

Supplemental Digital Content is available in the text.
Abstract
Background:
Beauty standards vary by race and region, which must be accounted for in creating beauty. Chinese have unique features, including a depressed nose, flat midface, and small chin, and have different cosmetic concerns. We performed a consensus study on filler injections based on the Chinese standard of beauty due to a lack of such study.
Methods:
We organized the YVOIRE Consensus Group, including 5 plastic surgeons. We discussed common problematic areas seen in Chinese and described techniques based on our experience with hyaluronic acid fillers, while considering peer-reviewed articles, followed by multiple consensus-developing sessions.
Results:
Chinese faces are characterized by retruded forehead, chin, and low nasal bridge, with certain features believed to bring good fortune. Therefore, profiles of the forehead, nose, lip, and chin have substantial effects on attractiveness. The demand for cosmetic procedures is high among the young generation who particularly desire nose and chin augmentation. Attractive Chinese facial shapes are characterized by a long, slender facial shape and pointed chin. Lips are narrow and thick. When injecting fillers for Chinese, it is necessary to apply special methods that produce results consistent with these characteristics.
Conclusions:
Understanding the concept and demand of beauty depending on race and region is important. Patients should be evaluated before aesthetic procedures. Maintaining hygiene during the procedure is crucial. Moreover, methods for preventing pain are essential. Fillers should be injected into the correct anatomical site and layer to minimize side effects and maximize effectiveness.
INTRODUCTION
Facial aging is a complex phenomenon, characterized by the interplay of diverse factors involving 3-dimensional changes in the skeletal and soft tissue structures.1,2 Facial aging varies in terms of age of onset, severity, and specific concerns depending on ethnicity.3,4 Ethnicity-specific skin aging manifestations are genetically determined by the skin type and other genetic variations. For example, Caucasians have earlier-onset and greater skin wrinkling than other populations. Generally, increased pigmentary problems are seen in Asians.5,6 In Asians, the combination of increased superficial fat and thickened dermis lessens the incidence of superficial rhytides.7 Particularly in the Chinese population, wrinkle development follows a biphasic trend, with a slow increase until the age of 40–50 years, followed by a rapid increase thereafter.8 Despite the similarities in physiological processes and facial aging among all races, differences in skeletal structural support, and the sagging propensity of facial soft tissues retard aging in Asians more than in Caucasians.7,8
In most Asian patients, the dense fat and fibrous connections between the superficial muscular aponeurotic system and deep fascia, delay midfacial sagging.7 Overall, the Asian face retains its youthful appearance for a longer time than that of Caucasians.7–9 In an Asian face, a straight profile (normal or bimaxillary retrusion) was perceived as the most attractive feature for both genders by experts.10 Asian patients whose lower face height values approximated the ethnic “ideal” (54%) tended to rank higher for facial attractiveness.11
These findings strongly suggest that aesthetic physicians should also consider 3-dimensional anatomical and anthropometric characteristics depending on the patient’s ethnicity in facial rejuvenation procedures.12,13 Asians, including Chinese, have unique, natural features and different cosmetic concerns compared with Caucasians. This arises from differences in skin pathophysiology, mechanisms of aging, and unique facial structures between the 2 ethnicities.14 It is, therefore, important for the cosmetic industry to obtain a complete understanding of such differences. Due to the lack of a single standard of beauty, it is important to accommodate the diversity of beauty in individuals from different ethnic backgrounds. Of note, racial, cultural, and environmental factors are involved in the perception of beauty.15,16
Hyaluronic acid (HA) filler is a minimally invasive and efficient method to achieve a desired 3-dimensional facial appearance.17 Herein, we describe a treatment protocol for the anterior frontal face. The current consensus paper is about the filler – YVOIRE (LG Chem Ltd., Seoul, Republic of Korea). In the product manual, YVOIRE is characterized as having a maximal rate of cross-linking, minimal alteration in HA structure, and optimization of dispersion of the cross-linking agent among the highly concentrated HA polymers.18
YVOIRE is commercially available as multiple variants: YVOIRE classic S or classic plus for the correction of fine wrinkles and facial volumization, YVOIRE volume S or volume plus for the correction of deep wrinkles and facial volumization, and YVOIRE contour or contour plus for facial volumization and contouring (http://global.lgyvoire.com/).
The efficacy and safety of YVOIRE are well documented.19–23 Nevertheless, no study has evaluated the consensus on filler injections based on the Chinese standard of beauty; therefore, we aimed to deduce the prevailing general agreement.
