

Abstract
A direct and quantitative linkage of air pollution-related health effects to emissions from different sources is critically important for decision-making since protecting public health is a final goal of air pollution controls. While many studies have attributed the PM2.5-related health effects to emission sources, they have seldom examined the complicated nonlinear relations between the two. Here we investigate the nonlinear relationships between PM2.5-related premature mortality in the Beijing-Tianjin-Hebei (BTH) region, one of the most polluted regions in the world, and emissions of multiple pollutants from multiple regions and sectors, through a combination of a chemical transport model, an extended response surface model, and concentration-response functions. In the BTH region, 129.2 thousand and 18.7 thousand people die annually due to long-term and short-term exposures to PM2.5, respectively. Among all pollutants, both long-term and short-term mortalities are most sensitive to emissions of primary inorganic PM2.5 (defined as all chemical components of primary PM2.5 other than organics), followed by NH3, nonmethane volatile organic compounds and intermediate volatility organic compounds (NMVOC+IVOC), and primary organic aerosol (POA). The sensitivities of long-term mortality to emissions of primary inorganic PM2.5, NH3 and NOx increase significantly with the increase of reduction ratio, while the sensitivities to POA, NMVOC+IVOC and SO2 roughly remain constant at various reduction ratios. The emissions of primary inorganic PM2.5, especially those from residential and commercial sources, contribute a larger fraction of mortality in winter than in other seasons. When emissions of multiple pollutants or those from both local and nonlocal emissions are controlled simultaneously, the sensitivity of long-term mortality substantially increases with the increase of reduction ratio, and this sensitivity is much larger than the arithmetic sum of the sensitivities to emissions of individual pollutants or from individual regions. In order to achieve large marginal health benefits, we suggest that stringent control measures on primary PM2.5 emissions should be enforced (especially in winter), that NOx emissions should be jointly controlled over a larger region beyond BTH, and that multi-pollutant and regional collaboration control strategies should be implemented.
Keywords: PM2.5, health effect, CMAQ/2D-VBS, Beijing-Tianjin-Hebei region, Extended Response Surface Model (ERSM)
1. Introduction
Atmospheric fine particle (PM2.5) pollution has adverse effects on human health (Shang et al., 2013; Lelieveld et al., 2015). The effects are especially important in the Beijing-Hebei-Tianjin (BTH) urban agglomeration region, one of the most heavily polluted regions in China (Wang et al., 2017; Cai et al., 2017). It’s estimated that monetize health losses caused by PM2.5 pollution in the BTH region can reach 134.3 billion RMB, which accounts for 2.16% of the GDP in this region (Lv and Li, 2016). Protecting public health is the ultimate goal of air pollution control. Therefore, it is crucially important for environmental decision making to quantitatively link the PM2.5-related health impacts to air pollutant emissions from different sources.
PM2.5 pollution is formed through complex physical and chemical processes. As a result, the relationships between PM2.5 concentrations and emissions of precursors are nonlinear, and the nonlinearity is especially significant in urban agglomerations (Zhao et al., 2015; Zhao et al., 2017; Xing et al., 2017). In addition, many studies (Martenies et al., 2015; Burnett et al., 2014; Burnett et al., 2018) pointed out that the relationships between PM2.5 concentrations and the resulting health effects are also nonlinear. When these two relationships are overlaid, we can expect highly nonlinear relationships between the PM2.5-associated health effects and the emissions of precursors. Quite a few studies (Fann et al., 2012; Wang et al., 2015; Heo et al., 2016; Andersson et al., 2009) have attributed the PM2.5-associated health effects to emission sources, but to be best of knowledge, none of them have explicitly considered the aforementioned nonlinear relationships, which brings inaccuracy to the source attribution results. Therefore, it’s a meaningful and also challenging scientific issue to quantify the complex nonlinear responses of PM2.5-related health impacts in urban agglomerations to emissions of key individual precursors from major emission sources.
In this study, we quantitatively evaluate the nonlinear relationships between premature mortality caused by long-term/short-term exposures to PM2.5 in the BTH region and emissions of multiple air pollutants from multiple regions and sectors, by combining a three-dimensional air quality model, concentration-response functions, and a response surface modeling technique. Based on these assessment results, we provide policy suggestions that maximize the marginal benefits on public health.
2. Methods
2.1. Health impact assessment methodology
In this study, we estimate the health effects due to both short-term and long-term exposures to ambient PM2.5. For long-term health impact assessment, Burnett et al. (2014) proposed integrated expose-response (IER) function, which were constructed by combining risk estimates from studies of ambient and household air pollution, and active/second-hand smoking that cover a full range of PM2.5 exposure up to about 30000 μg/m3 (Cohen et al., 2017; Burnett et al., 2014). The IER function is given by Eq. 1, which has been proved to fit best to the actual risk estimates among a variety of equation forms (Cohen et al., 2017; Burnett et al., 2014).
| (1) |
where ΔYi refers to PM2.5-induced mortality from endpoint i; y0,i refers to the actual mortality rate of endpoint i at the current PM2.5 concentration (C); P refers to exposed population; C0 refers to threshold PM2.5 concentration below which no health impact is expected. αi, γi, and δi are regression parameters for endpoint i. According to the IER function, the change in mortality due to a unit concentration change decreases significantly with the deterioration of PM2.5 pollution. Recently, Burnett et al. (2018) developed new concentration-response functions for long-term PM2.5 exposures based on only cohort studies of ambient air pollution, which resulted in larger mortality estimates. However, this would not change our major conclusions about the nonlinear emission-mortality relationships, since the general shape of the functions retained. In this study, we adopt the same health endpoints and IER parameters (αi, γi, and δi) as Burnett et al. (2014). These endpoints include ischemic heart disease (IHD), chronic obstructive pulmonary disease (COPD), lung cancer, and stroke. The disease specific baseline mortality rates by age and gender are obtained from the from Institute of Health Metrics and Evaluation (Global Burden of Disease Collaborative Network, 2017).
For health impact assessment of short-term exposure to PM2.5, the concentration-response relationships are derived in epidemiological studies based on time series analysis of PM2.5 and health. In most studies (Shang et al., 2013; Wang et al., 2015; Dominici et al., 2002; Kan and Chen, 2004), the incidence of mortality caused by air pollution is considered to be subject to Poisson distribution. Subsequently, the relationship between mortality and PM2.5 concentrations can be regressed in the following form by using Poisson regression (log-linear regression) or similar methods (Kan et al., 2008; Dominici et al., 2002; Shang et al., 2013; Kan and Chen, 2004).
| (2) |
where ΔYi, y0,i, P, C, and C0 have the same meaning as defined above. βi is a regression coefficient derived from epidemiological studies, which refers to excess risk of mortality per each increase in 1 μg/m3 of PM2.5. Reasonable regression results have been obtained using Eq. 2 in over 25 epidemiological studies conducted in China (Shang et al., 2013), where the PM2.5 concentrations range from very small to very large (mean concentration > 170 μg/m3), indicating the applicability of Eq. 2 to the Chinese environments. Based on Eq. 2, the relationship between ΔYi and C presents a slightly convex function form, indicating subtly less marginal effect at larger concentration increase. The health endpoints considered in the short-term assessment include all-cause mortality, respiratory mortality, and cardiovascular mortality. The baseline mortality rates are derived from China Health and Family Planning Statistics Yearbook 2015 (National Health and Family Planning Commission of China, 2015) and Huang and Zhang (2013), and the parameter estimates are taken from Chen et al. (2011). It should be noted that, in addition to mortality, the short-term PM2.5 exposure also leads to various types of morbidity (e.g., cardiovascular and respiratory hospital admissions or outpatients). We focus on mortality in the present study since it accounts about 80% of the total monetized health losses (Kan and Chen, 2004; Wu, 2016). It’s also worth noting that the estimation methods of both long-term and short-term mortality assume that the health effects depend only on the inhaled amount of PM2.5 and are independent of the chemical composition, which appears reasonable in view of the available quantitative epidemiological studies. However, some studies have reported that some aerosol species, such as the carbonaceous aerosols, could be significantly more toxic than others (Tuomisto et al., 2008; Lelieveld et al., 2015). This relative toxicity of different aerosol species may affect the relative contributions of different emission sources to PM2.5-related mortality, which warrants further in-depth study.
