

Abstract
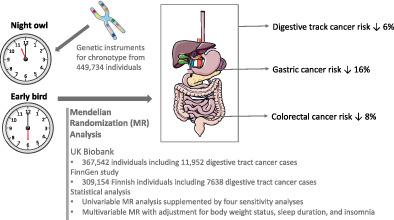
Morning chronotype has been associated with a reduced risk of prostate and breast cancer. However, few studies have examined whether chronotype is associated with digestive tract cancer risk. We conducted a Mendelian randomization (MR) study to assess the associations of chronotype with major digestive tract cancers. A total of 317 independent genetic variants associated with chronotype at the genome‐wide significance level (P < 5 × 10−8) were used as instrumental variables from a genome‐wide meta‐analysis of 449 734 individuals. Summary‐level data on overall and six digestive tract cancers, including esophageal, stomach, liver, biliary tract, pancreatic and colorectal cancers, were obtained from the UK Biobank (11 952 cases) and FinnGen (7638 cases) study. Genetic liability to morning chronotype was associated with reduced risk of overall digestive tract cancer and cancers of stomach, biliary tract and colorectum in UK Biobank. The associations for the overall digestive tract, stomach and colorectal cancers were directionally replicated in FinnGen. In the meta‐analysis of the two sources, genetic liability to morning chronotype was associated with a decreased risk of overall digestive tract cancer (odds ratio [OR] 0.94, 95% confidence interval [CI]: 0.90‐0.98), stomach cancer (OR 0.84, 95% CI: 0.73‐0.97) and colorectal cancer (OR 0.92, 95% CI: 0.87‐0.98), but not with the other studied cancers. The associations were consistent in multivariable MR analysis with adjustment for genetically predicted sleep duration, short sleep, insomnia and body mass index. The study provided MR evidence of inverse associations of morning chronotype with digestive tract cancer, particularly stomach and colorectal cancers.
Keywords: chronotype, colorectal cancer, digestive system cancer, gastric cancer, Mendelian randomization
What's new?
Cancers of the digestive tract are associated with various traditional risk factors, including smoking and obesity. A possible novel risk factor may be chronotype, an individual's natural tendency to sleep at a particular time. In our study, the authors assessed potential associations between digestive tract cancers and chronotype using Mendelian randomization analysis of UK Biobank and FinnGen study data. Overall risk of digestive tract cancer, stomach cancer and colorectal cancer was found to be inversely associated with genetic liability to morning chronotype. Analyses further indicate that the associations are independent of sleep duration, short sleep, insomnia and body mass index.
Abbreviations
- BMI
body mass index
- CI
confidence interval
- MR
Mendelian randomization
- OR
odds ratio
- SNP
single‐nucleotide polymorphisms
1. INTRODUCTION
Digestive tract cancer with 4.8 million new cases (26% of global cancer incidence) caused 3.4 million premature deaths (35% of cancer‐related mortality) in 2018 worldwide, which poses a large global disease burden. 1 Previous studies identified several risk factors for digestive tract cancer, including obesity, cigarette smoking, alcohol consumption and hepatitis B virus infection. 1 , 2 , 3 , 4 , 5 Primary and secondary prevention strategies targeting at above risk factors may play an important role in preventing and controlling gastrointestinal malignancies. 1 However, except for the above traditional risk factors, novel factors are scarcely studied, such as chronotype, possibly influencing the risk of gastrointestinal cancers.
Chronotype is the natural propensity for the individual to sleep at a particular time. Two extreme types of chronotype, termed morningness (an early bird) and eveningness (a night owl), means having an advanced and delayed sleep period, respectively. Evening chronotype associates with less physical activity 6 and unhealthy dietary habits 7 and thus could potentially have adverse health effects and increase the risk of cancer. 8 A matched case‐control study revealed that patients with gastroenteropancreatic neuroendocrine tumors had more commonly an evening chronotype compared to healthy controls. 9 Another study using metagenomic sequencing analysis found that morning chronotype was associated with a decreased abundance of Alistipes and an elevated abundance of Lachnospira. 10 These two gut microbiome genera may play a role in the development of cancers in the gastrointestinal tract, such as colorectal cancer. 11 , 12 Even though a few studies linked chronotype to digestive tract cancer, no studies examined this association.
Mendelian randomization (MR) is an epidemiological approach that can strengthen the causal inference by utilizing genetic variants as instrumental variables for an exposure. 13 The design has two merits. First, it can minimize confounding effects since genetic variants are randomly assorted at conception and therefore not correlated with environmental or self‐adopted factors that are usually confounders in the association between the exposure and outcome. 13 Second, the approach can diminish reverse causality because the onset and progression of disease cannot modify the germline genotype. 13 Previous MR studies revealed inverse associations of morningness with the risk of prostate and breast cancers. 14 , 15 , 16 Nevertheless, no studies were conducted to examine the associations between chronotype and digestive tract cancers. Here, we conducted an MR investigation to explore the causality of these associations.