METHODS
To discuss the best filler injection for the Chinese, we organized the YVOIRE Aesthetics Consensus Group comprising 1 surgeon from Korea and 4 from China (3 plastic surgeons, one maxillofacial surgeon, and one facial plastic surgeon), all of whom were experts in aesthetic facial treatments with fillers for 10 years. In the first meeting held in Seoul, Korea in May 2019, we discussed common problematic areas seen in both young and old Chinese patients and described techniques based on our experience with aesthetic facial treatments using HA fillers. After the first meeting, we held consensus-developing sessions via teleconferences and emails. The discussions were based on clinical experience and published literature with the search term filler + Asian/Caucasian + consensus/guidelines in PubMed. The recommendations, as they appear in this paper, were developed and evaluated based on the AGREE II domains.24 This article does not discuss any studies with human participants or animals by any of the authors.
RESULTS
Characteristics of the Chinese Face
Chinese are characterized by facial features, such as increased bizygomatic and bigonal width, retruded forehead, orbital rims, medial maxilla, pyriform margins, chin, and low nasal bridge with deficient anterior projection.25 The profiles of the forehead, nose, lip, and chin have substantial effects on the perceived attractiveness of the Chinese face.
In China, facial physiognomy and facial features are important in everyday life. It is strongly believed in Chinese populations that certain features of the face bring about luck or good fortune and vice versa.26,27 An attractive Chinese face is characterized by a long, narrow, and slender facial shape with a long philtrum, pointed and narrow chin, obtuse mandibular angle, straight facial profile, and to some extent, an anteriorly projecting chin and a concave or straight dorsum of the nose. Lips are narrow and thick, and the upper lip is relatively thick with well-defined Cupid’s bows with tapering volume toward the oral commissures.28,29 Interestingly in China, the demand for cosmetic procedures is high among the younger generation, with a strong desire for nose and chin augmentation. Their demands and expectations are different from those of the middle-aged and older individuals who require elimination of wrinkles or facial sagging.25
Treatment Protocol
For an objective assessment of the Chinese face, we divided the face into anterior frontal and posterior lateral parts. The anterior frontal part encompasses anatomical areas (Fig. 1). It plays a role in forming the facial profile. The posterior lateral part forms the lateral contour of the face. It encompasses the lateral forehead, temporal region, lateral cheek, and jaw line. The current treatment protocol was for the anterior frontal face.
Fig. 1.
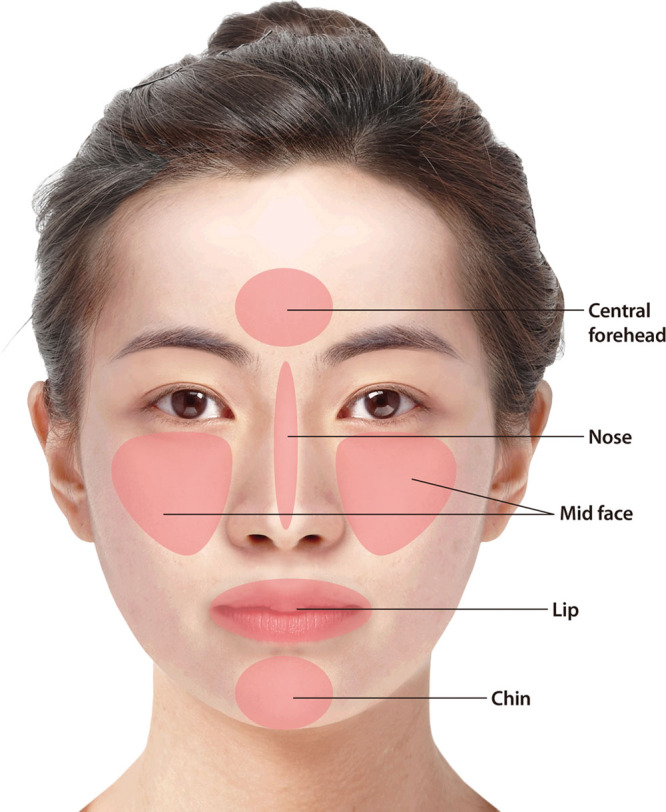
Image of a Chinese face, which is divided into the anterior frontal and posterior lateral face. The anterior frontal face encompasses anatomical areas such as the central forehead, nose, midface, lip, and chin.
There may be variations in the preoperative workup and injection techniques depending on institutions. We provided general considerations for injection techniques based on expert opinions below. This general injection protocol can be applied to all types of fillers. The injection technique is recommended for fillers with rheological characteristics similar to the YVOIRE filler.
(1) Pretreatment consultation: History-taking based on patient data (eg, age and sex), interviews for patient need determination, injection site and dose selection, pretreatment warnings, and obtaining informed consent is conducted.30,31
(2) Face washing and removal of make-up
(3) Pretreatment photograph (Fig. 2): Photographs of the basic frontal angle and oblique and lateral angles of both sides are needed. A picture taken from a special angle or expression depending on the patients’ condition may be required. For the before and after injection pictures, the lighting, background, and shooting angle should be the same.
Fig. 2.

Pre-treatment photographs of a Chinese woman.
(4) Pretreatment design using a marker: The area to be treated is marked, and for procedural ease, drawing of important anatomical structures, such as blood vessels and nerves or facial landmarks, such as a facial midline, is recommended.
