

ABSTRACT
Levels of women’s empowerment (WE) can contribute to differences in infant mortality rates (IMRs) across cities. We used a cross-sectional multilevel study to examine associations of WE with IMRs across 286 cities in seven Latin American countries. We estimated IMRs for 2014–2016 period and combined city socioeconomic indicators into factors reflecting living conditions and service provision. WE was operationalized: (1) in cities, by using scores for women’s labor force participation (WLFP) and educational attainment among women derived from education and employment indicators disaggregated by sex; (2) in countries, by including a scale of enforcements of laws related to women’s rights. We estimated adjusted percent differences in IMRs associated with higher WE scores across all cities and stratified by country GDP. We found substantial heterogeneity in IMRs and WE across cities. Higher WLFP was associated with lower IMRs. Higher women’s educational attainment was associated with lower IMRs only in cities from countries with lower GDP. Poorer national enforcement of laws protecting women’s rights was associated with higher IMRs in all countries. Women’s empowerment could have positive implications for population health. Fostering women’s socioeconomic development and girls’ education should be part of strategies to reduce IMRs in cities of Global South.
KEYWORDS: Women’s empowerment, infant mortality, Latin America
Background
As urban populations worldwide continue to grow, it has become increasingly important to identify how urban policies and programs can be leveraged to improve health in cities (Ezzati et al. 2018). Infant mortality is a key indicator of population health. Despite past evidence that infant mortality rates (IMRs) are lower in urban than in rural areas (de Carvalho and Wood 1978) important differences in IMRs exist both between and within cities (Kimani-Murage et al. 2014). Few studies have directly examined variations on IMRs across cities and its predictors.
A critical factor in promoting infant health is the status of women (Varkey and Lesnick 2010). Higher educational attainment in women of reproductive age has been linked to a reduction in IMRs at the country level, through reductions in adolescent birth rates and premature births (Gakidou et al. 2010), and through improvement in women’s skills as caregivers (Heaton 2015). Women with more financial autonomy appear to allocate more resources to their children’s health (Pratley 2016). In addition to effects on childbearing and childrearing, women’s social status is linked to women’s participation in political decision-making which has positive impacts on population levels of education (Clots-Figueras 2012) child welfare (Quamruzzaman and Lange 2016, Hessel et al. 2020), and the formulation of social policies that benefit living conditions in children (UN 2005).
Actions supporting women’s development have not taken place in the same way across countries and cities. Although women in cities are more likely to perceive some advantages over their rural counterparts in terms of employment and education (ECLAC 2016), women from lower socio- economic positions, in particular, remain more economically vulnerable and are more susceptible to ambient risks present in marginalized areas in urban settings, as they are more likely to remain at home or work near the place where they live (Chant 2013).
To date, evidence on effects of women’s empowerment on child’s health have been described mostly at national levels and involving cross-countries comparison (Pratley 2016, Macmillan et al. 2018). These approaches, however, are limited in accounting for the heterogeneity in women’s empowerment across what are often very diverse urban areas.
Latin America with its very high levels of urbanization and its many diverse cities provides a unique opportunity to understand the contributions of women’s empowerment to differences in IMRs across urban areas. The region has recently experienced significant emergence in feminist grass-roots movements in response to the unequal socioeconomic conditions and access to resources that women experience, particularly in large urban areas (Gasparini and Marchionni 2015). In this study we examine whether differences in measures of women’s empowerment are related to variability in IMRs across cities in Latin America and whether these relationships persist after accounting for other predictors of infant mortality in cities.
Methods
Sample
Data were drawn from the SALURBAL project, which included a total of 371 cities of 100,000 or more inhabitants in 2010 in 11 countries. Cities were defined as a single administrative unit or combination of adjacent administrative units (i.e. municipios, comunas, partidos, delegaciones, cantones, or corregimientos) that were part of the urban extent as determined from satellite imagery (Quistberg et al. 2019). For this study, we included cities for which vital statistics registries were available for 2014 to 2016 and had good quality death registrations (mortality coverage >90%) based on a separate analysis of adult mortality (Bilal et al. 2019). Of the 371 cities, 11 cities (5 cities in Nicaragua, and 3 cities in El Salvador and Guatemala, respectively) were excluded due to lack of vital statistics registries for the years of study; and 74 cities (9 cities in Brazil, 19 in Colombia, 31 in Mexico and 15 in Peru) were excluded because of mortality coverage <90%, leaving for analysis 286 cities located in Argentina, Brazil, Chile, Colombia, Costa Rica, Mexico, Peru, and Panama. Cities with inadequate mortality coverage had poorer living conditions and lower provision of water connected to public network compared to cities included in this study (see Supplementary material).
Outcome
Infant mortality rates (IMRs). We calculated IMRs (deaths less than 1 year of age per 1000 live births) for the period 2014–2016. Deaths and live births were retrieved based on deceased’s and maternal place of residence, respectively. Three years were pooled to increase stability of the estimates.
Exposures
Women’s empowerment (WE)
WE in cities was operationalized by retrieving indicators of education and employment disaggregated by sex from national censuses. We retrieved a total of 8 socioeconomic indicators and conducted principal component analyses (PCA) in order to identify distinct sets that could be combined into scores. The PCA identified two different domains that incorporated 6 of the 8 indicators. Variables related to school attendance were dropped as they were not related to the rest of the variables. Each indicator was standardized to a mean of zero and standard deviation (SD) of one and values for different indicators were added together to create two women’s empowerment scores:
Women’s labor force participation (WLFP), which describes aspects of women’s socio-economic position and also accounts for gender inequalities in education and employment (Howe et al. 2012, Chant 2013, ECLAC 2016). It includes the female-to-male ratio of the proportion of population aged 25 or older who completed secondary education or above, and the female-to-male ratio of the proportion of the population who completed university degree or above; labor force participation among females 15 years or older; and the ratio of the labor force participation rate among females to the labor force participation rate among males. Higher score values signify greater participation of women in labor force and greater education of women relative to men.
