

Abstract
The spread of coronavirus disease, 2019, has affected several countries in the world including Asian countries. The occurrences of COVID infections are uneven across countries and the same is determined by socioeconomic situations prevailing in the countries besides the preparedness and management. The paper is an attempt to empirically examine the socioeconomic determinants of the occurrence of COVID in Asian countries considering the data as of June 18, 2020, for 42 Asian countries. A multiple regression analysis in a cross‐sectional framework is specified and ordinary least square (OLS) technique with heteroscedasticity corrected robust standard error is employed to obtain regression coefficients. Explanatory variables that are highly collinear have been dropped from the analysis. The findings of the study show a positive significant association of per capita gross national income and net migration with the incidence of total COVID‐19 cases and daily new cases. The size of net migration emerged to be a potential factor and positive in determining the total and new cases of COVID. Social capital as measured by voters' turnout ratio (VTR) in order to indicate the people's participation is found to be significant and negative for daily new cases per million population. People's participation has played a very important role in checking the incidence of COVID cases and its spread. In alternate models, countries having high incidence of poverty are also having higher cases of COVID. Though the countries having higher percentage of aged populations are more prone to be affected by the spread of virus, but the sign of the coefficient of this variable for Asian country is not in the expected line. Previous year health expenditure and diabetic prevalence rate are not significant in the analysis. Therefore, people‐centric plan and making people more participatory and responsive in adhering to the social distancing norms in public and workplace and adopting preventive measures need to be focused on COVID management strategies. The countries having larger net migration and poverty ratio need to evolve comprehensive and inclusive strategies for testing, tracing, and massive awareness for sanitary practices, social distancing, and following government regulation for management of COVID‐19, besides appropriate food security measures and free provision of sanitary kits for vulnerable section.
1. INTRODUCTION
The contagious novel corona virus (COVID‐19) disease was initially identified in Wuhan, China in December 2019. Since then, the entire world has been transformed into a chaos hub; be it the challenging health problems it brought along with it or an inescapable economic blackout that was experienced all around the globe. The virus being a contagious one has managed to spread insanely to other countries in no time and after leading to the death of at least 213 people in China itself and with almost 10,000 cases nationally (BBC news, January 31, 2020), the World Health Organization (WHO) on March 12, 2020, declared the novel coronavirus outbreak as a global pandemic. Most of the countries were obviously not prepared for the pandemic and hence, death rates skyrocketed due to the lack of hospital beds and the inability to meet the health demands of an overcrowded inflow of COVID‐19 positive patients. Along with the huge toll that it took on human life, it has also posed a severe threat to the economy worldwide. The economies of some developed nations like the United States, China, United Kingdom, Germany, Italy, and France have undoubtedly been shaken. India being one of the fastest growing market economies is going to face a prolonged period of economic slowdown though it is tough to predict the exact magnitude of economic loss (Dev & Sengupta, 2020).
The numbers of the registered positive COVID‐19 cases are increasing exponentially and by far show no trend in being stable. Over 26 million cases with more than 0.8 million deaths are registered due to the COVID‐19 pandemic. Countries like United States, Brazil, Russia, Spain, UK, India, and Italy have the highest number of incidence of cases as well as deaths due to this global threat in the name of the novel coronavirus. The economy of the United States has suffered its most severe contraction in more than a decade in this year.
One of the reasons for the major economic breakdown is the inevitable decisions taken by the government following the suggestions of the WHO to maintain social distancing and people staying at home to reduce the number of cases of COVID‐19. Some countries which followed stringent government restrictions in lieu of keeping the contagious disease at bay are South Korea, New Zealand, Germany, and Japan. In Asia, countries like India, Iran, Turkey, Pakistan, Singapore, Saudi Arabia, and China have reported the highest number of cases pertaining to COVID‐19. A sharp recession in the economies of all the ASEAN countries has been seen lately.
A number of international agencies like World Bank, International Monetary Fund, and the Asian Development Bank have all forecasted a decline in regional growth due to the pandemic. The sudden drop in energy consumption all over the world due to nationwide lockdowns and travel ban has reduced the price of oil. Countries that have been dependent on the exports of fuel namely Indonesia and Malaysia have had a severe impact. The lack of effective demand has had multiplier effect on economies since consumption accounts to around 60% of GDP in major ASEAN countries (Searight, 2020).
Asia being the largest and most populous (4.6 billion as of 2020) continent has relatively more incidence of the cases due to COVID‐19. India shows the highest number of cases among the Asian countries and as it is the second‐largest populous country in the world. The country's figures relating to the incidence of COVID‐19 cases are increasing every day. Iran, Turkey, Pakistan, and Saudi Arabia are some of the other Asian countries that have also been showing increasing trends of COVID‐19 registered cases and deaths. China on the other hand, although was facing tremendous increase in the number of COVID‐19 positive cases during the onset of the hazardous disease, after a while has shown almost a stable and decreasing trend.
The present scenario of Asia in terms of the total number of registered positive COVID‐19 cases stands at more than 7 million from which almost 1.5 million cases are still active. The total number of deaths due to COVID‐19 is last recorded as 0.1 million. The numbers however are increasing every hour and hence may differ time to time. Nearly half of the world's population comes from the Asian countries. The socioeconomic evolution of these Asian countries in the past few decades has been tremendously contributing to the growth of the overall global economy. Hence, in a situation as scary and hazardous as a “Pandemic” the study of the determinants of COVID‐19 pandemic in the Asian countries plays an important role.
