

Abstract
Asthenopic and related symptoms are a major problem in school-going children. With the inception of computers and other gadgets for near work, the unseen problems arising out of constant and continuous near work, are on the rise. Parents wander from pillar to post, seeking respite from their child's constant complaints from near work; but despite best spectacle correction and avoidance of excessive near work, the complaints continue. Studies have shown that the majority of these problems arise from defects in accommodation, even in a young child. Therefore, various aspects of accommodation deficiencies have to be studied clinically, detected, and treated to ameliorate the symptoms.
Keywords: Accommodative therapy, amplitude of accommodation, asthenopia, facility of accommodation, flipper tests, insufficiency of accommodation
Accommodation is one of the greatest virtues we use to see clearly and comfortably. There are quite a number of visual problems that arise while using the eyes for near work, where accommodation comes into effect; but unfortunately, this aspect has been least studied and disregarded. Ocular asthenopia and host of related problems arising on near work, have never been scientifically attributed to anomalies in accommodation. More so, such problems have never been even thought to arise in children, as their accommodation is assumed to be great and flawless. We have nurtured this misbelief all along. Though this concept has been studied for many years and we have now a clear understanding of the accommodative mechanism, but it is rarely clinically applied in practice. Symptoms at near work like headaches, asthenopia, watering, blurring, redness, lack of concentration, etc., occur frequently in children, and every test is done from refraction to ocular motility–to find the cause–except accommodative tests.
But it may come as a surprise that accommodation is not as efficient in children as expected. Subjective symptoms usually emerge around 6–7 years of age, when children start getting extensively involved in near work, and there is a clear relation between accommodative parameters and these symptoms. Because accommodative dysfunctions may result in varied asthenopic symptoms, it is of utmost importance to identify this dysfunction to prevent unnecessary visual problems. Therefore, clear standards for diagnosing an accommodative dysfunction need to be further refined. Studies have shown that accommodative training, in cases of dysfunction, is an effective method in alleviating the symptoms.[1]
Mechanisim of accommodation
”Accommodation is the ability of the eye to change the refractive power of the crystalline lens to focus objects on the retina at various distances.'' The accommodative process includes the contraction of the ciliary muscles, relaxation of the lens zonules and lens capsule, increase in curvature of the lens and reduction in pupillary size.[2,3,4] In addition, the accommodative activity also produces a change in the visual axis, called convergence.[5]
This synkinetic association of accommodation, miosis, and convergence is called the 'near response'.
Basics of accommodation
Anatomically, three parts in the eye are involved in the accommodative process, i.e., a) Ciliary muscles-circular and meridional b) the Zonules, and c) the Crystalline lens. By far, all along, the focus has been always been on the characteristics of the lens in the accommodative process. Very little attention has been on the nature and efficiency of ciliary muscles. In children and younger persons, it is the power of ciliary muscles which is in question in accommodative anomalies.
Stimuli to accommodation
The characteristics of effective ''accommodative stimuli'', are the first step in our understanding of the accommodative system. There are a number of 'different' accommodative stimuli, which stimulate accommodation to varying degrees.[6,7,8,9]
These are:
Blur of the object
Proximity of the target
Changing target size
Chromatic aberration
Convergence of eyes
Spatial frequency.
These are all different stimuli to accommodation, with 'Blur' of an object having the greatest impact as stimuli, though independent of visual acuity.[10]
An important implication is the completely different character of these stimuli, which can act together as well as independently.
Amplitude of accommodation
The ability to focus a visual target at varying distances is known as accommodation, and is present to some extent from birth,[11] but improves rapidly by the first 6 months of life.[12,13,14] It is believed that a small child is able to focus from infinity down to very close to the eyes because of a high level of accommodation. However, it is to be noted that accommodation and convergence are not automatically linked from the start.[13]
The amount of accommodation, in diopters, needed to clearly focus an object from infinity to the nearest point possible, is the 'amplitude of accommodation'.[15]
The accommodative function is normally expressed by describing the accommodative amplitude and its dioptric value.
In 1912, Duane presented a result of accommodative amplitude in subjects from 8 yrs to 80 yrs. The given data are still commonly used as normality for accommodative amplitude. A formula based on Duane's data and later studied by Hoffstetter,[16] predicts the range of accommodative amplitude, (minimum amplitude = 18.5 – 0.3 age and maximum amplitude = 25 – 0.4.age). Based on this formula, a 3-year-old child is expected to have an average amplitude of 17.5 D.
