

This phase 3 randomized clinical trial assesses the efficacy of a clinician-driven treatment choice vs a circulating tumor cell count–driven choice for first-line treatment among women with hormone receptor–positive, ERBB2-negative metastatic breast cancer.
Key Points
Question
Can the circulating tumor cell (CTC) count be used as an alternative to the clinical evaluation as the basis for determining the first-line treatment choice (chemotherapy or endocrine therapy) in hormone receptor–positive, ERBB2 (also known as HER2)-negative metastatic breast cancer?
Findings
In this randomized clinical trial that allocated 778 patients to a clinician-driven choice arm or a CTC-driven choice arm, the CTC arm was noninferior for progression-free survival.
Meaning
The CTC count may be a reliable biomarker for choosing between chemotherapy and single-agent endocrine therapy as the first-line treatment in hormone receptor–positive ERBB2-negative metastatic breast cancer.
Abstract
Importance
The choice between chemotherapy and endocrine therapy as first-line treatment for hormone receptor–positive, ERBB2 (also known as HER2)-negative metastatic breast cancer is usually based on the presence of clinical features associated with a poor prognosis. In this setting, a high circulating tumor cell (CTC) count (≥5 CTCs/7.5 mL) is a strong adverse prognostic factor for overall survival and progression-free survival (PFS).
Objective
To compare the efficacy of a clinician-driven treatment choice vs a CTC-driven choice for first-line treatment.
Interventions
In the CTC arm, patients received chemotherapy or endocrine therapy according to the CTC count (chemotherapy if ≥5 CTCs/7.5 mL; endocrine therapy if <5 CTCs/7.5 mL), whereas in the control arm, the choice was left to the investigator.
Design, Setting, and Participants
In the STIC CTC randomized, open-label, noninferiority phase 3 trial, participants were randomized to a clinician-driven choice of first-line treatment or a CTC count–driven first-line treatment choice. Eligible participants were premenopausal and postmenopausal women 18 years or older diagnosed with hormone receptor–positive, ERBB2-negative metastatic breast cancer. Data were collected at 17 French cancer centers from February 1, 2012, to July 28, 2016, and analyzed June 2019 to October 2019.
Main Outcome and Measures
The primary end point was the investigator-assessed PFS in the per-protocol population, with a noninferiority margin of 1.25 for the 90% CI of the hazard ratio.
Results
Among the 755 women in the per-protocol population, the median (range) age was 63 (30-88) years [64 (30-88) years for the 377 patients allocated to the CTC arm and 63 (31-87) years for the 378 patients allocated to the standard arm]; 138 (37%) and 103 (27%) received chemotherapy, respectively. Median PFS was 15.5 months (95% CI, 12.7-17.3) in the CTC arm and 13.9 months (95% CI, 12.2-16.3) in the standard arm. The primary end point was met, with a hazard ratio of 0.94 (90% CI, 0.81-1.09).
Conclusions and Relevance
This randomized clinical trial found that the CTC count may be a reliable biomarker method for guiding the choice between chemotherapy and endocrine therapy as the first-line treatment in hormone receptor–positive, ERBB2-negative metastatic breast cancer.
Trial Registration
ClinicalTrials.gov Identifier: NCT01710605
Introduction
About two-thirds of newly diagnosed metastatic breast cancers (MBCs) display a hormone receptor–positive, ERBB2 (also known as HER2)-negative phenotype.1 In addition to being the principal component of breast cancer biology and genomic landscapes,2,3 hormone receptor status was first characterized as a strong predictive factor of response to endocrine therapy.4 In the context of hormone receptor–positive MBC, a key question therefore became whether endocrine therapy or chemotherapy, when administered as first-line therapy, would be the most beneficial treatment in terms of survival and quality of life. In 2003, a meta-analysis5 of published data aggregated 692 patients from 6 trials conducted between 1963 and 1995; compared with up-front endocrine therapy, first-line chemotherapy yielded higher toxicity and response rates but no longer overall survival (OS). Because of the palliative context of MBC, endocrine therapy has been then established as the preferred first-line treatment of hormone receptor–positive, ERBB2-negative MBC by all expert consensus.6,7,8 Experts, however, acknowledge exceptions to the systematic use of endocrine therapy as up-front therapy: patients with a rapidly evolving disease, clinically meaningful symptoms, impaired general condition, and/or life-threatening disease, commonly referred to as visceral crisis.9 Until recently, real-life studies repeatedly reported that chemotherapy is administered as first-line therapy in 15% to 50% of patients with hormone receptor–positive, ERBB2-negative MBC.10,11,12,13,14,15
The clinical validity of the circulating tumor cell (CTC) count (assessed by the CellSearch system [Menarini Silicon Biosystems]) as a prognostic marker was first reported 15 years ago in a study on 177 patients with MBC.16 This seminal demonstration showed that a CTC count of 5 cells per 7.5 mL or greater was associated with a shorter OS and progression-free survival (PFS) and prompted its clearance for clinical use by the US Food and Drug Administration (FDA).17 The CTC count later reached a level of evidence 1 as a prognostic marker following the results of a pooled analysis of 1944 patients with MBC.18 Multivariate analyses confirmed that the 3 prominent prognostic markers in patients with MBC are tumor subtype, performance status, and baseline CTC count. This result suggested that, in a population of patients with hormone receptor–positive, ERBB2-negative MBC with homogeneous performance status, baseline CTC count may be a more reliable, standardized, and reproducible prognostic factor than the characteristics commonly used by clinicians to drive their treatment decision.