The age-specific population data at city level in 2014 are acquired from the statistical bureaus of Beijing, Tianjin and Hebei, and the sub-city distribution of population is based on the LandScan dataset at 30”×30” (approximately 1 km×1 km) resolution (Oak ridge national laboratory, 2016). The spatial distribution of population is shown in Fig. S1. To give the uncertainty of the health effects, we calculate 95% confidence intervals (CIs) using 95% CIs of the parameters of the concentration-response functions for both short-term and long-term assessments.
We use sensitivity analysis method for health effect source apportionment. The sensitivity of health effects to emissions can be calculated with the following formula:
| (3) |
Where Si,j refers to the sensitivity of health endpoint i to emission source j; Rj refers to the ratio of emissions from source j to the base-case emissions; Hi,j is the health effect of endpoint i when the emission ratio of source j is Rj; Hi,0 refers to the health effect in the base case. For each emission source, we calculate Si,j for reduction ratios (1−Rj) of 10%, 30%, 50%, 65%, 80% to assess the nonlinear relationships between health effects and emission reductions.
2.2. Determination of exposed concentrations
The exposed concentrations of PM2.5 is one of the most important input variables in health effect assessment. Three-dimensional chemical transport models (CTMs) such as the Community Multi-scale Air Quality (CMAQ) model are frequently used to obtain exposed pollutant concentrations under specific emission scenarios. To improve the simulation of secondary organic aerosol (SOA), Zhao et al. (2016) incorporated the two-dimensional volatility basis set (2D-VBS) framework in CMAQ and developed the CMAQ/2D-VBS model. In this study, we use CMAQ/2D-VBS to obtain exposed concentrations of PM2.5 to evaluate the health effects in the base case.
The simulation period is January, March, July and October in 2014, representing four seasons. The Weather Research and Forecasting (WRF) model version 3.7 is used to simulate the meteorological field to provide input data for the CMAQ/2D-VBS model. The configurations of WRF and CMAQ/2D-VBS and the emission inventory used in this paper are same as Zhao et al. (2017). We apply double-nesting simulation domains, with grid resolutions of 36 km×36 km and 12 km×12 km. The first domain covers China and its surrounding areas, and the second domain covers the BTH region, as shown in Fig. 1. The simulated results from WRFv3.7 and CMAQ/2D-VBS model generally agree well with ground observations (Zhao et al., 2017).
Fig. 1.
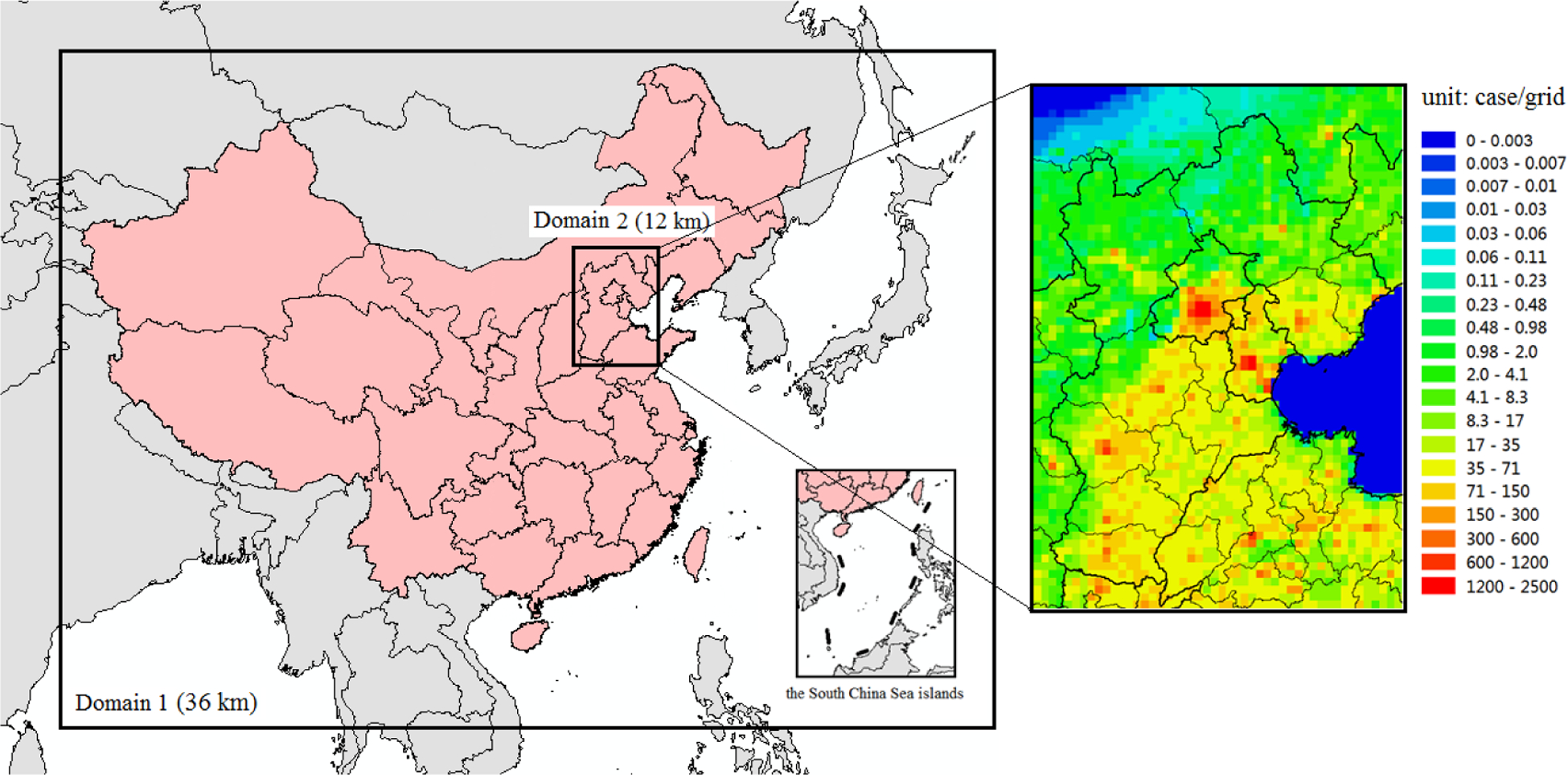
The simulation domain in this study (left) and the spatial distribution of deaths from stroke due to long-term exposure to PM2.5 pollution in the BTH region (right).
The 3-D CTM modeling is time-consuming and expensive when being used in source apportionment, so it’s not efficient to support decision making. The Extended Response Surface Modeling (ERSM) method established by Zhao et al. (2015) uses hundreds of simulation scenarios from a CTM and advanced statistical techniques to enable quick prediction of PM2.5 concentrations in any given emission scenario, and it shows good performances in several recent studies (Zhao et al., 2015; Zhao et al., 2017; Xing et al., 2017). In this study, we use the ERSM technique to acquire exposed concentration in multiple emission scenarios to comprehensively assess the complex nonlinear relationships between various emission sources and PM2.5-related mortality.
The establishment and validation of ERSM in the BTH region have been described in Zhao et al. (2017), so we only summarize several key points. First, we defined 5 target regions in the BTH region, i.e., Beijing, Tianjin, Northern Hebei, Eastern Hebei, and Southern Hebei (see Fig. 1). Next, we used 1121 scenarios simulated by CMAQ/2D-VBS to establish the ERSM prediction system, which maps atmospheric PM2.5 concentrations versus emissions of 55 combinations of regions, sectors, and pollutants. We assessed the performance of the ERSM prediction system using the “out-of-sample” and 2D-isopleths validation methods, and showed satisfying accuracy and stability of the prediction system.