Facets of accommodation
However, the accommodative function is more complicated than accommodative amplitude. The accommodative system is complex; and comprises not only the amplitude but number of other functions known as Facets of accommodation.[17,18,19,20] Any of them can be underdeveloped and can give rise to ocular symptoms.
Different facets of accommodation
Amplitude of accommodation
Tonic accommodation
Lag of accommodation
Convergence accommodation
Accommodative facility
Relative accommodation.
These facets differ greatly from each other with regard to function. They require different methods of measurement and are not explained by the same dioptric value. No method in use describes the complete accommodative function, also we do not use the same measuring system for different dioptric results. Furthermore, the dysfunction of each envisages a different set of symptoms.
Let us review each of these facets.
-
Amplitude of accommodation: As already stated, it is the total accommodative power of the eye and is expressed in dioptric equivalent and is reciprocal to the distance of the object from the eye. As age advances, the power of accommodation deteriorates, and the ability to see clearly at near diminishes. As a matter of fact, this ability or facet of accommodation is most relevant to the clinician and thus is the only one tested clinically in routine practice.
Amplitude tests:
-
Donder's push-up method: This method uses the Royal Air Force (RAF) ruler. (Also known as Prince ruler).In this, a ruler about 50 cm in length has markings on one side in cms and other side in dioptres. A sliding box is mounted on the ruler in which letter lines conforming to Snellens optotype size to be read from near. The subject holds the ruler with one end mounted on the nose and holds the other end with the hand. A +3.0 D lens is placed in front of the eyes to pull up the range of accommodation to 35 cms. The reading card or box is moved away till the print blurs and pulled up near till the print blurs again. The difference between the two readings gives the amplitude of accommodation.
- Sheard's method: Here, minus lenses are added at far distance target, monocularly or binocularly until blur at distance occurs. The power of lenses used gives the amplitude.
-
-
Tonic accommodation: Tonic accommodation (TA) or Dark Accommodation (DA) is a passive state of accommodation in the absence of any stimulus. This occurs when the eye is in complete darkness or when it is looking at a bright empty field. Basically, it is the inherent tone of the ciliary muscles when the eye at rest. Ironically, the resting 'tone' varies in different situations or differs in refractive errors.[21,22]
This tonic state of accommodation or the 'resting state tone' of the ciliary muscles can be unearthed only after total cycloplegia. Another way of measuring is by using an objective 'infrared optometer.[23]
Lag of accommodation: The amount by which the accommodative response of the eye is less than the dioptric stimulus to accommodation is defined as the 'accommodative lag'.[17,24,25] Clinical measurement of accommodative lag at near is typically done by dynamic retinoscopy. This is an objective method in which the patient views a near point target, while the examiner uses lenses to neutralize the fundal glow.
-
Convergence accommodation: Convergence accommodation is normally described by the ratio between convergence-accommodation and convergence, or the CA/C ratio.
The ratio is the measure of the effect of change in convergence on accommodation.
It is expressed as the change in accommodation (Diop.) for each change in convergence in Prism D.[26]
-
Accommodative facility: ' Accommodative facility' is the ability to rapidly change the power of the crystalline lens to various focus distances while maintaining a requisite angle of convergence (binocularly) or eliminating the influence of convergence (monocularly). This ability is important while changing the fixation from near to distance and back again.
Clinically, accommodative facility can be measured using lenses that stimulate accommodation (minus lenses) or inhibit accommodation (plus lenses). Any combination can be used for evaluation, but experience has shown that plus-minus 2D is a reasonable choice.[27] The procedure uses a plus-minus 2D lens pair mounted on a 'flipper frame' [Fig. 1]. A flipper is a frame on which two plus and two minus lenses are mounted.
The subject focuses with one pair of lenses at an object at a fixed distance (say 40 cms). When the object is clearly focused, a 'flip' of the frame is quickly performed to bring the other pair in front of the eyes, and the person focuses through them. This is then again repeated, and the number of cycles completed in one minute is noted as the 'accommodative facility' in 'cycles/min'(cpm).
Normative data on children have been collected by number of researchers. The results of the Flipper test in children aged 6-12 years were 5.0+- 2.5 cpm[28] in a study.
The cutoff parameter for a reduced facility to show symptoms is less than 3 cpm.
The facility testing is important and has bearing on the symptoms where children complain of difficulty in focusing on the board and then reading/writing at near.