In addition, we hypothesized that a CTC-driven treatment choice would lead to a lower rate of up-front chemotherapy than a clinician-driven choice, as numerous studies have shown that chemotherapy is often used as first-line therapy.10,11 The STIC CTC study was therefore set up to evaluate the clinical utility of CTC count as a stand-alone biomarker to guide the choice between chemotherapy and endocrine therapy as first-line therapy for hormone receptor–positive, ERBB2-negative MBC.
Methods
Study Design and Participants
The STIC CTC trial was an open-label, randomized, multicenter, phase 3, noninferiority trial evaluating a CTC-driven treatment choice vs a clinician-driven choice in patients with hormone receptor–positive, ERBB2-negative MBC. Data were collected at 17 French cancer centers from February 1, 2012, to July 28, 2016, and analyzed June 2019 to October 2019. Women 18 years or older diagnosed with a hormone receptor–positive, ERBB2-negative MBC were recruited in 17 French centers before any endocrine therapy or chemotherapy for their metastatic disease (Figure 1). Both premenopausal and postmenopausal patients could be included, as well as patients who relapsed during adjuvant endocrine therapy. The clinical condition of patients had to be adequate for receiving endocrine therapy or chemotherapy, with a life expectancy of more than 3 months and an Eastern Cooperative Oncology Group performance status of 3 or less.
Figure 1. Trial Profile.

Clinhigh indicates patients requiring chemotherapy according to the clinician-driven choice; Clinlow, patients requiring endocrine therapy (ET) according to the clinician-driven choice; CT, chemotherapy; CTC, circulating tumor cell; CTChigh, patients with ≥5 CTCs/7.5 mL; CTClow, patients with <5 CTCs/7.5 mL.
Patients were enrolled by the investigators and randomly allocated (1:1) to the clinician-driven choice (standard arm) or to the CTC-driven treatment choice (CTC arm). The randomization was done with permuted blocks of 6 patients at the statistics department of the study sponsor and was stratified by trial center and by performance status (0-1 vs 2-3). This study was a parallel, open-label trial; the CTC count was assessed in all included patients but remained masked if patients were allocated to the standard arm to not influence the physician’s choice.
All patients provided written informed consent before enrollment. This clinical trial was approved by a national ethics committee (CPP Ile-de-France 3). The protocol can be found in Supplement 1. This study followed the Consolidated Standards of Reporting Trials (CONSORT) reporting guideline.
Procedures
Before randomization, investigators had to declare their best treatment recommendation. Patients for whom endocrine therapy or chemotherapy was clinically recommended will be hereby referred to as clinical low or clinical high risk, respectively. The CTC counts were assessed using the FDA-cleared CellSearch system, as previously described.19 Each patient eligible for randomization had 2 risk estimates successively captured by the study clinical report form: the one established by the investigator (clinical low or clinical high) and the one determined by the CTC status (CTC low if <5 CTCs/7.5 mL or CTC high if ≥5 CTCs/7.5 mL).
In the clinician-driven choice arm, patients were treated according to the clinical choice of treatment as defined by the investigator (endocrine therapy if clinical low; chemotherapy if clinical high). In the CTC arm, the predefined clinical choice of treatment was dismissed, and patients were treated according to the CTC count: endocrine therapy if CTC low or chemotherapy if CTC high. In each arm, the choice of the agent(s) used for endocrine therapy or chemotherapy was left to the investigator, as several options are available for first-line endocrine therapy and chemotherapy.7 Premenopausal women received adequate ovarian function suppression when treated with endocrine therapy. The use of a targeted therapy in combination with endocrine therapy or chemotherapy was allowed, and maintenance endocrine therapy in patients who had no tumor progression while receiving chemotherapy was accepted.
Radiologic assessments were done locally by investigators using Response Evaluation Criteria in Solid Tumors, version 1.1. Adverse events were graded according to the Common Terminology Criteria for Adverse Events, version 4.0.
Outcomes
The primary end point was PFS, defined as the time from randomization to disease progression or death from any cause within 2 years after randomization. Participants without any events were censored for the primary analysis at 2 years after randomization. Patients were evaluated for any sign of tumor progression or adverse event every 2 months in addition to radiologic assessments. An increase in tumor serum markers alone could not define a progression.
Secondary end points were OS from the time of randomization, PFS in subgroup analyses (by treatment initially considered and CTC count), the rate of treatment changes (between the treatment initially considered by clinicians and that finally administered), the rate of patients receiving endocrine therapy in each arm, and the occurrence of adverse events. Quality of life and costs supported by the payer were also estimated as part of a joint medico-economic analysis that will be reported separately.
