

Abstract
For many years, data about heart failure (HF) was only limited to Western countries but in the last few years, well designed heart failure registries have been conducted in many developing countries. The purpose of this review is to summarize the current status regarding the epidemiology and management of heart failure in Middle East Arab countries (MEACs) by analysis of the results of the latest HF registries performed in these countries and to anticipate future perspectives, quality initiatives and areas of research and development. Data has shown that the average age of affected individuals is at least 10 years younger than their Western counterparts. Heart failure with preserved ejection fraction was generally under-represented in these registries to less than 30% of the whole population of heart failure. Coronary artery disease (CAD) constitutes about 55% of causes of heart failure in this region in comparison to about 70% in Western countries. An area that needs development is the investment in establishing specialized heart failure programs to cut the circle of non-compliance and repeated HF admissions to the hospitals. Advances in heart transplantation and mechanical circulatory support will continue to slow down and we are not expecting major changes in the near future but on the other hand, implantation of electronic devices like ICD and CRT is expected to increase significantly in the coming years in these countries.
Keywords: Heart failure, Epidemiology, Arab countries
1. Introduction
Recently, non-communicable diseases (NCDs) have globally shown increasing impact on health status, with disproportionately faster rates in developing countries [1]. Cardiovascular diseases, in particular heart failure, are on the top as a cause of mortality worldwide, including medium and low income countries [2]. This transition from infectious diseases to NCDs as the primary cause of mortality in developing countries is primarily connected to a tremendous rise in the incidence and prevalence of risk factors for coronary artery diseases including; diabetes mellitus, obesity, smoking and socioeconomic transition marked by increasing levels of sedentary life, lack of physical activities and increase in the consumption of fast fatty foods [3–6]. For many years, data about heart failure was only limited to Western countries but in the last few years, well designed heart failure registries have been conducted in many developing countries [11–15]. Most of these registries are quality initiatives aimed mainly at exploring the gap between real life practice and the common heart failure guidelines [11–15]. A lot of information is now available about heart failure in these countries. Middle East Arab countries (MEACs) include GULF countries (Saudi Arabia, United Arab Emirates, Qatar, Oman, Bahrain and Kuwait), Egypt, Yemen, Lebanon, Palestine, Syria, Jordan, and Iraq.
2. Objective
The purpose of this review is to summarize the current status regarding the epidemiology and management of heart failure in Middle East Arab countries (MEACs) by analysis of the results of the latest HF registries performed in these countries and to anticipate future perspectives, quality initiatives and areas of future research and development.
3. Methodology
A literature search was performed using electronic bibliographic databases (e.g. PubMed, COCHRANE and Elsevier/Science Direct) using the following keywords: heart failure, epidemiology, Arab countries. The search was limited to studies with data from countries of the Arab region. Most of the well-designed heart failure registries were from the GULF region and few were from Egypt, Lebanon, Sudan and Iraq.
4. Epidemiology and Risk Factors
Data about the prevalence of heart failure in this region is generally lacking. The estimated population in this region is ~250 000 000 and the global prevalence of HF is 1–2%, so we estimate ~3.75 million patients with HF in this region. Data has shown that the average age of affected individuals is at least 10 years younger than their Western counterparts [11–15]. This is an alarming sign as heart failure is known to be a disease of the elderly, but when the mean age of incidence is in the late fifties to early sixties, then it is not a disease of the elderly in the Middle East; it's rather a disease of middle to old age population. This information regarding age was consistent in all registries done for heart failure in Arab countries [11–15]. The explanation of this early occurrence of heart failure is multifactorial. The early incidence of coronary artery diseases was demonstrated in many registries as well and this is the first reported cause of heart failure in these countries [10,16]. Also the exceptionally high incidence of diabetes mellitus in these countries is a major risk factor for CAD and subsequently heart failure; in some reports, for example, diabetes mel-litus affects up to 25% of adults in the GULF countries [4]. Also there is a surge of obesity related mainly to socioeconomic transition and adoption of high caloric foods both of Western and traditional styles [4]. GULF countries are one of the highest in consumption of rice worldwide and among the highest in smoking as well [4,5]. Hypertension is also among the highest prevalent diseases in the Arab population, as 40–70% of heart failure patients were reported to have a history of hypertension [11–15]. Females constitute less than one third of the HF patients presented to the hospitals and this can be explained by less prevalence of CAD in females before menopause and also the reduced access of females to medical services compared to males in many countries of this region [11–15].