According to some experts, the hardest‐hit countries also had an aging population (Gardner, States, & Bagley, 2020; Lima et al., 2020) or an underdeveloped healthcare system (Mikhael & Al‐Jumaili, 2020; Tanne et al., 2020). Some others emphasized the role of the natural environment (Marco et al., 2020; Wu et al., 2020). In addition to this, several other factors like urbanization, poverty, low per capita income may also have some significant impact on the same. The argument however arises from the fact that the countries which have relatively low per capita income tend to perform poorly in managing health care services and providing health equipment like testing kits, personal protective equipment (PPE), and ventilators which are some of the urgent infrastructure needs.
However, evidences also suggest that the countries with high per capita income have also been affected with high incidence of the pandemic. These contrasting evidences are also seen in Asian countries. Asia being the amalgamation of both developed and developing countries gives us an ample scope to further analyze these evidences along with checking for other strong determinants of COVID‐19 such as social capital or people's participation ratio.
A number of studies have addressed the role that community participation has played through services like volunteering, adhering to the lockdown norms, and major steps people should take while countries are easing restrictions (Khongsai et al., 2020). The lockdown has created numerous difficulties to a larger section of the society. Therefore, the importance of social participation through sensitization of the issue as well as social services would help economies in controlling the virus and minimizing the aftershock of the pandemic (Gillespie et al., 2016; Marston, Renedo, & Miles, 2020). By the development of an economy, we do not always mean an increasing income or just reducing the poverty rates but it also includes an entire gamut of characteristics such as making people capable enough to perform different socioeconomic activities. People should act as both the agent to bring about the change as well as the beneficiary in the development process. Hence, people's participation too plays a key role in the development process. Besides people's participation, there are several other socioeconomic factors which may strongly determine the number of COVID‐19 registered cases and therefore there is an urgent need to study and identify the same mainly in Asian countries for the aforementioned reasons.
The rest of the paper is organized as follows: Section 2 provides the review of selected literature; Section 3 outlines the data and methodological framework of the study. Section 4 provides the analysis and interpretation of findings pertaining to the study and Section 5 concludes the study.
2. REVIEW OF SELECTED LITERATURE
In this section selected literature pertaining to socioeconomic factors determining contagious diseases including COVID‐19 have been reviewed.
Ghose, Seydou, and Sharmistha (2014) have analyzed the social determinants of HIV and tuberculosis for South Asian countries. They have observed that the incidence of infectious disease is related to a number of factors like houses that are overcrowded, poverty, inadequate nutrition, inequalities in the access to health care facilities, unhygienic conditions, and poor sanitation facilities. The study therefore emphasizes the need for ensuring quality and equity in the provision of health care. In addition, countries should emphasize on social stability, ensure a socially inclusive society, and ensure the involvement of communities in reducing health problems.
Mikhael and Al‐Jumaili (2020) have found that Arab countries like Bahrain, Saudi Arabia, Oman, Kuwait, Lebanon, and Oman have contacted the COVID‐19 virus due to the people visiting Iran. Iraq faced a lot of issues in the fight against COVID‐19 like lack of enough quarantine facilities, lack of enough testing facility, shortage of PPE kits, and lack of enough ambulances. Other factors those include are inadequate public awareness, unhygienic conditions, and people's resistance to high antibiotics. Qiu, Chen, and Shi (2020) have studied China's local and cross‐city transmissions. They observed that population movement from the source of the outbreak is a key factor. Social distancing measures like closed management of communities and restriction for family outdoor recreation activities would help in checking the spread.
Nicola et al. (2020) have summarized the socioeconomic effects of the pandemic. The decreased demand for the service sectors like trade hotel restaurant has reduced the demand for agricultural commodities. Panic buying due to measures like social distancing, isolating oneself, and ban on travels has led to shortages in stores. The price of oil has dropped and reduction in chemical industry production has been predicted around 1.2%. It has affected learners as educational institutions remain closed. Lack of nutrition due to the absence of free meals from schools is also an important social outcome. Stock markets have already witnessed a decline in its stock performance. Healthcare and pharmaceutical industries have been experiencing a high healthcare cost and a huge dearth of hospital beds and PPE. Hospitality, tourism, and aviation industries are facing serious losses.
Stojkoski, Utkovski, Jolakoski, Tevdovski, and Kocarev (2020) have analyzed the impact of socioeconomic factors like infrastructure in health, characteristics of the society, demographic factors, and economic factors. The results show that GDP per capita, population, and health spending have positive impact on COVID cases per million. The variables like the population using internet and lack of hygiene have a negative impact. Variables like life expectancy, population density have a negative impact on the registered COVID cases.
Mishra, Rath, and Dash (2020) have observed that the impact of COVID‐19 on stock returns is severe. Even the same is much worse than the effect of demonetization and GST implementation on stock returns. Szulczuk and Cheema (2020) have determined how a country's socioeconomic characteristics influence the COVID‐19 fatality rate making a cross country analysis. They have found that the number of medical doctors per 1,000 people is one of the significant factors and it has helped reduce the fatality rate from COVID‐19 the most. The number of hospital beds comes as second important factor. Also, a country with a higher unemployment rate seems to raise the fatality rate of COVID‐19 the most. According to them, the elderly and obese raise the fatality rate from COVID‐19 the most while current smokers and urban dwellers raise the fatality rate the least.