Statistical Analysis
The STIC CTC trial was designed to test the noninferiority of the CTC-based decision arm compared with the clinician-based decision arm, as we hypothesized that the number of patients treated with chemotherapy would be lower in the CTC arm, thus reducing the rate of chemotherapy-related adverse events. For the primary end point, the hazard ratio (HR) of progression in the CTC arm compared with the standard arm was estimated using a Cox proportional hazards model. The noninferiority hypothesis, sample size calculations, and hierarchical test procedures to assess superiority are detailed in the eMethods in Supplement 2. The analysis of the primary end point was to be performed when the number of events had reached 498, with a minimum median follow-up of 1 year. Results shown below therefore include an analysis of the primary end point based on the 498 first PFS events, while secondary end points are reported based on the total number of events observed.
The primary end point (2-year PFS) was evaluated in the per-protocol population, and a complementary PFS analysis was performed in the intention-to-treat population, as recommended for noninferiority trials.20 The OS was evaluated in the per-protocol population, but an intention-to-treat analysis was also conducted.
For the secondary end point, the PFS and OS curves were estimated using the Kaplan-Meier method and compared between the 2 arms using a log-rank test. Preplanned subgroup analyses were conducted with a log-rank test to compare PFS between subgroups defined by baseline clinical characteristics but also by the CTC count and the treatment choice of the clinician (chemotherapy or endocrine therapy) for PFS and OS. All analyses were done with the R software, version 3.4.4 (R Project for Statistical Computing).
Results
Patients
Between February 1, 2012, and July 28, 2016, 797 patients were included at 17 centers in France. Because 19 patients were not eligible for randomization and were excluded (Figure 1), 778 participants were randomized to the clinician-driven choice arm (n = 387) or to the CTC-driven choice arm (n = 391). Among the 755 women in the per-protocol population, the median (range) age was 64 (30-88) years for the 377 patients allocated to the CTC arm and 63 (31-87) years for the 378 allocated to the standard arm. The characteristics of the patients were balanced across the trial groups at baseline (eTable 1 in Supplement 2). Overall, 289 patients (38.3%) were CTC high.
In the standard arm, the 275 (72.7%) patients who were considered clinical low by the investigator received endocrine therapy, and the 103 (27.2%) who were considered clinical high received chemotherapy, whereas in the CTC arm, the 239 (63.4%) CTC low patients received endocrine therapy, and the 138 (36.6%) CTC high patients received chemotherapy. Overall, 463 (61.3%) patients had a concordant clinical and CTC risk assessment, either clinical low/CTC low (363 patients, 78.4%) or clinical high/CTC high (100 patients, 21.6%). On the other hand, 292 patients (38.7%) had a discordant CTC and clinical assessment: 189 (64.7%) patients were clinical low/CTC high, and 103 (35.3%) patients were clinical high/CTC low. Details of the treatment allocation can be found in Figure 1.
The treatments planned and actually delivered were recorded (eTable 2 and eTable 3 in Supplement 2). Planned treatments were similar between the 2 arms. Capecitabine was overall more often used in the CTC arm compared with the standard arm (23.9% vs 7.9%), as it was frequently prescribed to clinical low, CTC high patients allocated to the CTC arm and switched from endocrine therapy to chemotherapy.
Safety
The rate of grade 3 or 4 adverse events was low in both arms (eTable 4 in Supplement 2). Overall, there was a higher rate of chemotherapy-related adverse events of any grade in the CTC arm, with a higher incidence of anemia (20.4% vs 14.6% in the standard arm), alopecia (15.1% vs 10.6%), and vomiting (8.2% vs 4.8%).
Clinical Utility
The primary end point analysis was performed on the first 498 PFS events: 250 (50.2%) in the standard arm and 248 (49.8%) in the CTC arm. Median PFS was 13.9 months (95% CI, 12.2-16.3) in the standard arm and 15.5 months (95% CI, 12.7-17.3) in the CTC arm (Figure 2A). The primary end point was met with an HR for progression in the per-protocol population for the CTC arm of 0.94 (90% CI, 0.81-1.09). Because the upper limit of the CI was lower than the noninferiority margin of 1.25, the null hypothesis that the PFS in the CTC arm would be worse was rejected, and the noninferiority of the CTC arm compared with the standard arm was concluded. The preplanned test for superiority was not significant. Similar results were observed when considering all events (n = 542 events) in the per-protocol population but also in the intention-to-treat population (eFigure 1 in Supplement 2). There was no OS difference between the 2 arms (Figure 2B), with an HR of 0.91 (95% CI, 0.71-1.16).
Figure 2. Kaplan-Meier Curves of Progression-Free Survival (PFS) and Overall Survival (OS).
