

Patients posted for phacoemulsification underwent initial steps of wound construction and a continuous curvilinear capsulorhexis in a routine manner. Following this, microscope-integrated intraoperative optical coherence tomography (MIOCT) was focused along with the posterior cortical-capsular interface [Fig. 1a] and the surgeon performed a smooth hydro-dissection using a 27-gauge cannula mounted on a 2-cc syringe filled with balanced salt solution (BSS). The injected BSS jet traveled just underneath the anterior capsule and along with adjacent cortical matter till the equator. The dissection jet force then took a posterior course to reach the posterior pole of the cataractous lens. During this first phase, the separation between the cortex and capsule was minimal and quick, which was evident on MIOCT as initial shallow posterior bowing of the posterior capsule. In the second phase, fluid accumulated swiftly at the most dependent portion, that is, posterior pole [Fig. 1b], to cause a sudden expansile separation between the posterior-most cortical layer and posterior capsule. In the third phase, separation progressed in a centrifugal manner completing hydro-dissection [Fig. 2a] and a forward bulge of the lens was also evident clinically. However, even after completion of the fluid wave, the separation between the posterior capsule and the posterior cortex was not entirely thoroughgoing. Few tentacular extensions of residual cortical matter persisted between the capsule and lens [Fig. 2b].
Figure 1.
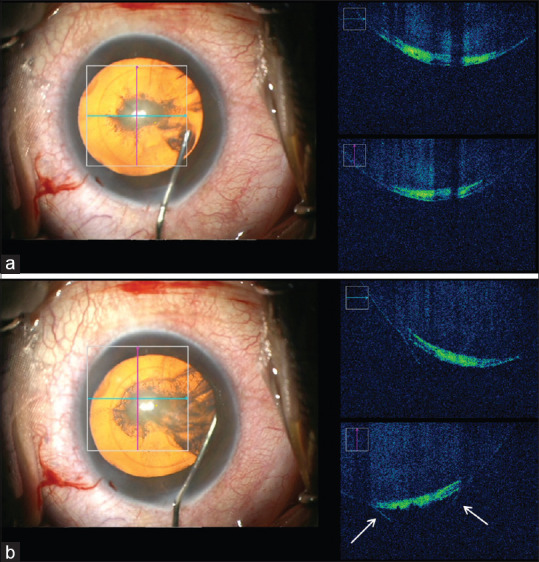
(a) Microscope-integrated intraoperative optical coherence tomography (MIOCT) focused on the posterior cortical-capsular interface. (b) Shows the initial stage of separation along with the posterior capsule and the cortical matter evident by posterior conical bulging of the posterior capsule (arrows)
Figure 2.
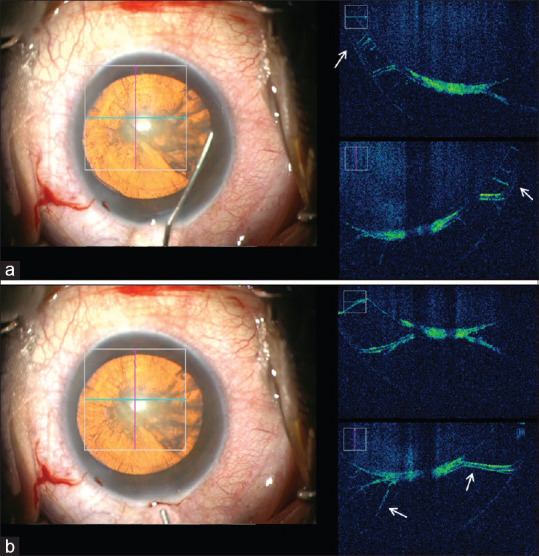
(a) Demonstrates centrifugal spread of the hydro-dissection wave (arrows). (b) Following a complete hydro-dissection, the near-total separation is evident by a complete posterior displacement of the capsule and anterior displacement of the cortical matter with few tentacular adhesions (arrows) between the two
Discussion
We observed hydro-dissection in 10 cases during routine cataract surgeries and found a more or less similar pattern of expansile separation at the interface [Video 1]. In some cases, the dissection was less evident due to varying levels of nuclear sclerosis and posterior cortical opacity. This MIOCT-based observation elucidates our understanding of the orientation of dissection forces in vivo for the first time and provides practical evidence of thrusting hydro-dissection forces maximally impacting posterior capsular apex followed by a centrifugal spread. This understanding acknowledges the existing practice of avoiding hydro procedure during cataract surgeries[1] with inherent/suspicious posterior capsular dearth.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Video Available on: www.ijo.in
Reference
- 1.Osher RH, Yu BC, Koch DD. Posterior polar cataracts: A predisposition to intraoperative posterior capsular rupture. J Cataract Refract Surg. 1990;16:157–62. doi: 10.1016/s0886-3350(13)80724-9. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.