Educational attainment among women (EAW) which includes the proportion of the female population aged 25 or older with complete high school or above and the proportion of the female population aged 25 year or older with complete university degree or above. Higher score values signify greater education achievement among women.
We also included a scale developed by the Women’s Stats Project measuring the degree to which countries have and enforce laws supporting women’s rights (country law enforcement scale or CLE scale), including education, family, and physical security (Women Stats Projects-Codebook 2019). We included the scale for year 2015. Values range from 0 to 4, with lower values signifying higher level of country enforcement.
Other covariates
Urban social environment
We included two urban social environment scores also based on PCA on a total of eight variables that were identified to be related with infant mortality in previous work (Ortigoza et al. 2020).
Score of living conditions which includes (1) percentage of household with piped water inside the dwelling, as a marker of house conditions; (2) percentage of households with overcrowding conditions (more than 3 people per room, excluding kitchen and bathroom); and (3) percentage of population aged 15–17 attending school, as a marker of social marginalization, since low school attendance among adolescents has been linked to poverty and early participation in the labor market, as well as exclusion from productive systems (Cardenas et al. 2015, Bodenhorn 2006), We reverse coded the overcrowding indicator so higher score values signify better living conditions and lower poverty levels.
Score of service provisions, which include public services that cities provide to dwellings, include (1) percent of households with access to water source from a municipal public or private water network and (2) percentage of households with sewage system connected to a municipal public or private sewage network. Higher score values signify better service provision in cities.
Vaccine coverage in infant population
City coverage of first dose of triple viral vaccine (MMR1, measles-mumps-rubella vaccine) among the population of children 1 year of age was used as a proxy of health care access among infants. MMR1 presents a schedule that is similar across countries and made it suitable for harmonization (PAHO 2019). Data for year 2016 was provided by World Health Organization (WHO 2019).
National gross domestic product per capita (GDP per capita)
We retrieved the national Real GDP (output-based) per population for 2015 for each country from Penn World Tables (Feenstra et al. 2019) and use the median value of the sample (15,530.7 US$) to categorize countries in two groups: above and below the median GDP per capita.
Statistical analysis
We first described variations in IMRs, and WE measures across cities within countries as well as the distribution of city level covariates across categories of city-level measures of WE. We then estimated the association of women’s empowerment predictors with IMRs using Poisson multilevel models (cities nested within countries). Each WE predictor was first explored separately and then included in a multivariable model with all predictors together. In order to determine associations of women’s empowerment measures with IMRs independently from other city-characteristics, we adjusted the final model for SE scores and MMR1 coverage. We explored effect modification by country GDP per capita, by repeating the same modelling sequence in countries with GDP per capita above and below the median value of the sample, and then by testing interactions between GDP per capita and city-level predictors.
Results
Figure 1 shows the distribution of women’s empowerment measures across cities. Women’s empowerment scores varied across countries but there was also substantial variation across cities within each country. For IMRs, the greatest heterogeneity is observed across cities within countries. The intra class correlation (ICC) was 0.43 implying that 57% of the total variance in IMRs was across cities within countries. For women’s empowerment measures, differences across countries were greater for women’s labor force participation score (ICC = 0.83) than for women’s educational attainment score (ICC = 0.63).
Figure 1.
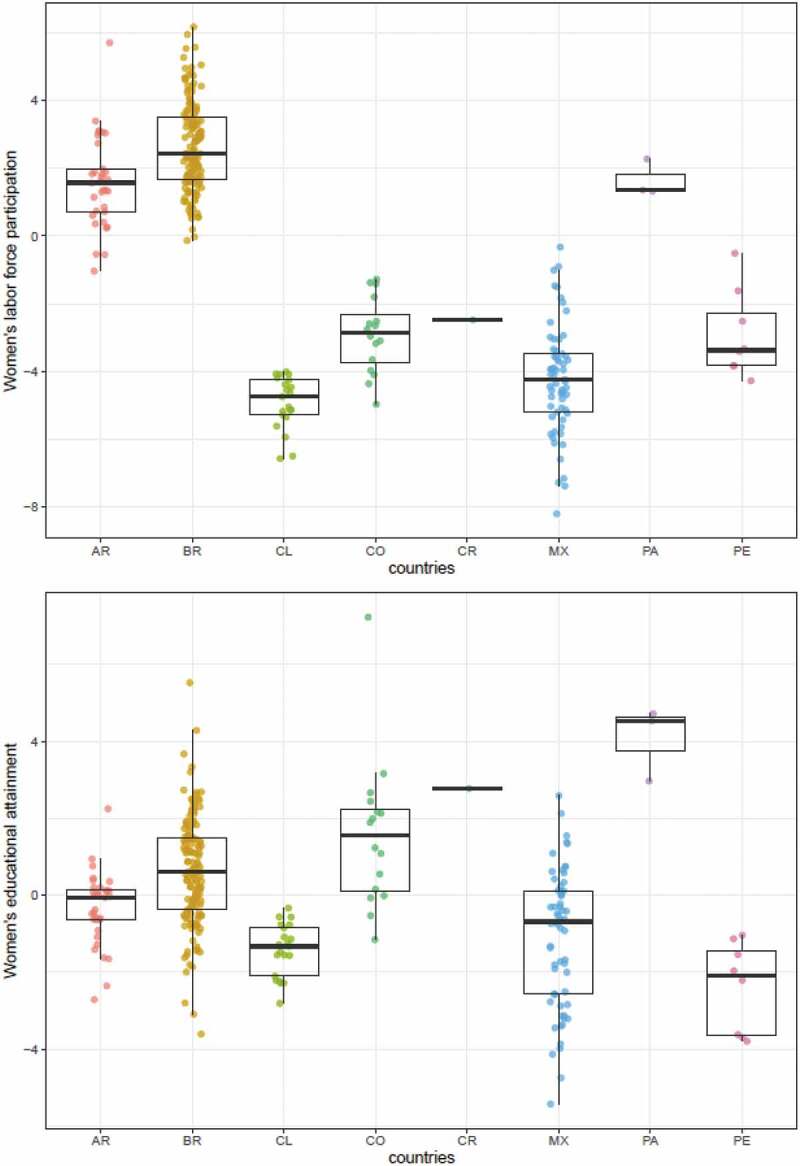
Distribution of women’s empowerment in cities by country (n = 286 cities).