3. Results and Discussion
3.1. Health effects in the base case
The long-term PM2.5-associated mortality from COPD, IHD, lung cancer, and stroke in the BTH region are shown in Fig. 2.
Fig. 2.
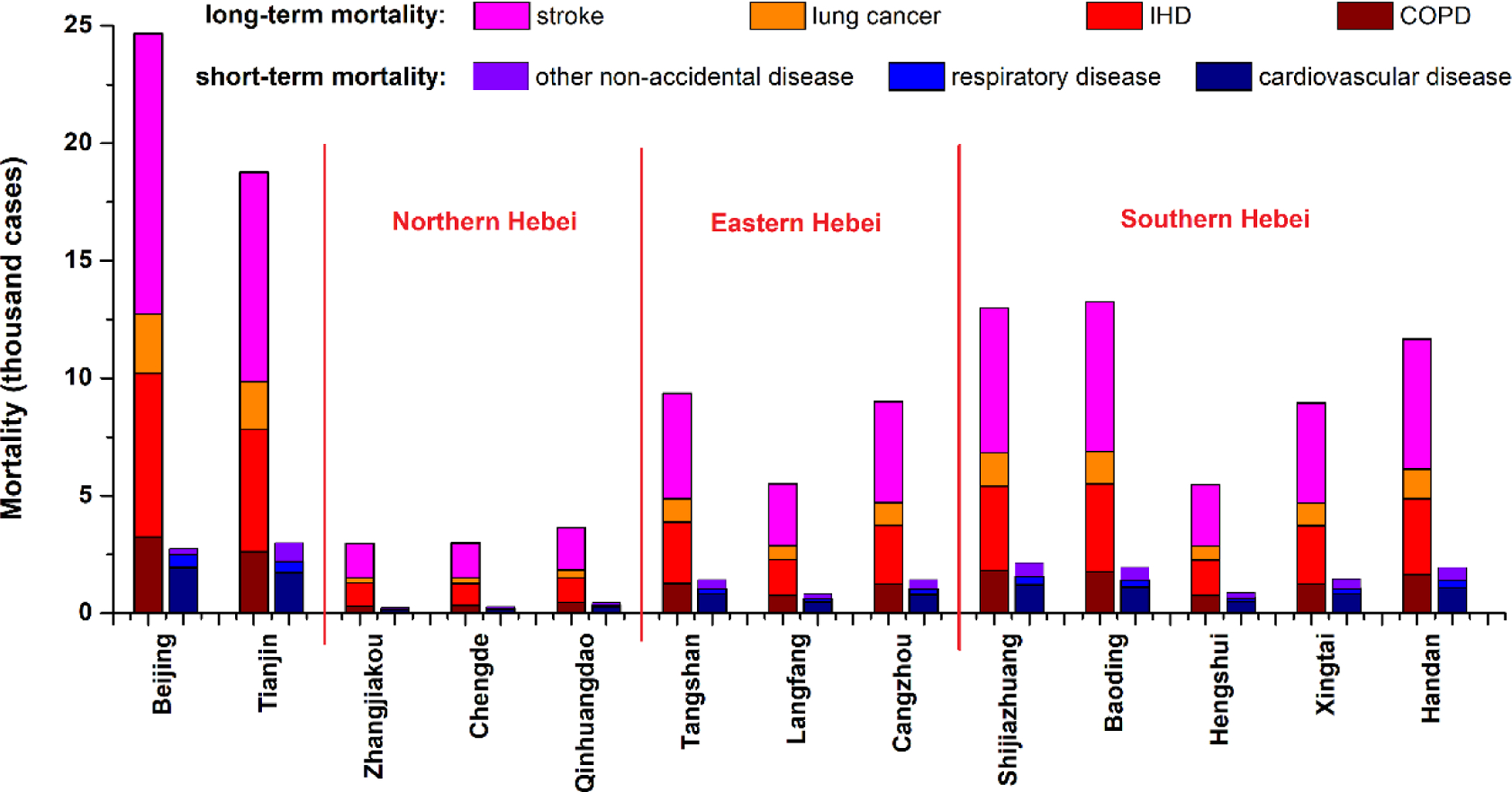
Premature mortality due to PM2.5 pollution in the BTH region. The two sets of colored bars for each city refer to mortality due to long-term and short-term exposures, respectively. Only median values of the mortality estimates are displayed in this figure.
According to our assessment, 17.42 (95% CI, 9.45–24.40) thousand, 36.29 (27.24–48.48) thousand, 13.53 (5.19–18.19) thousand, and 61.91 (27.71–79.93) thousand people die of COPD, IHD, lung cancer, and stroke due to long-term exposure to PM2.5 in the BTH region annually. Stroke is the most important health endpoint, accounting for 48% of the total premature deaths due to long-term exposure. Beijing, Tianjin, and cities in Southern Hebei are areas where people most severely suffer from PM2.5-related mortality, and Zhangjiakou, Chengde, Qinhuangdao are cities with the least mortality.
For the long-term exposure to PM2.5, the air pollution seems like a background that chronically affect people who live in the region. The short-term exposure to PM2.5, however, is quite different, because it raises more concerns when heavy pollution episode occurs. As Fig. 2 shows, 18.72 (11.20–25.65) thousand people die due to short-term exposure to PM2.5 in the BTH region annually, among which 59% and 16% die of cardiovascular and respiratory diseases, respectively. Similar to long-term effects, the majority of short-term health effects come from Beijing, Tianjin, and cities in Southern Hebei.
We also assess the spatial distribution of health effects due to PM2.5 pollution, and the long-term mortality from stroke is shown in Fig. 1. The spatial distribution characteristics of short-term mortality is highly similar (Fig. S2). Comparing the spatial distribution of the health effects with population and PM2.5 concentrations (Fig. S1), we can conclude that the health effects are strongly correlated with population. For this reason, high mortality appears in urban areas.
3.2. Nonlinear relationships between air pollutant emissions and health effects
We assess the nonlinearity between pollutant emissions control and health effects using the ERSM technique and the sensitivity analysis method described in Sections 2.1 and 2.2. For long-term exposure, to simplify the analysis, we sum up the mortality from COPD, IHD, lung cancer, and stroke to approximately represent the total PM2.5-related mortality. As shown in Fig. 3, among all pollutants, the annual mortality due to long-term exposure to PM2.5 is most sensitive to emissions of primary inorganic PM2.5, which is defined as all chemical components of primary PM2.5 other than organics, including black carbon, metals, crustal elements, etc. Primary organic aerosol (POA) is treated separately because it undergoes chemical reactions and produces SOA in the CMAQ/2D-VBS model, whereas primary inorganic PM2.5 is assumed to be chemically inert. Among all sources of primary inorganic PM2.5, the industry sector makes the largest contribution, followed by the residential and commercial sectors, while the contribution from power plants is negligible. The sensitivity of mortality to primary inorganic PM2.5 emissions increases gradually by ~20% when the emission reduction ratio increases from 10% to 80%. In contrast, the sensitivity of PM2.5 concentrations remains constant regardless of reduction ratio according to our previous study (Zhao et al., 2017). The difference is explained by the fact that the mortality reduction due to a unit drop of PM2.5 concentration is larger at lower PM2.5 concentration range, according to the curvilinear shape of the IER function. For this reason, emission of primary inorganic PM2.5 are expected to be controlled as stringent as possible to efficiently reduce the long-term mortality.
Fig. 3.
