

Abstract
Background:
There is currently no universally adopted terminology for defining human surface anatomical location. The lack of precision, accuracy and reliability of terms used by healthcare providers, in particular dermatologic surgeons, is unsatisfactory both for epidemiological research and for high quality patient care.
Objective:
To create a clinically relevant yet concise surface anatomy terminology for international use including the International Classification of Diseases and to map it to existing disparate terminologies.
Methods:
Widely used surface anatomy terminology data sets and diagrams were reviewed. A Delphi consensus convened to create a novel surface anatomy terminology. The new terminology was hierarchically mapped to SNOMED terms and NYU Numbers and physically mapped to 2D anatomical diagrams for clarity and reproducibility.
Results:
The final terminology data set contains 512 discrete terms arranged in a 9 level hierarchy and has been adopted by the World Health Organization for ICD-11.
Limitations:
Terms lack laterality and fine granularity for large sites.
Conclusion:
Consistent use of precise and accurate surface anatomy terms is crucial to the practice of dermatology, particularly procedural dermatology. The proposed terminology is designed to form the basis for evolution of a universally adoptable terminology set to improve patient care, interprovider communication and epidemiological tracking.
Keywords: surface topography, dermatology, surface anatomy, anatomical nomenclature
Graphical Abstract
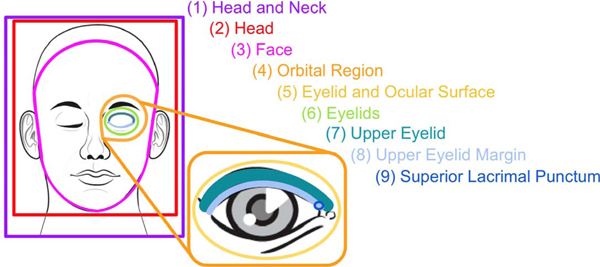
Figure 1. Demonstration of the hierarchical nature of the term set for the face with nine hierarchical levels beginning with Head and Neck and terminating in Superior Lacrimal Punctum. See Table II for corresponding term synonyms and crosslinking to SNOMED terms and NYU Numbers.
Introduction
There is currently no internationally accepted set of anatomical terms for use by dermatologists and other health care providers to enable recording of surface anatomy locations on the human body accurately and consistently. This lack of consensus results in errors of accuracy and precision that have clinical and research consequences. Clinically, inconsistent anatomic site terminology can lead to unnecessary biopsies, mistaken clinical/pathologic correlation, and wrong site surgery. These risks grow with the number of providers involved in the care of the patient, the number of biopsies/treatments the patient has had, and the length of follow up. For research purposes, detailed and consistent application of surface anatomy terminology provides a key stratification variable for epidemiology research, quality monitoring, recurrence monitoring, and study of the natural history of cutaneous processes. While digital photography is becoming ubiquitous and presents many advantages for anatomic site documentation, photo-documentation is currently not the norm and the consequences of inconsistent text-based terminology are magnified in the era of electronic medical records and ‘big data’ analyses.
Even if a consistent set of widely accepted terms were available, rising clinical volumes and increasing regulatory and reimbursement demands for documentation contribute to time pressure for clinicians that can undermine the precision and granularity of anatomic labeling. Lengthy free-text descriptions of precise anatomic labels are both inefficient and prone to errors. As a result, an exhaustive and precise set of anatomical terms would be best applied through automated linkage to anatomic drawings or clinical photographs.
Here we provide a synopsis and comparison of the major extant systems for anatomic labeling along with a proposed system that automatically links a consensus set of terms derived from these systems to a set of anatomic drawings.
Current terminology systems
There are currently a number of readily available surface anatomy maps and term sets, but each has weaknesses for routine application in dermatology practice and research.