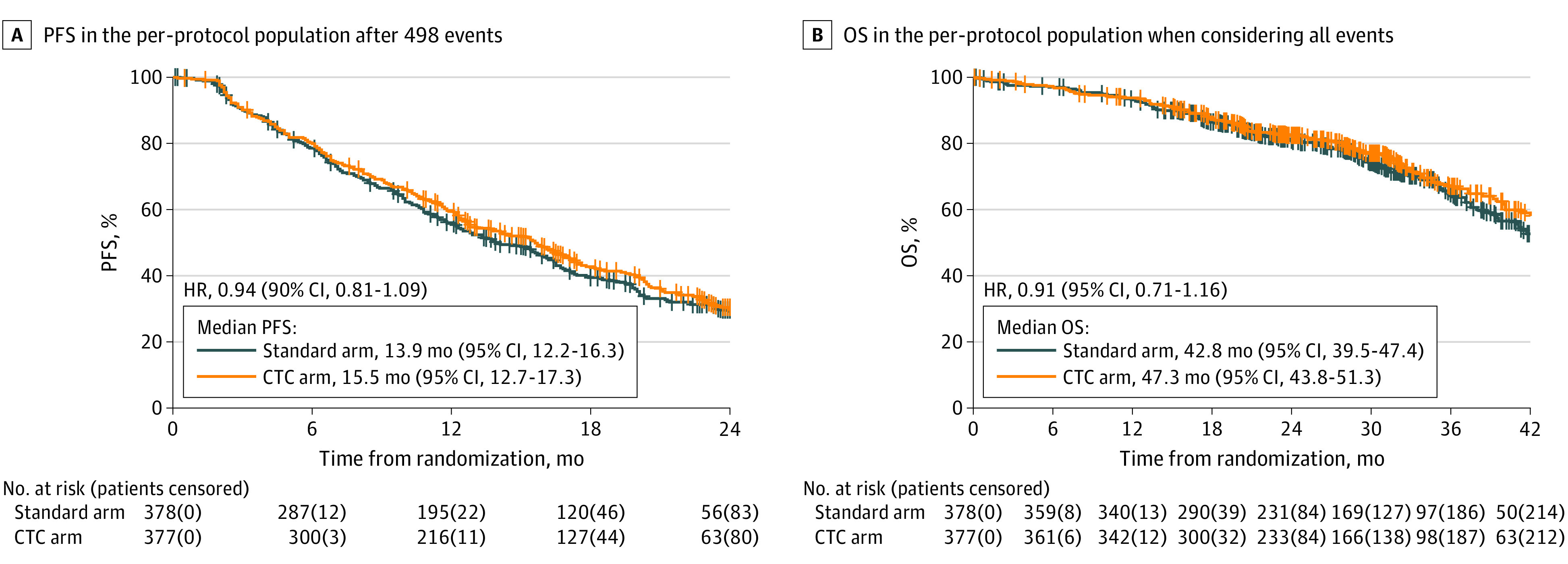
A, The PFS for each arm in the per-protocol population after 498 events had occurred; B, The OS for each arm in the per-protocol population when considering all events. CTC indicates circulating tumor cell; HR, hazard ratio.
In planned subgroup analyses according to baseline characteristics, age older than 60 years was the only factor associated with a PFS benefit of a CTC-driven treatment decision (eFigure 2 in Supplement 2), with an HR of 0.76 (95% CI, 0.61-0.94). Planned subgroup comparisons between the standard and CTC arms in the concordant clinical low, CTC low and clinical high, CTC high subgroups found no difference in PFS (HR, 1.03; 95% CI, 0.81-1.31; and HR, 0.90; 95% CI, 0.60-1.36, respectively; Figure 3A and B) and OS (HR, 1.08; 95% CI, 0.71-1.65; and HR, 0.90; 95% CI, 0.53 to 1.50, respectively; eFigure 3A and B in Supplement 2). In the discordant clinical high, CTC low subgroup, there was no difference in PFS (HR, 1.20; 95% CI, 0.79-1.84; Figure 3C) or OS (HR, 0.99; 95% CI, 0.48-2.02; eFigure 3C in Supplement 2) between the standard and CTC arms. However, in the discordant clinical low, CTC high subgroup, PFS was significantly higher in the CTC arm (HR, 0.62; 95% CI, 0.45-0.84; Figure 3D), whereas OS was not significantly different (HR, 0.69; 95% CI, 0.43-1.09; eFigure 3D in Supplement 2). In a nonplanned analysis, we compared the PFS of patients stratified by actual receipt of chemotherapy or endocrine therapy in both arms (eFigure 4 in Supplement 2).
Figure 3. Kaplan-Meier Curves of Progression-Free Survival (PFS) for Each Arm, When Considering All Events.
