

Abstract
Introduction:
The purpose of this study is to evaluate the efficacy and safety of complementary and alternative medicine in the treatment of autism spectrum disorder.
Methods and analysis:
We will electronically search Pubmed, Medline, Embase, Web of Science, the Cochrane Central Register of Controlled Trial, China National Knowledge Infrastructure, China Biomedical Literature Database, China Science Journal Database, and Wan-fang Database from their inception. Also, we will manually retrieve other resources, including reference lists of identified publications, conference articles, and gray literature. The clinical randomized controlled trials or quasi-randomized controlled trials related to complementary and alternative medicine treating autism spectrum disorder will be included in the study. The language is limited to Chinese and English. Research selection, data extraction, and research quality assessment will be independently completed by 2 researchers. Data were synthesized by using a fixed-effect model or random-effect model depend on the heterogeneity test. The Childhood Autism Rating Scale (CARS) and Autism Behavior Checklist (ABC) scores will be the primary outcomes. The scores of the Autism Treatment Evaluation Checklist and the Ritvo-Freeman Real Life Rating Scale will also be assessed as secondary outcomes. RevMan V.5.3 statistical software will be used for meta-analysis, and the level of evidence will be assessed by Grading of Recommendations Assessment, Development, and Evaluation (GRADE). Continuous data will be expressed in the form of weighted mean difference or standardized mean difference with 95% confidence intervals (CIs), whereas dichotomous data will be expressed in the form of relative risk with 95% CIs.
Ethics and dissemination:
The protocol of this systematic review does not require ethical approval because it does not involve humans. We will publish this article in peer-reviewed journals and presented at relevant conferences.
Systematic review registration:
OSF Registries, DOI: 10.17605/OSF.IO/ HA97R (https://osf.io/ha97r)
Keywords: autism spectrum disorder, complementary and alternative medicine, protocol, systematic review
1. Introduction
Similar to other neurodevelopmental disabilities, autism spectrum disorder (ASD) is considered lacking satisfactory cure and requiring long-term management.[1] The prevalence of ASD was reported raising in the last decades, ranged of 6.5 to 6.6 per 1000 or approximately 1 in 160 children are suffering from ASD.[2–4] Regardless of intellectual developing, ASD children remain within the spectrum as adults and reporting problems with their living, working, social abilities and mental health.[5,6]
To date, no medication is proven to be effective in treating core symptoms of ASD, varies of approaches investigated the use of anti-psychotics, stimulants and nonstimulants, antidepressants, (GABA)ergic and cholinergic agents, and oxytocin, among others in ASD, the limited evidences unsupported pharmacotherapy in children with ASD, and side-effects with long-term use can be burdensome.[7]
Despite of their limited evidence and potential adverse effects, the use of complementary and alternative medicine (CAM) is popular in children with ASD.[8] Among children with ASD, use of CAM ranges from 28% to 51%, with lifetime use as high as 71% in United States, and 46% in Germany.[8,9] CAM treatments are used for a variety of symptoms in children with ASD, including core symptoms of ASD, concentration, relaxation, gastrointestinal symptoms, sleep disturbance, communication, sensory issues, seizures, and for general health.[10] Melatonin, omega-3 fatty acids, methyl B12, oxytocin, vitamin supplementation, ginkgo biloba, acupuncture, hyperbaric oxygen therapy, and chelation therapy are common CAM forms applied on ASD children. These different forms of CAM were administrated for various symptoms in ASD; most parents selected CAM for their concern of side-effects from pharmacotherapy, and they also reported some benefits from CAM, despite of lacking evidences of these CAM treatments.[11–14] Therefore, to investigate the safety and efficacy of CAM in the treatment of ASD, we plan to conduct this systematic review (SR) and meta-analysis.
2. Methods
The protocol has been registered on OSF as Registration DOI: 10.17605/OSF.IO/HA97R (https://osf.io/ha97r). The protocol follows the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) 2015 statement guidelines.[15] We will report the changes in the full review if necessary.
2.1. Inclusion and exclusion criteria for study selection
2.1.1. Inclusion criteria
This study will include randomized controlled trials (RCTs) of complementary and alternative medicine treatment for autism spectrum disorder patients, whether using blind method or allocation concealment method, including those using a quasi-random method such as alternate allocation or allocation by birth date. We included both parallel and cross-over studies. The language of the trials to be included should be Chinese or English.