(5) Preparations: Antiseptic solutions such as 83% isopropyl alcohol, povidone-iodine, chlorhexidine, and solutions containing hypochlorous acid should be applied to prepare the target area.32 Extensive disinfection of any contactable area on the operator’s hand, filler syringe, needle, and cannula, as well as the entry point of the needle or cannula is conducted. The procedure is usually performed in the semi-Fowler’s position (30–45 degrees); however, the angle can be adjusted according to the patient’s condition and the injection site.33
(6) Anesthesia: Topical lidocaine 2.5% and prilocaine 2.5% creams are commonly used for local anesthesia, and they should be applied at least for 40 minutes. The cream is generously applied to the target site to make the underlying skin invisible, followed by sealing with a vinyl wrap. The vinyl wrap is removed immediately before treatment, which is followed by rinsing of the topical anesthetic.34
A. Anesthesia in cases of cannula is use: Injection of local anesthetics at the site where a cannula is placed is useful for pain control.
B. Nerve block: A substantial amount of pain may be felt when the filler is injected. Thus, performing nerve blockade in the supraorbital, supratrochlear, infraorbital, and/or mental nerves may be beneficial.34
(7) Basic injection techniques: Depending on the target sites and preferences, the following techniques may be used alone or in combination (Fig. 3).
Fig. 3.

Illustration of basic injection techniques. A, Linear threading technique. B, Serial puncture threading technique. C, Cross-hatching technique. D, Fan technique. E, Bolus techniques.
A. Linear threading technique: After insertion of the total length of the needle in the tissue, it is slowly retracted. This is accompanied by the injection of the filler. Each injection site forms a single long line.
B. Serial puncture threading technique: A small amount of filler is injected in the form of tiny boluses by inserting the needle multiple times at constant intervals. Implants are almost connected to each other, forming a continuous line by a proper adjustment of the interval.
C. Fan technique: A needle is inserted adjacent to the target site. After injecting in a single line in a retrograde manner, the direction of the needle is changed while keeping the same point of entry, and the filler is re-injected in a retrograde manner along a new line. With the repetition of this maneuver, injections are performed in a fan-shaped manner, which is advantageous for minimizing needle marks and performing injections in a relatively larger area.
D. Cross-hatching technique: After injecting a single linear thread, the needle is completely removed from the skin. This is followed by the injection of multiple linear threads, first parallel to the first line and then perpendicular to the first set of lines. Using this method, injections are delivered to the target site at different levels, wherever appropriate.
E. Bolus techniques: In this technique the needle passes through the skin to a deeper structure, and then a certain amount of filler is injected keeping the needle as still as possible at the target layer. When more lifting is required with a small amount of filler, the bolus technique can be used.34–36
(8) Use of a needle or cannula: For the injection of the filler, both a sharp needle and a cannula can be used. In cases in which a sharp needle is used, there is a variation in the size and shape of the needle depending on characteristics of the filler. If possible, it is recommended to use the needle contained in the package.36,37
The advantages of using a needle are that injections can be easily performed, it is possible to inject a small amount of filler and to perform an intradermal injection. A lack of caution could cause the intravascular injection of filler. Recently, cannulas have been increasingly used for preventing complications such as the intravascular injection of filler. The use of a cannula is safe and less painful and causes less bruising, but it requires considerable expertise for filler injection. Moreover, the use of a cannula does not preclude intravascular filler embolization; therefore, a complete understanding of the facial anatomy is mandatory because a filler can be injected into the blood vessels while using a cannula.38,39
(9) Selection of products: A high G’ filler is used for sculpting, volumizing, or contouring of the face and it is injected in the supraperiosteal or deep subcutaneous layer. However, for superficial injections and for lip augmentation, a lower G’ filler is preferred.30
(10) Injection techniques depending on the target area: Types of fillers as well as injection techniques, volume, and sites are summarized in Table 1 and Figure 4.
Table 1.
Summary of Injections of a Filler Depending on the Target Site
| Area | Filler | Technique | Accessory | Volume | Target Layer |
|---|---|---|---|---|---|
| Central forehead | Lower G’ | Bolus | Needle cannula | 0.5 ml | Supra-periosteal layer |
| High G’ | |||||
| Nasal dorsum | High G’ | Linear threading, bolus | Needle cannula | 1 ml | Supra-periosteal layer, supra-perichondral layer |
| Nasal tip | High G’ | Bolus | Needle cannula | Interdomal area, 0.2 ml; nasal columella, 0.2 ml, anterior nasal spine, 0.5 ml | Interdomal area, subcutaneous layer, nasal columella. Subcutaneous layer (between the inferior nasal cartilage and medial angle), anterior nasal spine, supra-periosteal layer |
| Mid cheek | High G’ | Bolus | Needle cannula | Unilateral side of the mid cheek, 1 ml | Supra-periosteal layer |
| Lip | Lower G’ | Bolus, linear threading | Needle cannula | Each upper and lower lip, 0.25–0.5 ml | Submucosal, subcutaneous layer |
| Chin | High G’ | Bolus | Needle cannula | 1 ml | Supra-periosteal layer |
Fig. 4.