2. METHODS
2.1. Outcome data sources
Genetic associations with six digestive tract cancers (esophageal, stomach, liver, biliary tract, pancreatic and colorectal cancers) and overall digestive tract cancer were obtained from the UK Biobank study and the FinnGen study. 17 The UK Biobank study is an ongoing cohort study that was initiated by recruiting about 500 000 adults between 2006 and 2010. Our study was based on data from a total of up to 367 542 individuals followed up until April 2022 after removal of those with non‐Caucasian ethnicity (to reduce population stratification bias), sex mismatch, excess heterozygosity and low genotype call rate, and those related by third degree or higher. We defined 11 952 digestive tract cancer cases including 1339 esophageal, 1086 stomach, 503 liver, 656 biliary tract, 1414 pancreatic and 7543 colorectal cancer patients. These cases were diagnosed by using codes of International Classification of Diseases (9th and 10th revisions) and self‐reported information verified by interview with a nurse from national registries (Table S1). For the FinnGen study, we used data from the R6 release that includes 309 154 Finnish individuals after excluding participants with ambiguous gender, high genotype missingness (>5%), excess heterozygosity (±4 SD) and non‐Finnish ancestry. 17 A total of 7638 patients with digestive tract cancers were ascertained, including 358 esophageal, 889 stomach, 442 liver, 157 biliary tract, 881 pancreatic and 4401 colorectal cancer patients. Similarly, cancer cases were defined by codes of International Classification of Diseases (8th, 9th and 10th revisions) with information from nationwide registries (Table S2). The associations were adjusted for age, sex and 10 genetic principal components in both data sources.
2.2. Genetic instrument selection
Single‐nucleotide polymorphisms (SNPs) associated with chronotype at the genome‐wide significance level (P < 5 × 10−8) were extracted from a genome‐wide meta‐analysis of 449 734 individuals of European‐ancestry from the UK Biobank and 248 098 individuals of European‐ancestry from 23andMe. 18 Linkage disequilibrium was estimated among selected SNPs based on the 1000 Genomes European reference panel. 19 SNPs in linkage disequilibrium (r 2 > .01) were excluded and the SNP with the smallest P value for the genetic association with chronotype was retained. After clumping, 317 SNPs in autosomal chromosomes were selected as instrumental variables (Table S3). The genetic score of these SNPs showed no associations with sleep duration and quality as well as insomnia. 18 In the main analysis, we used the estimates (beta and corresponding SE coefficients) of the associations between SNPs and chronotype from the meta‐analysis of UK Biobank and 23andMe to increase the power. In addition, we used the genetic association estimates obtained from only 23andMe to minimize the sample overlap in the sensitivity analysis (Table S3). Genetic associations were scaled to one point increase in chronotype category (−2 for definitely evening, −1 for more evening than morning, 0 for unknown, 1 for more morning than evening and 2 for definitely morning) and estimated by a linear mixed model with adjustment for age, sex, study center, genotyping array and genetic principal components. 18
2.3. Sleep features and body mass index data sources
Summary‐level data on sleep duration and short sleep (<7 hours/day) were obtained from a genome‐wide association analysis of 446 118 individuals of European ancestry (106 192 short sleep cases compared to 305 742 controls with 7‐ to 8‐hour sleep duration). 20 Genetic associations were adjusted for age, sex, 10 principal components of ancestry, genotyping array and genetic correlation matrix. 20 Summary‐level data on insomnia were extracted from a genome‐wide association study of 453 379 individuals of European ancestry (345 022 cases with any insomnia symptoms and 108 357 controls). 21 Genetic associations were adjusted for age, sex, 10 principal components of ancestry and genotyping array. 21 Genetic associations with body mass index (BMI) were extracted from the genome‐wide analysis in the Genetic Investigation of ANthropometric Traits consortium including 806 834 individuals with adjustment for age, sex and genetic principal components. 22
2.4. Statistical analysis
We used the random‐effects multiplicative inverse variance weighted method as the primary analysis to estimate the association between genetic liability to chronotype and the risk of digestive tract cancers. Given that the analysis is sensitive to outliers and horizontal pleiotropy, four sensitivity analyses, including the weighted median, 23 MR‐Egger, 24 MR‐PRESSO 25 and contamination mixture 26 methods, were utilized to examine the consistency of the results and detect horizontal pleiotropy if any. We described assumptions and strengths of above methods in Table 1. Heterogeneity across estimates of SNPs for one association was assessed by Cochran's Q value. The MR‐Egger intercept test was used to examine horizontal pleiotropy (P < .05). Possible outliers were identified by MR‐PRESSO analysis. Given that sleep features, short sleep in particular, were associated with the risk of several digestive tract cancers, 27 we performed multivariable MR analysis with adjustment for genetically predicted sleep duration and genetic liability to having short sleep and insomnia to reduce the corresponding pleiotropy. Considering that high BMI is an important risk factor for digestive tract cancers, 5 we also conducted multivariable MR analysis with adjustment for genetically predicted BMI to assess potential mediating effects of BMI on digestive tract cancer risk. We used the same set of instrumental variables (317 SNPs) as the univariable MR analysis in multivariable MR analysis. Beta and SE coefficients of the associations of SNPs with genetic liability to chronotype, sleep traits or BMI and cancers were regressed to obtained multivariable MR estimates using the multivariable random‐effects multiplicative inverse variance weighted method. The Benjamini–Hochberg false discovery rate correction was used to account for multiple comparisons. 28 All tests were two‐sided and performed using the TwoSampleMR, MR‐PRESSO and MendelianRandomization packages in the R software (version 4.0.2).