2.1.2. Exclusion criteria
Following studies would be excluded: case reports and reviews, literature not in English or Chinese language, and clinical research studies that compared different kinds of CAM.
2.2. Types of participants
We would include patients with ASD under the age of 18 years, regardless of sex or race, diagnosed by standard criteria such as the Diagnostic and Statistical Manual of Mental Disorders (DSM) or the International Classification of Diseases (ICD). We accept diagnoses by assessment tools such as the Autism Diagnostic Observation Scale (ADOS), Autism Diagnostic Interview Revised (ADI-R), Childhood Autism Rating Scale (CARS), Chinese Classification of Mental Disorder (CCMD), and other validated tools. Studies on ASD were included even if they did not refer to the diagnostic criteria.
2.3. Types of interventions and comparators
CAM therapies for treating ASD include modified/special diets, vitamins/minerals, food supplements, acupuncture, and Chinese medicine. These interventions can be used alone or in combination. Controlled interventions included control groups with no treatment, sham/placebo groups, or other conventional treatments.
2.4. Types of outcome measures
2.4.1. Primary outcomes
We select the score of Childhood Autism Rating Scale (CARS) and autism behavior checklist (ABC) as primary outcomes.
2.4.2. Secondary outcomes
We also care about the scores of the Autism Treatment Evaluation Checklist, and the Ritvo-Freeman Real Life Rating Scale; meanwhile, the social interaction skills, communication ability, or stereotypy, language ability, and cognitive function would be taken into consideration.
3. Data sources
3.1. Electronic searches
Following databases will be searched: PubMed, Web of Science, the Cochrane Central Register of Controlled Trials, AMED, MEDLINE, EMBASE, Cochrane Library, China National Knowledge Infrastructure (CNKI), Wanfang data, Chinese Scientific Journals Database (VIP), and China biomedical literature database (CBM). We will select the eligible studies published up to August 31, 2020. The search terms used in the SR are as follows: complementary and alternative medicine, autism spectrum disorder, neurodevelopmental disorder, melatonin, vitamin, Omega-3 fatty acids, acupuncture, hyperbaric oxygen therapy, chelation therapy, among others.
We will not apply any language, population, or national restrictions. The specific search strategy will be (taking PubMed as an example) listed on Table 1. Similar search strategy will be applied to other electronic databases.
Table 1.
Search strategy sample of PubMed.
| Number | Searches |
| #1 | randomized controlled trial[MeSH Terms] |
| #2 | autism spectrum disorder[MeSH Terms] |
| #3 | autism spectrum disorder[Text Word] |
| #4 | neurodevelopmental disorder[MeSH Terms] |
| #5 | neurodevelopmental disorder[Text Word] |
| #6 | or/#2–5 |
| #7 | complementary and alternative medicine[MeSH Terms] |
| #8 | acupuncture[MeSH Terms] |
| #9 | melatonin[MeSH Terms] |
| #10 | L-Carnosine[MeSH Terms] |
| #11 | N-acetylcysteine[MeSH Terms] |
| #12 | Omega-3 fatty acids[MeSH Terms] |
| #13 | vitamin[MeSH Terms] |
| #14 | tetrahydrobiopterin[MeSH Terms] |
| #15 | hyperbaric oxygen therapy[MeSH Terms] |
| #16 | chelation therapy[MeSH Terms] |
| #17 | or/#7–6 |
| #18 | #1and#6and#17 |
We will identify relevant randomized controlled trials and the selected studies will be analyzed according to the Cochrane Handbook.
3.2. Searching other resources
We also retrieve manual-related documents, such as replacing and supplementing some reference documents, medical textbooks, clinical laboratory manuals, and the World Health Organization International Registry of Clinical Trials. At the same time, we will contact experts and authors in this field to obtain important information that cannot be found in the search. The research flow chart is shown in Figure 1.
Figure 1.