-
Relative accommodation:
The total amount of accommodation, which can be exerted while the convergence remaining fixed, is called the 'relative accommodation'. This can be either 'positive relative accommodation (PRA) or 'negative relative accommodation' (NRA).
PRA is the amount of accommodation in excess of the accommodation needed for convergence and NRA is the amount of accommodation less, than needed for convergence.[5,29] In other words, the least amount of accommodation or maximum relaxation of accommodation with which one can see clearly at a fixed distance is the NRA and the maximum accommodation used over and above the need at a fixed distance is called PRA. To assess this flexibility, a simple test is used.[30] With a vergence stimulus fixed at 40 cms, positive lenses with 0.25 D increments are put in front of both eyes and the first sign of blur is noted. The amount of plus lenses used will give the value of NRA. Similarly, now minus lenses are used with increasing power in 0.25 D steps, binocularly, till the first sign of blur is noted. The increased amount of stimulus at this point is the PRA.
Tests for PRA and NRA are very helpful in determining accommodative dysfunctions in children.[31] A low NRA reveals accommodative spasticity; while a low PRA suggests that the focusing mechanism may be prone to tiring after concentrated near work.
It would be not out of place to discuss the AC/A ratio, as it is linked with accommodation. Due to the near vision reflex complex, a certain amount of convergence is expected when accommodation is in force. The relation between the dioptric change accommodation and the prismatic change in convergence is called the accommodative CONVERGENCE/ACCOMMODATION in ratio (AC/A ratio.) In simple terms, the AC/A ratio describes how much convergence is activated by an accommodative change of 1 D. Normally convergence of 3–5 PD occurs when 1 D of accommodation is exerted. An AC/A of 10 or more is termed as high ratio while an AC/A ratio less than 3 is termed as low.[19]
Figure 1.
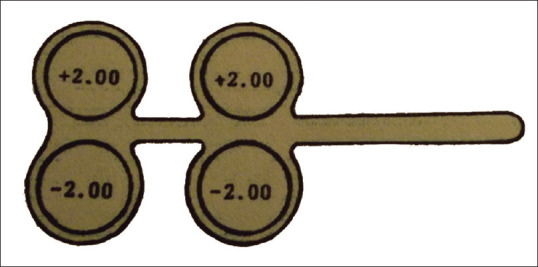
Flipper test frame with plus-minus 2D lenses test for accommodative facility
Practical dysfunctions
The accommodative system at a young age is quite flexible and resistant to fatigue. However, in clinical practice, accommodative dysfunction can occur in children and young people. Often children and teenagers complain of certain symptoms thatappear when doing near work. The refractive system is usually emmetrope or slightly ametropic, but that is not always in relation to the complaints. Unfortunately, there does not exist, as mentioned earlier, no simple, single standard procedure, which might include all facets of accommodative dysfunction. Because of this reason and because we do not have any clear cut method of treating accommodative problems, the accommodative system is not routinely examined. But it is of great importance to identify any accommodative dysfunction if any complaints exist, so that unnecessary near vision problems may be prevented. It is also important to identify any accommodative dysfunction or deficiency in school-going children, because this has a bearing on the performance of children in school.[32,33] Because the focusing system of eyes contribute to the learning process, any accommodative deficiency can make it unnecessarily difficult for the child to read and write and develop in studies. If the child's accommodative deficiencies are not resolved, he/she may develop dislike towards any near work and develop a lack of interest in studies. Therefore, we need to find a simple and easy-to-use method that identifies an accommodative dysfunction.
It is difficult to group accommodative dysfunctions, as the boundaries are often unclear. However, clinically it is useful to separate anomalies of accommodation into five distinct syndrome categories.[34]
Insufficiency of accommodation
Infacility of accommodation
Fatigue of accommodation
Spasm of accommodation
Paresis of accommodation.
These five syndromes constitute different accommodative disorders, having slightly different symptoms, and having a different impact on accommodative function.
A brief description of each would be helpful in identifying and treating the disorders.
An important aspect is that of symptoms related to accommodative dysfunction must be clearly recognized and understood. Most of the times, the clinician conscientious only on the refractive anomalies and attributes all symptoms to the refractive problem. It should be remembered that all symptoms need not be due to refractive error; time should be devoted to enquire about all symptoms especially arising from near work and tests should be employed to determine the type of accommodative anomaly.
Understanding the symptoms is of paramount importance in recognizing any accommodative anomaly.