TABLE 1.
Assumptions and strengths of used Mendelian randomization analyses
| Method | Assumptions | Strengths |
|---|---|---|
| The inverse variance weighted method | No unbalanced horizontal pleiotropy | Provides the most precise estimate if all instruments are valid |
| The weighted median method | More than 50% of weight from valid genetic instruments | Informs about the estimate supported by the majority of evidence |
| MR‐Egger regression | Associations of the genetic instruments with the exposure are uncorrelated with any pleiotropic effects of the instruments on the outcome | Provides consistent estimate under this assumption |
| MR‐PRESSO | The largest group of candidate instruments with similar estimates is the group of valid instrumental variables. | Detects outliers and provides estimate after removal of outliers |
| Contamination mixture method | Plurality of instruments are valid | Informs about the estimate supported by the plurality of evidence (ie, the estimate with the greatest amount of support) |
3. RESULTS
Genetic liability to morning chronotype was associated with a decreased risk of overall digestive tract cancer (odds ratio [OR] 0.95, 95% confidence interval [CI]: 0.90‐1.00), stomach cancer (OR 0.82, 95% CI: 0.68‐0.98), biliary tract cancer (OR 0.81, 95% CI: 0.66‐1.00) and colorectal cancer (OR 0.93, 95% CI: 0.86‐1.00) in the UK Biobank study (Figure 1). The associations for cancers of overall digestive tract, stomach and colorectum but not for biliary tract cancer were directionally consistent in the FinnGen study (Figure 1). In the combined analysis of the two data sources, genetic liability to morning chronotype was associated with a decreased risk of overall digestive tract cancer (OR 0.94, 95% CI: 0.90‐0.98), stomach cancer (OR 0.84, 95% CI: 0.73‐0.97) and colorectal cancer (OR 0.92, 95% CI: 0.87‐0.98). All three associations persisted after correction for multiple testing (Table S4). Genetic liability to being a morning person was not associated with cancers of the esophagus, liver or pancreas (Figure 1).
FIGURE 1.
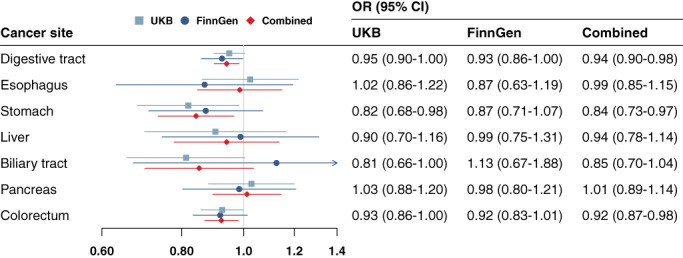
Associations of genetic liability to morning chronotype with risk of digestive tract cancers in the UK Biobank (UKB) and FinnGen study. CI, confidence interval; OR, odds ratio. The OR was scaled to genetically predicted one score increase in chronotype phenotype coded from −2 to 2, which indicates definitely evening to definitely morning [Color figure can be viewed at wileyonlinelibrary.com]
The associations remained consistent but with wider CIs in the sensitivity analyses (Table 2). Mild‐to‐moderate heterogeneity across SNPs' estimates was observed in all analyses. We observed no indication of horizontal pleiotropy in MR‐Egger intercept test (Table 2, P > .05). One outlier was identified in MR‐PRESSO analysis of colorectal cancer in UK Biobank and of biliary tract cancer in FinnGen; however, the associations were stable after removal of the outlier (Table 2). The associations remained stable in the analysis where estimate coefficients of SNP‐chronotype associations were obtained from only the 23andMe population (Table S5). The associations for overall digestive tract cancer, stomach cancer and colorectal cancer also remained stable in multivariable MR analysis with adjustment for genetically predicted sleep duration and BMI and genetic liability to having short sleep and insomnia (Table 3).
TABLE 2.