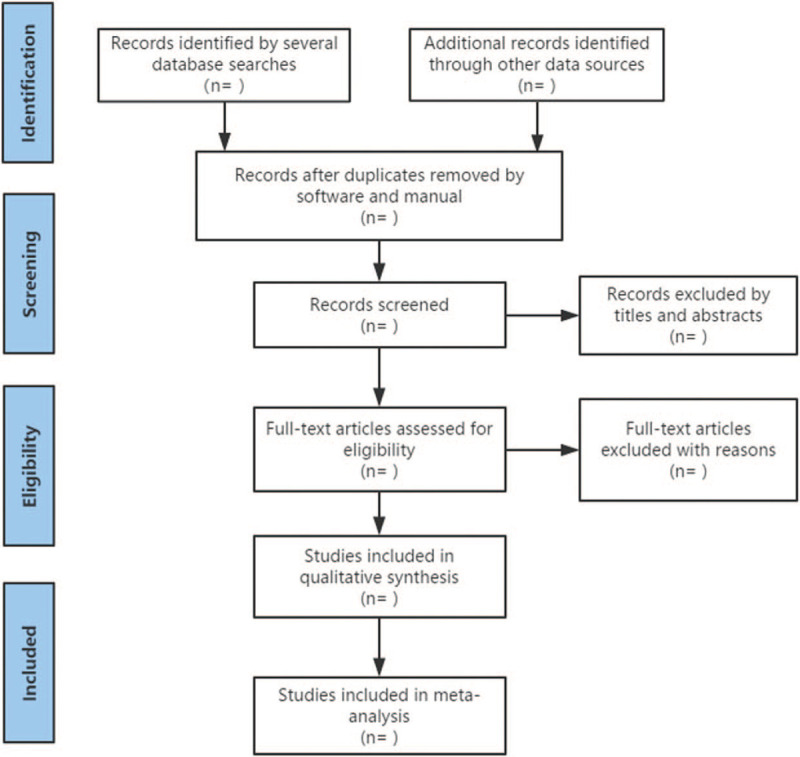
The research flow chart.
4. Data collection and analysis
4.1. Selection of studies
Two independent researchers (SB and JH) will assess the full-text articles from the search results independently against the inclusion and exclusion criteria. Discrepancies will be discussed and resolved by consensus with a third author (DR).
4.2. Data extraction and management
The following information will be extracted from each study: research number, data extractor, date of data extraction, general situation of the study, research methodology, research population, baseline comparability, interventions, main outcome indicators, secondary outcome indicators, combined drug use, adverse reactions or complications, among others. For those with questions or incomplete information, we will try to contact the author to obtain information before deciding whether to include it.
4.3. Assessment of the reporting quality and risk of bias
Two of the authors (SB and JH) individually assessed the risk of bias using assessments included in the study were evaluated in the Cochrane System Evaluator's Manual for RCT quality evaluation criteria. Assessing the risk of bias: random sequence generation; allocation concealment; blinding of participants and personnel; blinding of outcome assessment; incomplete outcome data; selective outcome reporting; other bias. Every domain was classified as high risk of bias, low risk of bias or unclear risk of bias. Any arising difference was resolved by discussion.
4.4. Measures of a treatment effect
We will measure continuous data with mean difference (MD) or standard MD for the therapeutic effect with 95% CIs. For dichotomous data, risk ratios (RR) with 95% CIs will be calculated.
4.5. Management of missing data
To obtain the missing data, we will contact the corresponding author. If no response will be obtained, we will analyze only the available data and describe the reason and impact of this exclusion in the paper.
4.6. Assessment of a reporting bias
Publication bias will be explored through funnel plot analysis. GRADE profiler 3.6 is used to evaluate the quality of evidence. The specific contents include: limitations of research, inconsistency of research results, indirect evidence, inadequate accuracy, publication bias. Finally, the quality of evidence is divided into 4 levels: high-level evidence, intermediate evidence, low-level evidence, and very low-level evidence.
4.7. Assessment of heterogeneity
All literature will use I2 value of the χ2 test (a = 0.1) to determine the heterogeneity. When I2 ≤50%, it is considered acceptable. When I2 > 50%, subgroup analysis should be performed to identify potential causes and record them.
4.8. Data synthesis and grading of quality of evidence
RevMan 5.3 software was used for statistical analysis of data. RR was used for binary variables and MD was used for continuous variables. Heterogeneity analysis will be conducted by heterogeneity test, P and I2 represent the size of heterogeneity among multiple studies. When P is >0.1 and I2 is <50%, it suggests heterogeneity is small, and on the contrary, it suggests heterogeneity is large. Heterogeneity is mainly handled by subgroup analysis. Sensitivity analysis is used to test the reliability of the overall effect.
4.9. Subgroup analysis
When the heterogeneity test results are heterogeneous, we will conduct subgroup analysis to explore the possible causes of heterogeneity. The effects of different types of acupuncture therapy including design scheme, severity of illness, age, sex, and mild or severe AP were analyzed. We will also delete low-quality and/or medium-quality studies to check the robustness of the results.