5. Heart Failure Presentations
Most of the registries done are on acute heart failure syndromes presented to the emergency room and admitted to the hospital. A minority of studies were done on ambulatory chronic heart failure patients [13]. Heart failure with preserved ejection fraction (HFpEF) was generally under-represented in these registries to less than 30% of the whole population of heart failure as shown in Table 1. This is attributed mainly to the lack of standard definition of the syndrome of HFpEF, the younger age of heart failure population in these countries, and heavy burden of comorbidities in HFpEF, causing those patients to be admitted to other services than cardiology with different primary diagnoses. There is marked underuse of the ambulance services in the transportation of those patients to the emergency departments, only about 6%, despite the heavy investment in these services in those countries. This could be attributed to underdevelopment of proper communicating ambulance systems, lack of population awareness, poor traffic infrastructure, and the heavy traffic burden in most of the big cities in this region.
Table 1.
Comparison between heart failure registries in Middle East Arab countries and data from the USA and Europe in patients with acute and chronic heart failure.
| Registry | HEARTS (acute) [7,8] | HEARTS (chronic) [9] | Gulf CARE [10] | Egyptian (acute) [11] | Egyptian (chronic) [11] | ADHERE [15,16] | ESC HF Long-Term Registry [17] |
|---|---|---|---|---|---|---|---|
| Region | Saudi Arabia | Saudi Arabia | 7 GULF countries | Egypt | Egypt | USA | Europe |
| Number of patients | 2610 | 685 | 5005 | 1475 | 670 | 105 388 | 5039 |
| Age, Mean (years) | 61.4 | 55.66 | 59 | 61 | 57 | 75 | 71 |
| Female, % | 34.2 | 29.9 | 37 | 30.4 | 35.8 | 51 | 37.3 |
| DM % | 64 | 52.7 | 50 | 45.4 | 31.8 | 44 | 38.9 |
| HTN, % | 71 | 66 | 61 | 43.5 | 40.8 | 73 | 62 |
| COPD, % | 19 | 19.5 | N/A | 14.8 | 13.3 | 31 | 15.2 |
| AF, % | 15.7 | 11.8 | 12 | 24.3 | 24.8 | 31 | 43.7 |
| CKD/dialysis, % | 29.6 | 22 | 15 | 17.6 | 13.4 | 29/5 | |
| Median EF | N/A | N/A | 35 | 36 | 40 | 34 | 38 |
| HFpEF, % | 27.1 (LVEF ≥0.40, %) | 13.3 (LVEF ≥0.40, %) | 31 (LVEF, >40%) | 22.0 (LVEF >45%) | 25.6 (LVEF >45%) | 46 (LVEF ≥0.40, %) | 32.8 (LVEF >45%) |
| Ischemic aetiology, % | 55.7 | 38.8 | 53 | 68.1 | 41.0 | 65 | 54 |
| Beta-blocker, at admission, % | 79 | 91.6 | 44 | 65.8 | 67.0 | 59 | 71.8 |
| ACE inhibitor/ARB, admission, % | 68.3 | 81.6 | 56 | 85.8 | 89.8 | 69 | 77 |
| Aldosterone antagonists, admission, % | 29 | 43.6 | 17 | 68.2 | 86.4 | NA | 55.3 |
| Days of hospital stay, median (IQR), % | 8 (9) | N/A | 6(4–10) | 4(3–5) | N/A | 4 (2–9) | N/A |
| Device therapy (ICD/CRT), % | 12.1 | 28.5 | 5.0 | 1.7 | 0.5 | 20 | 35 |
| Mortality %; | |||||||
| In-hospital, | 6.5 | N/A | 6.3 | 5 | 4 | 4.6 | |
| 1 month, | 8.3 | N/A | N/A | N/A | N/A | N/A | |
| 3-months, | N/A | N/A | 12.6 | N/A | N/A | N/A | |
| 6 months | 13.7 | N/A | N/A | N/A | N/A | N/A | |
| 12-months, | 19.5 | 9 | 20.2 | N/A | N/A | N/A | |
| 2 years, | 23.5 | N/A | N/A | N/A | N/A | N/A | |
| 3 years, | 24.3 | N/A | N/A | N/A | N/A | N/A | N/A |
HEARTS, heart failure assessment registry trial in Saudi Arabia; Gulf CARE, Gulf acute heart failure registry; ADHERE, Acute Decompensated Heart Failure National Registry; ESC, European Society of Cardiology; HF, heart failure; DM, diabetes mellitus; HTN, hypertension; COPD, chronic obstructive pulmonary disease; AF, atrial fibrillation; CKD, chronic kidney disease; HFpEF, heart failure with preserved ejection fraction; ACE, angiotensin converting enzyme; ARB, angiotensin receptors blocker; IQR, interquartile range; ICD, implantable cardioverter defibrillator; CRT, cardiac resynchronization therapy; NA, not available.
