Nigeria. The hypothesis is that there are incidences of rape in a Nigerian state with adult victims as well as under aged children.
Methods
Study design
This is a descriptive and retrospective study. Victims of rape that presented at the Tamar Sexual Assault Centre (TSAC) between 2014 and 2016 were studied regards their socio-demographics, experience, pathway of their cases and conclusion of cases and subsequently analysed and presented in bar charts. The retrospective approach to the study was based on the uniqueness of the population studied as well as fact that records in this centre of the stated time period was studied.
Study Population
The Tamar Sexual Assault Centre provides services to about 500,000 people within and around the State of Enugu. 21 The city of Enugu with a literacy level of about 70% is accessible by air and land. Residents who are predominantly Ibo by tribe and Christians are businessmen and women, civil servants, artisans, traders and farmers.21 The population can therefore be fairly generalizable as representation of the State picture in terms of the study topic. It is of course easily understandable that those at the city centre would access the centre more easily because of closeness than those that would travel from satellite cities which is a longer distance and may not boast of equally good roads.
Study Site
The Tamar Sexual Assault Centre was set up in 2014 to provide high quality and confidential, medical, counselling and other support services to victims/survivors of sexual violence. It supports recovery and encourages reporting of rape and other sexual assaults so that justice can be achieved. The Centre was set up in 2014 to provide high quality and confidential, medical, counselling and other support services to victims/survivors of sexual violence. It supports recovery and encourages reporting of rape and other sexual assaults so that justice can be achieved. The Centre is open 5 days a week within working hours and till midday on weekends and public holidays (especially cases demanding emergency attention and outpatient gynaecology cases) during the period of the study. The centre which is strategically sited in the heart of the city is accessible to people from the Enugu North, South and East Local Government Areas and of course from suburbs and surrounding cities.
Paths2 worked with J4A funded Tamar Sexual Assault Centre (SAC) between 2014 and 2016. The technical support provided to Tamar Sexual Assault Centre through the Desk stimulated spikes in rape case reporting rates in the Enugu metropolis. The collaboration of this centre with Paths2 also worked for a state government takeover of the SAC from DFID-J4A.
Specific input of paths 2 included:
Development of the strategic plan for the centre Development and delivery of media campaigns Setting up of media coalition Mounting of awareness raising art exhibition The Centre has eight permanent staff including two on secondment from Government (Ministries of Health; Gender Affairs and Social Development) and two consultant doctors, including the State Police Doctor/ Pathologist).
Ethical consideration
Ethical clearance to proceed on the study was obtained from the State Ministry of Health. Since disclosure of personal information can be harmful in several ways, disclosure is not made on names and actual identities of the individuals whose records were studied and analysed. A high level of importance was therefore attached to respect for privacy of the victims and confidentiality of information. This approach would definitely safeguard future studies of this kind so as not to make victims reluctant to share personal information. It is worthy of note that informed consent of victims had ab initio been sort by the TSAC to probability of their information being provided for research and statistical purposes as well as fight against such cases of rape; this also included informed consent to publication. This was however done with a reassurance that their privacy would be protected and that data would only be utilized except for such cases as their consent had been sort.
Data collection
Entries were made on various vital and necessary socio-demographics and other vital information of the victims like age, sex, area of residence, types of incidence (rape/ defilement, sexual assault etc) those victims that received treatment, those with Forensic Medical Report (FMR) forwarded to police, those with cases charged to court, those with cases at various stages of execution and ones convicted.
This secondary data was collection from the TSAC records for the stated period and purpose. Data was fed in computer from the records. Processes to ensure originality and correctness of data were equally employed as there was input control to ensure data was accurately captured and properly recorded. To ensure completeness and correctness of data transmitted data transmission controls was instituted. In like manner, the input, processing, and output control procedures were factored in the application controls to ensure processing objectives are attained.
Results
Figure 1 reflects that ages 13 years and above present most cases of rape in all the years assessed, followed closely by the age bracket 6 to 12 years. The under 5 years old represent the least affected age group. The exact percentages of these occurrences are aptly captured in the Figure 1.