4.10. Sensitivity analysis
Sensitivity analysis will be used to test the quality of the research contained in the sampled documents. The stability of the conclusions can be tested by re-analyzing the conclusions by inputting missing data and changing the type of research.
4.11. Ethics and dissemination
The results of the system review will be published in peer-reviewed journals, disseminated at relevant meetings, or disseminated in peer-reviewed publications, and we use aggregated published data to exclude individual patient data, so ethical approval, and informed consent is not required.
5. Discussion
CAM treatments are popular in the intervention of ASD. Evidences showed different forms of CAM might bring ASD children benefit in different aspects.
Studies showed the efficacy of melatonin in treating sleep disturbance on ASD children and adolescents, it was reported to be well tolerated and safe.[16,17] Omega-3 fatty acids have been examined to be a potential treatment for ASD, specific for the associated symptoms of hyperactivity, although most studies failed to show statistical significance in improving either autism core symptoms or hyperactivity, omega-3 fatty acids were showed well-tolerated.[18–21] As for vitamin D supplementation, a study found significant improvement on ASD children for CARS and ABC scores, and the improvements were more pronounced in children younger than 3 years.[22] As a major form of Chinese medicine, from clinical trials and SRs, acupuncture is reported to improve various developmental and behavioral aspects of children with ASD, it's safe but children experienced pain and cried during the treatment.[23–26] Tetrahydrobiopterin is an important cofactor in the biosynthesis of catecholamines and serotonin, and in the treatment of ASD, it is reported to significantly improve social interaction subscale of the CARS.[27]l-Carnosine is a dipeptide known for its antioxidant properties and proposed enhancement of γ-aminobutyric acid function in the brain, with possible anticonvulsive effects, it was showed to significantly improve CARS score on ASD children.[28] N-acetylcysteine (NAC) is an antioxidant with involvement in extracellular glutamate modulation, it seemed to be well-tolerated, and it might bring some benefits to ASD children for the associated symptom of irritability.[29] However, in treating ASD, some commonly used CAM treatments are reported ineffective, including methyl B12, oxytocin, ginkgo biloba, secretin, hyperbaric oxygen therapy, and chelation therapy.[30–38]
As a conclusion, CAM is widely used in the management of ASD, although evidences for their safety and efficacy are still in lack. We would like to conduct this SR and meta-analysis to further investigate CAM's clinical practice on ASD. However, there are some potential limitations of our study. First, differences of methodologic quality in the trials may cause significant heterogeneity. In addition, due to the limitations of language ability, we would only search literature in English and Chinese; this may lead to the potential risk of ignoring essential literature.
Author contributions
Biqin Shuai and Hongjiao Jin are co-first authors and contribute equally.
Conceptualization: Biqin Shuai, Yong Lin.
Data curation: Hongjiao Jin.
Formal analysis: Biqin Shuai.
Funding acquisition: Yong Lin.
Methodology: Yong Lin, Ning Zhao.
Project administration: Hongjiao Jin, Yong Lin.
Software: Renrong Duan.
Supervision: Yong Lin, Biqin Shuai
Validation: Zhu Li.
Visualization: Jiao Mao.
Writing – original draft: Biqin Shuai, Hongjiao Jin.
Writing – review & editing: Shenghua Liu, Mengyu Shi, Yan Luo.
Footnotes
Abbreviations: ABC = Autism Behavior Checklist, ASD = autism spectrum disorder, CAM = complementary and alternative medicine, CARS = Childhood Autism Rating Scale, CIs = confidence intervals, GRADE = Grading of Recommendations Assessment, Development, and Evaluation, MD = mean difference, PRISMA-P = preferred reporting items for systematic reviews and meta-analysis protocol, RR = relative risk, SMD = standardized mean difference, SR = systematic review.
How to cite this article: Shuai B, Jin H, Lin Y, Duan R, Zhao N, Li Z, Mao J, Luo Y, Shi M. Safety and efficacy of complementary and alternative medicine in the treatment of autism spectrum disorder: A protocol for systematic review and meta-analysis. Medicine. 2020;99:45(e23128).
BS and HJ are co-first authors.
The authors report no conflicts of interest.
Funding support: This study is supported by the National Natural Science Foundation (No.81760163).
All data generated or analyzed during this study are included in this published article [and its supplementary information files].