Ray and Subramanian (2020) have observed that most countries have adopted a lockdown strategy for flattening the curve. But the effectiveness of the same will depend upon how stringent countries are in implementing the model. Bahinipati et al. (2020) have analyzed the impact of COVID‐19 in the context of Andhra Pradesh, India. The study states that the policy makers take insights from behavioral economics to handle the pandemic in a more effective way. The states' informal sector is suffering and continues to suffer until normality returns. The regional food supply and farmers' income will have some serious effects if the lockdown goes on. The study suggests that the PDS system should be revamped and modernized in order to adjust to the current scenario.
Sumner, Hoy, and Ortiz‐Juarez (2020) have analyzed the social and economic impact of COVID‐19 on reduction in the per capita household income and consumption. They have observed that the COVID‐19 would increase the number of people living below the poverty line by 420 to 580 million. Bartscher, Seitz, Slotwinski, Siegloch, and Wehrhöfer (2020) have analyzed influence of social capital on the containment of COVID‐19 and mortality rate associated with the disease for seven European countries such as Germany, Austria, the Netherlands, Italy, Switzerland, Sweden, and the United Kingdom. The results show that an increase in social capital leads to 12% fewer cases in Germany and 32% fewer cases in Italy.
Patel et al. (2020) in his article mentioned that low socioeconomic status causes a number of factors through which COVID‐19 may occur. Overcrowded accommodation, employment opportunities that do not provide work from home facility, unstable work, and income conditions, reduced immunity due to poverty and seeking medical services at a more advanced stage of illness due to the same are some of the factors that he put out in his article. According to him, poverty makes an individual more vulnerable and hence susceptible to COVID‐19. He then urged the policymakers to introduce long‐term legislation to improve social welfare. Weill, Stigler, Deschenes, and Springborn (2020) have observed that the lower‐income communities show less social distancing than the same among the high‐income areas. Jalan and Sen (2020) have observed that public actions and enhancement of public trust by the people have helped Kerala, India in containing the COVID cases in the initial stage.
It is a known and studied fact that most of the Asian countries excluding few countries such as China, Japan, South Korea, Malaysia, Singapore, and Israel are characterized by low per capita income, slow GDP rate, and poor health infrastructural facilities. According to the human development index (HDI) report, the HDI of countries like India, Pakistan, Bangladesh, Afghanistan, and Iraq stands extremely low. In such a case, a pandemic as distorting as COVID‐19 only worsens the economic as well as social condition of these countries. Though the fight against COVID‐19 and checking spread of the disease mainly depend on its preparedness, management strategies, and resources they spent, but underlying socioeconomic factors are crucial in determining the number of cases and incidence. The geographic locations and ethnographic varieties attract quite a sum of tourists into these countries and therefore a huge influx of the same is experienced by these countries which certainly make sense for the increasing number of COVID‐19 positive cases. Therefore, the present study is an attempt to capture the socioeconomic determinants that affect the incidence of COVID among Asian countries.
3. DATA AND METHODOLOGY
Data for the study have been taken from various secondary sources like the United Nations Development Program and our world in data and the Institute for Demographic and Electoral Assistance. The study includes 46 Asian countries that have been recognized by the United Nations. The countries are Armenia, Afghanistan, Azerbaijan, Bahrain, Bangladesh, Bhutan, Brunei, Cambodia, China, Georgia, India, Indonesia, Iran, Iraq, Israel, Japan, Jordan, Kazakhstan, Kuwait, Kyrgyzstan, Laos, Lebanon, Malaysia, Maldives, Mongolia, Myanmar, Nepal, Oman, Pakistan, Philippines, Qatar, Saudi Arabia, Singapore, South Korea, Sri Lanka, Tajikistan, Thailand, Turkey, United Arab Emirates, Uzbekistan, Vietnam, Yemen and Palestine, Turkmenistan, Syria, and Timor.
This work is developed in the lines of Stojkoski et al. (2020). Socioeconomic factors like health expenditure share in GDP, net migration, old‐age dependency ratio, and gross national income per capita are important in understanding the prevailing situation and socioeconomic condition of the countries. Public choice variable such as voters' turnout ratio (VTR) is used as proxy for people's participation in countries. In order to understand the comorbidity factors, diabetic prevalence has been also considered in the analysis as a proxy. In order to understand the severity of COVID‐19, total COVID cases per million population, and new COVID cases per million population have been used as dependent variable alternatively. Though for pattern analysis we have used daily data up to June 18, 2020, for regression analysis, data have been used in cross‐sectional framework for June 18, 2020. As data are fluctuating on daily basis, while doing analysis data were available up to June 18, 2020. Considering the fact we have limited our analysis for the COVID positive cases as of June 18, 2020. Net migration, diabetic prevalence data are used for the year 2020, while socioeconomic factors have been used for the year 2018–2019 as available. The description of variables and data sources is provided in Table 1.
TABLE 1.