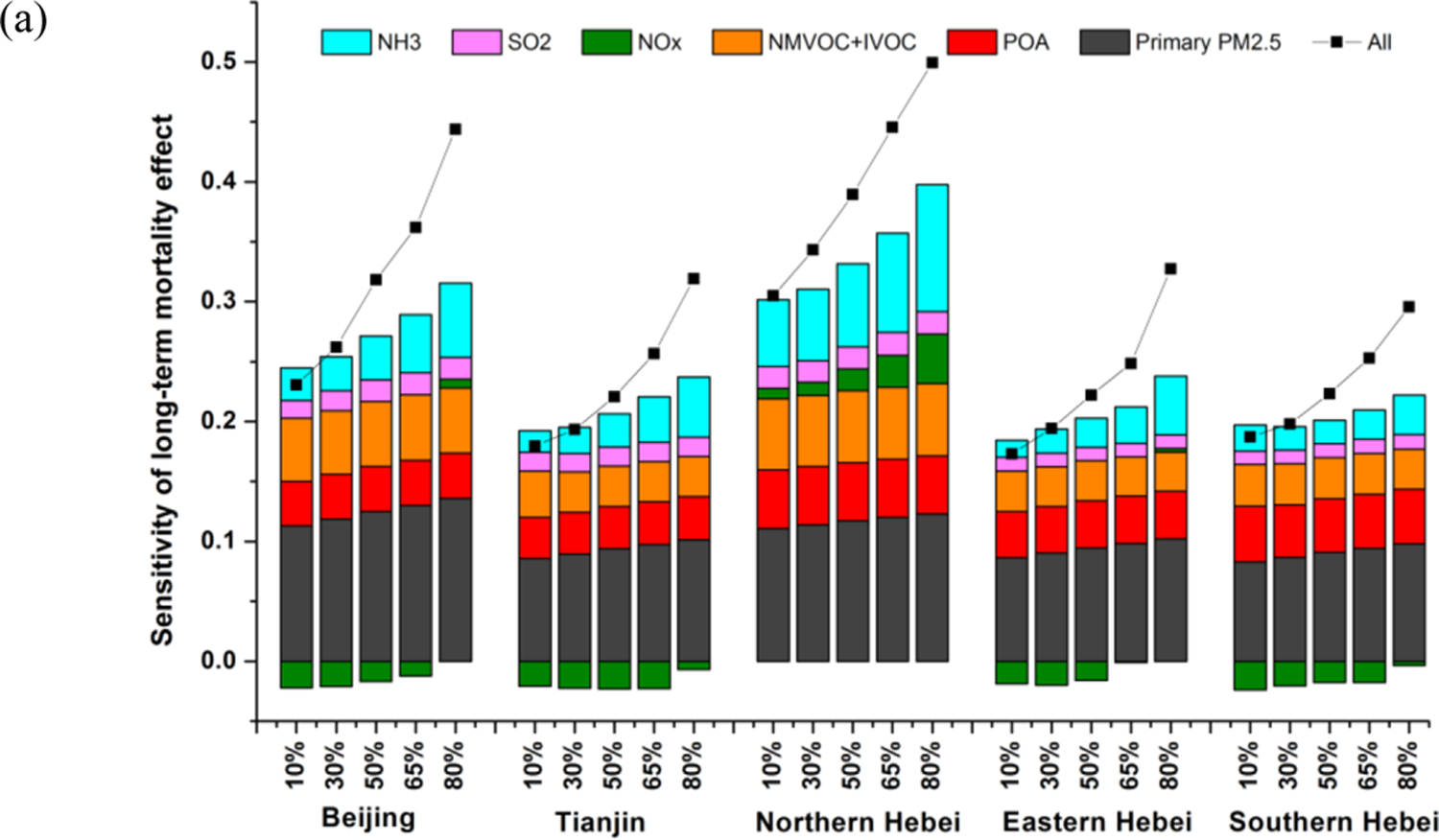
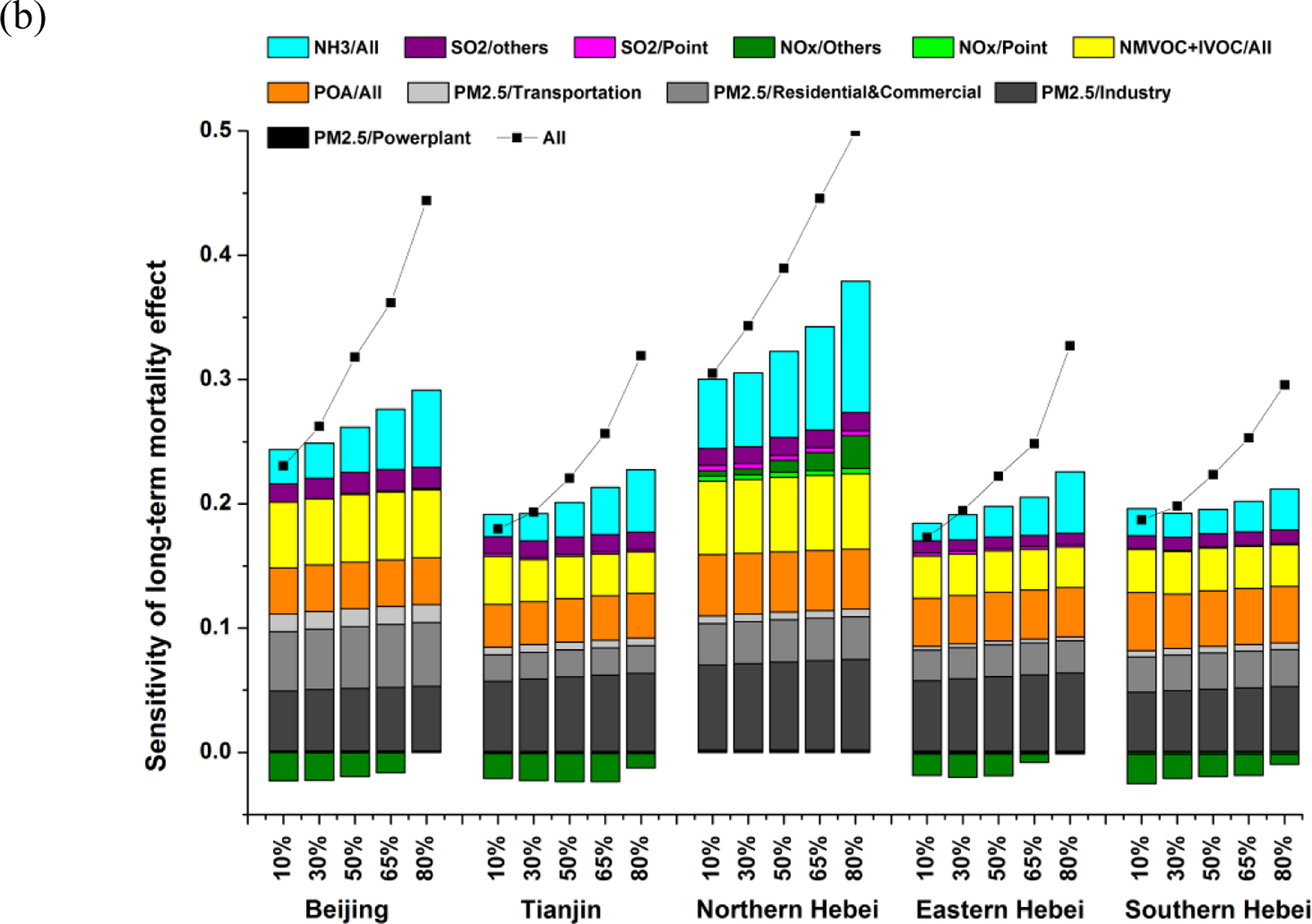
Sensitivity of annual mean mortality due to long-term exposure to PM2.5 to stepped control of individual air pollutants (a) and individual pollutant-sector combinations (b). The X-axis shows the reduction ratio (= 1 – emission ratio). The Y-axis shows the sensitivity of mortality, as defined by Eq. 3. The colored bars denote the sensitivity of mortality when a particular emission source is controlled while the others stay the same as the base case; the black dotted line denotes the sensitivity of mortality when all emission sources are controlled simultaneously.