Each dot represents a city-estimate of women’s labor force participation score (above) and women’s educational attainment score (below), and boxplots show its country median and range distribution. Scores were created based on z-score indicators, so that zero value represents the mean value of each measure. Ref: AR = Argentina; BR = Brazil, CL = Chile; CO = Colombia; CR = Costa Rica; MX = Mexico; PA = Panama; PE = Peru.
Selected characteristics of cities included in analyses by quartiles of women’s labor force participation score are shown in Table 1. All cities in Chile had levels of women’s labor force participation in the lowest quartile and all cities in Costa Rica and Panama were in middle quartiles. Cities in Colombia, Mexico and Peru were in the middle- to lower quartiles of women’s labor force participation while cities in Argentina and Brazil were in the mid -higher quartiles. Cities with low levels of women’s labor force participation had significantly lower proportion of population with adequate living conditions compared to the rest of the cities (Table 1). Cities in the lowest quartile of women’s labor force participation also showed significantly lower mean levels of women’s education than other cities: 32.8% and 9.4% for complete high school or more and complete university or more, respectively, compared to around 40% and 13% in the rest of the cities. Mean level of MMR1 coverage in the sample was 91.3% and did not differ by quartiles of women’s labor force participation. Mean IMR was 11.2 deaths per 1000 live births and IMRs were lowest in the lowest quartile of women’s labor force participation (Table 1).
Table 1.
City demographic and socio-economic characteristics by quartiles of women’s labor force participation score (n = 286 cities).
| Total |
Women’s Labor Force Participation Score |
||||
|---|---|---|---|---|---|
| n (% of sample) or mean (SD) | <P25 | P25–P75 | >P75 | p-value | |
| Overall number of cities n (%) | 286 | 71 (24.8%) | 144 (50.3%) | 71 (24.8%) | |
| Number of cities by country n (col%) | |||||
| Argentina | 33 (11.5%) | – | 26 (18.1%) | 7 (9.9%) | |
| Brazil | 143 (50.4%) | – | 79 (54.9%) | 64 (90.1%) | |
| Chile | 21 (7.3%) | 21 (29.6%) | – | – | |
| Colombia | 16 (5.6%) | 5 (7.0%) | 11 (7.6%) | – | |
| Costa Rica | 1 (0.3%) | – | 1 (0.7%) | – | |
| México | 61 (21.3%) | 42 (59.2%) | 19 (13.2%) | – | |
| Panama | 3 (1.0%) | – | 3 (2.1%) | – | |
| Peru | 8 (2.8%) | 3 (4.2%) | 5 (3.5%) | – | |
| Socio-economic predictors by domain, mean (SD) | |||||
| Living conditions | |||||
| % of households with piped water in the dwelling | 89.8 (11.6) | 81.5 (15.6) | 92.1 (8.6) | 93..3 (7.3) | <0.0001 |
| % of households with overcrowding in the house a | 4.8 (3.9) | 8.0 (4.4) | 4.2 (3.3) | 2.9 (2.2) | <0.0001 |
| % of population 15–17 attending school | 80.3 (7.5) | 73.9 (8.9) | 81.8 (6.4) | 83.6 (3.4) | <0.0001 |
| Score | −0.04 (0.7) | −0.61 (0.7) | 0.09 (0.6) | 0.26 (0.3) | <0.0001 |
| Service provision | |||||
| % of households with water connected to municipal network | 90.0 (10.6) | 91.1(9.5) | 91.4 (8.0) | 85.8 (14.6) | <0.0001 |
| % of households with sewage system connected to municipal network | 70.0 (25.2) | 80.9 (20.7) | 71.4 (23.1) | 56.2 (27.3) | <0.0001 |
| Score | −0.04 (0.4) | 0.09 (0.3) | 0.003 (0.3) | −0.26 (0.4) | <0.0001 |
| Women Empowerment measures, mean (SD) | |||||
| Education and labor force participation compared to men | |||||
| Ratio female/male in education achievement for complete high school level or above b | 1.03 (0.1) | 0.91 (0.1) | 1.03 (0.1) | 1.14 (0.1) | <0.0001 |
| Ratio female/male in education achievement for complete university or above c | 1.07 (0.2) | 0.76 (0.1) | 1.08 (0.2) | 1.34 (0.2) | <0.0001 |
| Labor force participation among women d | 49.8 (9.7) | 37.8 (4.6) | 51.7 (6.9) | 58.1 (5.9) | <0.0001 |
| Ratio female/male in labor force participatione | 0.66 (0.1) | 0.51 (0.1) | 0.68 (0.1) | 0.75 (0.1) | <0.0001 |
| Education achievement among women | |||||
| % of women 25+ who completed high school or above f | 38.4 (7.4) | 32.8 (8.0) | 40.3 (5.8) | 40.3 (6.5) | <0.0001 |
| % of women 25+ who completed university or above g | 12.7 (4.7) | 9.4 (5.0) | 14.3 (4.3) | 12.9 (3.6) | <0.0001 |
| Score | 0.09 (0.4) | −0.24 (0.3) | 0.22 (0.3) | 0.15 (0.3) | <0.0001 |
| MMR1 coverageh, mean % (SD) | 91.3 (13.8) | 94.3 (6.2) | 90.5 (15.0) | 89.9 (16.1) | 0.09 |
| Overall Infant mortality ratei, mean (SD) | 11.2 (2.8) | 10.9 (3.4) | 11.0 (2.2) | 12.0 (2.8) | 0.01 |
aOvercrowding is defined as more than 3 people per room, excluding kitchen and bathroom in a household. bDescribes the ratio of the female to the male proportion of the population aged 25 or above who completed high school or above. cDescribes the ratio of the female to the male proportion of the population aged 25 or above who completed university or above. dDescribes % of women ≥15 years who are part of the labor force among all women ≥15 years (employed or unemployed). eDescribes the ratio between female labor force participation rate and male labor force participation rate in population older than 15 years of age. fDescribes the % female population of 25 years or above with complete high school or above among overall female population of 25 years or above. gDescribes the % female population of 25 years or above with complete university level or above among overall female population of 25 years or above. hDescribes the % of children at age 1 who received the first dose of measles-mumps-rubella vaccine among overall population at age of 1. iInfant Mortality rate = number of infant deaths per 1000 live births.