Asthenopia is a cardinal symptom, which stands out prominently in accommodative deficiencies. Asthenopia is a term used to describe eye-strain or symptoms arising from the use of eyes for near work.
Though asthenopia is used loosely to describe all types of symptoms but scientifically explaining, it means purely eye strain and comprises of red eyes, frequent rubbing and irritation of eyes, and disinterest in doing near work after a certain time. Other symptoms arising from accommodative strain are headaches, diplopia, blurring, vertigo, drowsiness.[35,36]
As asthenopia is the flagbearer of any ocular morbidity, it would be not out of place to illustrate the reasons for asthenopia. Asthenopia, per se, can occur in the following condition[36]:
Accommodative Insufficiency
Accommodative Infacility
Accommodative Fatigue
Accommodative Spasm
Dyslexia
Hysteria
Ocular Inflammations
Phorias-Ocular motility disorders
Latent Nystagmus
Anisekonia
Refractive Errors: Astigmatism; Hyperopia; Anisometropia
Accommodative Paresis.
It thus becomes mandatory to recognize these conditions by exclusion and look for the accommodative reasons carefully.
Since this article is dedicated to accommodative problems, let us briefly discuss the five syndromes which occur clinically.
Insufficiency of accommodation: It is a condition in which the amplitude of accommodation is chronically below the lower limits of the expected amplitude of accommodation for the person's age.[37] Classically, the insufficiency of accommodation is a physiological phenomenon of advancing age and very rare in children. But studies have shown that this problem is not too uncommon in children. In one study,[38] in children aged 9–15 years, with low accommodative amplitude, had severe complaints of asthenopia, headaches, diplopia, and difficulty in reading,[39] and described various diagnostic criteria and stated that insufficiency of accommodation occurs when the amplitude is reduced by more than 2 D below Duane's expected values for age. Therefore, the clinical recognition of accommodative insufficiency is important in preventing unwanted frustration in school-going children.[40] The clinician should keep his mind open where such accommodative insufficiency is suspected, especially in circumstances of certain syndromes or the child is on drugs for psychological disorders
Infacility of accommodation: As previously discussed, this is a condition in which a rapid change of accommodation from far to near and vice-versa is failing and raises symptoms of asthenopia. It differs from insufficiency in that clear vision is eventually achieved, albeit after some time.[41] If changing fixation from distance to near takes more than one second, an abnormal condition is likely to be present. Children who need to change fixation rapidly from distance to near, as is commonly done in school in viewing blackboard and then writing at near, start complaining of ocular pain or headaches after long hours in school
Fatigue of accommodation: Fatigue of accommodation is described as the inability of the ciliary muscle to maintain contraction while viewing a near target with a resulting blurring of the object and shift of accommodation towards a far point.[42] Normally, in young children, the amplitude is so much in reserve that this condition is rare. If in a child there is doubt of such a situation, then thorough cycloplegic refraction is warranted to weed out hyperopia or astigmatism. Still, the reading habits and light source should also be enquired into
Spasm of accommodation: Spasm of accommodation is a constant or intermittent involuntary and inappropriate ciliary contraction.[43] It may be unilateral or bilateral. Symptoms include distance and/or near blur, visual distortion, constant brow ache or headaches, and sometimes diplopia[41]
Paresis of accommodation: Paresis of accommodation could be partial or complete
The most common cause of paresis is the use of cycloplegic drops whether deliberate or inadvertent. It should be understood that the use of cycloplegic drops used for refraction has a duration of effect, but it may not be surprising if the effect continues well beyond the stipulated time frame. In every case of suspected cycloplegic used, whether at your clinic or elsewhere, the type and date of cycloplegic used must be enquired.
Accommodative paresis can also be functional, owing to weakness or fatigue of ciliary muscles.[34]
Near work performance can also be hampered due to accommodative syndromes stated above, neurological disorders, use of certain sedatives, anticholinergic drugs, antipsychotic drugs, hysteria, etc., The 'accommodative facility' can be inherently deficient despite the amplitude being normal.[36] Thus, a thorough test of various facets of accommodation should be done to arrive at a correct diagnosis of the accommodative problem, and to decide on the type and extent of treatment.
Accommodative Therapy
Accommodative dysfunctions are not an uncommon visual anomaly in children and the symptoms typically occur during near work. Out of the dysfunctions mentioned above, accommodative insufficiency, accommodative infacility, and accommodative fatigue are the most common dysfunctions encountered in children.[44] After ruling out neurological, pharmaceutical, and general health issues, the standard treatment of accommodative dysfunction is generally orthoptic exercises or addition of plus lens for near.