Figure 1.
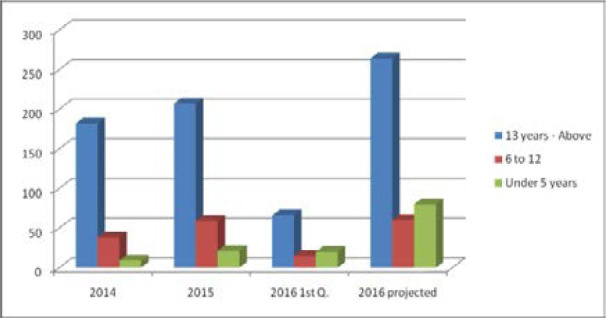
Rape Trends 2014 to 2016 for victims of different age groups
Figure 1 shows that most victims of rape are in the age range of 13 and above. In 2014, 2015, 1st quarter 2016 and projected 2016 those that are 13 year and above that were raped represent 79%, 72%, 65% and 65% of the total number of rape cases in the state respectively. Those in age brackets 6 to 12 years represent 17%, 21%, 15% and 15% of those raped in 2014, 2015, 1s quarter 2016 and projected 2016 respectively while rape victims who are under 5 years represent 3%, 7%, 20% and 20% in 2014, 2015, 1s quarter 2016 and projected 2016 respectively in the State.
Figure 2 provides evidence that most less than 5 years old affected actually happen to be infants.
Figure 2.
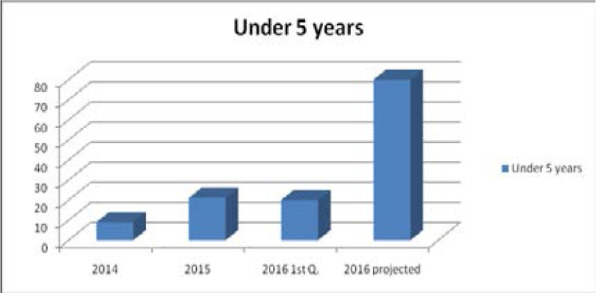
Rape Trends for the under 5 years old
(Most of the U-5 victims are actually less than 1 year old babies!)
The greatest incidence of occurrence in those aged 6 to 12 years old happened in 2015 and 2016 as projected. This is captured in Figure 3.
Figure 3.
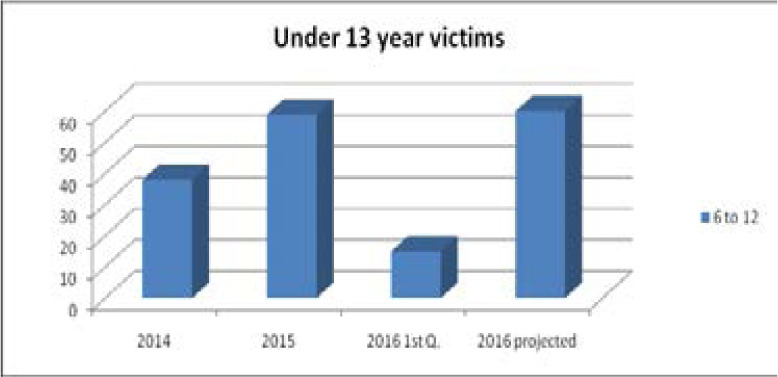
Rape Trends for under 13 years old victims
Figure 4 shows a steep rise of 133% of children less than 5 years old sexually assaulted between 2014 to 2015. This is more pronounced compared to other ages. As an addendum, a total of 516 victims of sexual assault had reported to the TSAC within April 2014 and June 2016.
Figure 4.