The web-based terminology database SNOMED CT (Systematized Nomenclature of Medicine - Clinical Terms) is a detailed and extensive clinical terminology including but not limited to anatomic, pathologic, procedural, event, and demographic terms. It is owned, maintained, and distributed by the International Health Terminology Standards Development Organisation (IHTSDO).1 SNOMED CT was originally created by the College of American Pathologists and now contains over 320,000 concepts, each with its own SCTID (SNOMED CT Identifier) code. Its weakness, however, lies in its incomplete coverage of detailed surface anatomy, and the large number of options with many overlapping terms for the same location, each with its own SCTID code. Thus, two lesions occurring in exactly the same location could be coded and later analyzed differently. For example, nape of the neck correlates to “Entire posterior portion of neck”, “Entire skin of nuchal region”, “Entire surface region of back of neck” and “Structure of surface region of back of neck”.
The Foundational Model of Anatomy ontology (FMA), created by the Structural Informatics Group at the University of Washington, is a system of internal and surface anatomy which is entirely online.2 It was aligned with SNOMED-CT and Galen and adopted by the European Committee for Standardization. Its design is purely ontological (i.e. a conceptual model) with text labels (and associated FMA ID numbers) without a coordinated graphic location, requiring the user to have a fairly detailed anatomical knowledge. Although the system is multi-axial, it is no longer possible to view the full hierarchy satisfactorily since the withdrawal of the Foundational Model Explorer (FME), which previously enabled the hierarchy to be visualized in its entirely through a series of drop-down options. Despite these issues, it is a thorough system and includes laterality.
The third edition of the World Health Organization’s International Classification of Diseases for Oncology (ICD-O-3) is another web-based terminology set with associated codes which has historically been used by tumor and cancer registries.3 It utilizes a dual classification scheme consisting of a morphologic code and a topographic code. Only the morphology component was incorporated into SNOMED. The topography component was derived from the Neoplasms chapter of ICD-10. While the pairing of diagnosis and location, and the integration with other systems is desirable, ICD-O is geared more towards internal malignancies rather than disorders of the skin and the terms and corresponding topography codes are far too broad for finer epidemiological tracking and analysis for dermatologic conditions, for which less than ten locations are available (e.g “skin of trunk” and “skin of upper limb and shoulder”).
Each of these terminologies has its own weaknesses, with most systems being too specific, not specific enough, or too inclusive. While the United States has only recently transitioned to ICD-10, many countries have been using ICD-10 for well over a decade and are now making preparations for the recently released eleventh revision (ICD-11). ICD-11 will enable disorders to be linked to precise anatomical locations including laterality and surface topography, a provisional new classification of which was drawn up and agreed by members of the ICD-11 Dermatology Topic Advisory Group and co-opted experts at an international workshop held in Manchester, UK, in January 2014. This ad hoc Dermatology Anatomy Terminology Working Group was informed by existing classifications from the British Association of Dermatologists and the US Anatomy Mapper project.3 An important issue considered at the workshop was the appropriate granularity to be incorporated, with recognition that creating a system that is too finely granular may inhibit adoption. The Group was able to achieve consensus (Table 1). The proposed surface topography classification (ICD-ST) has been accepted by WHO for incorporation into ICD-11 (ICD-ST). It has subsequently been agreed at the International Skin Imaging Collaboration (ISIC) meeting held in 2017 in New York City, USA, that ICD-ST should be used as the foundation for a Delphi Consensus study on classification of surface topography. ICD-ST represents a strong starting point for a future internationally standardized surface anatomy terminology.