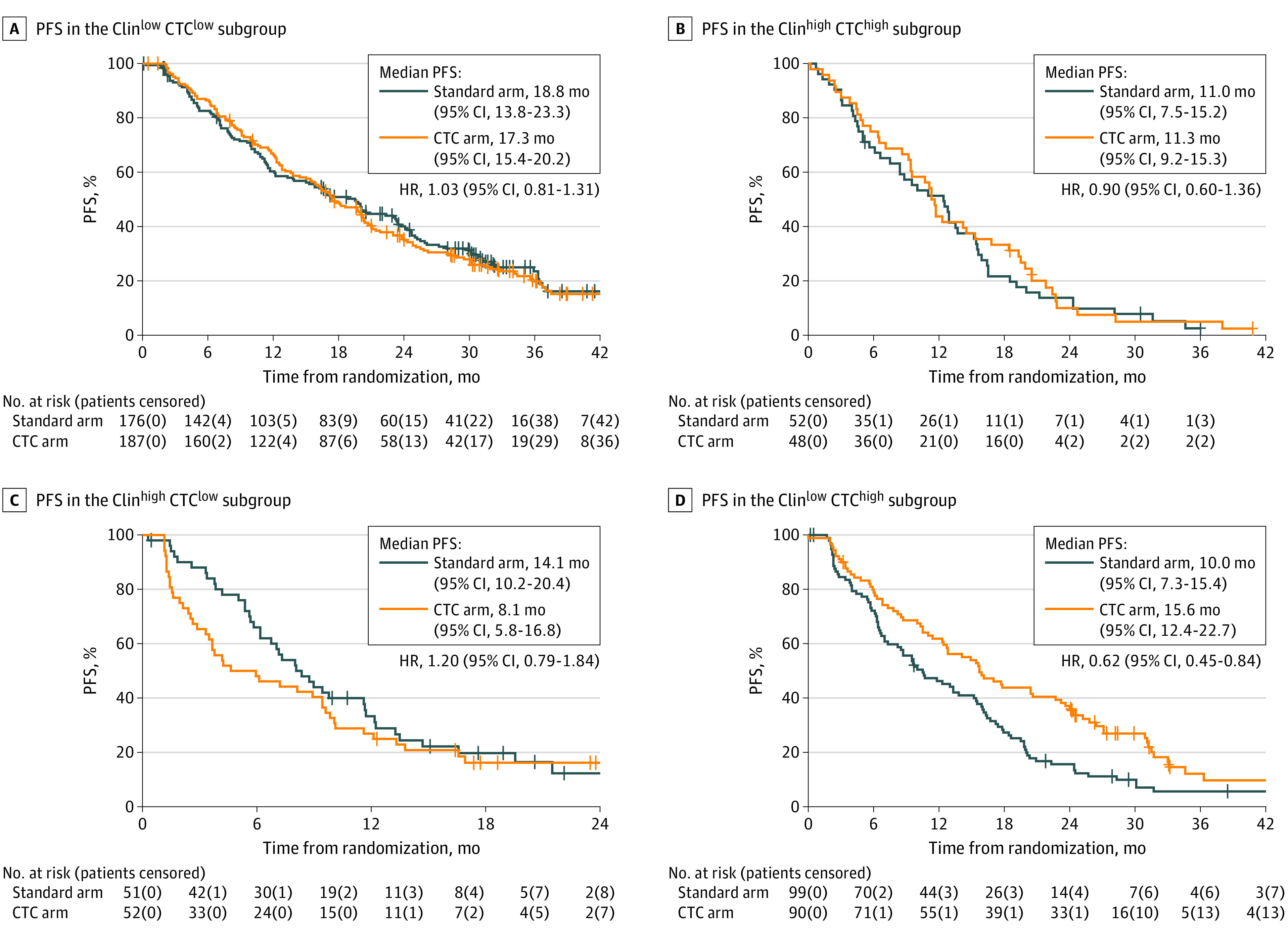
A, The PFS in the Clinlow CTClow subgroup; B; The PFS in the Clinhigh CTChigh subgroup; C, The PFS in the Clinhigh CTClow subgroup; D; The PFS in the Clinlow CTChigh subgroup. Clinhigh indicates patients requiring chemotherapy according to the clinician-driven choice; Clinlow, patients requiring endocrine therapy according to the clinician-driven choice; CTC, circulating tumor cell; CTChigh, patients with ≥5 CTCs/7.5 mL; CTClow, patients with <5 CTCs/7.5 mL; HR, hazard ratio.
In another nonplanned subgroup analysis, we pooled the discordant clinical high, CTC low and clinical low, CTC high subgroups and used a multivariate Cox model to compensate for the lack of randomization between chemotherapy and endocrine therapy in these pooled subgroups. The PFS and OS were significantly higher in patients treated with chemotherapy compared with patients treated with endocrine therapy, with an HR of 0.66 (95% CI, 0.51-0.87) and 0.62 (95% CI, 0.41-0.95), respectively (eFigure 5 in Supplement 2). We investigated the prognostic role of CTCs by comparing PFS and OS between the CTC high and CTC low groups in all 755 patients: PFS and OS were significantly lower in the CTC high group, with an HR estimated by the Cox model of 1.49 (95% CI, 1.27-1.76) and 1.94 (95% CI, 1.52-2.49), respectively. Assessing whether adapting the treatment strategy on the CTC count would decrease its prognostic impact, we found that the prognostic impact of a high CTC count (compared with a low CTC count) was lower in the CTC arm than in the standard arm for PFS (HR, 1.22; 95% CI, 0.97-1.54; and HR, 1.84; 95% CI, 1.47 to 2.31, respectively) and OS (HR, 1.64; 95% CI, 1.15-2.34; and HR, 2.24; 95% CI, 1.58-3.17, respectively).