In cases of accommodative insufficiency, what is needed is a proper distance correction, addition of appropriate plus lenses for near or both.[45] Orthoptic exercises to strengthen vergence or accommodation by the 'push-up' technique should also be employed.
Addition of plus lens is recommended in cases of excessive 'lag of accommodation', 'very low PRA', or 'fatigue of accommodation'. The prescription can be either in the form of normal reading glasses or bifocals.[31]
Orthoptic exercise is a sequence of activities individually prescribed and monitored by the clinician to develop efficient visual skills and processing. Orthoptic exercise is indicated when there is spasticity in the accommodative system or accommodation is poorly controlled.[46] It is also indicated if the patient cannot clear the initial plus lens flip on the +- 2.0 D or if the NRA is low (that is, less than + 1.5 D). 'Flipper' method is one such extremely efficient method aimed at developing accommodative facility and 'push-up' exercise to strengthen vergence and accommodation. There is scientific and clinical evidence to support the efficacy of using facility therapy to 'strengthen' or improve accommodative function.[47] Use of synoptophore is a time tested machine for orthoptic exercises, but the patients' regular attendance is doubtful; even home-based exercises have proved to be equally effective and should be relied upon.
Conclusion
The knowledge of how the neuronal accommodative system functions, is still limited. The general consensus that young children or teenagers, with strong accommodative amplitudes, are immune to accommodative anomalies, is misleading. We already know that the amplitude of accommodative is quite high in young children. Furthermore, we understand that accommodation in young children is extremely flexible and resistant to fatigue. Though this old data is still what we normally believe, the ocular accommodation in children is not as sufficient or efficient as we expect. There is no simple standard procedure that includes all accommodative facets for examination. The accommodative system is, therefore, not routinely examined because of the lack of such method and more so because of the concept that there cannot be any fallacy of accommodation in children. Young school children may have an insufficient accommodative ability that causes subjective symptoms when reading. Excluding all pathological or pharmaceutical entities, a 'general weakness' in a child is enough to cause near work dysfunctions. Therefore, it is prudent and mandatory to look seriously into any complaints arising out of near work in children.
Proper cycloplegic refraction is primary to all complaints, whether or not the visual acuity is normal. After a correct lens prescription, if the complaints persist, then a thorough accommodative test should be performed. Accommodative spasm is not infrequent in an uncorrected hyperope, especially if the person is involved in excessive, long near work—as in computer work. The ordeal of 'computer vision syndrome' is now well documented. But we rarely go into the tests for accommodative anomalies arising in this syndrome.
With all said and done, near work complaints and problems are on the increase in children, courtesy computers and mobile game gadgets, and as a vigilant clinician, it is imperative that we take the near vision complaints of children seriously and make a conscious effort to look for accommodative anomalies.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
References
- 1.Weisz CL. Clinical therapy for accommodative responses. Transfer effects upon performance. Am Optom Assoc. 1979;50:209–16. [PubMed] [Google Scholar]
- 2.Brown N. The change in shape and internal form of the lens of the eye on accommodation. Exp Eye Res. 1972;15:441–59. doi: 10.1016/0014-4835(73)90136-x. [DOI] [PubMed] [Google Scholar]