6. Burden of Comorbidities in Heart Failure Patients
Besides the burden of risk factors mentioned above, there are other comorbidities that complicate heart failure presentation in these countries [11–15]. Renal failure is present in about a quarter of those patients and constitutes the biggest challenge and burden, both on the patients and health care facilities. Renal failure interferes with the application of many therapeutic strategies and lifesaving medical regimens. Anemia was demonstrated in about 20% of heart failure patients and it is underestimated and poorly treated [11–15]. Anemia and iron deficiency badly affect the quality of life of heart failure patients and are important therapeutic targets according to the recent studies and guidelines of heart failure. Atrial fibrillation, on the other hand, was less present in HF patients in this region. if compared with international registries. Atrial fibrillation was present in only 12–15%, both in the acute and chronic settings [11–15]. This could be explained by the younger age of the population, lower contribution of HFpEF, and the under use of continuous ECG monitoring (HOLTER) to diagnose paroxysmal atrial fibrillation. The incidence of asthma/COPD was comparable to most of the international registries [11–15,19–21].
7. Diagnostic Modalities Used to Diagnose HF
There are some variations in the use of diagnostic modalities for HF among countries of this region. In GULF countries, the access to advanced imaging modalities, especially echocardiography, is much higher than other countries in the region. Echocardiography was utilized in nearly 97% of the heart failure population in Saudi Arabia and about 93% in other GULF countries [12–14]. On the other hand, the use of Cardiac MRI is still very underused in most of these countries mainly due to either unavailability of the service or the qualified personnels. There is marked and unexplained underuse of natriuretic peptides either for diagnosing or for the follow-up of heart failure patients in those countries. Most probably, this underuse is mainly due to the unavailability of the kits, the expensiveness of the test in many countries of the region, and the lack of knowledge regarding its role in HF diagnosis and management.
8. Heart Failure Etiology in the Arab Region
Not surprisingly, coronary artery diseases (CAD) came as the first cause of heart failure in this region, which this was expected given the heavy burden of CAD risk factors, namely diabetes mellitus, hypertension and smoking. CAD constitutes about 55% of causes of heart failure in this region in comparison to about 70% in Western countries [11–15,19–21] as shown in Table 1 and Fig. 1. The second cause was dilated nonischemic cardiomyopathy with about 16–18% of the cases as represented with most acute heart failure registries, which is more representative of the etiology than outpatient settings. A wide variety of etiologies have been considered as the cause. These included idiopathic dilated cardiomyopathy, post myocarditis, peripartum cardiomyopathy, toxic and drug related cardiomyopathy. Extraordinary rise in the diagnosis of dilated non-ischemic cardiomyopathy in the registries of chronic heart failure is mainly related to selection bias, as most of these patients are being recruited from heart failure specialized clinics with more bias towards including patients with nonischemic than ischemic cardiomyopathies. Hypertension comes in as the third cause of heart failure in this population constituting about 10–12% of causes, which is different from Western countries where hypertension was the second cause of heart failure in most of the recent registries. Surprisingly, rheumatic valvular heart disease comes in as the fourth cause of heart failure, comprising only of 7–11% of the causes in most countries of the region, even in those where rheumatic fever was classically defined as endemic [11–15]. It is clear that there is a major decline in the incidence of rheumatic heart disease and its progression to heart failure in the region[17]. In one study in Baghdad, Iraq, more than 50 years ago, 47.9% of patients admitted with heart failure had rheumatic heart disease, and bilharziasis was associated with a considerable number of cases of hypertension and with a small percentage of cases of cor pulmonale [18]. The authors stated that prevention of rheumatic fever and bilharziasis should constitute the corner-stone of any effective control programme of cardiovascular disease at that stage of medical development in Iraq [18]. These two studies show how the situation has changed over the last four decades in this region.