Discussion
The STIC CTC trial is, to our knowledge, the first attempt to demonstrate the clinical utility of a biomarker to guide the choice of first-line treatment in hormone receptor–positive, ERBB2-negative MBC, a setting characterized by a lack of predictive biomarker and high interphysician variability. The aim of this trial was to demonstrate that using the CTC count, a single and reproducible biomarker, was an alternative to the highly multiparametric clinical choice. As a therapeutic de-escalation was planned in at least 1 patient subgroup (clinical high, CTC low), a noninferiority design was favored.
In the overall population, the STIC CTC trial reached its primary objective and reported no overt survival difference between the 2 arms. While the overall rate of chemotherapy use was not lower in the CTC arm, the reproducibility of the CTC could allow for treatment standardization in this population. The apparent superior benefit of the CTC-based strategy in older adult patients might stem from the observed significant association between older age and more systematic use of endocrine therapy as the clinically favored treatment, whatever the other clinicopathologic characteristics. Using the CTC count as a single biomarker is therefore a reliable, standardized option to guide the treatment choice between single-agent endocrine therapy and chemotherapy in hormone receptor–positive, ERBB2-negative MBC.
Survival data further substantiate the prognostic impact of CTC count. Interestingly, the prognostic impact of the CTC count was reduced in patients randomized in the CTC arm, suggesting that prognostic markers—and not only predictive markers—might be partly “actionable” in MBC. In contrast to our initial hypothesis, the CTC-driven treatment choice did not lead to a de-escalation from chemotherapy to endocrine therapy in the overall study population, with a higher rate of patients treated with up-front chemotherapy in the CTC arm (36.6%). However, the use of higher thresholds (eg, ≥10 CTC/7.5 mL) could have yielded a lower rate of chemotherapy in the CTC arm.
Unique findings were derived from the 38.7% of patients who had a discordant CTC and clinical assessment (ie, in the clinical low, CTC high and clinical high, CTC low subgroups). The use of chemotherapy yielded a significantly longer PFS and a non–statistically significant trend toward longer PFS in the former and latter subgroups, respectively. Interestingly, when pooling these 2 subgroups, chemotherapy was significantly associated with a benefit in both PFS and OS when compared with endocrine therapy in a multivariate analysis. This last analysis was unplanned and should be treated with caution, yet it suggests that up-front chemotherapy could be beneficial to patients with intermediate-risk estimate.
Limitations
The STIC CTC trial has several limitations. First, the study was conducted before the results of the first-line cyclin-dependent kinase 4/6 (CDK4/6) inhibitors’ pivotal trials.21,22,23,24 While the STIC CTC results suggest that single-agent endocrine therapy is suboptimal in patients with intermediate prognosis, first-line combinations of endocrine therapy with CDK4/6 inhibitors have improved the outcome of these patients and have become the preferred first-line treatment option in patients without visceral crisis.
Noteworthy, as CDK4/6 inhibitors have been reimbursed in France since 2015, most patients included in our trial should have received CDK4/6 inhibitors as part of a further line of treatment—a strategy that has not been proved inferior to the first-line use of these drugs. Although the STIC CTC has a limited utility for patients eligible for first-line CDK4/6 inhibitors, this study highlights that the clinical prognostic assessment can be usefully completed by the CTC count. To further explore this potential in the CDK4/6 inhibitors era, CTC count is now being evaluated as part of a phase 3 study (AMBRE trial, NCT04158362) comparing first-line chemotherapy with endocrine therapy and abemaciclib in patients with hormone receptor–positive, ERBB2-negative MBC with visceral metastases and high tumor burden.
Second, although the CellSearch system is the only FDA-cleared CTC detection technology for MBC, some mesenchymal-like CTCs may be missed. The molecular characterization of CTCs, which was not performed in our trial, can also reveal cancer cell characteristics that may predict the efficacy of endocrine therapy, CDK4/6 inhibitors, or chemotherapy.25
Conclusions
The results of this trial demonstrate the reliability and clinical utility of CTC count to guide the choice between single-agent endocrine therapy and chemotherapy as first-line treatment of hormone receptor–positive, ERBB2-negative MBC, at the cost of a higher proportion of patients treated with chemotherapy. On the other hand, our results suggest that clinical low, CTC low patients (48.1% of the study population) have an excellent prognosis, with an 18-month median PFS and a 50-month median OS. Future trials in this population could focus on delaying the introduction of CDK4/6 inhibitors to limit the associated adverse events or to evaluate more aggressive strategies for patients with oligometastatic disease.