Description of variables
| Variable | Abbreviation | Description | Unit | Source |
|---|---|---|---|---|
| Total COVID‐19 positive cases | TCCPM | Total COVID‐19 positive cases per million population | Ratio | Our world in data |
| New COVID‐19 positive cases | NCCPM | New COVID‐19 positive cases per million | Ratio | Our world in data |
| Per capita gross national income | PCGNI | Gross national income divided by population | Ratio | United Nations Development Program |
| Share of health expenditure in 3.DP | HE | Health expenditure divided by GDP | Percentage | United Nations Development Program |
| Net migration | NM | Net migration represented by the difference between the number of people who come into a country and number of people who moved out of the same country | Ratio | United Nations Development |
| Old age dependency ratio | ODR | Old age dependency ratio is the number of people (in the age group of 65 and older) per 100 people (ages 15–64) | Ratio | United Nations Development Program |
| Voters' turnout ratio | VTR | Number of voters casted vote as a percentage of the total eligible voters | Ratio | Institute for Demographic and Electoral Assistance. |
| VTR dummy | VTRD | One for countries that are ruled by representatives elected by the people and 0 for countries under the rule of a king or a dictator | Dummy | Institute for Demographic and Electoral Assistance. |
| Diabetic prevalence rate | DPR | Diabetes prevalence refers to the percentage of people aged 20–79 who have type 1 or type 2 diabetes | Rate | Our world in data |
| Poverty line | PL | Percentage of people below poverty line | Percentage | United Nations development program |
Source: Compiled by authors.
Variables have been selected with proper reasons and considering their potential influence on the occurrence of infectious diseases. Health expenditure measures the preparedness of a country with respect to the COVID outbreak. Higher level of expenditure in health would ensure a country with ample health infrastructure both physical and manpower that will help to tackle the crises. Net migration is an important variable that affects the population density in urban areas. Countries with high migration rates are supposed to be affected by larger COVID incidences. Thirdly, the old‐age dependency ratio has been taken as countries with higher proportion of the old population are more susceptible to the disease. Another variable considered for the analysis includes the per capita gross national income. The reason for the inclusion of the variable is to analyze the impact of income on the incidence of the disease. An interesting variable of concern is the social capital. Social capital refers to the collective action of people in achieving a common objective. An attempt is made to measure people's participation or social capital through VTR. Therefore, collective action and more public response would have a negative impact on the incidence of the disease. Co‐morbidity factor like the diabetic prevalence rate has been taken into account in order to understand whether people with co‐morbidity are more affected by COVID‐19. The reason for the same is that people with diabetes have low immunity as a result of which are largely susceptible to the disease. Lastly, an important variable considered in the analysis is the poverty rate. This is considered alternatively in lieu of per capita national income in order to avoid multi‐collinearity. Countries with a larger proportion of population living below the poverty line also indicate that a large section of people in those countries may not have access to basic amenities. Large scale poverty also denotes the accumulation of slums in urban centers. Therefore, both lack of immunity and proliferation of slums lead to a faster spread of the disease. The descriptive statistics of variables used in the study are given in Table 2. In addition, the pattern of total cases and new positive COVID‐19 cases in Asian countries has been analyzed.
TABLE 2.
Descriptive statistics
| NCPM | PCGNI | HE | NM | ODR | PL | DPR | TCCPM | VTR dummy | |
|---|---|---|---|---|---|---|---|---|---|
| Mean | 39.71 | 22,900.43 | 5.41 | 2.06 | 9.92 | 0.74 | 39.71 | 2,267.93 | 5.41 |
| Maximum | 380.76 | 110,489.0 | 10.90 | 31.10 | 46.20 | 0.94 | 380.7 | 28,869.24 | 10.90 |
| Minimum | 0.00 | 1,433.000 | 2.30 | −4.60 | 1.30 | 0.46 | 0.00 | 2.611 | 2.30 |
| Std. dev. | 77.45 | 25,519.16 | 2.31 | 7.21 | 7.65 | 0.11 | 77.45 | 4,978.3 | 2.31 |
| Observations | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 | 42 |
Source: Computed by authors using EViews.
Multivariate cross‐sectional regression has been performed to analyze the impact of these factors on the total cases and new cases of COVID‐19. For the regression analysis the study uses only 42 countries as data pertaining to Palestine, Turkmenistan, Syria, and Timor have not been included due to the non‐availability of data. The general functional forms of the model to indicate dependent and explanatory variables are given as:
Ordinary least square estimation technique is adopted to obtain the regression coefficients. Correlation matrix of the independent variables is computed to check for the presence of multi‐collinearity. It is shown in Tables 3 and 4. It is observed that there is no problem of multi‐collinearity. As analysis involves cross country analysis, presence of heteroscedasticity may influence the coefficients. In order to correct for the existence of heteroscedasticity, White heteroscedasticity‐consistent standard errors and covariances have been used.
TABLE 3.