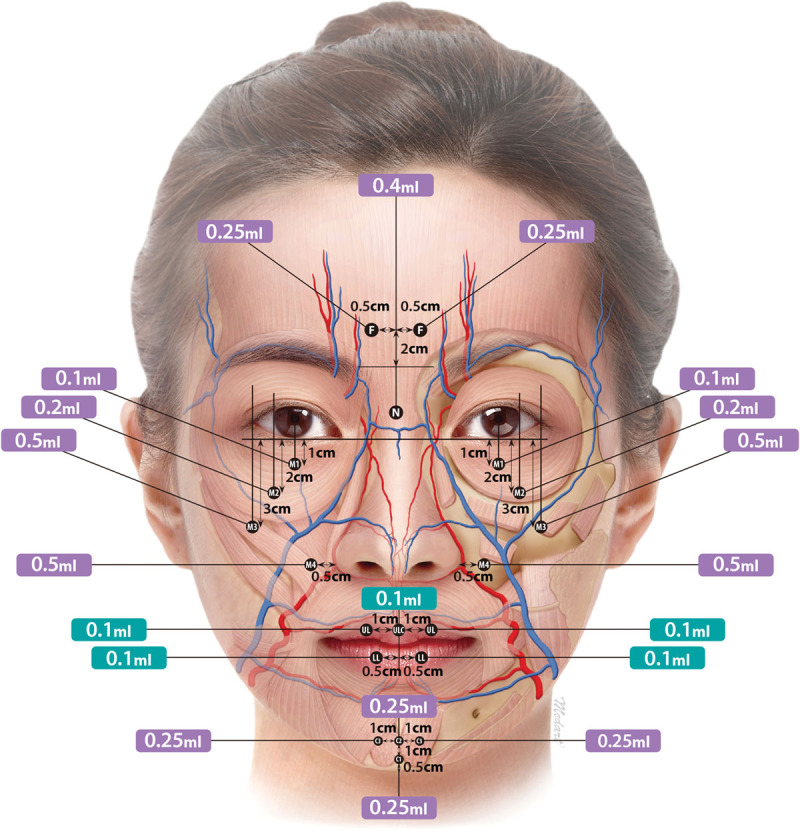
Summary of Injections of a filler depending on the target site. Note: Purple and green colors indicate the sites for which injections of higher and lower G’ filler are recommended, respectively.
A. Central forehead: Filler is injected into the deepest portions on the left and right side of the center of the forehead. In most cases, these injection points are located approximately 0.5 cm lateral to the center) on the horizontal line drawn 2 cm superior to the line connecting the inner end of each eyebrow. Approximately 0.25 ml of filler is injected into each point.40,41 Patients with a severely depressed forehead may receive an additional injection of fillers using a cannula.
B. Nose: (See Video 1 [online], which displays nasal bridge treatment procedures) (See Video 2 [online], which displays nasal dorsum and tip displays treatment procedures)
Video 1. Nasal bridge. Video 1 from “Expert consensus on hyaluronic acid filler facial injection for Chinese patients”.
Video 2. Nasal dorsum and tip. Video 2 from “Expert consensus on hyaluronic acid filler facial injection for Chinese patients”.
Nasal bridge: Fillers (volume, 0.3–0.5 ml) are injected, for which a needle is used for the supraperiosteal layer in the most depressed area on the midline between the eyes. A bolus injection is commonly performed. Moreover, a retrograde linear threading technique may also be used for the supraperiosteal or suprachondral layer, a cannula is used accordingly.42
Nasal tip: Fillers are injected to the point where the midline of the nasal columella meets the nostril tip. Target layers include the subcutaneous layer in the interdomal area of the nasal tip, the area between the medial crus of the lower nasal cartilage, and the supraperiosteal layer around the nasal spine. A bolus injection is commonly given. Injection doses include 0.2 ml for the nasal tip, 0.2 ml for the nasal columella, and 0.5 ml for the area adjacent to the anterior nasal spine.43
C. Midface: (See Video 3 [online], which displays mid face treatment procedures.
Video 3. Mid face. Video 3 from “Expert consensus on hyaluronic acid filler facial injection for Chinese patients”.