Table 2 shows percent differences in IMRs associated with a one SD higher WE and SE scores, one-unit higher CLE scale, and 1% higher MMR1 vaccine coverage. In the unadjusted analyses, only the score of educational attainment among women and CLE scale showed significant associations with IMRs (models 2 and 3). In the final model (model 5), a higher score of women’s labor force participation and a higher value on the CLE scale were both significantly associated with IMRs: a one SD higher score of women’s participation in labor force was associated with 6.1% (95% CI −11.1 –0.8%) lower IMRs, and a one unit higher in CLE scale (less enforcement) was associated with a 16.6% (95% CI 3.6 31.4) higher IMR, after accounting for SE scores and MMR1 coverage (model 5). Better living conditions and better service provision were also associated with lower IMRs in the full model. The country random intercept remained statistically significant in all models suggesting the persistence of unexplained variation across countries even after city level factors were accounted for (Table 2). City-level factors explained part of the variability in IMRs across countries, as evidenced by a decrease in the country variance from 0.04 in the null model to 0.02 in the final model (model 5).
Table 2.
Estimated percent differences in IMRs associated with city- and country-level predictors (n = 286 cities).
| Model 1 |
Model2 |
Model 3 |
Model 4 |
Model 5 |
||||||
|---|---|---|---|---|---|---|---|---|---|---|
| % |
95% |
% |
95% |
% |
95% |
% |
95% |
% |
95% |
|
| Diff | CI | Diff | CI | Diff | CI | Diff | CI | Diff | CI | |
| Women’s labor force participation scorea | −5.9 | −20.5 11.3 | −4.5 | −17.5 10.4 | −6.1 | −11.1 −0.8 | ||||
| Educational attainment among women scoreb | −9.9 | −15.1 −4.3 | −9.4 | −17.5 −0.5 | −0.7 | −7.0 6.2 | ||||
| CLE scale 2015c | 16.8 | 1.7 34.3 | 20.2 | 3.0 40.4 | 16.6 | 3.6 31.4 | ||||
| Living conditions scored | −11.9 | −18.5 −4.9 | ||||||||
| Services provision scoree | −10.6 | −15.8 −5.2 | ||||||||
| MMR1 coveragef | −0.1 | −0.2 0.1 | ||||||||
| Variance | Estimate | SE | Estimate | SE | Estimate | SE | Estimate | SE | Estimate | SE |
| Country intercept | 0.05 | 0.02 | 0.04 | 0.02 | 0.02 | 0.01 | 0.03 | 0.01 | 0.02 | 0.004 |
Null model variance, mean (SD) = 0.04 (0.02).Note: Bold numbers are indicating statistically significant results for alpha level <0.05. Estimates corresponds to percent differences in IMRs for 1 SD higher scores of women’s labor force participation, women’s educational attainment, living conditions, and services provision; and for 1% higher MMR1 coverage and 1 point-higher CLE scale. aWomen’s labor force participation score includes the female to the male proportion of the population aged 25 or above who completed high school or above; the female to the male proportion of the population aged 25 or above who completed university degree or above; % of women ≥15 years who are part of the labor force among all women ≥15 years (employed or unemployed); ratio between female labor force participation rate and male labor force participation rate in population older than 15 years of age. bEducational attainment among women score includes % female population with high school level or above among female population aged 25 years or above, % of female population with complete university degree or above among female population aged 25 years or above. cCountry law enforcement (CLE) scale is defined as the degree to which countries have and enforce laws supporting women’s rights, including education, family, and physical security. Scale ranges 0–4: Scale reference: (0) The laws are well enforced by the government; and is a high priority of the government; (1) laws are mostly enforced, and the government appears to be fairly proactive; (2) spotty enforcement of laws; the government may or may not signal its interest; (3) little effective enforcement; improving the situation of women appears to be a low priority for the government; (4) virtually no enforcement of laws, or such laws do not even exist. dLiving conditions Score includes % of households with piped water in the dwelling, % of households with overcrowding (3+ per room) in the house, and % of population 15–17 attending school. eServices provision Score includes: % of households with water connected to municipal network, and % of households with sewage system connected to municipal network. fMMR1 coverage represents the percentage of children at age 1 who received the first dose of measles-mumps-rubella vaccine among overall population at age of 1.