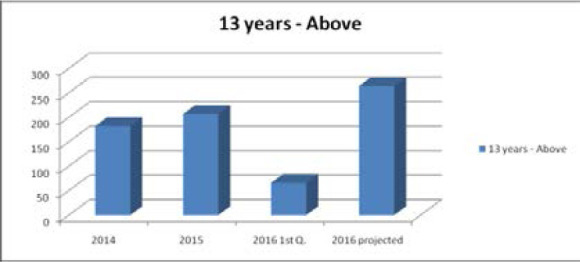
Rape Trends for the victims 13 years and above
(Trend here (figure 2a-c) shows that from 2014 to 2015 percentage of children under 5 that were raped changed by 133% point. By the end of 2016 following projection based on the first quarter of 2016, there will be 281% change in number of children under 5 years would have been raped. From 2014 to 2015 percentage of children 6 to 12 years that were raped changed by 55%. By the end of 2016 following projection based on the first quarter of 2016, there will be 2% increase in number of children 6 to 12 years would have been raped. Also from 2014 to 2015 percentage of children 13 years and above that were raped changed by 14%. By the end of 2016 following projection based on the first quarter of 2016, there will be 28% increase in number of children 13 years and above that have been raped).
Note: Report for 2016 is projected from 1st quarter of 2016.
Of this number, 312 were under the age of 18 (minors) with 135 of them under 10 years of age and 204 above 18.
488 of the victims were provided with medical treatment between the stated periods of April 2014 to June 2016. 308 Forensic Medical Reports (FMR) were forwarded to the Nigeria Police Force.
40 cases was charged to court of which 5 cases were discharged, 7 cases at prosecution stage, 27 cases awaiting trial and 1 perpetrator prosecuted and imprisoned for 14 years, following trial.
A breakdown of the types of incidents and number experienced was:
| Type of incident | Number |
| Rape/Defilement | 463 |
| Attempted Rape | 16 |
| Sexual Assault | 22 |
| Others (Domestic violence | 15 |
| Total number of cases | 516 |
Discussion
Rape cases in our environment have persistently remained unreported as victims are scared of the resultant societal stigma/ controversial attention that come with it. There is the concern by especially female victims that potential husbands may lose interest as this feeling pervades ‘how could I marry someone raped by other men; without protection that could have been armed robbers and bad people?’ Anyway, this is close to the truth of what obtains. A particular study found that the annual incidence of rape was 198 per 100, 000 women. This probably was far less than the actual figures, as many of the rapes remain unreported. In South Africa, the incidence of rapes and attempted rapes reported by the Cape Times (1999) in South Africa was approximately 300 per 100, 000 women which is very high.22
It is also a common belief in a rural South African suburb called Transkei that rape is unreported. Estimate has it that for every 36 cases of rape, only one is reported. 23 This is actually somewhat what is obtainable in this study as prior to the establishment of the Tamar Assault Centre rape cases were largely unreported. Skeletal reports were at police posts and area commands and pursuit of these cases basically low as the societal attitude to rape is essentially complex.