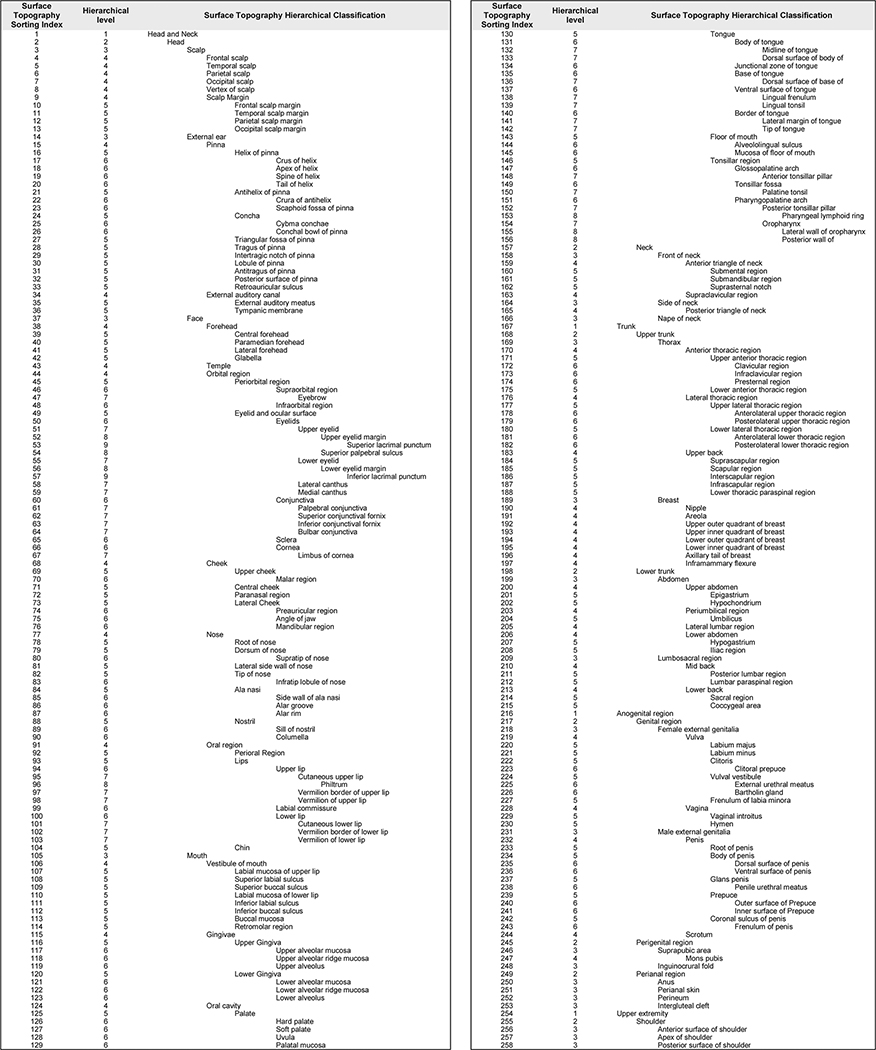
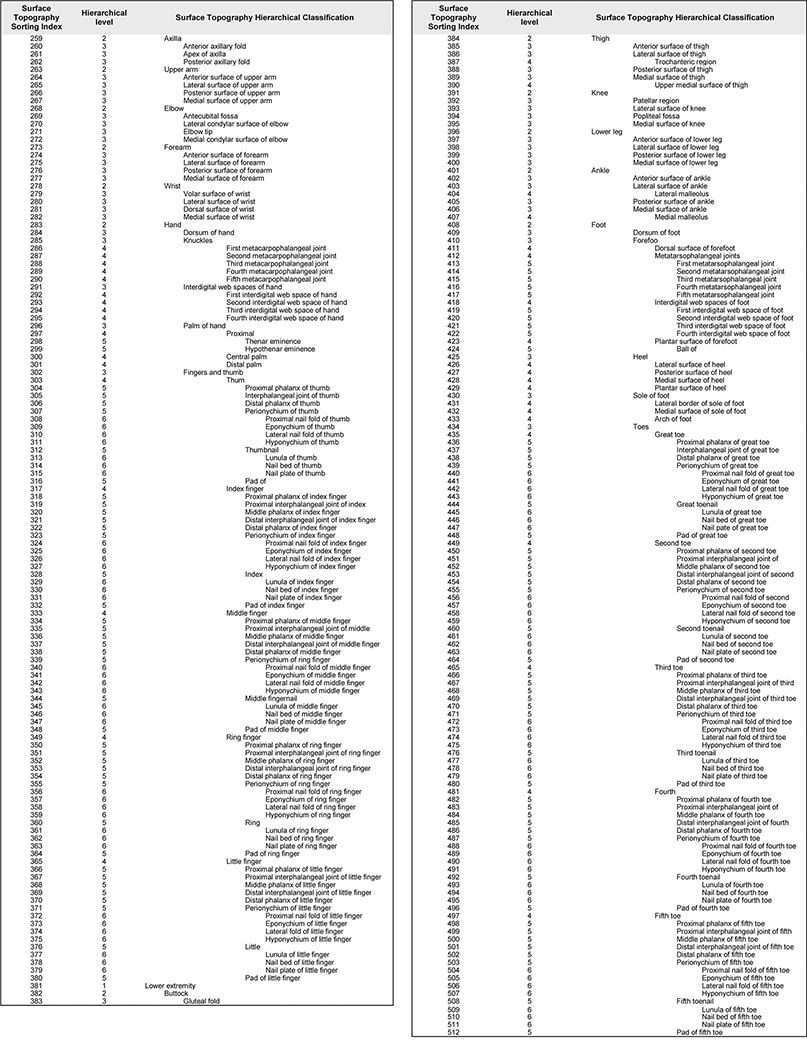
Table I.