When countries were grouped by the value of GDP per capita (Table 3), higher scores of women’s labor force participation were associated with lower IMRs in countries below and above the GDP per capita median. The association was stronger in countries above the median GDP per capita, but the interaction was not statistically significant. Higher scores for living conditions were significantly and similarly associated with lower IMRs in countries above and below the median GDP per capita. In contrast, women’s educational attainment and service provision were only associated with lower IMRs in countries with GDP per capita below the median: the percent difference in IMRs per one SD higher score was −3.6% (95% CI −6.3 −0.9) for women’s educational attainment and −12.6% (95% CI −13.5 −11.7) for service provision (Table 3).
Table 3.
Estimated percent differences in IMRs for city and country-level predictors by country’s GDP/capita.
| Countries below median GDPg |
Countries above median GDPh |
Test for interaction* |
|||||
|---|---|---|---|---|---|---|---|
| n = 168 cities |
N = 118 cities |
||||||
| % difference | 95% CI | % difference | 95% CI | p-value | |||
| Women’s labor force participation scorea | −5.8 | −10.0 | –1.4 | −14.6 | −17.6 | −11.5 | 0.26 |
| Educational attainment among women scoreb | −3.6 | −6.3 | –0.9 | 7.8 | −3.1 | 20.0 | 0.02 |
| CLE score 2015c | 34.0 | −13.9 | 108.5 | 13.7 | −29.0 | 82.0 | 0.32 |
| Living conditions scored | −15.1 | −22.0 | –7.4 | −12.9 | −16.7 | −9.0 | 0.03 |
| Services provision scoree | −12.6 | −13.5 | –11.7 | 4.9 | −5.1 | 16.0 | <0.0001 |
| MMR1 coveragef | −0.1 | −0.1 | 0.01 | −0.2 | −0.9 | 0.6 | 0.91 |
Note:Bold numbers are indicating statistically significant results for alpha level <0.05. Estimates corresponds to percent differences in IMRs for 1 SD higher scores of women’s labor force participation, women’s educational attainment, living conditions, and services provision; and for 1% higher MMR1 coverage and 1 point-higher CLE scale. *Each interaction was tested separately along with the full model. aWomen’s labor force participation score includes the female to the male proportion of the population aged 25 or above who completed high school or above; the female to the male proportion of the population aged 25 or above who completed university degree or above; % of women ≥15 years who are part of the labor force among all women ≥15 years (employed or unemployed); ratio between female labor force participation rate and male labor force participation rate in population older than 15 years of age. bEducational attainment among women score includes % female population with high school level or above among female population aged 25 years or above, % of female population with complete university degree or above among female population aged 25 years or above. cCountry law enforcement (CLE) scale is defined as the degree to which countries have and enforce laws supporting women’s rights, including education, family, and physical security. Scale ranges 0–4: Scale reference: (0) The laws are well enforced by the government; and is a high priority of the government; (1) laws are mostly enforced, and the government appears to be fairly proactive; (2) spotty enforcement of laws; the government may or may not signal its interest; (3) little effective enforcement; improving the situation of women appears to be a low priority for the government; (4) virtually no enforcement of laws, or such laws do not even exist. dLiving conditions Score includes % of households with piped water in the dwelling, % of households with overcrowding (3+ per room) in the house, and % of population 15–17 attending school. eServices provision Score includes: % of households with water connected to municipal network, and % of households with sewage system connected to municipal network. fMMR1 coverage represents the percentage of children at age 1 who received the first dose of measles-mumps-rubella vaccine among overall population at age of 1. gCountries with GDP/capita below the median (15,530.7 US$) are Brazil, Colombia, Costa Rica, and Peru. hCountries with GDP/capita above the median (15,530.7 US$) are Argentina, Chile, Mexico, and Panama.
Discussion
In this study of 286 Latin American cities, we found significant heterogeneity across cities in both IMRs and women’s empowerment. Higher women’s participation in the work force was linked to lower IMRs, independently of the level of health care coverage and socioeconomic conditions. Lower enforcement of laws related to women’s rights was related to higher IMRs. These associations were observed in countries below and above the median GDP per capita. However, GDP per capita modified the associations between IMRs and women’s educational attainment, such that a significant and negative association with IMRs was observed only in countries with GDP per capita below the median.
We found that heterogeneity in women’s empowerment measures across cities within countries was greater for women’s educational attainment than for women’s labor force participation. Women’s participation in labor force could be influenced by cultural and gender – role patterns that may differ more across countries than across cities within countries. The great heterogeneity observed in women’s educational attainment and in IMRs across cities within countries highlights the importance of examining features of cities as drivers of both access to women’s education (Beall 1996) and IMRs (Ortigoza et al. 2020).
In our study a one SD higher score of women’s labor force participation was associated with 6% lower IMRs. Similar associations have been reported in the United States: state measures of women’s employment and earnings were associated with lower infant mortality and teen birth rates after accounting for income inequality and state racial composition (Koenen et al. 2006). To our knowledge, ours is the first study to investigate these associations at the city level and across a large sample of cities in lower and middle-income countries.
A higher participation of women in the labor market has been described as an important contributor to the reduction of poverty and inequality in Latin America, particularly in urban areas where there is an increasing proportion of women-headed households (Gasparini and Marchionni 2015, ECLAC 2016). It has been posited that women with access to paid work and corresponding income make decisions regarding household expenditures and savings that are more oriented to children, which eventually contribute to better nutrition, care, and long-term human capital accumulation (Smith et al. 2004, Gasparini and Marchionni 2015). The increasing participation of women in the labor market has also been linked to decreasing natality and fertility which are also associated with lower infant mortality (Hojman 1992, Gakidou et al. 2010). This decline in natality and fertility is also a central feature of the progressive emancipation of women from a narrowly defined role in domestic and reproductive life (Chant 2013, Soto-Villagrán 2014).