Associations of genetic liability to morning chronotype with digestive tract cancers in MR sensitivity analyses
| Cancer | Cases | Controls | Cochran's Q | P intercept | Weighted median | MR‐Egger | Contamination mixture | MR‐PRESSO | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | OR | 95% CI | P | |||||
| UK Biobank | ||||||||||||||||
| Digestive tract | 11 952 | 270 458 | 320 | .963 | 0.93 | 0.86‐1.01 | .099 | 0.95 | 0.81‐1.11 | .547 | 0.94 | 0.88‐1.00 | .078 | 0.95 | 0.90‐1.00 | .069 |
| Esophagus | 1339 | 366 203 | 368 | .835 | 1.11 | 0.85‐1.46 | .447 | 0.98 | 0.60‐1.59 | .921 | 1.05 | 0.78‐1.38 | .662 | 1.02 | 0.86‐1.22 | .789 |
| Stomach | 1086 | 366 456 | 332 | .530 | 0.82 | 0.62‐1.08 | .162 | 0.70 | 0.42‐1.17 | .179 | 0.66 | 0.49‐0.90 | .010 | 0.82 | 0.68‐0.98 | .033 |
| Liver | 503 | 367 039 | 300 | .710 | 0.80 | 0.53‐1.21 | .297 | 0.79 | 0.38‐1.65 | .535 | 0.61 | 0.20‐1.49 | .312 | 0.90 | 0.70‐1.16 | .433 |
| Biliary tract | 656 | 366 886 | 269 | .821 | 0.73 | 0.51‐1.04 | .082 | 0.76 | 0.40‐1.44 | .400 | 0.77 | 0.49‐1.07 | .129 | 0.81 | 0.66‐1.00 | .056 |
| Pancreas | 1414 | 366 128 | 310 | .937 | 1.09 | 0.84‐1.41 | .528 | 1.05 | 0.67‐1.62 | .842 | 1.23 | 0.99‐1.51 | .068 | 1.03 | 0.88‐1.20 | .722 |
| Colorectum | 7543 | 359 999 | 393 | .697 | 0.91 | 0.81‐1.01 | .077 | 0.96 | 0.78‐1.19 | .733 | 0.84 | 0.78‐0.92 | .001 | 0.92 | 0.85‐0.99 | .030 |
| FinnGen | ||||||||||||||||
| Digestive tract | 7638 | 204 070 | 301 | .675 | 0.91 | 0.81‐1.02 | .103 | 0.89 | 0.72‐1.09 | .258 | 0.92 | 0.84‐1.01 | .091 | 0.93 | 0.86‐1.00 | .041 |
| Esophagus | 358 | 204 070 | 294 | .440 | 0.68 | 0.40‐1.13 | .139 | 0.63 | 0.26‐1.52 | .302 | 0.34 | 0.21‐0.76 | .014 | 0.87 | 0.63‐1.19 | .387 |
| Stomach | 889 | 204 070 | 297 | .545 | 0.96 | 0.70‐1.33 | .813 | 1.03 | 0.58‐1.81 | .927 | 1.07 | 0.71‐1.58 | .789 | 0.87 | 0.71‐1.07 | .193 |
| Liver | 442 | 204 070 | 280 | .669 | 0.91 | 0.58‐1.43 | .687 | 0.84 | 0.38‐1.87 | .670 | 0.35 | 0.22‐1.43 | .076 | 0.99 | 0.75‐1.31 | .937 |
| Biliary tract | 157 | 204 070 | 340 | .131 | 1.37 | 0.64‐2.93 | .423 | 3.13 | 0.76‐12.9 | .116 | 0.00 | 0.00‐41.3 | NA | 1.16 | 0.70‐1.94 | .557 |
| Pancreas | 881 | 204 070 | 289 | .073 | 0.78 | 0.57‐1.06 | .117 | 0.60 | 0.34‐1.07 | .085 | 0.74 | 0.54‐1.02 | .068 | 0.98 | 0.80‐1.21 | .877 |
| Colorectum | 4401 | 204 070 | 305 | .763 | 0.94 | 0.81‐1.08 | .372 | 0.96 | 0.73‐1.25 | .738 | 0.84 | 0.76‐0.94 | .004 | 0.92 | 0.83‐1.01 | .090 |
Abbreviations: CI, confidence interval; OR, odds ratio.
Note: The P intercept is the P for MR‐Egger intercept test and a P intercept < .05 indicates horizontal pleiotropy. One outlier was identified in MR‐PRESSO analysis of colorectal cancer in UK Biobank and that of biliary tract cancer in FinnGen.
TABLE 3.
Results of multivariable MR analysis with adjustment for sleep duration, short sleep, insomnia and BMI in the meta‐analysis of UK Biobank and FinnGen
| Cancer | Model | OR | 95% CI | P value |
|---|---|---|---|---|
| Digestive tract cancer | Univariable MR | 0.94 | 0.90‐0.98 | .007 |
| MVMR adjusted for sleep duration | 0.94 | 0.90‐0.98 | .009 | |
| MVMR adjusted for short sleep | 0.94 | 0.90‐0.99 | .010 | |
| MVMR adjusted for insomnia | 0.94 | 0.90‐0.98 | .008 | |
| MVMR adjusted for BMI | 0.94 | 0.90‐0.98 | .008 | |
| Stomach cancer | Univariable MR | 0.84 | 0.73‐0.97 | .014 |
| MVMR adjusted for sleep duration | 0.84 | 0.74‐0.97 | .015 | |
| MVMR adjusted for short sleep | 0.84 | 0.73‐0.97 | .015 | |
| MVMR adjusted for insomnia | 0.84 | 0.73‐0.96 | .013 | |
| MVMR adjusted for BMI | 0.84 | 0.73‐0.96 | .013 | |
| Colorectal cancer | Univariable MR | 0.92 | 0.87‐0.98 | .009 |
| MVMR adjusted for sleep duration | 0.93 | 0.87‐0.98 | .013 | |
| MVMR adjusted for short sleep | 0.93 | 0.87‐0.98 | .013 | |
| MVMR adjusted for insomnia | 0.92 | 0.87‐0.98 | .012 | |
| MVMR adjusted for BMI | 0.93 | 0.87‐0.98 | .012 |
Abbreviations: BMI, body mass index; CI, confidence interval; MR, Mendelian randomization; MVMR, multivariable Mendelian randomization; OR, odds ratio.