Filler (0.1 ml) is injected into the point (M1) 1 cm inferior to the orbital rim on the midpupillary line in the sub–orbicularis oculi fat pad in the pre-zygomatic space, and is an effective procedure to correct the tear trough.44
Filler (0.2 ml) is injected to the point (M2) 2 cm inferior to the orbital rim on a perpendicular line drawn from the lateral limbus in the upper part of the deep medial cheek fat. This is an essential procedure for patients who need augmentation of the apple of the cheeks, but it is not required for those with well-developed cheeks.45,46
Filler (0.5 ml) is injected into the point (M3) 3 cm inferior to the orbital rim on a perpendicular line drawn from the lateral canthus in the lateral part of the deep medial cheek fat. This is an essential procedure for patients who need the “apple muscle” and for middle-aged patients who need midface rejuvenation.47,48
Filler (0.5 ml) is injected into each of the left and right points (M4) 5 mm lateral to each alar base in the medial part of the deep medial cheek fat. This is an effective procedure for the correction of the nasolabial folds. Injections are administered in the most depressed-looking area on naked-eye observation. A needle is used, but a cannula may also be used. Cannula use requires an entry point on the vertical line on the lateral orbital rim.49
D. Chin: Filler (0.25 ml) is injected into the point (C1) 5 mm superior to the mandibular border on the facial midline and is a useful procedure for chin elongation. Filler (0.25 ml) is injected into the point (C2) 1 cm superior to C1 and is a useful procedure for chin projection. This injection is commonly given by inserting the needle at C1 and then advancing it upwards toward C2 and depositing the material at C2.
Filler (0.25 ml) is injected into the point (C3) 1 cm left and right from C2. This is a useful procedure for the volume augmentation of the chin. The injection is commonly given through upward displacement of the needle from C1.50
E. Lip (lower lip, upper lip, and center of the upper lip): Filler (total volume 0.1–0.2 ml) is injected into the layer underneath the dry mucosa that is located 5 mm left and right from the midline of the lower lip. Filler (total volume 0.1–0.2 ml) is injected into the layer underneath the dry mucosa that is located 1 cm left and right from the midline of the upper lip.
Filler (0.1 ml) is injected into the layer underneath the dry mucosa of the projected area in the center of the upper lip. Additionally, a total volume of 0.5 ml may also be applied for the augmentation of the entire lip.51 The needle is used for this procedure, but a cannula may also be used. Cannula use requires the formation of an entry point in the mouth corner.
(11) Post-treatment management: After injection of the filler, swelling, pain, erythema, and pruritus at the site of injection may occur, all of which normally appear and disappear within 1–2 days.52 If these symptoms persist or new symptoms appear, patients should immediately contact their physicians.53 After the injection of the filler in the lips, swelling may occur and persist for slightly longer periods of time.54 There is also a possibility that the lips might appear asymmetric. However, such swelling commonly disappears within 1–2 days. To obtain best treatment outcomes, patients should visit their physicians 1–2 weeks later. They should be evaluated regarding the need for a touch-up injection. However, patients cannot receive a touch-up injection until any swelling has resolved. If there is asymmetry after injection, it should be corrected within 7–10 days. Massage by the patients themselves should be avoided.55 The photographs before and after the procedure according to the above guidelines are shown in Supplemental Digital Content 1. (See figure, Supplemental Digital Content 1, which displays the illustrative cases. A, a: Before injection, b: after injection (injection area/product/injection volume: central forehead/YVOIRE volume plus/0.5 ml, nose/YVOIRE volume plus/0.3 ml, lip/YVOIRE classic plus/0.5 ml). B, a: Before injection, b: after injection (injection area/product/injection volume: central forehead/YVOIRE classic plus/0.5 ml, nose/YVOIRE volume plus/0.4 ml, chin/YVOIRE volume plus/1 ml). C, a: Before injection, b: after injection (injection area/product/injection volume: chin/YVOIRE volume plus/1 ml; http://links.lww.com/PRSGO/B498.) The procedure is shown in Video 1.
DISCUSSION
The concept of beauty notably varies by race and region. It is, therefore, mandatory to understand the concept and demand of beauty depending on the race and region, which is essential for performing a more complete procedure. Caucasians undergo filler treatment mainly to correct wrinkles and other facial changes caused by aging and to maintain a youthful appearance, as looking young and attractive is considered to be as important as maintaining good physical health.56 Consequently, early clinical trials and consensus papers on facial cosmetic procedures were mainly for patients older than 65 years of age.57 In contrast, Chinese people undergoing cosmetic procedures are relatively younger than white and receive fillers for volume correction for inborn features such as flat noses, depressed foreheads, depressed midfacial areas, and small chins rather than for the treatment of wrinkles. Nevertheless, middle-aged and older individuals still have requirements of wrinkles or facial sagging elimination.25 This is influenced by differences in views of beauty, anthropological facial skeletal structure, and face reading.58 From this viewpoint, patients should be evaluated before planning the procedure. Although the filler procedure is simple and safe, the treatment involves injection of foreign substances into the body. Special attention is, therefore, needed for disinfection and maintaining cleanliness during the procedure. Additionally, methods for preventing pain are also very essential. To date, many side effects have been reported in relation to filler procedures. To minimize these side effects, a grounded understanding of anatomy is essential, and this anatomical knowledge must be fully applied to the filler procedure. It is also important to determine whether a cannula or needle should be used to minimize side effects and achieve the best results. Various fillers have been introduced, and each filler has different characteristics; an understanding of the filler characteristics is important to prevent complications.