Among the precursors, the long-term mortality is primarily sensitive to the emissions of NH3, nonmethane volatile organic compounds and intermediate volatility organic compounds (NMVOC+IVOC), and POA, and their relative importance differs according to reduction ratio and region (Fig. 3). The sensitivities of mortality to emissions of POA, NMVOC+IVOC and SO2 roughly remain constant at various reduction ratios. In contrast, the sensitivities to NH3 emissions increase substantially with the increase of reduction ratio due to a transition from NH3-rich to NH3-poor conditions. The sensitivities of mortality to NOx emissions can be either negative or positive, depending on region and reduction ratio — they tend to be more negative at small reduction ratio and more positive at large reductions, since a small reduction in NOx emissions is likely to produce more oxidants due to a NMVOC-limited photochemical regime, thus leading to formation of more secondary inorganic and organic aerosols. However, the results would be quite different if the NOx emissions outside the BTH region are jointly controlled. As shown in Fig. S3, when NOx emissions in the whole China are uniformly reduced, the sensitivities of mortality in BTH are positive even at a small reduction ratio. The reason is that NOx emission reductions in upwind regions are more likely to result in a net PM2.5 decrease compared with local emission reductions, since the photochemistry typically changes from a NMVOC-limited regime in local urban areas at surface to a NOx-limited regime in downwind areas or at upper levels (Xing et al., 2011). Therefore, it is critically important to enforce stringent NOx emission controls over a large spatial area beyond the BTH region.
Regarding emission sectors, the contributions of SO2 and NOx emissions are dominated by non-point sources (Fig. 3b). When all pollutants are controlled together, the sensitivity of mortality dramatically increases with reduction ratio, and this sensitivity is remarkably larger than the sum of the sensitivities to emissions of individual pollutants, indicating extra health benefits will be achieved if a multi-pollutant control strategy is implemented.
As for short-term exposure, we assess the sensitivities of all-cause mortality to emissions of various pollutants from various sectors (Fig. 4). The characteristics of the results are largely similar to those of long-term exposure. What is found to be different is that, when the emission reduction ratio increases from 10% to 80%, the sensitivity of mortality to primary inorganic PM2.5 emissions increases so slightly that it seems to be constant. This can be explained by the fact that the nonlinearity of the concentration-response function for short-term assessment (Eq. 2) is much weaker than that of the IER function (Eq. 1). When all pollutants are controlled together, the sensitivity of mortality is similar to or less than the sum of the sensitivities to emissions of individual pollutants, and the sensitivity only increases slightly with reduction ratio.
Fig. 4.
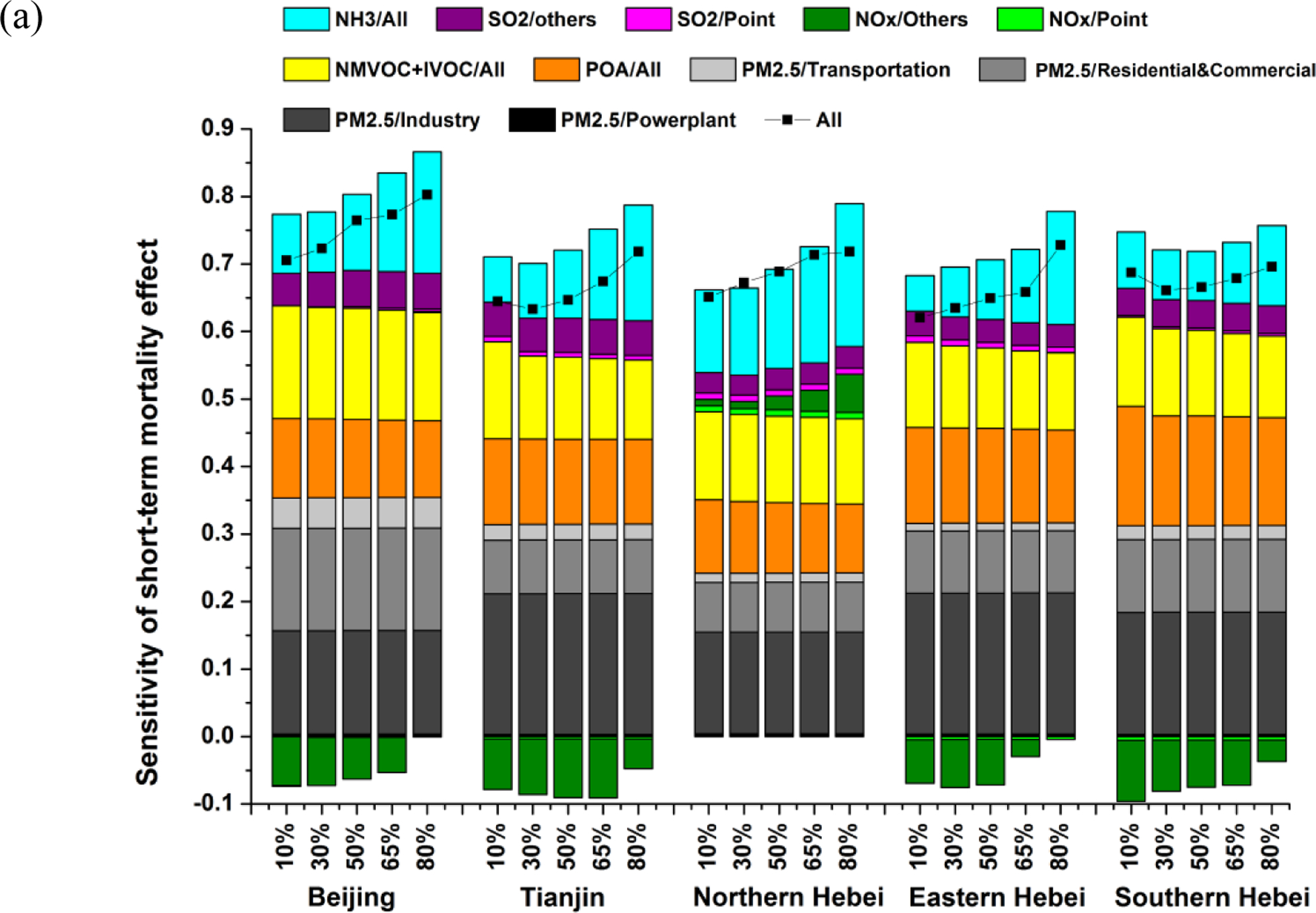
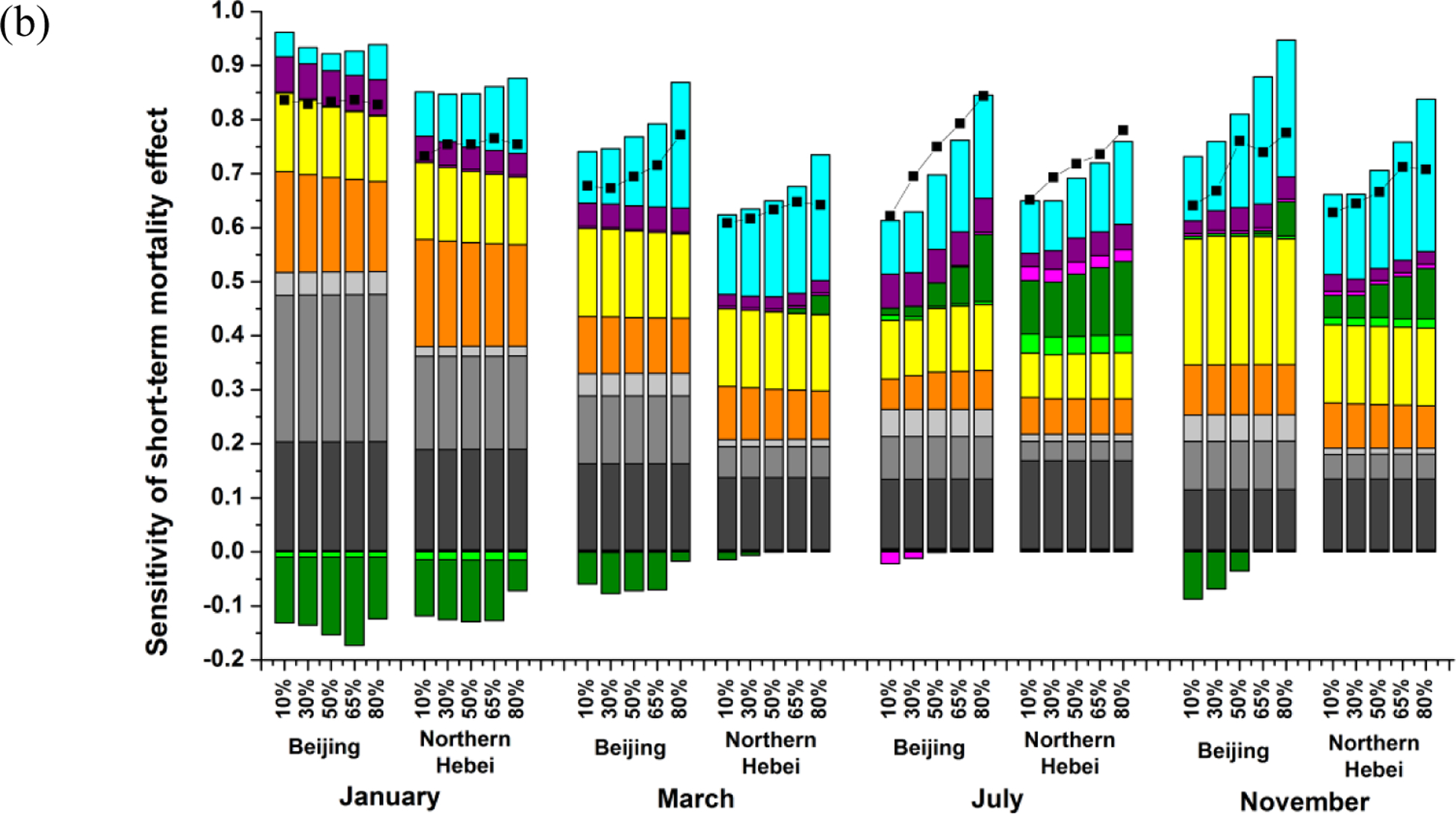