4. DISCUSSION
We conducted an MR study to examine the associations between genetically proxied chronotype and risk of overall and six site‐specific digestive tract cancers in UK Biobank and FinnGen. We found robust inverse associations of genetic liability to morning chronotype with risk of overall digestive tract cancer, stomach cancer and colorectal cancer. The associations were consistent in both data sources and remained stable after adjustment for sleep duration, short sleep and insomnia. BMI appeared not to mediate the above associations. Of note, these findings relate to a naturally morning chronotype instead of a morning behavior (eg, an evening type may be forced to behave like a morning type due to social reasons such as work, despite sleeping hours).
As a novel health‐related factor, chronotype has been studied in relation to cancer risk in a few studies in recent decades. Observational evidence is consistent on the association between morning chronotype and reduced risk of breast and prostate cancers. 29 , 30 These associations were further strengthened in MR studies. 14 , 15 , 16 , 31 Being an early bird was also associated with the lower risk of other hormone‐related cancers, like ovarian and endometrial cancers, 32 , 33 and lung cancer. 34 However, little data were available on association between chronotype and digestive tract cancer. A case‐control study including a total of 318 participants found that patients with gastroenteropancreatic neuroendocrine tumors had a higher percentage of having evening chronotype compared to the healthy controls. 9 That study further showed that a higher chronotype score indicating a higher adherence to morningness was also associated with lower risk of metastasis, grading G2 and progressive disease. 9 Even though the study controlled for several important confounders, like age, sex and BMI, the observed associations might still be biased by residual confounding, which hindered the examination on the causal impact of chronotype on gastroenterological cancer. Our MR results supported this observational study and strengthened the causality of the inverse association between morning chronotype and digestive tract cancer. Notably, we further examined the associations with gastrointestinal tract cancers by site and found strong effects on stomach and colorectal cancers. We also observed an inverse association between morning chronotype and biliary tract cancer in UK Biobank, but not in the combined analysis, which was caused by the heterogeneous association observed in FinnGen. Thus, larger studies are needed to further explore the association between morning chronotype and biliary tract cancer.
Some underlying mechanisms in support of morningness and the reduced risk of digestive tract cancer have been proposed albeit scarcely examined. First, chronotype has been linked to the profile of gut microbiota that may influence the development of digestive tract cancer. 10 , 35 A detailed appraisal of mediation of gut microbiota in the association between chronotype and digestive tract cancer is of importance for clinical and therapeutic work. Second, genetic liability to morning chronotype has been associated with increased intake of foods known to constitute a healthy diet (eg, fresh fruit and bran cereals) and lower intake of unhealthy foods and beverages (eg, processed meat and beer). 36 Those foods are associated with risk of digestive tract cancers, particularly stomach and colorectal cancer. 37 , 38 Third, evening chronotype has been associated with DNA methylation of certain gene sites, like BACH2, JRK and RPS6KA2, which are related to the cancer development. 39 Fourth, evening chronotype may be associated with impaired metabolic homeostasis, like insulin resistance and increased levels of low‐density lipoprotein, 40 which have been associated with an increased risk of colorectal cancer. 41 , 42 In addition, increased levels of BMI have been proposed to be a possible mediator in the association between chronotype and digestive tract cancer since people with morning preference have a decreased frequency of obesity 43 that is a causal risk factor for digestive tract cancers. 5 However, we found no evidence that our findings were mediated by BMI.
Chronotype can be influenced by genetic and environmental factors including cultural and social influences, urban lifestyle, exposure to light, sleep schedule and so on. 44 Given the protective effects of a morning chronotype on several cancer outcomes, 14 , 15 , 16 , 31 strategies that formulate a morning type, like limiting evening screen time and maintaining a regular sleep schedule, should be promoted to reduce the disease burden of these cancers. In addition, chronotype may influence the disease risk via altering diet preference and pattern. 8 For example, individuals with an evening type were more likely to skip breakfast, delay mealtime and increase calorie intake during night and alcohol consumption compared to those with a morning chronotype. 7 Even though it is unclear that which diet‐related pathway mediates the association between chronotype and digestive tract cancer, this finding implies that (a) chronotype and diet information should be considered when estimating risk of digestive cancer; and (b) a diet intervention may be an efficient strategy to lower risk of digestive tract cancer among individuals with an evening chronotype.