Fig. 1.
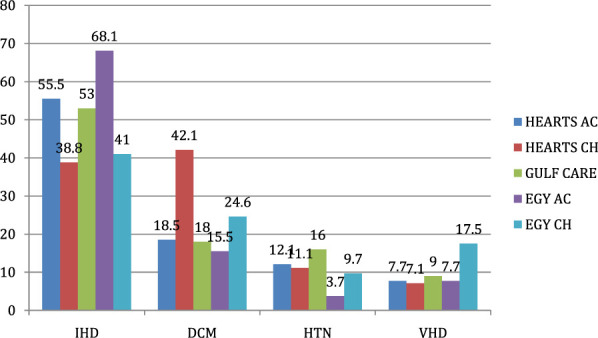
Distribution of heart failure causes in 5 of the heart failure registries in Arab countries. HEARTS AC, HEARTS acute; HEARTS CH, HEARTS chronic; EGY AC, Egyptian acute; EGY CH, Egyptian chronic; IHD, ischemic heart disease; DCM, dilated cardiomyopathy; HTN, hypertension; VHD, valvular heart disease.
9. Treatment Options
Surprisingly, the rate of evidence-based therapies for heart failure use was high, especially in the GULF countries. In two big registries both beta blocker and ACEIs/ARBs use was above 80% for each group at least at the time of discharge from the hospitals or in the chronic ambulatory settings [12–14]. The rate of beta blocker use even exceeded 90% in a selected group of ambulatory heart failure patients in one study [13]. Most of the new heart failure therapies are registered and available in those countries, including the new ARNI (angiotensin receptor neprilysin inhibitor) group. Ivabradine is available in all countries of the region except Saudi Arabia. For ARNI, there are many restrictions for its use given the high cost and the limited experience as with most countries in the world. Mineralocorticoid receptor antagonists (MRA) are being used in the rate of 35–55% in most of the available registries, which matches its use worldwide. For implantable cardioverter defibrillator (ICD)/cardiac resynchronization therapy (CRT), there is wide variation in the rate of use among countries of the region with Saudi Arabia being the highest. The average rate of use in GULF countries for ICD is about 10–20% and for CRT it is about 3–8% among eligible patients. In countries like Egypt, the use of these devices is among the lowest worldwide and only less than 1% of heart failure patients have ICD/CRT devices [15].
10. Heart Transplantation and Mechanical Circulatory Support
Heat transplantation is very limited in Arab countries with lack of legislation as well as social and possibly religious issues surrounding heart transplantation. Saudi Arabia is an exception in this regard, with an active heart transplantation center performing up to 30 cases per year with results matching other transplant centers in the western countries. Lebanon and UAE have a very limited numbers of heart transplantation.
On the other hand, long term mechanical circulatory support is now available in few countries in the region, mainly in Saudi Arabia, Egypt, Kuwait, UAE and Lebanon. In Saudi Arabia, most of its use is as a bridge to transplantation with just few cases as destination therapy. In Egypt, however, all of the cases are for destination or as a bridge to recovery as there is no heart transplantation. Many obstacles are surrounding the institution of long term mechanical circulatory support programs, not all of them financial, but logistic factors, including patient's satisfaction with these current devices with external parts, drive line, physician awareness, and late referral. In my opinion, once the fully implanted devices are available, the growth in implanting these devices in the region will be one of the highest among countries of the world.
11. Heart Failure Programs and Heart Failure Clinics
The majority of heart failure patients in this region are still being looked after by non-heart failure specialists. Only few countries, especially in the GULF regions, have developed structured heart failure programs with specialized heart failure clinics run by certified heart failure cardiologists and include nurses, pharmacists and other disciplines. In Saudi Arabia, for example, there are at least 10 heart failure clinics distributed through the country and they clearly made a big change in the care of heart failure patients. UAE, Qatar, Kuwait and Lebanon have some of these clinics but other countries of the region, unfortunately, are still a way behind in establishing these clinics which are now part of the international heart failure recommendations.