Sensitivity of annual mean (a) and monthly mean (b) short-term PM2.5-related mortality to stepped control of individual pollutant-sector combinations. The meanings of X-axis, Y-axis, colored bars, and black dotted lines are the same as Fig. 3.
We further analyze the seasonal feature of sensitivity of short-term mortality to emissions of various pollutants and sectors. We choose Beijing and Northern Hebei as examples, as shown in Fig. 4b. The sensitivities show significant discrepancy in different months. In winter, primary inorganic PM2.5 contributes a much larger fraction of mortality than other seasons, as a result of weaker vertical mixing and slower reactions of gaseous precursors. Among different sources of primary inorganic PM2.5, the residential and commercial sectors make relatively larger contributions in winter due to household heating. The sensitivities of mortality to gaseous precursors are generally larger in summer than in winter because of accelerated chemical reactions due to stronger radiation and higher temperature. The sensitivities to NOx are more complicated — they are mostly negative in winter and positive in summer, and change from negative to positive with the increase of reduction ratio in spring and autumn, because the photochemistry is prone to be NMVOC-limited in winter and NOx-limited in summer (Zhao et al., 2013; Zhao et al., 2015; Xing et al., 2017).
3.3. Nonlinear relations between region-specific emission control and health effects
We examine the nonlinear relationships between region-specific emission control and health effects by using the same method applied in Section 3.2. Here we select long-term mortality in Beijing as an example, as shown in Fig. 5. For any pollutant, the mortality in Beijing is most sensitive to local emissions among the five regions, but the relative contributions of local and non-local sources differ significantly according to pollutants. For primary inorganic PM2.5, POA, and SO2, local emissions account for more than 60% of the total contributions from all regions. With respect to NH3 and NMVOC+IVOC, local emissions account for about 50% and one third, respectively. The sensitivity of mortality to local primary inorganic PM2.5 emissions increases by ~20% when the reduction ratio increases from 10% to 80%, while the sensitivity to local NH3 emissions nearly doubles in response to such increase in the reduction ratio. For SO2, POA, and NMVOC+IVOC, no obvious change in sensitivities with the reduction ratio is noted. For NOx, the sensitivity to local emissions is negative, whereas the sensitivities to emissions from other regions, especially Southern Hebei from which a large amount of air pollutants are transported to Beijing (Chang et al., 2018), could change from negative to positive when the reduction ratio increases from 10% to 80%.
Fig. 5.
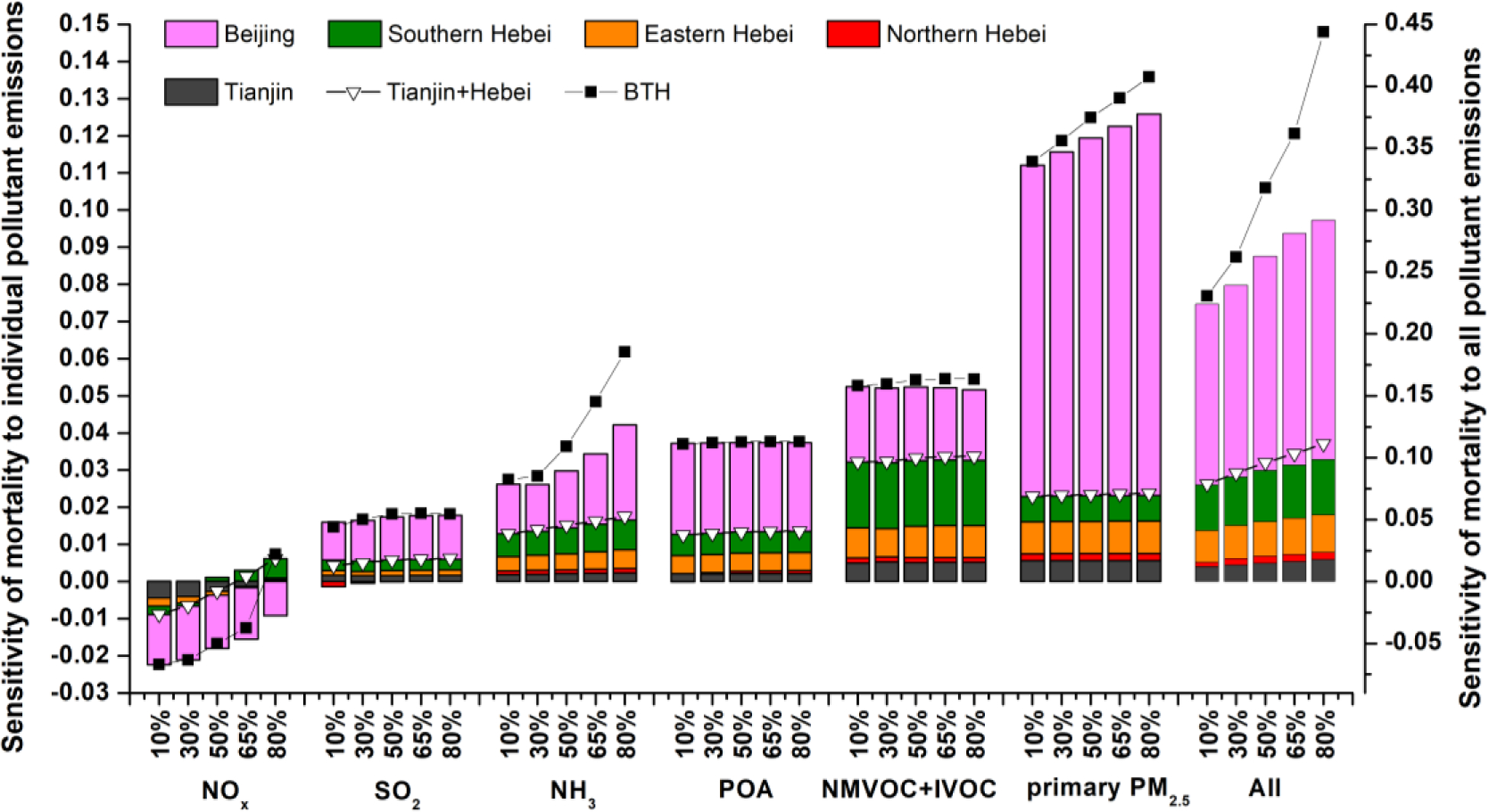
Sensitivity of annual mean mortality caused by long-term exposure to PM2.5 in Beijing to stepped control of individual/all air pollutants from various regions. The meanings of X-axis, Y-axis, colored bars, and black dotted lines are the same as Fig. 3. Hollow triangle dotted lines denote the sensitivity of mortality when all emission sources from regions except Beijing are controlled simultaneously.