Correlation matrix
| VTR | ODR | HE | NM | PCGNI | DPR | |
|---|---|---|---|---|---|---|
| VTR | 1 | −0.066792 | −0.4040888 | 0.000948 | 0.1276547 | −0.2119620 |
| ODR | −0.066792 | 1 | 0.4049216 | −0.245687 | 0.255845 | −0.201511 |
| HE | −0.404088 | 0.404921 | 1 | 0.05485976 | −0.048593 | −0.090826 |
| NM | 0.000948 | −0.245687 | 0.054859 | 1 | 0.443269 | 0.480300 |
| PCGNI | 0.127654 | 0.255845 | −0.048593 | 0.443269 | 1 | 0.447977 |
| DPR | −0.211962 | −0.201511 | −0.090826 | 0.480300 | 0.447977 | 1 |
Source: Authors calculation using EViews.
TABLE 4.
Correlation matrix
| VTR | ODR | HE | NM | PL | DPR | |
|---|---|---|---|---|---|---|
| VTR | 1 | −0.06679 | −0.40408 | 0.00094 | −0.05572 | −0.21196 |
| ODR | −0.06679 | 1 | 0.40492 | −0.24568 | 0.46204 | −0.20151 |
| HE | −0.40408 | 0.40492 | 1 | 0.05485 | 0.133689 | −0.09082 |
| NM | 0.00094 | −0.24568 | 0.05485 | 1 | 0.200719 | 0.48030 |
| PCGNI | −0.05572 | 0.46204 | 0.13368 | 0.20071 | 1 | 0.18211 |
| DPR | −0.21196 | −0.20151 | −0.09082 | 0.4803 | 0.18211 | 1 |
Source: Authors calculation using EViews.
4. RESULTS AND DISCUSSION
Findings pertaining to pattern and determinants COVID‐19 cases in Asian countries have been presented and discussed in this section.
4.1. Pattern analysis
The pattern of COVID‐19 cases and new cases on daily basis for Asian countries are shown in this subsection. Figure 1 shows the pattern average of total COVID‐19 cases and new cases reported daily basis for Asian countries.
FIGURE 1.
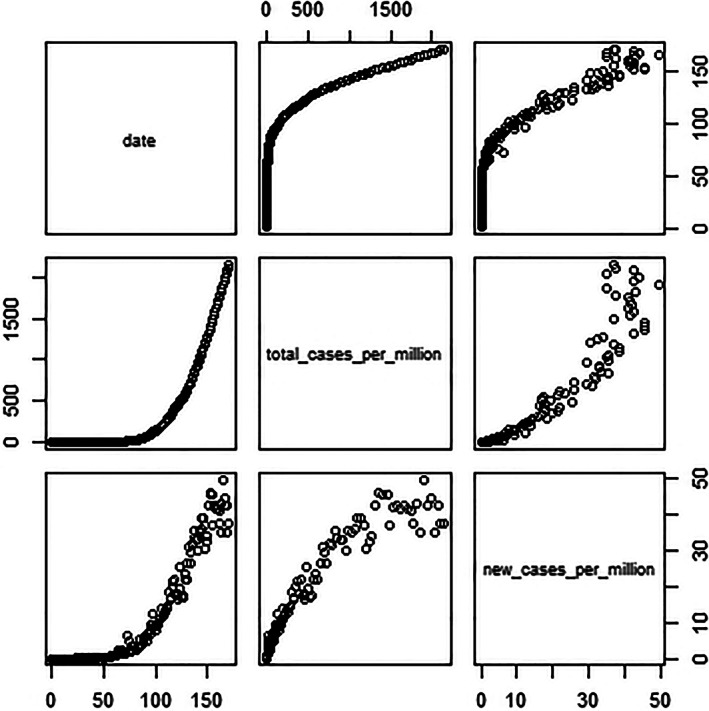
Average total cases and new cases of COVID‐19 for Asia. Source: Authors' calculation from the source data
Figure 1 clearly explains how both the average total cases and average new cases have shown an increasing trend. The second graph in the first column measures the average total cases of COVID‐19 shows an increasing trend over time. The number of cases has been increasing over the time period for Asian countries. The third graph in the first column clearly shows that the average number of new cases has been increasing over the time period for Asian countries. The scatter plot for both total cases and new cases are shown in the third graph in the second column and the second graph in the third column. The responsiveness of new cases to total cases is elastic in the initial stages and becomes inelastic towards the latter time period. Therefore, it has been observed that over time although the total cases have been increasing, the change that is measured by the new cases is now at a constant rate.
Figure 2 shows the panel plot for the seven countries that have had the highest average. A majority of cases have been recorded for most of the Arabian countries. These countries are all hubs for huge migration as a result the incidence of the disease would be the highest due to population density. The new cases have increased over time, whereas the numbers of new positive cases have been stable.
FIGURE 2.
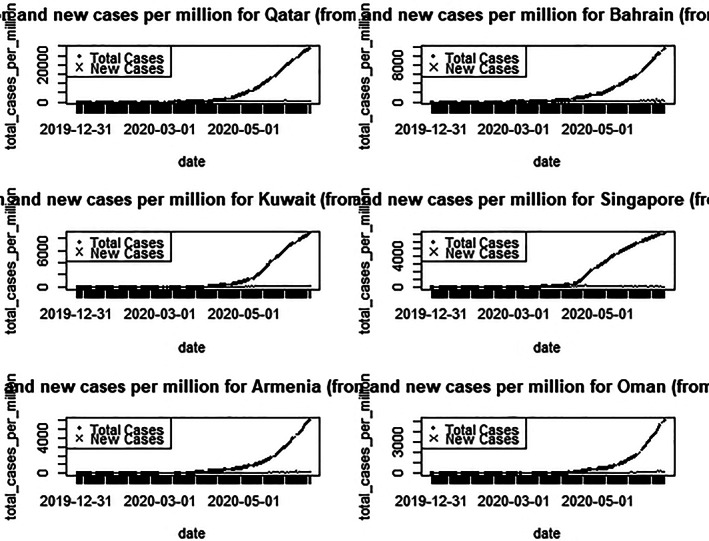
Total cases per million and new cases per million. Source: Authors' calculation from the source data
4.2. Socioeconomic determinants
In this section, results pertaining to socioeconomic determinants are presented. Table 5 presents the determinants of total number COVID positive cases per million population.