In the full sample, educational attainment among women was associated with IMRs in the expected direction but the association disappeared when SE scores linked to living conditions and service provision were added to the model. However, analyses stratified by country GDP per capita showed that higher educational attainment among women was associated with lower IMRs even after adjustment for SE indicators in countries with GDP per capita below the sample median. It is possible that in countries with lower GDP per capita, women’s access to education remains an important barrier, possibly limiting labor force participation and its favorable effects (Howe et al. 2012). It is also possible that in countries with higher GDP per capita the measure of women’s education that we used may not capture differences in women’s circumstances relevant to IMRs after labor force participation is accounted for.
We showed that poor enforcement of laws concerning women’s right at a national level was associated with higher infant mortality: one-point higher CLE scale was associated with almost a 17% higher IMR. This adds to the evidence that fostering women’s development and improving women’s status may bring benefits beyond women’s own interests (Varkey and Lesnick 2010, Clots-Figueras 2012). These findings support the importance of actively engaging women in urban politics and governance to assure sustainability of this progress (ECLAC 2016, Hessel et al. 2020).
Some strengths of the study include the extensive compilation and harmonization of data on women’s empowerment and IMRs across a wide range of cities in Latin America and the incorporation of country as well as city level effects via multilevel modelling. Findings from this work support the importance of considering indicators of women and child’s health as part of the measures used for monitoring the achievements derived from women’s economic empowerment (Buvinic et al. 2020).
Although we included two important measures of women’s empowerment, we were not able to characterize other aspects of WE such as political participation of women in local and national governments which have been shown to be related to infant mortality in the region (Hessel et al. 2020). Due to data limitation we were not able to characterize the proportion of women living in poverty or the level of women’s income in cities. However, we showed that cities with lower levels of women’s labor force participation had also significantly lower proportion of population with adequate living conditions, suggesting the connection between urban poverty and low access to work and economic opportunities for women. Our measure of labor force participation does not capture the types of jobs that women are employed in or the benefits that their jobs may confer. Future work needs to further explore the intersection of women’s employment and income, education, and political participation as predictors of IMRs since opportunities for progress related to labor force participation (as well as the health consequences of employment itself) may be different for poor women or women with low education compared to wealthier women and women with higher education (UN 2017). Women with less education living in poor urban areas are more likely to have informal employments and hence they are more sensitive to economic downturns (UN 2017). Low wage jobs even in the formal economy can have adverse health and social impacts. Limited mobility and safety conditions in marginalized areas may constrain opportunities for better jobs or for job advancement (UN 2017). Indicators of women’s empowerment included in this study relied on census data and hence focused on access to resources for women’s empowerment such as eductation or employment. We were not able to include indicators related to other important domains of women’s empowerment such decision-making power (i.e. control over household expenditure), gender-based violence or measures of the empowering process itself (Buvinic et al. 2020) (i.e. self and collective-esteem), considered by many feminist scholars to be key aspects of women’s empowerment (Cornwall and Anyidoho 2010, Cornwall 2014). As future research continue to explore how women’s development in cities contributes to population’s health, more data need to be available at sub-national levels in order to better characterize the progress of women in urban areas.
Other limitations include the cross-sectional and ecological design and the use of a measure of vaccine coverage as a proxy of health-care access. Previous studies have shown that one-time and low complexity interventions, like measles vaccine coverage campaigns, tend to be more equally distributed in a population than specific high-skilled interventions (Barros and Victora 2013). A more accurate depiction of health-care coverage in the infant population may require the combination of several indicators related to family planning, antenatal care, multiple vaccine coverages and access to treatment during episodes of disease like diarrhea or pneumonia (Barros et al. 2012).
Under-registration of deaths is always a concern in analyses of infant mortality (Ribotta 2016). We addressed this issue in part by restricting the study to cities with good quality of data based on adult mortality estimations. However, it is possible that registration of infant deaths and live births is influenced by factors different from those that affect under-registration of adult mortality. If more underegistration of infant deaths is associated with lower women’s empowerment, the associations we report may be underestimates of true associations.
Conclusion
As urbanization continues to increase all over the world, it is critical to identify urban policies that can be most impactful in reducing infant deaths, which remain high even in many urban areas. Our results illustrate the potential benefits that fostering women’s development, may bring to child wellness in cities. Strategies involving the education of girls and increasing employment opportunities for women need to be considered and coordinated with other cost-effective interventions already implemented in the region (such as perinatal care & skilled birth, vaccine delivery, nutritional supplements, oral rehydration and antibiotics therapy) as part of programs that promote child health. In addition, women and children need to count as priority beneficiaries of urban planning interventions, as they represent a large proportion of the urban poor in many cities from low and middle-income countries. More systematic data on women’s socioeconomic achievement as well as on indicators measuring the process of women’s empowerment will be needed at the city-level in order to assess and monitor the implementation of these strategies and their impacts.
Supplementary Material
Acknowledgments
We thank Usama Bilal, Lance Ballester and Kari Moore for their support in the harmonization and creation of the mortality data.
The authors acknowledge the contribution of all SALURBAL project team members. For more information on SALURBAL and to see a full list of investigators, see https://drexel.edu/lac/salurbal/team/.
Biographies
Ana Ortigoza, MD PhD. Ana initiated her career as pediatrician in Argentina, after pursuing a PhD in Epidemiology she focuses now on examining the connections between social and built environment in cities among maternal, child, and adolescents, particularly in Latin America.