The study has several strengths. The major one is MR design that strengthened the causal inference by minimizing confounding. We combined data from two large‐scaled biobanks, which increased the power of the analysis. In addition, the consistency of results from two sources indicated the robustness of our findings. We conducted multivariable MR analysis and ruled out the possibility that our MR results might be biased by pleiotropic effects of sleep‐related features. The current analysis was confined to the European population, which reduced the population structure bias. Several limitations deserve consideration when interpreting our results. First, the population confinement to the European population may limit the generalizability of our findings to other populations. Second, we may overlook the moderate associations due to inadequate power caused by a small number of cases for certain cancers even though we combined two data sources. Third, the interplay of chronotype and diet cannot be studied in our study based on summary‐level statistic data. 44
In summary, this MR study found the inverse associations between morning chronotype and digestive tract cancers, in particular cancers of stomach and colorectum. These findings suggest a causal role of being an early bird instead of a night owl in lowering digestive tract cancer. The mechanism behind these associations needs further study.
AUTHOR CONTRIBUTIONS
Shuai Yuan: Study conception and design; data acquisition and analysis; drafting the article and figures; reviewing the article. Amy M. Mason: Data acquisition and analysis; reviewing the article. Olga E. Titova: Reviewing the article. Mathew Vithayathil: Data acquisition and analysis; reviewing the article. Siddhartha Kar: Data acquisition and analysis; reviewing the article. Jie Chen: Reviewing the article. Xue Li: Reviewing the article. Stephen Burgess: Data acquisition and analysis; reviewing the article. Susanna C. Larsson: Study conception and design; data acquisition and analysis; reviewing the article. The work reported in the article has been performed by the authors, unless clearly specified in the text.
FUNDING INFORMATION
Our study was supported by funding from the Swedish Cancer Society (Cancerfonden) and by core funding from the: United Kingdom Research and Innovation Medical Research Council (MC_UU_00002/7), British Heart Foundation (RG/13/13/30194; RG/18/13/33946) and NIHR Cambridge Biomedical Research Centre (BRC‐1215‐20014) [*]. SCL further acknowledges research support from the Swedish Heart‐Lung Foundation (Hjärt‐Lungfonden) (20210351), the Swedish Research Council for Health, Working Life and Welfare (Forte); grant no. 2018‐00123 and the Swedish Research Council (Vetenskapsrådet); grant no. 2019‐00977. XL is supported by the Natural Science Fund for Distinguished Young Scholars of Zhejiang Province (LR22H260001). AMM is funded by the EU/EFPIA Innovative Medicines Initiative Joint Undertaking BigData@Heart grant 116074. SB is supported by a Sir Henry Dale Fellowship jointly funded by the Wellcome Trust and the Royal Society (204623/Z/16/Z). *The views expressed are those of the author(s) and not necessarily those of the NIHR or the Department of Health and Social Care.
CONFLICT OF INTEREST
The authors declare no conflicts of interest.
ETHICS STATEMENT
The UK Biobank received ethical permits from the Northwest Multi‐centre Research Ethics Committee, the National Information Governance Board for Health and Social Care in England and Wales and the Community Health Index Advisory Group in Scotland. All participants provided written informed consent. All studies included in cited genome‐wide association studies had been approved by a relevant review board. The present MR analyses were approved by the Swedish Ethical Review Authority (2019‐02793).
Supporting information
Appendix S1 Supporting Information.
ACKNOWLEDGEMENTS
Genetic association estimates were obtained from the UK Biobank study and the FinnGen study. Analyses of UK Biobank data were performed under application 29202.
Yuan S, Mason AM, Titova OE, et al. Morning chronotype and digestive tract cancers: Mendelian randomization study. Int J Cancer. 2023;152(4):697‐704. doi: 10.1002/ijc.34284
Funding information British Heart Foundation, Grant/Award Numbers: RG/13/13/30194, RG/18/13/33946; Swedish Cancer Society (Cancerfonden); NIHR Cambridge Biomedical Research Centre, Grant/Award Number: BRC‐1215‐20014; United Kingdom Research and Innovation Medical Research Council, Grant/Award Number: MC_UU_00002/7; Sir Henry Dale Fellowship jointly funded by the Wellcome Trust and the Royal Society, Grant/Award Number: 204623/Z/16/Z; EU/EFPIA Innovative Medicines Initiative Joint Undertaking BigData@Heart, Grant/Award Number: 116074; Natural Science Fund for Distinguished Young Scholars of Zhejiang Province, Grant/Award Number: LR22H260001; Swedish Research Council (Vetenskapsrådet), Grant/Award Number: 2019‐00977; Swedish Research Council for Health, Working Life and Welfare (Forte), Grant/Award Number: 2018‐00123; Swedish Heart‐Lung Foundation (Hjärt‐Lungfonden), Grant/Award Number: 20210351
DATA AVAILABILITY STATEMENT
This work has been conducted using the UK Biobank Resource. The UK Biobank is an open access resource and bona fide researchers can apply to use the UK Biobank dataset by registering and applying at http://ukbiobank.ac.uk/register-apply/. Further information is available from the corresponding author upon request.