TABLE 5.
Total COVID cases per million population as the dependent variable
| Model A | Model B | Model C | Model D | |
|---|---|---|---|---|
| PCGNI | 0.081628* | 0.133342* | ||
| PL | 4,588.642*** | 4,533.335 | ||
| HE | 170.5377 | 268.4281 | 90.63936 | −37.70550 |
| NM | 166.0909* | 208.7379* | 225.4832* | 360.5083 |
| ODR | −88.45547* | −151.6870** | −32.82346 | −41.41700 |
| VTR | −6.624669 | 10.85139 | ||
| VTR (dummy) | 310.6794 | −3,778.646 | ||
| DPR | 198.2683 | −1,261.873 | 1,560.093 | 770.6377 |
| c | −149.7874 | 1,288.068 | −6,334.898 | 444.9559 |
| R squared | 0.777302 | 0.673399 | 0.655275 | 0.506167 |
| F statistic | 0.00000 | 0.000000 | 0.000007 | 0.00000 |
Indicates statistical significance of coefficients at 1% level of significance.
Indicates statistical significance of coefficients at 5% level of significance.
Indicates statistical significance of coefficients at 10% level of significance.
Source: Authors calculation using EViews.
Model A in Table 5 shows a positive significant relationship of per capita gross national income on the total COVID cases. Countries having higher per capita income are showing higher traces of COVID‐19 cases. This can be explained in terms of the growth‐based and countries having more economic activities all over the world are more affected by COVID cases. Similar pattern is observed in the case of Asian countries. PCGNI coefficient emerged to be significant and positive. This suggests that countries with high per capita GNI are having higher COVID cases in Asia. Economic advancement has led to more economic activities and more movement of people. As a result, the incidence of COVID rates and exposure increases.
On the other hand, the variable like net migration rate (NM) has a positive significant relationship on a countries' total number of COVID cases as well as daily new cases. Migrants are usually concentrated in cities those are centers for economic activities. Migrants' movement between countries has created more exposure and contact of COVID patients. Sirkeci&Yucesahin, (2020) have suggested that monitoring origins and destinations of immigrants may help better in manging COVID‐19.
Old age dependency ratio (ODR) has a negative significant relationship on the total number of cases per million. Studies have verified that the morbidity rate was higher in the younger generation than in the older sections of the society (Cortis, 2020). Though there is observations from earlier infectious diseases that old aged population are more prone to be affected in spread of virus, but in the recent COVID cases, even young adults and children are also affected.
Another variable that was proved to be positively significant was the poverty rate. Countries having a higher poverty rates are those countries where more people live below the income line deciding poverty rate. The income is an important factor determining the nutritional intake of the citizens. The nutritional intake plays a very important role in deciding the immunity resistance of people. Studies have confirmed the importance of immunity in fighting the pandemic. A similar result has been obtained in model C and model D in which poverty ratio is used in lieu of PCGNI in order to understand the influence of poverty on incidence of COVID. Countries having high poverty rates have been susceptible to more COVID cases (model C in Table 5). Health expenditure and diabetes prevalence rate are not significant in the analysis above. Models B and D use VTR dummy in place of VTR ratio. However, both the variables are not significant for total number of COVID cases.
Table 6 shows the regression coefficients of new cases per million population in the Asian countries. A model showing the impact on new cases per million has been analyzed in Table 6. The variables like per capita gross national income, net migration, and poverty line have been positively significant on the new cases per million. An interesting fact that has been observed is the impact of social capital measured by the voter's turnover ratios is negatively related with the new cases per million. The World Health Organization has emphasized the importance of people's participation in helping fight against the pandemic. People's participation plays a major role by maintaining social distancing, hand washing, rendering social services, and strictly adhering to government's advisory. Besides, people would be more responsive to create awareness among their circle for social distancing and avoid public gatherings.
TABLE 6.
Total new cases per million as the dependent variable
| Model A | Model B | Model C | Model D | |
|---|---|---|---|---|
| PCGNI | 0.000729*** | 0.001225 | ||
| PL | −5.373405 | 3.964700 | ||
| HE | −0.124730 | 4.351650 | −1.153153 | 1.334687 |
| NM | 4.557108* | 4.764891* | 5.306898* | 6.322142* |
| ODR | −0.983269 | −1.942100** | −0.044295 | −0.594274 |
| VTR | −0.890436** | −0.747261*** | ||
| VTR (dummy) | −12.55149 | −53.44859 | ||
| DPR | −4.530121 | −3.858449 | 9.902987 | 17.28749 |
| c | 89.85447* | 16.91086 | 61.24099 | 32.12198 |
| R squared | 0.604658 | 0.598900 | 0.576038 | 0.538036 |
| F statistic | 0.000000 | 0.000000 | 0.000127 | −5.373405 |
Indicates statistical significance of coefficients at 1% level of significance.