Proposed Hierarchy of 512 Surface Topography Terms
 |
 |
To further expand our ICD-ST proposal, we are recommending adoption of the system of post-coordination built into ICD-11, which enables a set of “extensions” including location to be appended to stem concepts. Extensions allow for more specific data to be captured without an explosion in the number of codes required to achieve this, thus promising higher accuracy and precision than is currently available. The hierarchical nature of the proposed system with the facility to qualify enables different levels of anatomic detail to be recorded appropriately, ranging from large areas, for example “Head and Neck”, all the way down to the smallest areas, e,g, “Perionyhcium of the left fifth toe”. Extensions to surface topography terms such as laterality, directional additions, histologic subtype, and Boolean values can transform “squamous cell carcinoma of nose” to “recurrent, previously irradiated, invasive squamous cell carcinoma of the left posterosuperior lateral sidewall of nose,” for example.
Anatomy Mapping
The need for standardized anatomical terms is clear, but accurate use of terms is partly dependent on the user, as knowledge of anatomy is required, particularly in areas with non-discrete borders. A potential solution to this issue is computerized anatomic mapping. With visual maps, an accurate term can be easily generated with a single click. With the increasing sophistication of computer graphics and their incorporation into electronic health record systems via computers, tablets, smartphones, smart cameras enabled with DICOM (Digital Imaging COmmunication in Medicine) functionality or other means, there is opportunity for increasingly precise, accurate and thorough documentation, which may become a requirement for full reimbursement in the future in many countries. With a potential shift to value-based payments, it is important that dermatologists thoroughly document the treatments they perform in order to illustrate the value and extent of the services they provide in a given encounter, a focus of the American Academy of Dermatology’s DataDerm initiative.5 An appropriately designed user interface with standardized clickable body surface graphics incorporated into the electronic health record will enable this to be done in an accurate and reliable manner. In very busy practices or when technical difficulties such as a crashed server occur, historical, established maps or the maps presented on anatomymapper.com can be printed and sites manually marked by providers for later documentation by medical assistants. In addition to being fast and easy, maps may serve as an educational tool to assist staff and medical trainees learn terminology themselves.
An anatomic numbering system (hereby referred to as “NYU Numbers”) was created under the direction of Dr. Alfred W. Kopf for The New York University Melanoma Cooperative Group in 1972 and has been used at a number of well-respected institutions throughout the years including New York University, Memorial Sloan Kettering Cancer Center, Cleveland Clinic and Mayo Clinic.6 The NYU Numbers have distinctly bordered surface regions labeled with numbers rather than text-based terms. This map has sometimes arbitrary borders on areas such as the scalp, which has a single defined area that most would regard as including both the parietal and occipital scalp regions. Furthermore, the NYU Numbers do not have a standardized or widely used legend correlating the numbers with anatomic topography terms and thus it does not assist in the generation of descriptive anatomical terms for documentation.
Anatomy Mapper™ is an easy-to-use web-based interactive map, created by one of the authors, which displays a precise anatomic term on hovering over a specific body location, enabling its text descriptor to be exported with a mouse click.7 There are many advantages to this type of system which pairs terms with a map: these include increased accuracy, increased efficiency and improved inter-operator agreement. While this system efficiently generates text-based documentation, it does not yet have a publicly available image markup facility.