It is found in this study that 13 years and above age range present the most cases of raped victims in all the years assessed followed by those aged 6 to 12 years. This is somewhat similar to data derived from a similar study where the most common age group that reported sexual assault was between 11 and 20 years, citing age group more vulnerable as most sexually active age range.10 This could as well be attributed to the fact that this age group would have developed very prominent physical attributes of a full-fledged female that the prodding eyes of the morally decadent and sexually mentally warped rapists could not resist in the height of their obsession/madness. In most areas of poor economic status, where families share restrooms and bathrooms in the local parlance referred as ‘yards’, the men who though grew up seeing this young females given birth to are thrown off seeing their full sexual maturity. Those men that could not contain it with just noticing these features move on to prey and feed their eyes clandestinely as these young children and teenagers make use of the common bathrooms. In a most obsessed state, they even go ahead to seek a taste though forcefully and immorally. In this scenario we are faced with a case of rape.25,26
As above results reflect, less than 5 year old victims of rape appear to be predominantly infants. This is in line with available evidence which is consistent with most pathetic stories stemming from rape of minors and infants sometimes by caregivers and biologic parents. It is worthy of note here that children are very vulnerable, as they are the weakest members in a society in which violence is rife.22 Some erroneous belief that sex with under aged children especially the extremely young is a form of cure for HIV has been attributed in certain studies as a motivation factor for child rape.22 This is as much alarming as it is nauseating and has led to innocent children even infants being subjected to sexual abuse which otherwise would not have happened.27
A factor that could be attributed to more cases of infant victims in the under 5 year age group captured could be their vulnerability and people's attention wading off that any human being could even brood the thought nor go on to actualize it. This kind of case therefore becomes the most shocking and difficult subset experienced. This view has been captured in similar studies. 28,29
In this study, in the year 2015 and 2016 as projected, greatest incidence of rape had occurred in victims aged 6 to 12 years old. This age group also happened to be second the most common age group affected in all the years assessed after ages 13 years and above. This is relatively consistent with findings from previous studies.10 It is however alarming and a matter of serious concern that percentage of children under 5 years old who were raped changed by 133% point from 2014 to 2015. There is data to support that more victims report from particular parts of the metropolis. One wonders what this is attributable to. Different situations could be called into question such as socio-economic status, education level, areas more prone to violence which are all in directly related to poor socio-economic status.30
In a study in South Africa, in 2001, 78 cases (39/ 100, 000 women a year) were reported. The rape victims increased more than twice (88/ 100. 000) in 2001, and reached the highest level (417/ 100, 000) in 2006. The mean rate of sexual assault was therefore 198/ 100, 000 women in a year.22 The prevalence of rape had increased tenfold between 2001 and 2006. This showed a similar pattern with the results of this study especially amongst children as percentage of children under 5 that were raped changed by 133% point from 2014 to 2015. 10 In fact different alarming viewpoints of reasons to the rape intent continue to circulate. Part of the very intriguing of these is that of certain personalities whose only way of enjoying sex is when it is forceful and violent. A certain number of interrogations of culprits have opined this as a drive to rape.
There are myriads of problems associated with this increased rate of rape and sexual abuse. Top on the list is the likely increase in HIV transmission. This is because the last thing on the rapist mindset during the ignominious act is safe sex/sexual protection. There is therefore no use of condom, rough sex with attendant predisposition to increased chances of HIV transmission. HIV/AIDS remain however, a double-edged sword. On the one hand rape victims are more vulnerable to HIV infection and on the other hand, some HIV-infected persons are looking for unfounded mythical cure by raping children.31,32
The good news for victims reporting to the Tamar Assault Centre is that victims now receive PEP (Post Exposure Prophylaxis) treatment, other medical treatments, counselling, psychosocial support and assistance in prosecuting offenders though actually much needs to be done. All raped women should actually have immediate access to counselling and antiretroviral drugs.10 The burden of rape is enormous. There is the issue of societal attitude to victims (stigma), the psychological and physical trauma on the victims themselves, the cost of the attention the situation demands medically; in terms of forensic investigations, prosecution of the case and search for justice are all substantially weighty. It is therefore an issue that yells for more governmental/societal concern, funding to and directed research; health education/awareness creation and a sustained attention to view of combating/reducing the cases. This health promotion effort is the thrust of this research article.
Limitations
Issues of originality and correctness of data was a major limitation. However processes to ensure originality and correctness of data were equally employed as there was input control to ensure data was accurately captured and properly recorded. To ensure completeness and correctness of data transmitted also, data transmission controls was instituted.
Conclusion
Rape victims are predominantly 13 years and above age group in all the years assessed. However, though least affected age group, the under 5 years old when victims, are more of infants.
Recommendation
Families should be more careful in employing care givers for their children and infants.
More enlightenment so that children and teenagers are subtly made conscious of this societal ill, in that way they are better equipped to evade present and future predator uncles, family friends and care givers.
Acknowledgements
Thanks to God Almighty for making this study possible.