Indicates statistical significance of coefficients at 5% level of significance.
Indicates statistical significance of coefficients at 10% level of significance.
Source: Authors calculation using EViews.
5. CONCLUSION AND POLICY SUGGESTIONS
The study analyses the socioeconomic determinants of COVID‐19 for the 42 Asian countries. A linear multiple regression model in a cross‐sectional framework has been used to study the factors that contribute to the incidence of the pandemic. A number of factors like the net migration and per capita gross national income are found to have a positive significant relationship on the occurrence of total COVID cases in Asian countries. In alternate models, countries having high incidence of poverty are also having higher cases of COVID. In addition, voter's turnover ratio as a proxy for people's participation emerged significant and negative for daily new cases.
Growth‐based countries have not been able to fight the pandemic efficiently. They have witnessed higher surge of COVID cases. Opening up economic activities has created the problem of spreading the virus. Similar pattern is observed in case of Asian countries. Countries having high per capita GNI are more affected by COVID. Rather strategies such as stringent social distancing and contact tracing and testing are important.
The countries having larger reverse migration have been more affected by COVID. Effective management of migrants coming back to the country from COVID‐prone zone will help countries to check on COVID positive cases. Another important influence that arises for daily new COVID cases is people's participation as measured by VTR. It significantly and negatively affects the occurrence of daily new cases. This suggests that countries in which people have active participation in public programmers or they are more sensitive to adhere to governments' advice and guidelines can restrict occurrence of new cases. In those cases social distancing and voluntary participation of people for testing and preventive measures would be successful. Therefore, people‐centric plans and involvement of people are crucial to check the spread of virus.
Fighting poverty has been the target for both millennium development goals as well as sustainable development goals. It is a known fact that a number of Asian countries have low per capita incomes and low infrastructure facilities in health. The need to eradicate poverty is of utmost interest as countries facing poverty have also faced high incidence of the disease. The countries in Asia which are more poverty ridden are also affected with higher COVID rates. Though it is contrasting to findings of high‐income countries are also more affected because of more economic activities and movement of people. However, the implementation of social distancing and safe sanitary practices in areas of more concentration of poor is not relatively easy. Creating awareness, provision of sanitary kits, and making people more participatory are important in managing COVID crises. Therefore, countries in Asia will have to follow an inclusive strategy to be well equipped to manage crises.
ACKNOWLEDGEMENTS
The authors would like to extend their sincere thanks to Prof. A. P. Dash for his suggestions and constant encouragement. Thanks are due to anonymous reviewers for useful suggestions for development of the work. However, the authors are solely responsible for errors if any.
Biographies
Rittu Susan Varkey has a Ph.D in Economics from Central University of Tamil Nadu, India. She is presently working as Assistant Professor, Department of Economics, CHRIST University , Bengaluru. Her specialization includes Development economics and Health economics.
Justin Joy has a Ph.D in Economics from Central University of Tamil Nadu, India. She is presently working as Assistant Professor, Department of Economics, CHRIST University , Bengaluru. His area of interest includes Public Finance and Macroeconomics.
Gargee Sarmah is Doctoral Scholar at Department of Economics, Central University of Tamil Nadu, India. Her area of interest is Public finance.
Prasant Kumar Panda has a Ph.D in Economics from Pondicherry University, India. He is presently working as Professor, Department of Economics, Central University of Tamil Nadu, India. He has received training in Public Finance and Policy from National Institute of Public Finance and Public Policy, New Delhi. He was a KN Raj Teacher fellow at Centre for Development studies, Trivendrum . His area of research includes Public finance and policy, Federal fiscal Transfers, and Health Economics. He is the life member of the Indian Econometric Society and Indian association for research in national income and wealth.
Varkey RS, Joy J, Sarmah G, Panda PK. Socioeconomic determinants of COVID‐19 in Asian countries: An empirical analysis. J Public Affairs. 2021;21:e2532. 10.1002/pa.2532
REFERENCES
- Bahinipati, C. S. , Sirohi, R. A. , Biswal, D. , Gouthami, K. , Suresh, G. , & Singh, M. (2020). Covid‐19: Policy interventions and socio‐economic impact in Andhra Pradesh, India. Technical report, Munich Personal RePEc Archive.
