

Abstract
Purpose:
The aim of this study was to test the discomfort experienced during intravitreal injections with eyelid retraction between an eyelid speculum, cotton-tipped applicator (CTA), and unimanual eyelid retraction techniques.
Methods:
In total, 99 patients receiving intravitreal bevacizumab were enrolled into this prospective study. Participants were randomized to one of the three methods, given subconjunctival 2% lidocaine and then injected in the superior temporal quadrant. Immediately after the procedure, each patient was given a visual analog scale (VAS) to rate their discomfort.
Results:
The mean pain scores for eyelid retraction with unimanual, CTA, and speculum groups were 0.788 (standard deviation [SD] 0.70, 95% confidence interval [CI] 0.448–1.128), 0.945 (SD 1.28, 95% CI 0.600–1.291), and 1.561 (SD 1.28, 95% CI 1.210–1.912), respectively. A one-way analysis of variance (ANOVA) test revealed a significant difference between the groups (P = 0.006). Post hoc analysis also revealed a difference in mean pain scores between the speculum and both the CTA and the unimanual methods.
Conclusion:
Our study shows that the unimanual and CTA methods for eyelid retraction are significantly less painful for patients compared to the speculum method. Patient comfort is of the utmost importance as intravitreal injections are performed millions of times a year with most patients requiring multiple injections.
Keywords: Cotton-tipped applicator, eyelid retraction, eyelid speculum, intravitreal injection, unimanual, visual analog scale
Patient comfort is an important factor in compliance and satisfaction. With millions of intravitreal injections (IVIs) performed each year, even small improvements in patients' experiences could lead to significant benefit. During the process of an IVI, the method of eyelid retraction has been shown to be one of the most significant aspects of discomfort for patients.[1]
Many ophthalmologists use an eyelid speculum to retract the eyelids, but potentially more comfortable methods exist such as the bimanual-assisted eyelid retraction,[2] conjunctival mold,[3] Desmarres Lid Retractor,[4] and the cotton-tipped applicator (CTA) lid retraction method.[5,6] The purpose of our study was to test the comfort of both the CTA eyelid retraction method, which has yet to be evaluated, and the unimanual lid retraction, which has not been described in the literature but is performed by many ophthalmologists.
Methods
Between October 2017 and March 2018, participants receiving IVIs of bevacizumab (1.25 mg/0.05 mL) were enrolled into a prospective randomized control study. The study was approved by the Institutional Review Board and informed consent was obtained from all patients. The inclusion criteria of the study were adult patients receiving 30-gauge IVIs in the superior temporal quadrant. The exclusion criteria of the study were patients with a povidone-iodine allergy or sensitivity and those with prior ocular surgery other than uncomplicated cataract surgery.
The unimanual eyelid retraction method involves using one finger to manually elevate the superior eyelid [Fig. 1a]. A speculum may also be used to retract both the upper and lower eyelids [Fig. 1b]. The CTA method for lid retraction consists of using a CTA soaked in 5% povidone-iodine and tetracaine being placed under the lateral one-third of the eyelid [Fig. 1c]. The wood handle remains unaided in place for 30 s, at which point it is used as a lever to elevate the superior eyelid away from the injection site and provide stability to the globe [Fig. 1d].
Figure 1.
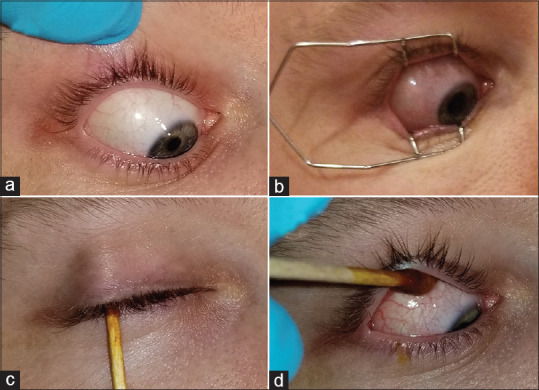
Methods of eyelid retraction. The unimanual eyelid retraction method consists of using one finger to manually elevate the superior eyelid (a). A speculum may also be used to retract both the upper and lower eyelids (b). The cotton-tipped applicator (CTA) method for lid retraction consists of using CTA soaked in 5% povidone-iodine and tetracaine placed in the lateral one-third of the eyelid (c). The wood handle remains unaided in place for 30 s, at which point it is used as a lever to elevate the superior eyelid away from the injection site and provide stability to the globe (d)
After agreeing to the study, a random number generator was used to allocate the patient to eyelid retraction by speculum, unimanual, or CTA method. Preinjection preparation was standardized with all the patients: Selection of music choice via an online streaming service was made by the patient, 1 drop of tetracaine was placed in the inferior fornix, a small bleb of subconjunctival 2% lidocaine was created 5–8 mm posterior to the injection site, then multiple drops of 5% povidone-iodine were placed onto the injection site for 90 s. Those patients in the CTA group had a CTA soaked in 5% povidone-iodine and 1 drop of tetracaine placed at the injection site and left for 30 s, as seen in Fig. 1c then it was used as a lever to elevate the upper eyelid and the IVI was performed. For participants in the unimanual and speculum groups, patients had 1 more drop of tetracaine and 5% povidone-iodine placed onto the injection site immediately prior the injection.