We believe that the filler injection points and the amount of filler injection recommended in this paper are very useful to achieve a beautiful face as per the standards in the Chinese population. However, clinical studies should be conducted in the future to investigate patient satisfaction and side effects according to this recommended injection method. This article has a limitation in that the number of invited experts was small in view of a large Chinese population. In the future, more experts should be invited to provide various opinions to achieve a consensus.
CONCLUSIONS
Understanding the concept and demand of beauty depending on race and region is important. Patients should be evaluated before aesthetic procedures. Maintaining hygiene and asepsis during the procedure is crucial. Moreover, methods for preventing pain are essential. Filler should be injected into the correct anatomical site and layered to minimize side effects and maximize effectiveness.
ACKNOWLEDGEMENT
This study was supported by the LG Chem Ltd.
Supplementary Material
Footnotes
Published online 28 October 2020.
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Related Digital Media are available in the full-text version of the article on www.PRSGlobalOpen.com.
REFERENCES
- 1.Wong CH, Mendelson B. Newer understanding of specific anatomic targets in the aging face as applied to injectables: aging changes in the craniofacial skeleton and facial ligaments. Plast Reconstr Surg. 2015;1365 suppl44S–48S. [DOI] [PubMed] [Google Scholar]
- 2.Kim SJ, Kim SJ, Park JS, et al. Analysis of age-related changes in Asian facial skeletons using 3D vector mathematics on picture archiving and communication system computed tomography. Yonsei Med J. 2015;56:1395–1400. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Vierkötter A, Krutmann J. Environmental influences on skin aging and ethnic-specific manifestations. Dermatoendocrinol. 2012;4:227–231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Giacomoni PU, Rein G. Factors of skin ageing share common mechanisms. Biogerontology. 2001;2:219–229. [DOI] [PubMed] [Google Scholar]
- 5.Alaluf S, Heath A, Carter N, et al. Variation in melanin content and composition in type V and VI photoexposed and photoprotected human skin: the dominant role of DHI. Pigment Cell Res. 2001;14:337–347. [DOI] [PubMed] [Google Scholar]
- 6.Nouveau-Richard S, Yang Z, Mac-Mary S, et al. Skin ageing: a comparison between Chinese and European populations. A pilot study. J Dermatol Sci. 2005;40:187–193. [DOI] [PubMed] [Google Scholar]
- 7.Sykes JM. Management of the aging face in the Asian patient. Facial Plast Surg Clin North Am. 2007;15:353–60, vi. [DOI] [PubMed] [Google Scholar]
- 8.Tsukahara K, Fujimura T, Yoshida Y, et al. Comparison of age-related changes in wrinkling and sagging of the skin in Caucasian females and in Japanese females. J Cosmet Sci. 2004;55:351–371. [PubMed] [Google Scholar]
- 9.Shirakabe Y, Suzuki Y, Lam SM. A new paradigm for the aging Asian face. Aesthetic Plast Surg. 2003;27:397–402. [DOI] [PubMed] [Google Scholar]
- 10.Soh J, Chew MT, Wong HB. A comparative assessment of the perception of Chinese facial profile esthetics. Am J Orthod Dentofacial Orthop. 2005;127:692–699. [DOI] [PubMed] [Google Scholar]
- 11.Oh HS, Korn EL, Zhang X, et al. Correlations between cephalometric and photographic measurements of facial attractiveness in Chinese and US patients after orthodontic treatment. Am J Orthod Dentofacial Orthop. 2009;136:762.e1–14; discussion 762. [DOI] [PubMed] [Google Scholar]
- 12.Farkas LG, Katic MJ, Forrest CR, et al. International anthropometric study of facial morphology in various ethnic groups/races. J Craniofac Surg. 2005;16:615–646. [DOI] [PubMed] [Google Scholar]
- 13.Oh SR, Priel A, Korn BS, et al. Applied anatomy for the aesthetic surgeon. Curr Opin Ophthalmol. 2010;21:404–410. [DOI] [PubMed] [Google Scholar]
- 14.Berardesca E, Maibach H. Racial differences in skin pathophysiology. J Am Acad Dermatol. 1996;34:667–672. [DOI] [PubMed] [Google Scholar]
- 15.Carter EL. Race vs ethnicity in dermatology. Arch Dermatol. 2003;139:539–540; author reply 540. [DOI] [PubMed] [Google Scholar]
- 16.Elgart ML. Defining skin of color. Cutis. 2003;71:142; author reply 142–143; discussion 143–145. [PubMed] [Google Scholar]
- 17.Klein AW, Elson ML. The history of substances for soft tissue augmentation. Dermatol Surg. 2000;26:1096–1105. [PubMed] [Google Scholar]
- 18.Moon HJ. What makes the difference of YVIORE®? HICE (high concentration equalized) cross-liking technology. Available at https://www.prime-journal.com/what-makes-the-difference-of-yvoire-hice-high-concentration-equalized-cross-linking-technology/. Accessed March 22, 2019.