Trial Protocol
eMethods.
eFigure 1. Kaplan-Meier curves of progression-free survival for each arm, when considering all events in the per-protocol population (A) and in the intention-to-treat population (B)
eFigure 2. Pre-specified subgroup analysis of progression-free survival in patients treated according to clinician-driven treatment choice compared with patients treated according to CTC-driven treatment choice
eFigure 3. Kaplan-Meier curves of overall survival for each arm, when considering all events, in the Clinlow/CTClow subgroup (A), in the Clinhigh/CTChigh subgroup (B), in the Clinhigh/CTClow subgroup (C) and in the Clinlow/CTChigh subgroup (D)
eFigure 4. Kaplan-Meier curves of progression-free survival of patients treated by chemotherapy or endocrine therapy in the standard arm (A) and in the CTC arm (B)
eFigure 5. Kaplan-Meier curves of progression-free (A) and overall survival (B) of patients treated by chemotherapy or endocrine therapy in the pooled Clinhigh/CTClow and Clinlow/CTChigh subgroup
eTable 1. Baseline clinical and pathological characteristics of patients in the per-protocol population
eTable 2. Planned treatments, declared by physicians at inclusion, before randomization and CTC count
eTable 3. Treatments actually received in the per-protocol population
eTable 4. Adverse events. Number of patients for each event and corresponding percentage
Data Sharing Statement
References
- 1.Gobbini E, Ezzalfani M, Dieras V, et al. Time trends of overall survival among metastatic breast cancer patients in the real-life ESME cohort. Eur J Cancer. 2018;96:17-24. doi: 10.1016/j.ejca.2018.03.015 [DOI] [PubMed] [Google Scholar]
- 2.Hammond MEH, Hayes DF, Dowsett M, et al. American Society of Clinical Oncology/College Of American Pathologists guideline recommendations for immunohistochemical testing of estrogen and progesterone receptors in breast cancer. J Clin Oncol. 2010;28(16):2784-2795. doi: 10.1200/JCO.2009.25.6529 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Ng CKY, Schultheis AM, Bidard F-C, Weigelt B, Reis-Filho JS. Breast cancer genomics from microarrays to massively parallel sequencing: paradigms and new insights. J Natl Cancer Inst. 2015;107(5):djv015. doi: 10.1093/jnci/djv015 [DOI] [PubMed] [Google Scholar]
- 4.Osborne CK. Tamoxifen in the treatment of breast cancer. N Engl J Med. 1998;339(22):1609-1618. doi: 10.1056/NEJM199811263392207 [DOI] [PubMed] [Google Scholar]
- 5.Wilcken N, Hornbuckle J, Ghersi D. Chemotherapy alone versus endocrine therapy alone for metastatic breast cancer. Cochrane Database Syst Rev. 2003;(2):CD002747. doi: 10.1002/14651858.CD002747 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Partridge AH, Rumble RB, Carey LA, et al. Chemotherapy and targeted therapy for women with human epidermal growth factor receptor 2-negative (or unknown) advanced breast cancer: American Society of Clinical Oncology clinical practice guideline. J Clin Oncol. 2014;32(29):3307-3329. doi: 10.1200/JCO.2014.56.7479 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Cardoso F, Senkus E, Costa A, et al. 4th ESO-ESMO international consensus guidelines for advanced breast cancer (ABC 4). Ann Oncol. 2018;29(8):1634-1657. doi: 10.1093/annonc/mdy192 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Mukai H, Aihara T, Yamamoto Y, et al. ; Japanese Breast Cancer Society . The Japanese Breast Cancer Society clinical practice guideline for systemic treatment of breast cancer. Breast Cancer. 2015;22(1):5-15. doi: 10.1007/s12282-014-0563-x [DOI] [PubMed] [Google Scholar]
- 9.Hart CD, Migliaccio I, Malorni L, Guarducci C, Biganzoli L, Di Leo A. Challenges in the management of advanced, ER-positive, HER2-negative breast cancer. Nat Rev Clin Oncol. 2015;12(9):541-552. doi: 10.1038/nrclinonc.2015.99 [DOI] [PubMed] [Google Scholar]
- 10.Jacquet E, Lardy-Cléaud A, Pistilli B, et al. Endocrine therapy or chemotherapy as first-line therapy in hormone receptor-positive HER2-negative metastatic breast cancer patients. Eur J Cancer. 2018;95(95):93-101. doi: 10.1016/j.ejca.2018.03.013 [DOI] [PubMed] [Google Scholar]
- 11.Caldeira R, Scazafave M. Real-world treatment patterns for hormone receptor-positive, human epidermal growth factor receptor 2-negative advanced breast cancer in Europe and the United States. Oncol Ther. 2016;4(2):189-197. doi: 10.1007/s40487-016-0033-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Lobbezoo DJA, van Kampen RJW, Voogd AC, et al. In real life, one-quarter of patients with hormone receptor-positive metastatic breast cancer receive chemotherapy as initial palliative therapy: a study of the Southeast Netherlands Breast Cancer Consortium. Ann Oncol. 2016;27(2):256-262. doi: 10.1093/annonc/mdv544 [DOI] [PubMed] [Google Scholar]