Ariela Braverman, MD. Ariela is pediatrician by training in Mexico, and is currently pursuing a PhD in Epidemiology at Drexel University. Her doctoral thesis is focused on understanding the influence of social environment, women’s empowerment, and access to services on adolescent pregnancy in Latin American cities.
Philipp Hessel, PhD. Philipp holds a PhD in Demography and masters in Sociology and Social Research. He is currently associate professor at Escuela de Gobierno A. Lleras in Universidad de los Andes. His research combine demography, public health, and policy research. He recently published a study about women’s political representation and its association with under-five mortality in Brazilian municipalities.
Vanessa Di Cecco, MPH. Vanessa is the editor-in-chief of the Salud Colectiva journal in its English version. She is currently pursuing a PhD in gender studies at Universidad Nacional de Buenos Aires. Her main research focus is the study of gender disparities in health, particularly in low- and middle-income countries.
Amélia Augusta Friche, PhD. Guta is a researcher and professor at Observatório de Saúde Urbana de Belo Horizonte at the Federal University of Mina Gerais (OSUBH-GPE). Her research focuses on social determinants of health and health impact assessment of urban redevelopment interventions.
Waleska Teixeira Caiaffa, MD PhD. Waleska is professor in Epidemiology at Universidade Federal de Minas Gerais (UFMG) and leads the Urban Health Observatory in Belo Horizonte (OSUBH-GPE). Her research focus involves social determinants of health, health impact assessment of urban environment interventions, and the distribution of communicable and non-communicable diseases including drug use in the urban context.
Ana V. Diez Roux, MD PhD. Ana is Dean and Distinguished University Professor of Epidemiology at Drexel University, where she also leads the Urban Health Collaborative. She is the principal investigator of the SALURBAL project. She is internationally known for her research on the social determinants of population health and the study of how neighborhoods affect health. Her research areas include social epidemiology and health disparities, environmental health effects, urban health, psychosocial factors in health, cardiovascular disease epidemiology, and the use of multilevel methods.
Correction Statement
This article has been corrected with minor changes. These changes do not impact the academic content of the article.
Funding Statement
This work was supported by the Wellcome Trust initiative ‘Our Planet, Our Health’ (grant 205177/Z/16/Z). The study funder had no role in study design, data collection, data analysis, data interpretation, or writing of this study. The corresponding author had full access to all the data in the study and had final responsibility for the decision to submit for publication.
Disclosure statement
No potential conflict of interest was reported by the author(s).
Geolocation information
The SALURBAL project is a study based on 371 cities of 100,000 or more residents in eleven countries from Latin America. The current study was based on 286 cities located in Argentina, Brazil, Chile, Colombia, Costa Rica, Mexico, Panama, and Peru.
Supplementary material
Supplemental data for this article can be accessed here
References
- Barros, A.J. and Victora, C.G., 2013. Measuring coverage in MNCH: determining and interpreting inequalities in coverage of maternal, newborn, and child health interventions. PLoS medicine, 10 (5), e1001390. doi: 10.1371/journal.pmed.1001390 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Barros, A.J.D., et al., 2012. Equity in maternal, newborn, and child health interventions in countdown to 2015: a retrospective review of survey data from 54 countries. The lancet, 379 (9822), 1225–1233. doi: 10.1016/S0140-6736(12)60113-5 [DOI] [PubMed] [Google Scholar]
- Beall, J., 1996. Participation in the city: where do women fit in? Gender & development, 4 (1), 9–16. doi: 10.1080/741921946 [DOI] [PubMed] [Google Scholar]
- Bilal, U., et al., 2019. Inequalities in life expectancy in six large Latin American cities from the SALURBAL study: an ecological analysis. The lancet planetary health, 3 (12), e503–e510. doi: 10.1016/S2542-5196(19)30235-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bodenhorn, H., 2006. Urban poverty, school attendance, and adolescent labor force attachment: some historical evidence. Cambridge, MA: National Bureau of Economic Research. [Google Scholar]
- Buvinic, M., et al., 2020. Measuring women’s economic empowerment. A compendium of selected tools. Washington, DC: Data2X & Center For Global Development. [Google Scholar]
- Cardenas, M., de Hoyos, M., and Szekely, M.. 2015. Out-of-school and out-of-work youth in Latin America: a persistent problem in a decade of prosperity. Economia, 16 (1), 37. [Google Scholar]
- Chant, S., 2013. Cities through a “gender lens”: a golden “urban age” for women in the global south? Environment and urbanization, 25 (1), 9–29. doi: 10.1177/0956247813477809 [DOI] [Google Scholar]
- Clots-Figueras, I., 2012. Are female leaders good for education? Evidence from India. American economic journal: applied economics, 4 (1), 32. [Google Scholar]
- Cornwall, A., 2014. Women’s empowerment: what works and why? Andrea Cornwall. Helsinki, Finland: UNU-WIDER, World Institute for Development Economics Research, 33. [Google Scholar]
- Cornwall, A. and Anyidoho, N.A., 2010. Introduction: women’s Empowerment: contentions and contestations. Development, 53 (2), 144–149. doi: 10.1057/dev.2010.34 [DOI] [Google Scholar]
- de Carvalho, J. and Wood, C., 1978. Mortality, income distribution, and rural-urban residence in Brazil. Population and development review, 4, 15. doi: 10.2307/1972857 [DOI] [Google Scholar]