- 19.Lee JH, Kim SH, Park ES. The efficacy and safety of HA IDF plus (with lidocaine) versus HA IDF (without lidocaine) in nasolabial folds injection: a randomized, multicenter, double-blind, split-face study. Aesthetic Plast Surg. 2017;41:422–428. [DOI] [PubMed] [Google Scholar]
- 20.Romeo F. Upper eyelid filling approach [U.E.F.A.] technique: state of the art after 500 consecutive patients. Aesthetic Plast Surg. 2019;43:663–672. [DOI] [PubMed] [Google Scholar]
- 21.Rho NK, Park JY, Youn CS, et al. Early changes in facial profile following structured filler rhinoplasty: an anthropometric analysis using a 3-dimensional imaging system. Dermatol Surg. 2017;43:255–263. [DOI] [PubMed] [Google Scholar]
- 22.Park KY, Kim JM, Seok J, et al. Comparative split-face study of durational changes in hyaluronic acid fillers for mid-face volume augmentation. Dermatol Ther. 2019;32:e12950. [DOI] [PubMed] [Google Scholar]
- 23.Huh CH, Eom Y, Yang SD, et al. A randomized, active-controlled, 52-week study of hyaluronic acid fillers for anteromedial malar region augmentation. Plast Reconstr Surg Glob Open. 2020;8:e2648. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Brouwers MC, Kho ME, Browman GP, et al. ; AGREE Next Steps Consortium. AGREE II: advancing guideline development, reporting and evaluation in health care. J Clin Epidemiol. 2010;63:1308–1311. [DOI] [PubMed] [Google Scholar]
- 25.Liew S, Wu WT, Chan HH, et al. Consensus on changing trends, attitudes, and concepts of Asian beauty. Aesthetic Plast Surg. 2016;40:193–201. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.McGrath C, Liu KS, Lam CW. Physiognomy and teeth: an ethnographic study among young and middle-aged Hong Kong adults. Br Dent J. 2002;192:522–525. [DOI] [PubMed] [Google Scholar]
- 27.Kim NH, Chung JH, Park RH, et al. The use of botulinum toxin type A in aesthetic mandibular contouring. Plast Reconstr Surg. 2005;115:919–930. [DOI] [PubMed] [Google Scholar]
- 28.Moon HJ. Scientific analysis of an average attractive Chinese face: the ‘YVOIRE’ face. https://www.prime-journal.com/scientific-analysis-of-an-average-attractive-chinese-face-the-yvoire-face/. Accessed December 10, 2019.
- 29.Samizadeh S, Wu W. Ideals of facial beauty amongst the Chinese population: results from a large national survey. Aesthetic Plast Surg. 2018;42:1540–1550. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Vedamurthy M, Vedamurthy A, Nischal K. Dermal fillers: do’s and dont’s. J Cutan Aesthet Surg. 2010;3:11–15. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.De Boulle K, Heydenrych I. Patient factors influencing dermal filler complications: prevention, assessment, and treatment. Clin Cosmet Investig Dermatol. 2015;8:205–214. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 32.Chapman I, Hsu JTS, Stankiewicz K, et al. Use of hypochlorous acid as a preoperative antiseptic before placement of dermal fillers: an alternative to the standard options. Dermatol Surg. 2018;44:597–599. [DOI] [PubMed] [Google Scholar]
- 33.Winkler AA. Injection facial fillers. https://emedicine.medscape.com/article/1574158-overview#a2. Accessed November 20, 2018.