Thanks to PATHS 2/ DFID for the technical support to this project
Deep sense of appreciation to my parents Sir & Lady J.N. Idoko. This is in memorial to my great dad. To my wife Chichi, I keep thanking God for the gift of you and our lovely Arthur, Adriel and Adaoma.
Abbreviations
- TSAC
Tamar Sexual Assault Centre
- J4A
Justice for All
- DFID
Department for International Development
- PATHS 2
Partnership for Transforming Health Systems 2
- FMR
Forensic Medical Report
- HIV
Human Immunodeficiency Virus
- AIDS
Acquired Immune Deficiency Syndrome
- PEP
Post Exposure Prophylaxis
Financial Disclosure
The authors of this paper reported no financial disclosures.
References
- 1.Sexual Violence-World Health Organization. http://www.who.int/violence_injury_prevention/violence/global_campaign/.../chap6.pdf. Accessed 27 Dec 2017.
- 2.Definition of Rape by Merriam-Webster. https://www.merriam-webster.com/dictionary/rape. Acessed 27 Dec 2017.
- 3.Jewkes R. Preventing sexual violence: A rights-based approach. The Lancet. 2002;360:1092–3. doi: 10.1016/S0140-6736(02)11135-4. PubMed. [DOI] [PubMed] [Google Scholar]
- 4.Nigeria News today & breaking news. https://www.naija.ng/62035.html. Accessed 20 Dec 2017.
- 5.Naija Bush Sex. http://www.nigeriastandardnewspaper.com/ED11crime.htm. Accessed 27 Dec 2017.
- 6.Child Rape Cases Nigeria. https://ynaija.com/tag/child-rape-cases-nigeria/. Accessed 23 Dec 2017.
- 7.Rape-Latest Nigeria News. https://latestnigerianews.com.ng/tag/rape/. Accessed Dec 20 2017.
- 8.Rape Victims - Online Nigeria News. https://news2.onlinenigeria.com/keywords/rape-victims. Accessed 27 Dec 2017.
- 9.News - Vanguard News. https://www.vanguardngr.com > News. Accessed 27 Dec 2017.
- 10.Meel BL. An epidemiology of sexual assault among elderly women in the Mthatha area of South Africa. Med Sci Law. 2017 Apr;57(2):69–74. doi: 10.1177/0025802416683610. [DOI] [PubMed] [Google Scholar]
- 11.Amah N, Shittu SO, Abdul MA. Risk scoring for domestic violence in pregnancy. Niger J Clin Pract. 2008;11:18–21. PubMed. [PubMed] [Google Scholar]
- 12.Adeleke NA, Olowookere AS, Hassan MB, Komolafe JO, Asekun-Olorinmove EO. Sexual assault against women at Osogbo South western Nigeria. Niger J Clin Pract. 2012 Apr;15(2):190–3. doi: 10.4103/1119-3077.97316. [DOI] [PubMed] [Google Scholar]
- 13.Kapp C. Rape trial in South Africa. The Lancet. 2006;367:18–9. doi: 10.1016/S0140-6736(06)68285-8. PubMed. [DOI] [PubMed] [Google Scholar]
- 14.Jewkes R, Abrahams N. The epidemiology of rape and sexual coercion in South Africa: an overview. Soc Sci Med. 2002;55(7):1231–244. doi: 10.1016/s0277-9536(01)00242-8. PubMed. [DOI] [PubMed] [Google Scholar]
- 15.Finkelhor D, Shattuck A, Turner AH, Hamby SL. The Lifetime Prevalence of Child Sexual Abuse and Sexual Assault Assessed in Late Adolescence. Journal of adolescent Health. 2014;55(329):329–33. doi: 10.1016/j.jadohealth.2013.12.026. [DOI] [PubMed] [Google Scholar]
- 16.Department of Justice, office of Justice Programs, Bureau of Justice Statistics . 2000. Sexual Assault of Young Children as Reported to Law Enforcement. [Google Scholar]
- 17.Nigerians React to Rise in Rape Cases in Nigeria. https://www.naija.ng. Accessed 27 Dec 2017.