- 13.Bonotto M, Gerratana L, Di Maio M, et al. Chemotherapy versus endocrine therapy as first-line treatment in patients with luminal-like HER2-negative metastatic breast cancer: a propensity score analysis. Breast. 2017;31:114-120. doi: 10.1016/j.breast.2016.10.021 [DOI] [PubMed] [Google Scholar]
- 14.Watanabe J, Hayashi T, Tadokoro Y, Nishimura S, Takahashi K. Clinical pattern of primary systemic therapy and outcomes of estrogen receptor-positive, HER2-negative metastatic breast cancer: a review of a single institution. Breast Cancer Res Treat. 2017;166(3):911-917. doi: 10.1007/s10549-017-4478-z [DOI] [PubMed] [Google Scholar]
- 15.Zanotti G, Hunger M, Perkins JJ, Horblyuk R, Martin M. Treatment patterns and real world clinical outcomes in ER+/HER2- post-menopausal metastatic breast cancer patients in the United States. BMC Cancer. 2017;17(1):393. doi: 10.1186/s12885-017-3379-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Cristofanilli M, Budd GT, Ellis MJ, et al. Circulating tumor cells, disease progression, and survival in metastatic breast cancer. N Engl J Med. 2004;351(8):781-791. doi: 10.1056/NEJMoa040766 [DOI] [PubMed] [Google Scholar]
- 17.Bidard F-C, Proudhon C, Pierga J-Y. Circulating tumor cells in breast cancer. Mol Oncol. 2016;10(3):418-430. doi: 10.1016/j.molonc.2016.01.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Bidard F-C, Peeters DJ, Fehm T, et al. Clinical validity of circulating tumour cells in patients with metastatic breast cancer: a pooled analysis of individual patient data. Lancet Oncol. 2014;15(4):406-414. doi: 10.1016/S1470-2045(14)70069-5 [DOI] [PubMed] [Google Scholar]
- 19.Allard WJ, Matera J, Miller MC, et al. Tumor cells circulate in the peripheral blood of all major carcinomas but not in healthy subjects or patients with nonmalignant diseases. Clin Cancer Res. 2004;10(20):6897-6904. doi: 10.1158/1078-0432.CCR-04-0378 [DOI] [PubMed] [Google Scholar]
- 20.Piaggio G, Elbourne DR, Pocock SJ, Evans SJW, Altman DG; CONSORT Group . Reporting of noninferiority and equivalence randomized trials: extension of the CONSORT 2010 statement. JAMA. 2012;308(24):2594-2604. doi: 10.1001/jama.2012.87802 [DOI] [PubMed] [Google Scholar]
- 21.Im S-A, Lu Y-S, Bardia A, et al. Overall survival with ribociclib plus endocrine therapy in breast cancer. N Engl J Med. 2019;381(4):307-316. doi: 10.1056/NEJMoa1903765 [DOI] [PubMed] [Google Scholar]
- 22.Finn RS, Martin M, Rugo HS, et al. Palbociclib and letrozole in advanced breast cancer. N Engl J Med. 2016;375(20):1925-1936. doi: 10.1056/NEJMoa1607303 [DOI] [PubMed] [Google Scholar]
- 23.Hortobagyi GN, Stemmer SM, Burris HA, et al. Ribociclib as first-line therapy for HR-positive, advanced breast cancer. N Engl J Med. 2016;375(18):1738-1748. doi: 10.1056/NEJMoa1609709 [DOI] [PubMed] [Google Scholar]
- 24.Goetz MP, Toi M, Campone M, et al. MONARCH 3: abemaciclib as initial therapy for advanced breast cancer. J Clin Oncol. 2017;35(32):3638-3646. doi: 10.1200/JCO.2017.75.6155 [DOI] [PubMed] [Google Scholar]
- 25.Paoletti C, Muñiz MC, Thomas DG, et al. Development of circulating tumor cell-endocrine therapy index in patients with hormone receptor-positive breast cancer. Clin Cancer Res. 2015;21(11):2487-2498. doi: 10.1158/1078-0432.CCR-14-1913 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Trial Protocol
eMethods.
eFigure 1. Kaplan-Meier curves of progression-free survival for each arm, when considering all events in the per-protocol population (A) and in the intention-to-treat population (B)
eFigure 2. Pre-specified subgroup analysis of progression-free survival in patients treated according to clinician-driven treatment choice compared with patients treated according to CTC-driven treatment choice
eFigure 3. Kaplan-Meier curves of overall survival for each arm, when considering all events, in the Clinlow/CTClow subgroup (A), in the Clinhigh/CTChigh subgroup (B), in the Clinhigh/CTClow subgroup (C) and in the Clinlow/CTChigh subgroup (D)
eFigure 4. Kaplan-Meier curves of progression-free survival of patients treated by chemotherapy or endocrine therapy in the standard arm (A) and in the CTC arm (B)
eFigure 5. Kaplan-Meier curves of progression-free (A) and overall survival (B) of patients treated by chemotherapy or endocrine therapy in the pooled Clinhigh/CTClow and Clinlow/CTChigh subgroup
eTable 1. Baseline clinical and pathological characteristics of patients in the per-protocol population
eTable 2. Planned treatments, declared by physicians at inclusion, before randomization and CTC count
eTable 3. Treatments actually received in the per-protocol population
eTable 4. Adverse events. Number of patients for each event and corresponding percentage
Data Sharing Statement