- 3.Jampel RS. Representation of the near response on the cerebral cortex of the macaque. Amer J Ophthal. 1959;48:573–82. doi: 10.1016/0002-9394(59)90608-7. [DOI] [PubMed] [Google Scholar]
- 4.Von Noorden GK. The near-vision complex Theory and Management of Strabismus. 3rd ed. 5. C V Mosby and CO; 1985. pp. 85–100. [Google Scholar]
- 5.Morgan M. The clinical aspects of accommodation and convergence. Am J Optom Arch. 1944;21:301–13. [Google Scholar]
- 6.Kruger PB, Pola J. Changing target size is a stimulus for accommodation. J Optom Soc. 1985;2:1832–5. doi: 10.1364/josaa.2.001832. [DOI] [PubMed] [Google Scholar]
- 7.Rosenfield M, Ciuffreda KJ, Hung GK. The linearity of proximally induced accommodation and vergence. Invest Ophthal Vis Sci. 1991;32:2985–91. [PubMed] [Google Scholar]
- 8.Mathews S, Kruger PB. Spatio temporal transfer function of human accommodation. Visionn Res. 1994;34:1965–80. doi: 10.1016/0042-6989(94)90026-4. [DOI] [PubMed] [Google Scholar]
- 9.Rosenfield M, Cohen AS. Push-up amplitude of accommodation and target size. Ophthalmic Physio Opt. 1995;15:231–2. doi: 10.1016/0275-5408(95)90576-n. [DOI] [PubMed] [Google Scholar]
- 10.White JM, Wick B. Accommodation in humans with juvenile macular degeneration. Vision Res. 1995;35:873–80. doi: 10.1016/0042-6989(94)00181-k. [DOI] [PubMed] [Google Scholar]
- 11.Banks MS. The development of visual accommodation during early infancy. Child Dev. 1980;51:646–66. [PubMed] [Google Scholar]
- 12.Banks MS. Infant refraction and accommodation. Int Ophthal Clin. 1980;20:205–32. doi: 10.1097/00004397-198002010-00010. [DOI] [PubMed] [Google Scholar]
- 13.Hainlein L, Riddel P, Grouse J, Abramore I. Development of accommodation and convergence in infancy. Behav Brain Res. 1992;49:33–50. doi: 10.1016/s0166-4328(05)80192-5. [DOI] [PubMed] [Google Scholar]
- 14.Bobier W, Guinta A, Kurtz S, Howland HC. Prism induced accommodation in infants. Vision Res. 2000;40:529–37. doi: 10.1016/s0042-6989(99)00196-0. [DOI] [PubMed] [Google Scholar]
- 15.Duane A. Normal values of accommodation at all ages. J Am Med Assoc. 1912;59:1010–3. [Google Scholar]
- 16.Hoffstetter HW. Useful age –amplitude formula. Optom World. 1950;38:42–5. [Google Scholar]
- 17.Rouse MW, Hutter RF, Shiftlett R. A normative study of accommodative lag in elementary school children. Am J Optom Physiol. 1984;61:693–7. doi: 10.1097/00006324-198411000-00008. [DOI] [PubMed] [Google Scholar]
- 18.Rosner J, Rosner J. Relation between tonic accommodation and visual perceptual skills development in 6-12 year children. Optom Vis Sci. 1989;66:526–9. doi: 10.1097/00006324-198908000-00006. [DOI] [PubMed] [Google Scholar]
- 19.Von Noorden GK, Avilla CW. Accommodative convergence in hypermetropia. Am J Ophthalmol. 1990;110:287–92. doi: 10.1016/s0002-9394(14)76346-9. [DOI] [PubMed] [Google Scholar]
- 20.Miwa T, Tokora T. Dark focus of accommodation in children with accommodative esotropia and hyperopic anisometropia. Acta Ophthalmol (Copenh) 1993;71:819–24. doi: 10.1111/j.1755-3768.1993.tb08606.x. [DOI] [PubMed] [Google Scholar]
- 21.Rosenfield M, Ciuffreda KJ, Gilmartin B. Factors affecting accommodative adaptation. Optom Vis Sci. 1992;69:270–5. doi: 10.1097/00006324-199204000-00003. [DOI] [PubMed] [Google Scholar]
- 22.Chiu NN, Rosenfield M. Tonic accommodation, tonic vergence, and surround propinquity. Ophthalmic Physiol Optics. 1994;14:290–2. doi: 10.1111/j.1475-1313.1994.tb00010.x. [DOI] [PubMed] [Google Scholar]
- 23.Gray LS, Gilmartin B, Winn B. The magnitude and distribution of open-loop accommodation using three different methods of opening the loop. Optom Vis Sci. 1998;75:897–902. doi: 10.1097/00006324-199812000-00012. [DOI] [PubMed] [Google Scholar]