For any individual pollutant, when emissions from all regions except Beijing are controlled together, the overall sensitivity of mortality nearly equals the arithmetic sum of the sensitivities to each single region, indicating quasi-linear effects of emission control among region outside Beijing. Nevertheless, when emissions from all regions including Beijing are controlled together, the overall sensitivity of mortality exceeds the arithmetic sum of the sensitivities to emissions from each single region, and the differences are more pronounced when the reduction ratio is large and/or multiple pollutants are controlled simultaneously (see the rightmost columns in Fig. 5). This implies that additional health benefits will be achieved when multi-pollutant and regional collaboration control strategies are implemented. Although we used Beijing as an example in the preceding analysis, similar increment in sensitivity due to multi-region and multi-pollutant controls is also found for other regions in BTH.
4. Conclusion and implications
In this study, we systemically assessed the nonlinear relationships between PM2.5-related mortality and air pollutant emissions in the BTH region by integrating the CMAQ/2D-VBS chemical transport model, the ERSM technique, and state-of-the-art concentration-response functions.
About 17.42 thousand, 36.29 thousand, 13.53 thousand and 61.91 thousand people die of COPD, IHD, lung cancer, and stroke respectively due to long-term exposure to PM2.5 in the BTH region annually. The annual mortality due to short-term exposure to PM2.5 is about 18.72 thousand. The PM2.5-related health effects are most severe in Beijing, Tianjin, and cities of Southern Hebei.
Among all pollutants, premature mortality due to both long-term and short-term exposures to PM2.5 is most sensitive to emissions of primary inorganic PM2.5. The sensitivity of long-term mortality to primary inorganic PM2.5 increases significantly with reduction ratio, as a result of the curvilinear IER function. For precursors, the PM2.5-related mortality is primarily sensitive to emissions of NH3, NMVOC+IVOC, and POA, and their relative importance differs according to reduction ratio and region. The sensitivities of mortality to NH3 and NOx increase significantly with the increase of reduction ratio, while the sensitivities to POA, NMVOC+IVOC and SO2 roughly remain constant at various reduction ratios. For long-term exposure, when all pollutants are controlled together, the sensitivity of mortality significantly increases with reduction ratio, and it’s much larger than the sum of the sensitivities to emissions of individual pollutants. For short-term exposure, however, the sensitivity of mortality to joint control of all pollutants is similar to the sum of sensitivities to individual pollutants.
The sensitivities of mortality to emission controls differ with seasons. In winter, emissions of primary inorganic PM2.5, especially those from residential and commercial sources, contribute more to mortality than in other seasons. In contrast, the sensitivities of mortality to gaseous precursors are generally larger in summer than in winter.
Over 60% of the contributions from emissions of primary inorganic PM2.5, POA, and SO2 to long-term mortality in Beijing are attributed to local emissions. For NH3 and NMVOC+IVOC, local emissions account for a smaller fraction, i.e., 50% and one third, respectively. When emissions from local and nonlocal emissions are controlled simultaneously, the overall sensitivity of mortality exceeds the arithmetic sum of the sensitivities to emissions from each single region, and the differences are more pronounced for larger reduction ratio and/or for joint control of multiple pollutants.
The findings from this study are important for the development and optimization of health-oriented air pollution control policies in BTH and its surrounding areas. First, a sharp reduction in emissions of primary PM2.5 is suggested considering that PM2.5-related mortality is most sensitive to it among all pollutants and that the sensitivity increases with reduction ratio. A particular focus shall be placed on primary PM2.5 emissions from residential and commercial sectors in winter, which have been largely neglected in China’s control policies until recently. Second, stringent control policies should be implemented for NOx and NH3 emissions in the BTH region in view of their increasing sensitivities with reduction ratio. For NOx, joint controls over a larger region beyond BTH are necessary in order to avoid possible side effects. Finally, multi-pollutant, multi-sector and regional collaboration control strategies are recommended wherever possible, because the sensitivity of long-term mortality to the joint emission controls are substantially larger than the sum of sensitivities to controls of individual pollutants or regions.