References
- [1].Myers SM, Johnson CP. American Academy of Pediatrics Council on Children With Disabilities. Management of children with autism spectrum disorders. Pediatrics 2007;120:1162–82. [DOI] [PubMed] [Google Scholar]
- [2].Fombonne E, Zakarian R, Bennett A, et al. Pervasive developmental disorders in Montreal, Quebec, Canada: prevalence and links with immunizations. Pediatrics 2006;118:e139–50. [DOI] [PubMed] [Google Scholar]
- [3].Dosreis S, Weiner CL, Johnson L, et al. Autism spectrum disorder screening and management practices among general pediatric providers. J Dev Behav Pediatr 2006;27:S88–94. [DOI] [PubMed] [Google Scholar]
- [4].(WHO) WHO. Autism spectrum disorders. Available at: http://www.who.int/mediacentre/factsheets/autism-spectrum-disorders/en/date last accessed). [Google Scholar]
- [5].Seltzer MM, Shattuck P, Abbeduto L, et al. Trajectory of development in adolescents and adults with autism. Ment Retard Dev Disabil Res Rev 2004;10:234–47. [DOI] [PubMed] [Google Scholar]
- [6].Howlin P, Goode S, Hutton J, et al. Adult outcome for children with autism. J Child Psychol Psychiatry 2004;45:212–29. [DOI] [PubMed] [Google Scholar]
- [7].Goel R, Hong JS, Findling RL, et al. An update on pharmacotherapy of autism spectrum disorder in children and adolescents. Int Rev Psychiatry 2018;30:78–95. [DOI] [PubMed] [Google Scholar]
- [8].Hofer J, Bachmann C, Kamp-Becker I, et al. Willingness to try and lifetime use of complementary and alternative medicine in children and adolescents with autism spectrum disorder in Germany: A survey of parents. Autism 2019;23:1865–70. [DOI] [PubMed] [Google Scholar]
- [9].Black LI, Clarke TC, Barnes PM, et al. Use of complementary health approaches among children aged 4-17 years in the United States: National Health Interview Survey, 2007-2012. Natl Health Stat Report 2015;78:1–9. [PMC free article] [PubMed] [Google Scholar]
- [10].DeFilippis M. The use of complementary alternative medicine in children and adolescents with autism spectrum disorder. PsychoPharmacology Bulletin 2018;48:40–63. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Smith CA, Parton C, King M, et al. Parents’ experiences of information-seeking and decision-making regarding complementary medicine for children with autism spectrum disorder: a qualitative study. BMC Complement Med Ther 2020;20:4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [12].Akins RS, Krakowiak P, Angkustsiri K, et al. Utilization patterns of conventional and complementary/alternative treatments in children with autism spectrum disorders and developmental disabilities in a population-based study. J Dev Behav Pediatr 2014;35:1–0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [13].Perrin JM, Coury DL, Hyman SL, et al. Complementary and alternative medicine use in a large pediatric autism sample. Pediatrics 2012;130: suppl 2: S77–82. [DOI] [PubMed] [Google Scholar]
- [14].Christon LM, Mackintosh VH, Myers BJ. Use of complementary and alternative medicine (CAM) treatments by parents of children with autism spectrum disorders. Research in Autism Spectrum Disorders 2010;4:249–59. [Google Scholar]
- [15].Shamseer L, Moher D, Clarke M, et al. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: elaboration and explanation. BMJ 2015;350:g7647. [DOI] [PubMed] [Google Scholar]
- [16].Cortesi F, Giannotti F, Sebastiani T, et al. Controlled-release melatonin, singly and combined with cognitive behavioural therapy, for persistent insomnia in children with autism spectrum disorders: a randomized placebo-controlled trial. J Sleep Res 2012;21:700–9. [DOI] [PubMed] [Google Scholar]
- [17].Wright B, Sims D, Smart S, et al. Melatonin versus placebo in children with autism spectrum conditions and severe sleep problems not amenable to behaviour management strategies: a randomised controlled crossover trial. J Autism Dev Disord 2011;41:175–84. [DOI] [PubMed] [Google Scholar]
- [18].Bent S, Hendren RL, Zandi T, et al. Internet-based, randomized, controlled trial of omega-3 fatty acids for hyperactivity in autism. J Am Acad Child Adolesc Psychiatry 2014;53:658–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Bent S, Bertoglio K, Ashwood P, et al. A pilot randomized controlled trial of omega-3 fatty acids for autism spectrum disorder. J Autism Dev Disord 2010;41:545–54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [20].Amminger GP, Berger GE, Schafer MR, et al. Omega-3 fatty acids supplementation in children with autism: a double-blind randomized, placebo-controlled pilot study. Biol Psychiatry 2007;61:551–3. [DOI] [PubMed] [Google Scholar]