- 24.Wick B, Hall P. Relation among accommodative facility, lag, and amplitude in elementary school children. Am J Optom Physiol. 1987;64:593–8. doi: 10.1097/00006324-198708000-00005. [DOI] [PubMed] [Google Scholar]
- 25.Goss D, Zhai H. Clinical and laboratory investigations of the relationship of accommodation and convergence. Doc Ophthalmol. 1994;86:349–80. doi: 10.1007/BF01204595. [DOI] [PubMed] [Google Scholar]
- 26.Tseutaki TK, Schor CM. Clinical method for measuring adaptation of tonic accommodation and vergence accommodation. Am J Optom Physiol. 1987;64:437–49. doi: 10.1097/00006324-198706000-00009. [DOI] [PubMed] [Google Scholar]
- 27.McKenzie KM, Kerr SR, Rouse MW. Study of accommodative facility testing reliability. Am J Optom Physiol Opt. 1987;64:186–94. doi: 10.1097/00006324-198703000-00005. [DOI] [PubMed] [Google Scholar]
- 28.Jackson T, Goss D. Variation and correlation of clinical tests of accommodative function in school age children. J Am Optom Assoc. 1991;62:857–66. [PubMed] [Google Scholar]
- 29.Gettes BC. Accommodation-Practical Refraction. 4. New York, USA: Grunne and Straton; 1957. [Google Scholar]
- 30.Hung GK, Ciffureda KJ. Sensitivity analysis of relative accommodation and vergence. Trans Biomed Eng. 1994;41:241–8. doi: 10.1109/10.284942. [DOI] [PubMed] [Google Scholar]
- 31.Weisz CL. How to find and treat accommodative disorders. Rew Optom. 1983:2:48–54. [Google Scholar]
- 32.Flax N. The contribution of visual problems to learning disability. J Am Optom Assoc. 1970;41:841–3. [PubMed] [Google Scholar]
- 33.Sucher DF, Stewart J. Vertical fixation disparity in learning disabled. Optom Vis Sci. 1993;70:1038–42. doi: 10.1097/00006324-199312000-00008. [DOI] [PubMed] [Google Scholar]
- 34.Duke-Elder S. Paresis of accommodation System of Ophthalmology. Vol. 12. London: Henry Kimpton; 1971. [Google Scholar]
- 35.Hoffman LG, Rouse M. Refarral recommendations for binocular vision. Am J Optom Sci. 1980;51:119–26. [PubMed] [Google Scholar]
- 36.Hennesay D. Relation of symptoms to accommodative infacility in school children. Am J Optom Sci. 1984;61:177–83. doi: 10.1097/00006324-198403000-00005. [DOI] [PubMed] [Google Scholar]
- 37.Daum KM. Accomodative insufficiency. Am J Optom Physiol. 1983;60:352–8. doi: 10.1097/00006324-198305000-00002. [DOI] [PubMed] [Google Scholar]
- 38.Matsau T, Ohatsuki H. Accommodative and convergence insufficiency in school going children. Arch Clin Exp Ophthalmol. 1992;230:166–70. doi: 10.1007/BF00164657. [DOI] [PubMed] [Google Scholar]
- 39.Morgan MW. Analysis of clinical data. Am J Optom Arch. 1944;21:477–90. [Google Scholar]
- 40.Chrousos G, O'Neil J. Accomodation deficiency in healthy young indivisuals. J Ped Ophthalmol Strab. 1988;25:177–80. doi: 10.3928/0191-3913-19880701-07. [DOI] [PubMed] [Google Scholar]
- 41.Michaels DD. Accommodation: Clinical aspects. Am Acad Ophthalmol Focal Points. 1987:5. [Google Scholar]
- 42.Piguen RG, Miller RJ. Fatigue of accommodation: Changes in accommodation after visual work. Am J Optom Physiol. 1985;62:853–63. [PubMed] [Google Scholar]
- 43.Goldstein JH, Schneekloth BB. Spasm of near reflex. Surv Ophthal. 1996;40:269–78. doi: 10.1016/s0039-6257(96)82002-9. [DOI] [PubMed] [Google Scholar]
- 44.Suchoff IB, Petito GT. The efficacy of visual therapy. J Am Optom Assoc. 1986:70–100. [PubMed] [Google Scholar]
- 45.Goss DA. Clinical accommodation testing. Curr Opin Ophthalmol. 1992;3:78–283. doi: 10.1097/00055735-199202000-00011. [DOI] [PubMed] [Google Scholar]
- 46.Cooper J, Feldman J, Selenow A. Reduction of asthenopia after accommodative facility training. Am J Optom Physiol. 1987;64:430–6. doi: 10.1097/00006324-198706000-00008. [DOI] [PubMed] [Google Scholar]
- 47.Liu JS, Lee M, Lang G, Ciuffreda KJ. Objective assessment of accommodation orthoptics. Am J Orthop Physiol. 1979;56:285–94. doi: 10.1097/00006324-197905000-00002. [DOI] [PubMed] [Google Scholar]