- 18.Jealous Family Members: A Family Relationship Problem. https://www.wehavekids.com. Accessed 27 Dec 2017.
- 19.What is the right - punishment for rapists? https://www.punchng.com/right-punishment-rapists. Accessed 20 Dec 2017.
- 20.Violence Against Women: Where are the solutions? https://www.ncbi.nim.nih.gov/pmc/articles/PMC4462781/. Accessed 27 Dec 2017.
- 21.Ilechukwu GC, Ilechukwu CGA, Ubesie AC, Onyire NB, Emechebe G, Eze JC. Relationship Between Nutritional Status and Intensity of Common Intestinal Helminths Among Children in Enugu, South East Nigeria. Ann Med Health Sci Res. 2014;(2):119–22. doi: 10.4103/2141-9248.138027. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Abarder G. Western Cape cops tops for serious crime. Cape Times. 1999 May;13:9.14. [Google Scholar]
- 23.Martins LJ. Forensic evidence collection for sexual assault: A South African Perspective. International J of Gynecology and Obstetrics. 2002;78(1):105–10. doi: 10.1016/S0020-7292(02)00054-1. [DOI] [PubMed] [Google Scholar]
- 24.Go VF, Sethulakshmi CJ, Bentley ME, Sivaram S, Srikrishnan AK, Solomon S, et al. When HIV-prevention messages and gender norms clash: The impact of domestic violence on women's HIV risk in slums of Chennai, India. AIDS and behavior. 2003;7:263–272. doi: 10.1023/a:1025443719490. PubMed. [PubMed: 14586189] [DOI] [PubMed] [Google Scholar]
- 25.Goldstein DM. AIDS and women in Brazil: The emerging problem. Social Science and Medicine. 1994;39:919–929. doi: 10.1016/0277-9536(94)90204-6. [PubMed: 7992125] [DOI] [PubMed] [Google Scholar]
- 26.Irwin KL, Edlin BR, Wong L, Faruque S, McCoy HV, Word C, et al. Urban rape survivors: Characteristics and prevalence of human immunodeficiency virus and other sexually transmitted infections. Obstetrics and Gynecology. 1995;85:330–336. doi: 10.1016/0029-7844(94)00425-d. [PubMed: 7862367] [DOI] [PubMed] [Google Scholar]
- 27.Meels BL. The myth of child rape as a cure for HIV/ AIDS in Transkei: A case report. Medicine, Science and the Law. 2003:85–8. doi: 10.1258/rsmmsl.43.1.85. [DOI] [PubMed] [Google Scholar]
- 28.Bhandari S., Winter D., Messer D., Metcalfe C. Family characteristics and long-term effects of childhood sexual abuse. British Journal of Clinical Psychology. 2011;50(4):435–451. doi: 10.1111/j.2044-8260.2010.02006.x. [PubMed] [Google Scholar] [DOI] [PubMed] [Google Scholar]
- 29.Browne A., Finkelhor D. Impact of child sexual abuse: A review of the research. Psychological Bulletin. 1986;99(1):66–77. [PubMed] [Google Scholar] [PubMed] [Google Scholar]
- 30.Bates LM, Schuler SR, Islam F, Islam K. Socioeconomic factors and processes associated with domestic violence in rural Bangladesh. International Family Planning Perspectives. 2004;30:190–199. doi: 10.1363/3019004. [PubMed: 15590385] [DOI] [PubMed] [Google Scholar]
- 31.Meel BL. HIV seroconversion following sexual abuse. Clin Forensic Med. 2005 Oct;12(5):268–70. doi: 10.1016/j.jcfm.2004.10.016. [DOI] [PubMed] [Google Scholar]
- 32.Meel BL. HIV/AIDS post-exposure prophylaxis (PEP) for victims of sexual assault in South Africa. Med Sci Law. 2005 Jul;45(3):219–24. doi: 10.1258/rsmmsl.45.3.219. [DOI] [PubMed] [Google Scholar]