12. Future Perspectives
With this early onset of heart failure in the region, more efforts and investments should be directed towards prevention of heart failure and risk factor control. The second area that needs development is the extension in establishing specialized heart failure programs with more dependence on trained nurses to cut the circle of non-compliance and repeated admissions to the hospitals. Advances in heart transplantation and mechanical circulatory support will continue to slow down and we are not expecting major changes in the near future but on the other hand, implantation of electronic devices like ICD and CRT is expected to increase significantly in the coming years. More structured research identifying the prevalence and incidence of heart failure and studying the uniqueness and needs of our population is required. Considering the cost awareness era we are living in, more effective strategies to improve patient outcomes, access to care, and efficiency of services is the strategy that most healthcare authorities should focus on in the future. Public awareness programs are necessary as well to facilitate better provision of care as the patient involvement is core in the success of heart failure programs.
Abbreviations
- HF
Heart failure
- MEACs
Middle East Arab countries
- CAD
Coronary artery disease
- ICD
Implantable cardioverter defibrillator
- CRT
Cardiac resynchronization therapy
- NCDs
Non-communicable diseases
- HFpEF
Heart failure with preserved ejection fraction
- ACEIs
Angiotensin converting enzyme inhibitors
- ARBs
Angiotensin receptor blockers
- ARNI
Angiotensin receptor neprilisin inhibitor
- MRA
Mineralocorticoid receptor antagonists
- UAE
United Arab Emirates
Declaration of Competing Interest
The authors have no conflicts of interest relevant to this article.
References
- 1.Terzic A, Waldman S. Chronic diseases: the emerging pandemic. Clin Transl Sci. 2011;4(3):225–6. doi: 10.1111/j.1752-8062.2011.00295.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 to 2030. PLoS Med. 2006;3(11):e442. doi: 10.1371/journal.pmed.0030442. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Abegunde DO, Mathers CD, Adam T, Ortegon M, Strong K. The burden and costs of chronic diseases in low-income and middle-income countries. Lancet. 2007;370(9603):1929–38. doi: 10.1016/S0140-6736(07)61696-1. [DOI] [PubMed] [Google Scholar]
- 4.Guy GW, Nunn AVW, Thomas LE, Bell JD. Obesity, diabetes, and longevity in the Gulf: is there a Gulf metabolic syndrome? JDM. 2009;1:43–54. [Google Scholar]
- 5.Bassiony MM. Smoking in Saudi Arabia. Saudi Med J. 2009;30(7):876–81. [PubMed] [Google Scholar]
- 6.Najafi F, Jamrozik K, Dobson AJ. Understanding the ‘epidemic of heart failure’: a systematic review of trends in determinants of heart failure. Eur J Heart Fail. 2009;11:472–9. doi: 10.1093/eurjhf/hfp029. [DOI] [PubMed] [Google Scholar]
- 7.Pang PS, Komajda M, Gheorghiade M. The current and future management of acute heart failure syndromes. Eur Heart J. 2010;31:784–93. doi: 10.1093/eurheartj/ehq040. [DOI] [PubMed] [Google Scholar]
- 8.Gheorghiade M, Braunwald E. Hospitalizations for heart failure in the United States-a sign of hope. JAMA. 2011;6:705–6. doi: 10.1001/jama.2011.1510. [DOI] [PubMed] [Google Scholar]
- 9.Agarwal AK, Venugopalan P, de Bono D. Prevalence and aetiology of heart failure in an Arab population. Eur J Heart Fail. 2001;3:301. doi: 10.1016/s1388-9842(00)00149-5. [DOI] [PubMed] [Google Scholar]