REFERENCES
- 1. Arnold M, Abnet CC, Neale RE, et al. Global burden of 5 major types of gastrointestinal cancer. Gastroenterology. 2020;159:335‐349. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. O'Sullivan J, Lysaght J, Donohoe CL, Reynolds JV. Obesity and gastrointestinal cancer: the interrelationship of adipose and tumour microenvironments. Nat Rev Gastroenterol Hepatol. 2018;15:699‐714. [DOI] [PubMed] [Google Scholar]
- 3. Haas SL, Ye W, Löhr JM. Alcohol consumption and digestive tract cancer. Curr Opin Clin Nutr Metab Care. 2012;15:457‐467. [DOI] [PubMed] [Google Scholar]
- 4. Song C, Lv J, Liu Y, et al. Associations between hepatitis B virus infection and risk of all cancer types. JAMA Netw Open. 2019;2:e195718. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Vithayathil M, Carter P, Kar S, Mason AM, Burgess S, Larsson SC. Body size and composition and risk of site‐specific cancers in the UK Biobank and large international consortia: a mendelian randomisation study. PLoS Med. 2021;18:e1003706. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Sempere‐Rubio N, Aguas M, Faubel R. Association between chronotype, physical activity and sedentary behaviour: a systematic review. Int J Environ Res Public Health. 2022;19:9646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Mazri FH, Manaf ZA, Shahar S, Mat Ludin AF. The association between chronotype and dietary pattern among adults: a scoping review. Int J Environ Res Public Health. 2019;17:68. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8. Srour B, Plancoulaine S, Andreeva VA, et al. Circadian nutritional behaviours and cancer risk: new insights from the NutriNet‐santé prospective cohort study: disclaimers. Int J Cancer. 2018;143:2369‐2379. [DOI] [PubMed] [Google Scholar]
- 9. Barrea L, Muscogiuri G, Pugliese G, et al. Chronotype: what role in the context of gastroenteropancreatic neuroendocrine tumors? J Transl Med. 2021;19:324. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Carasso S, Fishman B, Lask LS, Shochat T, Geva‐Zatorsky N, Tauber E. Metagenomic analysis reveals the signature of gut microbiota associated with human chronotypes. FASEB J. 2021;35:e22011. [DOI] [PubMed] [Google Scholar]
- 11. Meng C, Bai C, Brown TD, Hood LE, Tian Q. Human gut microbiota and gastrointestinal cancer. Genom Proteom Bioinf. 2018;16:33‐49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12. Feng Q, Liang S, Jia H, et al. Gut microbiome development along the colorectal adenoma‐carcinoma sequence. Nat Commun. 2015;6:6528. [DOI] [PubMed] [Google Scholar]
- 13. Burgess S, Thompson SG. Mendelian Randomization: Methods for Using Genetic Variants in Causal Estimation. London, UK: Chapman and Hall/CRC; 2015. [Google Scholar]
- 14. Hayes BL, Robinson T, Kar S, et al. Do sex hormones confound or mediate the effect of chronotype on breast and prostate cancer? A Mendelian randomization study. PLoS Genet. 2022;18:e1009887. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15. Chen F, Wen W, Long J, et al. Mendelian randomization analyses of 23 known and suspected risk factors and biomarkers for breast cancer overall and by molecular subtypes. Int J Cancer. 2022;151:372‐380. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Sun X, Ye D, Jiang M, Qian Y, Mao Y. Genetically proxied morning chronotype was associated with a reduced risk of prostate cancer. Sleep. 2021;44:zsab104. [DOI] [PubMed] [Google Scholar]
- 17. Kurki MI, Karjalainen J, Palta P, et al. FinnGen: Unique genetic insights from combining isolated population and national health register data. medRxiv. 2022. doi: 10.1101/2022.03.03.22271360. [DOI] [Google Scholar]
- 18. Jones SE, Lane JM, Wood AR, et al. Genome‐wide association analyses of chronotype in 697,828 individuals provides insights into circadian rhythms. Nat Commun. 2019;10:343. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Clarke L, Zheng‐Bradley X, Smith R, et al. The 1000 genomes project: data management and community access. Nat Methods. 2012;9:459‐462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20. Dashti HS, Jones SE, Wood AR, et al. Genome‐wide association study identifies genetic loci for self‐reported habitual sleep duration supported by accelerometer‐derived estimates. Nat Commun. 2019;10:1100. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Lane JM, Jones SE, Dashti HS, et al. Biological and clinical insights from genetics of insomnia symptoms. Nat Genet. 2019;51:387‐393. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Pulit SL, Stoneman C, Morris AP, et al. Meta‐analysis of genome‐wide association studies for body fat distribution in 694 649 individuals of European ancestry. Hum Mol Genet. 2019;28:166‐174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Bowden J, Davey Smith G, Haycock PC, Burgess S. Consistent estimation in Mendelian randomization with some invalid instruments using a weighted median estimator. Genet Epidemiol. 2016;40:304‐314. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. Bowden J, Davey Smith G, Burgess S. Mendelian randomization with invalid instruments: effect estimation and bias detection through egger regression. Int J Epidemiol. 2015;44:512‐525. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25. Verbanck M, Chen CY, Neale B, Do R. Detection of widespread horizontal pleiotropy in causal relationships inferred from Mendelian randomization between complex traits and diseases. Nat Genet. 2018;50:693‐698. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26. Burgess S, Foley CN, Allara E, Staley JR, Howson JMM. A robust and efficient method for Mendelian randomization with hundreds of genetic variants. Nat Commun. 2020;11:376. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27. Titova OE, Michaëlsson K, Vithayathil M, et al. Sleep duration and risk of overall and 22 site‐specific cancers: a Mendelian randomization study. Int J Cancer. 2021;148:914‐920. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc B Methodol. 1995;57:289‐300. [Google Scholar]
- 29. Papantoniou K, Castaño‐Vinyals G, Espinosa A, et al. Night shift work, chronotype and prostate cancer risk in the MCC‐Spain case‐control study. Int J Cancer. 2015;137:1147‐1157. [DOI] [PubMed] [Google Scholar]
- 30. Papantoniou K, Castaño‐Vinyals G, Espinosa A, et al. Breast cancer risk and night shift work in a case‐control study in a Spanish population. Eur J Epidemiol. 2016;31:867‐878. [DOI] [PubMed] [Google Scholar]
- 31. Richmond RC, Anderson EL, Dashti HS, et al. Investigating causal relations between sleep traits and risk of breast cancer in women: mendelian randomisation study. BMJ. 2019;365:l2327. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32. Costas L, Frias‐Gomez J, Benavente Moreno Y, et al. Night work, chronotype and risk of endometrial cancer in the screenwide case‐control study. Occup Environ Med. 2022;79:624‐627. [DOI] [PubMed] [Google Scholar]
- 33. Leung L, Grundy A, Siemiatycki J, et al. Shift work patterns, chronotype, and epithelial ovarian cancer risk. Cancer Epidemiol Biomarkers Prev. 2019;28:987‐995. [DOI] [PubMed] [Google Scholar]
- 34. Xie J, Zhu M, Ji M, et al. Relationships between sleep traits and lung cancer risk: a prospective cohort study in UK Biobank. Sleep. 2021;44:zsab089. [DOI] [PubMed] [Google Scholar]
- 35. Yachida S, Mizutani S, Shiroma H, et al. Metagenomic and metabolomic analyses reveal distinct stage‐specific phenotypes of the gut microbiota in colorectal cancer. Nat Med. 2019;25:968‐976. [DOI] [PubMed] [Google Scholar]
- 36. Dashti HS, Chen A, Daghlas I, Saxena R. Morning diurnal preference and food intake: a Mendelian randomization study. Am J Clin Nutr. 2020;112:1348‐1357. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Vingeliene S, Chan DSM, Vieira AR, et al. An update of the WCRF/AICR systematic literature review and meta‐analysis on dietary and anthropometric factors and esophageal cancer risk. Ann Oncol. 2017;28:2409‐2419. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38. Vieira AR, Abar L, Chan DSM, et al. Foods and beverages and colorectal cancer risk: a systematic review and meta‐analysis of cohort studies, an update of the evidence of the WCRF‐AICR continuous update project. Ann Oncol. 2017;28:1788‐1802. [DOI] [PubMed] [Google Scholar]
- 39. Adams CD, Jordahl KM, Copeland W, et al. Nightshift work, chronotype, and genome‐wide DNA methylation in blood. Epigenetics. 2017;12:833‐840. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 40. Lotti S, Pagliai G, Colombini B, Sofi F, Dinu M. Chronotype differences in energy intake, cardiometabolic risk parameters, cancer, and depression: a systematic review with meta‐analysis of observational studies. Adv Nutr. 2022;13:269‐281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Carter P, Vithayathil M, Kar S, et al. Predicting the effect of statins on cancer risk using genetic variants from a Mendelian randomization study in the UK Biobank. Elife. 2020;9:e57191. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Murphy N, Song M, Papadimitriou N, et al. Associations between glycemic traits and colorectal cancer: a Mendelian randomization analysis. J Natl Cancer Inst. 2022;114:740‐752. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Muscogiuri G, Barrea L, Aprano S, et al. Chronotype and adherence to the Mediterranean diet in obesity: results from the opera prevention project. Nutrients. 2020;12:12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 44. Almoosawi S, Vingeliene S, Gachon F, et al. Chronotype: implications for epidemiologic studies on chrono‐nutrition and cardiometabolic health. Adv Nutr. 2019;10:30‐42. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Appendix S1 Supporting Information.
Data Availability Statement
This work has been conducted using the UK Biobank Resource. The UK Biobank is an open access resource and bona fide researchers can apply to use the UK Biobank dataset by registering and applying at http://ukbiobank.ac.uk/register-apply/. Further information is available from the corresponding author upon request.