- [21].Mankad D, Dupuis A, Smile S, et al. A randomized, placebo controlled trial of omega-3 fatty acids in the treatment of young children with autism. Mol Autism 2015;6:18. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [22].Feng J, Shan L, Du L, et al. Clinical improvement following vitamin D3 supplementation in Autism Spectrum Disorder. Nutr Neurosci 2017;20:284–90. [DOI] [PubMed] [Google Scholar]
- [23].Yau CH, Ip CL, Chau YY. The therapeutic effect of scalp acupuncture on natal autism and regressive autism. Chin Med 2018;13:30. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [24].Wong VC, Sun JG. Randomized controlled trial of acupuncture versus sham acupuncture in autism spectrum disorder. J Altern Complement Med 2010;16:545–53. [DOI] [PubMed] [Google Scholar]
- [25].Liu C, Li T, Wang Z, et al. Scalp acupuncture treatment for children's autism spectrum disorders: A systematic review and meta-analysis. Medicine (Baltimore) 2019;98:e14880. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [26].Lee B, Lee J, Cheon JH, et al. The Efficacy and Safety of Acupuncture for the Treatment of Children with Autism Spectrum Disorder: A Systematic Review and Meta-Analysis. Evid Based Complement Alternat Med 2018;2018:1057539. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [27].Danfors T, von Knorring AL, Hartvig P, et al. Tetrahydrobiopterin in the treatment of children with autistic disorder: a double-blind placebo-controlled crossover study. J Clin Psychopharmacol 2005;25:485–9. [DOI] [PubMed] [Google Scholar]
- [28].Chez MG, Buchanan CP, Aimonovitch MC, et al. Double-blind, placebo-controlled study of L-carnosine supplementation in children with autistic spectrum disorders. J Child Neurol 2002;17:833–7. [DOI] [PubMed] [Google Scholar]
- [29].Nikoo M, Radnia H, Farokhnia M, et al. N-acetylcysteine as an adjunctive therapy to risperidone for treatment of irritability in autism: a randomized, double-blind, placebo-controlled clinical trial of efficacy and safety. Clin Neuropharmacol 2015;38:11–7. [DOI] [PubMed] [Google Scholar]
- [30].Rossignol DA, Frye RE. A review of research trends in physiological abnormalities in autism spectrum disorders: immune dysregulation, inflammation, oxidative stress, mitochondrial dysfunction and environmental toxicant exposures. Mol Psychiatry 2012;17:389–401. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [31].Yatawara CJ, Einfeld SL, Hickie IB, et al. The effect of oxytocin nasal spray on social interaction deficits observed in young children with autism: a randomized clinical crossover trial. Mol Psychiatry 2016;21:1225–31. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [32].Hasanzadeh E, Mohammadi MR, Ghanizadeh A, et al. A double-blind placebo controlled trial of Ginkgo biloba added to risperidone in patients with autistic disorders. Child Psychiatry Hum Dev 2012;43:674–82. [DOI] [PubMed] [Google Scholar]
- [33].Williams K, Wray JA, Wheeler DM. Intravenous secretin for autism spectrum disorders (ASD). Cochrane Database Syst Rev 2012;CD003495. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [34].Sampanthavivat M, Singkhwa W, Chaiyakul T, et al. Hyperbaric oxygen in the treatment of childhood autism: a randomised controlled trial. Diving Hyperb Med 2012;42:128–33. [PubMed] [Google Scholar]
- [35].Rossignol DA, Rossignol LW, Smith S, et al. Hyperbaric treatment for children with autism: a multicenter, randomized, double-blind, controlled trial. BMC Pediatr 2009;9:21. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [36].Sakulchit T, Ladish C, Goldman RD. Hyperbaric oxygen therapy for children with autism spectrum disorder. Can Fam Physician 2017;63:446–8. [PMC free article] [PubMed] [Google Scholar]
- [37].Davis TN, O’Reilly M, Kang S, et al. Chelation treatment for autism spectrum disorders: a systematic review. Res Autism Spectr Disord 2012;7:49–55. [Google Scholar]
- [38].James S, Stevenson SW, Silove N, et al. Chelation for autism spectrum disorder (ASD). Cochrane Database Syst Rev 2015;CD010766. [DOI] [PubMed] [Google Scholar]