- 10.AlHabib KF, Hersi A, AlFaleh H, Kurdi M, Arafah M, Youssef M, et al. The Saudi project for assessment of coronary events (SPACE) registry: design and results of a phase I pilot study. Can J Cardiol. 2009;25:e255–8. doi: 10.1016/s0828-282x(09)70513-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.AlHabib KF, Elasfar AA, AlBackr H, AlFaleh H, Hersi A, AlShaer F, et al. Design and preliminary results of the heart function assessment registry trial in Saudi Arabia (HEARTS) in patients with acute and chronic heart failure. Eur J Heart Fail. 2011;13(11):1178–84. doi: 10.1093/eurjhf/hfr111. [DOI] [PubMed] [Google Scholar]
- 12.Alhabib KF, Elasfar AA, Alfaleh H, Kashour T, Hersi A, AlBackr H, et al. Clinical features, management,and short-and long-term outcomes of patients with acute decompensated heart failure: phase I results of the HEARTS database. Eur J Heart Fail. 2014;16(4):461–9. doi: 10.1002/ejhf.57. [DOI] [PubMed] [Google Scholar]
- 13.Waleed Alhabeeb, Abdelfatah Elasfar, Hanan AlBackr, Fayez AlShaer, Almasood Ali, Hussam Alfaleh, et al. Clinical characteristics, management and outcomes of patients with chronic heart failure: results from the heart function assessment registry trial in Saudi Arabia (HEARTS-chronic) Int J Cardiol. 2017 doi: 10.1016/j.ijcard.2017.02.087. . Under press. [DOI] [PubMed]
- 14.Kadhim Sulaiman, Prashanth Panduranga, Ibrahim Al-Zakwani, Alawi A, Alsheikh-Ali, AlHabib Khalid F, et al. Clinical characteristics, management, and outcomes of acute heart failure patients: observations from the Gulf acute heart failure registry (Gulf CARE) Eur J Heart Fail. 2015;17:374–84. doi: 10.1002/ejhf.245. [DOI] [PubMed] [Google Scholar]
- 15.Hassanein M, Abdelhamid M, Ibrahim B, Elshazly A, Aboleineen MW, Sobhy H, et al. Clinical characteristics and management of hospitalized and ambulatory patients with heart failure–results from ESC heart failure long-term registry–Egyptian cohort. ESC Heart Failure. 2015;2:159–67. doi: 10.1002/ehf2.12046. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Albackr HB, Alhabib KF, Ullah A, Alfaleh H, Hersi A, Alshaer F, et al. Prevalence and prognosis of congestive heart failure in Saudi patients admitted with acute coronary syndrome (from SPACE registry) Coron Artery Dis. 2013;24(7):596–601. doi: 10.1097/MCA.0b013e328364d98f. [DOI] [PubMed] [Google Scholar]
- 17.Sorour KA. Rheumatic heart disease in Egypt: gloomy past and promising future. Egypt Heart J. 2014;66:139–42. [Google Scholar]
- 18.Damluji SF, Al-Saffar G, Thamer MA, Mary AS. Congestive heart failure in women in Iraq. Bull World Health Organ. 1964;31(3):337–44. [PMC free article] [PubMed] [Google Scholar]
- 19.Adams KF, Jr, Fonarow GC, Emerman CL, LeJemtel TH, Costanzo MR, Abraham WT, et al. ADHERE Scientific Advisory Committee and Investigators. Characteristics and outcomes of patients hospitalized for Acute decompensated heart failure in in the United States: rationale, design, and preliminary observations from the first 100,000 cases in the Acute Decompensated Heart Failure National Registry (ADHERE) Am Heart J. 2005;149:209–16. doi: 10.1016/j.ahj.2004.08.005. [DOI] [PubMed] [Google Scholar]
- 20.Atherton JJ, Hayward CS, Wan Ahmad WA, Kwok B, Jorge J, Hernandez AF, et al. ADHERE International–Asia Pacific Scientific Advisory Committee Patient characteristics from a regional multicenter database of acute decompensated heart failure in Asia Pacific (ADHERE International–Asia Pacific) J Card Fail. 2012;18:82–8. doi: 10.1016/j.cardfail.2011.09.003. [DOI] [PubMed] [Google Scholar]
- 21.Crespo-Leiro MG, Anker SD, Maggioni AP, Coats AJ, Filippatos G, Ruschitzka F, et al. Heart failure association (HFA) of the European society of cardiology (ESC). European society of cardiology heart failure long-term registry (ESC-HF-LT): 1-year follow-up outcomes and differences across regions. Eur J Heart Fail. 2016 Jun;18(6):613–25. doi: 10.1002/ejhf.566. [DOI] [PubMed] [Google Scholar]