Following the IVI, all patients had their eyes thoroughly rinsed with eyewash solution. Within 1 min of the injection, the patient was given a standard 100-mm-long visual analog scale (VAS) and asked to rate their pain from 0 mm (no pain) to 100 mm (the worst pain) regarding the entire process of the IVI.
An analysis of variance (ANOVA) test revealed that for a significance of 5% and power of 80%, 81 participants would need to be enrolled; we decided to enroll total 99 patients to help ensure that a difference would be found between the groups. An ANOVA test was used to compare the pain scale means of three groups and Tukey–Kramer test was used for a post hoc analysis. A t test was then used to compare the pain scale means of treatment naïve to those with prior injections.
Results
A total of 99 patients were enrolled (45 men, 54 women, mean age 64.5 years, range 47–88), with the manual, CTA, and speculum groups having 34, 32, and 33 patients, respectively. The mean pain scores for eyelid retraction with unimanual, CTA, and speculum groups were 0.788 (standard deviation [SD] 0.70, 95% confidence interval [CI] 0.448–1.128), 0.945 (SD 1.28, 95% CI 0.600–1.291), and 1.561 (SD 1.28, 95% CI 1.210–1.912), respectively [Fig. 2]. A one-way ANOVA test revealed a significant difference between the groups (P = 0.006). Post hoc analysis with Tukey–Kramer test revealed a difference in mean pain scores between the speculum and both the CTA and the unimanual methods.
Figure 2.
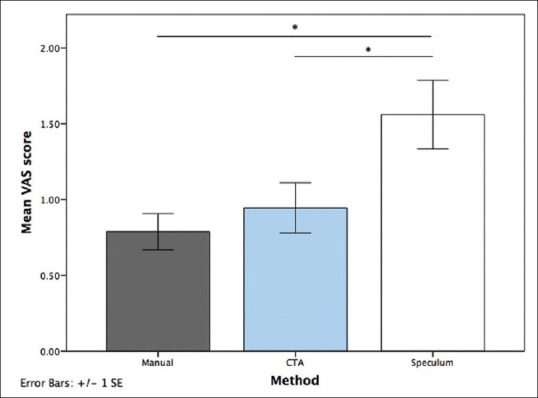
Discomfort associated with eyelid retraction. The mean visual analog scale (VAS) of pain scores for the unimanual, cotton-tipped applicator (CTA), and eyelid speculum groups are shown with standard error (SE) bars. A significant difference was observed between the speculum group and both the unimanual and CTA methods
The average number of injections prior to being included in this study was 4.814 (range 1–23) with 33 patients being treatment naïve. There were 13, 7, and 11 treatment naïve patients in the unimanual, speculum, and CTA groups and t test did not reveal any difference in the mean pain scores between naïve participants and those who had prior injections at the time of recruitment (P = 0.58).
No patients in any group had endophthalmitis, lens touch, retinal tear or detachment.
Discussion
The eyelid speculum may be useful for patients receiving intravitreal implants as they necessitate more ocular manipulation or in patients that squeeze heavily. However, for most patients needing IVIs, we recommend considering a more comfortable method to improve patient satisfaction. Our results show that the CTA and unimanual eyelid retraction methods are significantly more comfortable than an eyelid speculum.
The CTA and unimanual eyelid retraction methods have the additional benefits of not requiring a second provider, as is needed with the bimanual method,[2] or any instruments that need replacement[3] or sterilization such as an eyelid speculum. These two methods also expose the anesthetized cornea to the air for a minimal duration compared to the speculum, which may improve comfort after the anesthesia effect dissipates. The CTA method is quick and an efficient method with the added benefits that it stabilizes the globe.
The CTA and unimanual eyelid retraction methods are most easily used in the superior temporal quadrant; therefore, the speculum group received injections in the superior temporal quadrant for consistency. Although no significant subconjunctival hemorrhages were identified in any patients included in this study, we have found that when they do occur, they are less noticeable when located superiorly as they are covered by the eyelid.