- ECLAC , 2016. Equality and women’s autonomy in the sustainable development agenda. In: XIII Conference on women in Latin American and the Caribbean, 25–28 October, Montevideo. [Google Scholar]
- Ezzati, M., et al., 2018. Cities for global health. British medical journal, 363, k3794. doi: 10.1136/bmj.k3794 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Feenstra, R.C., Inklaar, R., and Timmer, M., 2015. The next generation of the penn world table. American economic review, 105 (10), 3150–3182. doi: 10.1257/aer.20130954 [DOI] [Google Scholar]
- Gakidou, E.C.K., Lozano, R., and Murray, C., 2010. Increased educational attainment and its effect on child mortality in 175 countries between 1970 and 2009: a systematic analysis. The lancet, 376, 16. doi: 10.1016/S0140-6736(10)61257-3 [DOI] [PubMed] [Google Scholar]
- Gasparini, L. and Marchionni, L., 2015. Bridging gender gaps? The rise and deceleration of female labor force participation in Latin America: an overview. Buenos Aires: Centro de Estudios Distributivos, Laborales y Sociales Maestría en Economía (CEDLAS) Facultad de Ciencias Económicas, Universidad de La Plata. Contract No.: Documento de Trabajo Nro. 185. [Google Scholar]
- Heaton, T.B., 2015. Are improvements in child health due to increasing status of women in developing nations? Biodemography and social biology, 61 (3), 252–265. doi: 10.1080/19485565.2015.1047487 [DOI] [PubMed] [Google Scholar]
- Hessel, P., et al., 2020. Increases in women’s political representation associated with reductions in child mortality in Brazil. Health affairs, 39 (7), 1166–1174. doi: 10.1377/hlthaff.2019.01125 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hojman, D., 1992. Evolution of infant and child mortality in Chile: a model. Applied economics, 24, 8. doi: 10.1080/00036849200000011 [DOI] [PubMed] [Google Scholar]
- Howe, L.D., et al., 2012. Measuring socio-economic position for epidemiological studies in low- and middle-income countries: methods of measurement in epidemiology paper. International journal of epidemiology, 41 (3), 871–886. doi: 10.1093/ije/dys037 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimani-Murage, E.W., et al., 2014. Trends in childhood mortality in Kenya: the urban advantage has seemingly been wiped out. Health & place, 29, 95–103. doi: 10.1016/j.healthplace.2014.06.003 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Koenen, K.C., Lincoln, A., and Appleton, A., 2006. Women’s status and child well-being: a state-level analysis. Social science & medicine, 63 (12), 2999–3012. doi: 10.1016/j.socscimed.2006.07.013 [DOI] [PubMed] [Google Scholar]
- Macmillan, R., Shofia, N., and Sigle, W., 2018. Gender and the politics of death: female representation, political and developmental context, and population health in a cross-national panel. Demography, 55 (5), 1905–1934. doi: 10.1007/s13524-018-0697-0 [DOI] [PubMed] [Google Scholar]
- Ortigoza, A.F., et al., 2020. Characterising variability and predictors of infant mortality in urban settings: findings from 286 Latin American cities. Journal of epidemiology and community health. doi: 10.1136/jech-2020-215137 [DOI] [PMC free article] [PubMed] [Google Scholar]
- PAHO . Vaccine calendar in the Americas. Panamerican Health Organization (PAHO). Available from: http://ais.paho.org/imm/IM_JRF_VACCINE_SCHEDULE.asp [Accessed 7 April 2019]. [Google Scholar]
- Pratley, P., 2016. Associations between quantitative measures of women’s empowerment and access to care and health status for mothers and their children: a systematic review of evidence from the developing world. Social science & medicine, 169, 119–131. doi: 10.1016/j.socscimed.2016.08.001 [DOI] [PubMed] [Google Scholar]
- Quamruzzaman, A. and Lange, M., 2016. Female political representation and child health: evidence from a multilevel analysis. Social science & medicine, 171, 48–57. doi: 10.1016/j.socscimed.2016.10.025 [DOI] [PubMed] [Google Scholar]
- Quistberg, D.A., et al., 2019. Building a data platform for cross-country urban health studies: the SALURBAL study. Journal of urban health, 96 (2), 311–337. doi: 10.1007/s11524-018-00326-0 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ribotta, B., 2016. Estimaciones sub-nacionales de la cobertura de las estadísticas vitales. Experiencias recientes en América Latina. In: VII Congreso de la Asociación Latinoamericana de población (ALAP) y XX Encontro Nacional de Estudos Populacionais (ABEP), 17–22 October 2016 Fos de Iguazu, Brazil. [Google Scholar]
- Smith, L.C., et al., 2004. The importance of women’s status for child nutrition in developing countries. Washington, DC: International Food Policy Research & Department of International Health, Emory University. [Google Scholar]
- Soto-Villagrán, P., 2014. Patriarcado y orden urbano. Nuevas y viejas formas de dominacion de genero en la ciudad. Revista venezolana de estudios de la mujer, 19 (42), 16. [Google Scholar]
- UN , 2005. Equal participation of women and men in decision-making processes, with particular emphasis on political participation and leadership. New York: United Nations Division for the Advancement of Women. [Google Scholar]
- UN , 2017. Progress of women in Latin America and the Caribbean. Transforming economies, realizing rights. New York: UN Women. [Google Scholar]
- Varkey, P.K.S. and Lesnick, T., 2010. Empowerment of women and its association with the health of the community. Journal of women’s health, 19 (1), 7. doi: 10.1089/jwh.2009.1444 [DOI] [PubMed] [Google Scholar]
- WHO , 2019. Subnational immunization coverage data. Available from: https://www.who.int/immunization/monitoring_surveillance/data/subnational/en/ [Accessed 7 April 2019].
- Women Stats Projects-Codebook . Available from: http://www.womanstats.org/CodebookCurrent.htm#MULTIVAR [Accessed 7 April 2019].
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.