- 34.Vedamurthy M, Vedamurthy A. Dermal fillers: tips to achieve successful outcomes. J Cutan Aesthet Surg. 2008;1:64–67. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Brandt FS, Cazzaniga A. Hyaluronic acid gel fillers in the management of facial aging. Clin Interv Aging. 2008;3:153–159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Vedamurthy M. Soft tissue augmentation—use of hyaluronic acid as dermal filler. Indian J Dermatol Venereol Leprol. 2004;70:383–387. [PubMed] [Google Scholar]
- 37.Rho NK, Chang YY, Chao YY, et al. Consensus recommendations for optimal augmentation of the Asian face with hyaluronic acid and calcium hydroxylapatite fillers. Plast Reconstr Surg. 2015;136:940–956. [DOI] [PubMed] [Google Scholar]
- 38.Wu K, Xie L, Wang M, et al. Comparison of the microstructures and properties of different microcannulas for hyaluronic acid injection. Plast Reconstr Surg. 2018;142:150e–159e. [DOI] [PubMed] [Google Scholar]
- 39.Tansatit T, Apinuntrum P, Phetudom T. A dark side of the cannula injections: how arterial wall perforations and emboli occur. Aesthetic Plast Surg. 2017;41:221–227. [DOI] [PubMed] [Google Scholar]
- 40.Cong LY, Phothong W, Lee SH, et al. Topographic analysis of the supratrochlear artery and the supraorbital artery: implication for improving the safety of forehead augmentation. Plast Reconstr Surg. 2017;139:620e–627e. [DOI] [PubMed] [Google Scholar]
- 41.Sykes JM, Cotofana S, Trevidic P, et al. Upper face: clinical anatomy and regional approaches with injectable fillers. Plast Reconstr Surg. 2015;136(5 suppl):204S–218S. [DOI] [PubMed] [Google Scholar]
- 42.Tansatit T, Moon HJ, Rungsawang C, et al. Safe planes for injection rhinoplasty: a histological analysis of midline longitudinal sections of the Asian nose. Aesthetic Plast Surg. 2016;40:236–244. [DOI] [PubMed] [Google Scholar]
- 43.Moon HJ. Injection rhinoplasty using filler. Facial Plast Surg Clin North Am. 2018;26:323–330. [DOI] [PubMed] [Google Scholar]
- 44.Carruthers J, Rzany B, Sattler G, et al. Anatomic guidelines for augmentation of the cheek and infraorbital hollow. Dermatol Surg. 2012;387 pt 21223–1233. [DOI] [PubMed] [Google Scholar]
- 45.Li D, Wang X, Wu Y, et al. A randomized, controlled, multicenter study of Juvéderm Voluma for enhancement of malar volume in Chinese subjects. Plast Reconstr Surg. 2017;139:1250e–1259e. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Rohrich RJ, Pessa JE, Ristow B. The youthful cheek and the deep medial fat compartment. Plast Reconstr Surg. 2008;121:2107–2112. [DOI] [PubMed] [Google Scholar]
- 47.Stern CS, Schreiber JE, Surek CC, et al. Three-dimensional topographic surface changes in response to compartmental volumization of the medial cheek: defining a malar augmentation zone. Plast Reconstr Surg. 2016;137:1401–1408. [DOI] [PubMed] [Google Scholar]
- 48.Wang W, Xie Y, Huang RL, et al. Facial contouring by targeted restoration of facial fat compartment volume: the midface. Plast Reconstr Surg. 2017;139:563–572. [DOI] [PubMed] [Google Scholar]
- 49.Surek CC, Beut J, Stephens R, et al. Pertinent anatomy and analysis for midface volumizing procedures. Plast Reconstr Surg. 2015;135:818e–829e. [DOI] [PubMed] [Google Scholar]
- 50.Tansatit T, Phumyoo T, Jitaree B, et al. Investigation of the presence and variation of the ascending mental artery: conventional dissections and ultrasonographic study. J Cosmet Dermatol. 2019;18:1821–1829. [DOI] [PubMed] [Google Scholar]
- 51.Tansatit T, Apinuntrum P, Phetudom T. Cadaveric assessment of lip injections: locating the serious threats. Aesthetic Plast Surg. 2017;41:430–440. [DOI] [PubMed] [Google Scholar]
- 52.Ozturk CN, Li Y, Tung R, et al. Complications following injection of soft-tissue fillers. Aesthet Surg J. 2013;33:862–877. [DOI] [PubMed] [Google Scholar]
- 53.Cohen JL. Understanding, avoiding, and managing dermal filler complications. Dermatol Surg. 2008;34(suppl 1):S92–S99. [DOI] [PubMed] [Google Scholar]
- 54.Stojanovič L, Majdič N. Effectiveness and safety of hyaluronic acid fillers used to enhance overall lip fullness: a systematic review of clinical studies. J Cosmet Dermatol. 2019;18:436–443. [DOI] [PubMed] [Google Scholar]
- 55.Sclafani AP, Fagien S. Treatment of injectable soft tissue filler complications. Dermatol Surg. 2009;35(suppl 2):1672–1680. [DOI] [PubMed] [Google Scholar]
- 56.Maisel A, Waldman A, Furlan K, et al. Self-reported patient motivations for seeking cosmetic procedures. JAMA Dermatol. 2018;154:1167–1174. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 57.Sundaram H, Liew S, Signorini M, et al. ; Global Aesthetics Consensus Group. Global aesthetics consensus: hyaluronic acid fillers and botulinum toxin type A-recommendations for combined treatment and optimizing outcomes in diverse patient populations. Plast Reconstr Surg. 2016;137:1410–1423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58.Chao YYY, Chhabra C, Corduff N, et al. PAN-ASIAN CONSENSUS—key recommendations for adapting the World Congress of Dermatology Consensus on combination treatment with injectable fillers, toxins, and ultrasound devices in Asian Patients. J Clin Aesthet Dermatol. 2017;10:16–27. [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.