- Bartscher, A. K. , Seitz, S. , Slotwinski, M. , Siegloch, S. , & Wehrhöfer, N. (2020). Social capital and the spread of covid‐19: Insights from European countries. Technical Report, CESifo Working Paper No. 8346. [DOI] [PMC free article] [PubMed]
- Cortis, D. (2020). On determining the age distribution of Covid‐19 pandemic. Frontiers in Public Health, 8, 202. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dev, S. M. , & Sengupta, R. (2020). Covid‐19: Impact on the Indian economy. http://www.igidr.ac.in/pdf/publication/WP-2020-013.pdf
- Gardner, W. , States, D. , & Bagley, N. (2020). The coronavirus and the risks to the elderly in long‐term care. Journal of Aging & Social Policy, 32(4), 1–6. [DOI] [PubMed] [Google Scholar]
- Ghose, B. , Seydou, I. , & Sharmistha, G. (2014). Social Determinants of Infectious Diseases in South Asia. International Scholarly Research Notices, 2014. 10.1155/2014/135243. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gillespie, A. M. , Obregon, R. , El Asawi, R. , Richey, C. , Manoncourt, E. , Joshi, K. , … Quereshi, S. (2016). Social mobilization and community engagement central to the Ebola response in West Africa: Lessons for future public health emergencies. Global Health: Science and Practice, 4(4), 626–646. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Jalan, J. , & Sen, A. (2020). Containing a pandemic with public actions and public trust: The Kerala story. Indian Economic Review. 10.1007/s41775-020-00087-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Khongsai, L. , Anal, T. S. C. , Rapheileng, A. S. , Kh, T. S. , Shah, M. K. , & Pandey, D. (2020). Combating the spread of COVID‐19 through community participation. Global Social Welfare, 1–6. 10.1007/s40609-020-00174-4. [Epub ahead of print] [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lima, C. K. T. , de Medeiros Carvalho, P. M. , de Arajo Araruna Silva Lima, I. , De Oliveira Nunes, J. V. A. , Saraiva, J. S. , de Souza, R. I. , … Neto, M. L. R. (2020). The emotional impact of coronavirus 2019‐nCoV (new Coronavirus disease). Psychiatry Research, 287, 112915. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marco, Di M. , Baker, M.L. , Daszak, P. , De Barro, P. , Eskew, E.A. , Godde, C.M. , & Karesh, W.B. (2020). Opinion: Sustainable development must account for pandemic risk. Proceedings of the National Academy of Sciences, 117(8), 3888–3892. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marston, C. , Renedo, A. , & Miles, S. (2020). Community participation is crucial in a pandemic. The Lancet, 395(10238), 1676–1678. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mikhael, E. M. , & Al‐Jumaili, A. A. (2020). Can developing countries face novel coronavirus outbreak alone? The Iraqi situation. Public Health in Practice, 1, 100004. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mishra, A. K. , Rath, B. N. , & Dash, A. K. (2020). Does the Indian financial market nosedive because of the COVID‐19 outbreak, in comparison to after demonetisation and the GST? Emerging Markets Finance and Trade, 56(10), 2162–2180. [Google Scholar]
- Nicola, M. , Alsafi, Z. , Sohrabi, C. , Kerwan, A. , Al‐Jabir, A. , Iosifidis, C. , … Agha, R. (2020). The socio‐economic implications of the coronavirus pandemic (COVID‐19): A review. International Journal of Surgery, 78, 185–193. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Patel, J. A. , Nielsen, F. , Badiani, A. A. , Assi, S. , Unadkat, V. A. , Patel, B. , … Wardle, H. (2020). Poverty, inequality and COVID‐19: The forgotten vulnerable. Public Health, 183, 110–111. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Qiu, Y. , Chen, X. , & Shi, W. (2020). Impacts of social and economic factors on the transmission of coronavirus disease 2019 (COVID‐19) in China. Journal of Population Economics, 33, 11271172. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ray, D. , & Subramanian, S. (2020). India's lockdown: An interim report. Technical report. National Bureau of Economic Research. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Searight, A . (2020). The economic toll of Covid‐19 on Southeast Asia: Recession looms as growth prospects dim. Technical report. Washington, DC: Center for Strategic and International Studies (CSIS). [Google Scholar]
- Sirkeci, I. , & Yucesahin, M. M. (2020). Coronavirus and migration: Analysis of human mobility and the spread of Covid‐19. Migration Letters, 17(2), 379–398. [Google Scholar]
- Stojkoski, V , Utkovski, Z , Jolakoski, P , Tevdovski, D , & Kocarev, L (2020). The socio‐economic determinants of the coronavirus disease (COVID‐19) pandemic. https://arxiv.org/abs/2004.07947.
- Sumner, A. , Hoy, C. , & Ortiz‐Juarez, E. (2020). Estimates of the impact of Covid‐19 on global poverty. Technical report, UNU‐WIDER Working Paper 2020/43.
- Szulczuk, K. , & Cheema, M. A. (2020). Covid‐19: The impact of socioeconomic characteristics on the fatality rate. Technical report.
- Tanne, J. H. , Hayasaki, E. , Zastrow, M. , Pulla, P. , Smith, P. , & Rada, A. G. (2020). Covid‐19: How doctors and healthcare systems are tackling coronavirus worldwide. BMJ, 368, m1090. [DOI] [PubMed] [Google Scholar]
- Weill, J. A. , Stigler, M. , Deschenes, O. , & Springborn, M. R. (2020). Social distancing responses to COVID‐19 emergency declarations strongly differentiated by income. Proceedings of the National Academy of Sciences, 117(33), 19658–19660. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wu, X. , Nethery, R.C , Sabath, B.M. , Braun, D. , & Dominici, F. (2020). Exposure to air pollution and covid‐19 mortality in the United States. medRxiv, https://www.medrxiv.org/content/10.1101/2020.04.05.20054502v2. [DOI] [PMC free article] [PubMed] [Google Scholar]