In our clinic, we routinely use topical anesthesia rather than subconjunctival lidocaine as it is efficient and effective. However, subconjunctival 2% lidocaine has been shown to be most effective in decreasing discomfort during IVIs[7,8] and therefore was selected as the method for anesthesia in this study so that the discomfort experienced by participants would be more reflective of the eyelid retraction rather than other steps of the procedure.
While comfort is important to consider with IVIs, the most important aspect is to ensure a low risk of endophthalmitis. The eyelids and eyelashes are a source of injection and must be retracted during IVIs.[9] The unimanual eyelid retraction method presented here is very similar to the lid splinting eyelid retraction technique that has been described by Munro et al. In their study, 78,009 patients had IVIs with the lid splinting technique with 12 cases (0.015%) of endophthalmitis, which is similar to reported rates with speculum use.[10] Regardless of the method used to retract the eyelids, it is imperative to have the eyelids retracted, and if there is concern for a patient to squeeze heavily during the procedure, a speculum may be warranted in that patient.
The strengths of this study include its prospective design, randomization, large sample size, and standardization of procedures. It is limited in that it was not blinded, VAS of pain is subjective, and we did not control for patients that were treatment naïve. However, a subsequent analysis revealed that that there was no difference between naïve patients and those with prior injections (P = 0.58).
Conclusion
In conclusion, the CTA and unimanual eyelid retraction methods were significantly more comfortable for patients as compared with the speculum method. These two methods may be performed without an assistant and no equipment requires sterilization. We believe that preferentially using these two methods as opposed to the eyelid speculum may allow better compliance of patients with IVIs and achieve maximization of their visual potential since many patients require multiple injections.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
Footnotes
Clinical Trial Registration: NCT04144985 (https://clinicaltrials.gov/ct2/show/NCT04144985?term = eyelid + retraction&draw = 2 and rank=1)
References
- 1.Tailor R, Beasley R, Yang Y, Narendran N. Evaluation of patients' experiences at different stages of the intravitreal injection procedure––What can be improved? Clin Ophthalmol. 2011;5:1499–502. doi: 10.2147/OPTH.S24358. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Fineman MS, Hsu J, Spirn MJ, Kaiser RS. Bimanual assisted eyelid retraction technique for intravitreal injections. Retina. 2013;33:1968–70. doi: 10.1097/IAE.0b013e318287da92. [DOI] [PubMed] [Google Scholar]
- 3.Ratnarajan G, Nath R, Appaswamy S, Watson SL. Intravitreal injections using a novel conjunctival mould: A comparison with a conventional technique. Br J Ophthalmol. 2013;97:395–7. doi: 10.1136/bjophthalmol-2012-302155. [DOI] [PubMed] [Google Scholar]
- 4.Mason RW. Use of a Desmarres retractor for upper lid and lash isolation during intravitreal injections. Retina. 2013;33:2175–6. doi: 10.1097/IAE.0b013e3182999a1b. [DOI] [PubMed] [Google Scholar]
- 5.Shrier E, Raevis J, Li J, Yazdanyar A, Azam Z, Fahd Y. Safety of superior-temporal intravitreal injection using the cotton-tip applicator lid-retraction technique. J Ocular Biol. 2017;5:1–4. [Google Scholar]
- 6.Shrier E. Cotton-tip applicator lid retraction technique for controlled intravitreal injection. Retina. 2014;34:1244–6. doi: 10.1097/IAE.0000000000000219. [DOI] [PubMed] [Google Scholar]
- 7.Andrade G, Carvalho A. Comparison of 3 different anesthetic approaches for intravitreal injections: A prospective randomized trial. Arg Bras Oftalmol. 2015;78:27–31. doi: 10.5935/0004-2749.20150008. [DOI] [PubMed] [Google Scholar]
- 8.Shiroma HF, Takaschima AKK, Farah ME, Höfling-Lima AL, de Luca Canto G, Benedetti RH, et al. Patient pain during intravitreal injections under topical anesthesia: A systematic review. Int J Retina Vitreous. 2017;3:23. doi: 10.1186/s40942-017-0076-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Avery RL, Bakri SJ, Blumenkranz MS, Brucker AJ, Cunningham ET, Jr, D'Amico DJ, et al. Intravitreal injection technique and monitoring: Updated guidelines of an expert panel. Retina. 2014;12:S1–18. doi: 10.1097/IAE.0000000000000399. [DOI] [PubMed] [Google Scholar]
- 10.Munro M, Williams GR, Ells A, Fielden M, Kherani A, Mitchell P, et al. Lid splinting eyelid retraction technique: A minimised sterile approach for intravitreal injections. Br J Ophthalmol. 2018;102:1254–8. doi: 10.1136/bjophthalmol-2017-311081. [DOI] [PubMed] [Google Scholar]