Supplementary Material
References
- Andersson C, Bergstrom R, and Johansson C: Population exposure and mortality due to regional background PM in Europe - Long-term simulations of source region and shipping contributions, Atmos. Environ, 43, 3614–3620, 10.1016/j.atmosenv.2009.03.040, 2009. [DOI] [Google Scholar]
- Burnett R, Chen H, and Szyszkowicz M: Global estimates of mortality associated with long-term exposure to outdoor fine particulate matter, P. Natl. Acad. Sci. USA, DOI 10.1073/pnas.1803222115, 2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Burnett RT, Pope CA, Ezzati M, Olives C, Lim SS, Mehta S, Shin HH, Singh G, Hubbell B, Brauer M, Anderson HR, Smith KR, Balmes JR, Bruce NG, Kan HD, Laden F, Pruss-Ustun A, Michelle CT, Gapstur SM, Diver WR, and Cohen A: An Integrated Risk Function for Estimating the Global Burden of Disease Attributable to Ambient Fine Particulate Matter Exposure, Environ. Health. Persp, 122, 397–403, Doi 10.1289/Ehp.1307049, 2014. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cai SY, Wang YJ, Zhao B, Wang SX, Chang X, and Hao JM: The impact of the “Air Pollution Prevention and Control Action Plan” on PM2.5 concentrations in Jing-Jin-Ji region during 2012–2020, Sci. Total. Environ, 580, 197–209, 10.1016/j.scitotenv.2016.11.188, 2017. [DOI] [PubMed] [Google Scholar]
- Chang X, Wang SX, Zhao B, Cai SY, and Hao JM: Assessment of inter-city transport of particulate matter in the Beijing-Tianjin-Hebei region, Atmos. Chem. Phys, 18, 4843–4858, 10.5194/acp-18-4843-2018, 2018. [DOI] [Google Scholar]
- Chen RJ, Li Y, Ma YJ, Pan GW, Zeng G, Xu XH, Chen BH, and Kan HD: Coarse particles and mortality in three Chinese cities: The China Air Pollution and Health Effects Study (CAPES), Sci. Total. Environ, 409, 4934–4938, 10.1016/j.scitotenv.2011.08.058, 2011. [DOI] [PubMed] [Google Scholar]
- Cohen AJ, Brauer M, Burnett R, Anderson HR, Frostad J, Estep K, Balakrishnan K, Brunekreef B, Dandona L, Dandona R, Feigin V, Freedman G, Hubbell B, Jobling A, Kan H, Knibbs L, Liu Y, Martin R, Morawska L, Pope CA, Shin H, Straif K, Shaddick G, Thomas M, van Dingenen R, van Donkelaar A, Vos T, Murray CJL, and Forouzanfar MH: Estimates and 25-year trends of the global burden of disease attributable to ambient air pollution: an analysis of data from the Global Burden of Diseases Study 2015, Lancet, 389, 1907–1918, 10.1016/s0140-6736(17)30505-6, 2017. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dominici F, McDermott A, Zeger SL, and Samet JM: On the use of generalized additive models in time-series studies of air pollution and health, American Journal Of Epidemiology, 156, 193–203, 10.1093/aje/kwf062, 2002. [DOI] [PubMed] [Google Scholar]
- Fann N, Baker KR, and Fulcher CM: Characterizing the PM2.5-related health benefits of emission reductions for 17 industrial, area and mobile emission sectors across the U.S, Environ. Int, 49, 141–151, 10.1016/j.envint.2012.08.017, 2012. [DOI] [PubMed] [Google Scholar]
- Global Burden of Disease Collaborative Network: Global Burden of Disease Study 2016 (GBD 2016) results tool, available from http://ghdx.healthdata.org/gbd-results-tool, Institute for Health Metrics and Evaluation (IHME), Seattle, United States, 2017. [Google Scholar]
- Heo J, Adams PJ, and Gao HO: Public Health Costs of Primary PM2.5 and Inorganic PM2.5 Precursor Emissions in the United States, Environ. Sci. Technol, 50, 6061–6070, 10.1021/acs.est.5b06125, 2016. [DOI] [PubMed] [Google Scholar]
- Huang DS, and Zhang SQ: Health benefit evaluation for PM2.5 pollution control in Beijing-Tianjin-Hebei region of China, China Environmental Science, 33, 166–174, 2013. [Google Scholar]
- Kan HD, and Chen BH: Particulate air pollution in urban areas of Shanghai, China: health-based economic assessment, Sci. Total. Environ, 322, 71–79, 10.1016/j.scitoenv.2003.09.010, 2004. [DOI] [PubMed] [Google Scholar]
- Kan HD, London SJ, Chen GH, Zhang YH, Song GX, Zhao NQ, Jiang LL, and Chen BH: Season, sex, age, and education as modifiers of the effects of outdoor air pollution on daily mortality in Shanghai, China: The Public Health and Air Pollution in Asia (PAPA) study, Environ. Health. Persp, 116, 1183–1188, 10.1289/ehp.10851, 2008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lelieveld J, Evans JS, Fnais M, Giannadaki D, and Pozzer A: The contribution of outdoor air pollution sources to premature mortality on a global scale, Nature, 525, 367-+, 10.1038/nature15371, 2015. [DOI] [PubMed] [Google Scholar]
- Lv LY, and Li HY: Health economic evaluation of PM10 and PM2.5 pollution in Beijing-Tianjin-Hebei region of China, Acta Scientiarum Naturallum Universitatis Nankaiensis, 49, 69–77, 2016. [Google Scholar]
- Martenies SE, Wilkins D, and Batterman SA: Health impact metrics for air pollution management strategies, Environ. Int, 85, 84–95, 10.1016/j.envint.2015.08.013, 2015. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Health and Family Planning Commission of China: China Health and Family Planning Statistics Yearbook 2015, Peking Union Medical College Press, Beijing, China, 2015. [Google Scholar]
- Oak ridge national laboratory: LandScan dataset 2016, available at https://web.ornl.gov/sci/landscan/, 2016.
- Shang Y, Sun ZW, Cao JJ, Wang XM, Zhong LJ, Bi XH, Li H, Liu WX, Zhu T, and Huang W: Systematic review of Chinese studies of short-term exposure to air pollution and daily mortality, Environ. Int, 54, 100–111, 10.1016/j.envint.2013.01.010, 2013. [DOI] [PubMed] [Google Scholar]
- Tuomisto JT, Wilson A, Evans JS, and Tainio M: Uncertainty in mortality response to airborne fine particulate matter: Combining European air pollution experts, Reliability Engineering & System Safety, 93, 732–744, 10.1016/j.ress.2007.03.002, 2008. [DOI] [Google Scholar]
- Wang J, Wang S, Voorhees AS, Zhao B, Jang C, Jiang J, Fu JS, Ding D, Zhu Y, and Hao J: Assessment of short-term PM2.5-related mortality due to different emission sources in the Yangtze River Delta, China, Atmos. Environ, 123, 440–448, 10.1016/j.atmosenv.2015.05.060, 2015. [DOI] [Google Scholar]
- Wang JD, Zhao B, Wang SX, Yang FM, Xing J, Morawska L, Ding AJ, Kulmala M, Kerminen VM, Kujansuu J, Wang ZF, Ding DA, Zhang XY, Wang HB, Tian M, Petaja T, Jiang JK, and Hao JM: Particulate matter pollution over China and the effects of control policies, Sci. Total. Environ, 584, 426–447, 10.1016/j.scitotenv.2017.01.027, 2017. [DOI] [PubMed] [Google Scholar]
- Wu WJ: Health Effect Attributed to Ambient Fine Particle Pollution in the Beijing-Tianjin-Hebei Region and its Source Apportionment, M.S. thesis, School of Environment, Tsinghua University, Beijing, China, 98 pp., 2016. [Google Scholar]
- Xing J, Wang SX, Jang C, Zhu Y, and Hao JM: Nonlinear response of ozone to precursor emission changes in China: a modeling study using response surface methodology, Atmos. Chem. Phys, 11, 5027–5044, DOI 10.5194/acp-11-5027-2011, 2011. [DOI] [Google Scholar]
- Xing J, Wang SX, Zhao B, Wu WJ, Ding DA, Jang C, Zhu Y, Chang X, Wang JD, Zhang FF, and Hao JM: Quantifying Nonlinear Multiregional Contributions to Ozone and Fine Particles Using an Updated Response Surface Modeling Technique, Environ. Sci. Technol, 51, 11788–11798, 10.1021/acs.est.7b01975, 2017. [DOI] [PubMed] [Google Scholar]
- Zhao B, Wang SX, Wang JD, Fu JS, Liu TH, Xu JY, Fu X, and Hao JM: Impact of national NOx and SO2 control policies on particulate matter pollution in China, Atmos. Environ, 77, 453–463, DOI 10.1016/j.atmosenv.2013.05.012, 2013. [DOI] [Google Scholar]
- Zhao B, Wang SX, Xing J, Fu K, Fu JS, Jang C, Zhu Y, Dong XY, Gao Y, Wu WJ, Wang JD, and Hao JM: Assessing the nonlinear response of fine particles to precursor emissions: development and application of an extended response surface modeling technique v1.0, Geosci. Model. Dev, 8, 115–128, DOI 10.5194/gmd-8-115-2015, 2015. [DOI] [Google Scholar]
- Zhao B, Wang SX, Donahue NM, Jathar SH, Huang XF, Wu WJ, Hao JM, and Robinson AL: Quantifying the effect of organic aerosol aging and intermediate-volatility emissions on regional-scale aerosol pollution in China, Sci. Rep-Uk, 6, 28815, 10.1038/srep28815, 2016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zhao B, Wu WJ, Wang SX, Xing J, Chang X, Liou KN, Jiang JH, Gu Y, Jang C, Fu JS, Zhu Y, Wang JD, Lin Y, and Hao JM: A modeling study of the nonlinear response of fine particles to air pollutant emissions in the Beijing-Tianjin-Hebei region, Atmos. Chem. Phys, 17, 12031–12050, DOI 10.5194/acp-17-12031-2017, 2017. [DOI] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.