Finally, there are commercial dermatology-specific EHR systems with and without maps that enable fast, accurate documentation. Some systems function in 2D while others provide 3D maps for notation of lesions. While 3D maps facilitate precise documentation of lesions on curved body areas, increased time in mouse clicks and model rotations causes decreased overall efficiency. While 2D maps can be printed and notated in times of technology failure or to increase the speed of documentation, the same cannot be said for 3D maps. Therefore, while there are obvious advantages to 3D models they are not without their drawbacks. There are clear advantages to the even more advanced systems that incorporate photo documentation superimposed on a map or assist in coding of location and/or diagnosis. All of these dermatology-specific systems are, however, generally very expensive and unlikely to be accessible to primary care physicians, non-dermatologists or physician extenders, all of whom are performing more and more dermatologic evaluations and biopsies. Additionally, the need for a publicly available standardized terminology set that can be adopted by the international community is not being met by these proprietary systems.
DICOM began as a radiology initiative in 1993 to establish standards for formatting, storage, printing and secure transmission of medical images and has since crossed over into a number of specialties including dermatology.8,9 Photographs encoded as DICOM images that can be uploaded to PACS are becoming increasingly common, especially since the advent of DICOM cameras and smartphone applications. While these photographs are immensely useful for tracking lesions over time and sharing among providers, the “Body Part Examined” DICOM terminology set used to identify the photographed lesion location is very weak, consisting of only 25 location terms, with a laterality notation.9 With such a minimal number of surface topography terms available, when photographs are taken close-up it may be difficult to discern the true location of the lesion(s) imaged, particularly if only close-up views are available. Thus, even the gold standard in medical photography has significant room for improvement.
Although we do not claim that we have presented an exhaustive list of available maps and/or topographic term lexicons, we have attempted to illustrate the advantages and pitfalls of each and to propose a system which avoids the dangers we have highlighted by combining standardized terms with detailed anatomic surface maps.
While standardized anatomic maps are promising tools, they should be considered an adjunct to, rather than a replacement for photo-documentation. Photographs are the best way to record the precise location of a lesion in a given individual and are especially important for those occurring at the borders of anatomic regions (e.g., posterior shoulder v. back) where no clear boundaries exist.
Proposal for a Hierarchical Terminology System Cross-linking ICD Topography to SNOMED CT and NYU Numbers
In this paper we have described a new detailed surface anatomy terminology classification which will be a component part of the recently released ICD-11. Terms have been arranged in a hierarchical format for ease of use with 9 levels of granularity. There exist 5 level 1 terms, 20 level 2 terms, 68 level 3 terms, 79 level 4 terms, 170 level 5 terms, 134 level 6 terms, 27 level 7 terms, 7 level 8 terms, and 2 level 9 terms (Table I). Approximately 2000 SNOMED terms with SCTID codes and 310 NYU Numbers were then cross-linked back to the 512 standardized terms. A representation of the heirarchical format of the terms is demonstrated in the graphical abstract and corresponding Table II showing linkage to SNOMED and NYU Numbers. In correlating anatomic locations across systems, a larger standardized data pool is created for retrospective analysis and prospective tracking of topographic data from NYU Numbers and SNOMED. Though not a part of the original 512 terms, we propose the addition of 32 optional qualifiers, such as “posterolateral”, “superomedial”, etc., for optional further subdivision of larger areas. These qualifiers were in some cases included in SNOMED terms but never in NYU Numbers. Our cross-linking of SNOMED/SCTID and NYU Numbers can be accessed online at http://anatomymapper.com/terms.10 Two very important sites for dermatologic oncology are the ear and nose, which are poorly represented in existing classifications. Examples of the granularity of the proposed terminology set crosslinked to SNOMED/SCTID and NYU Numbers for the ear and nose can be seen in Tables III and IV.
Table II.
Demonstrating the hierarchical terminology structure depicted in the graphical abstract with correlated SNOMED terms and associated SCTIDs and NYU numbers. TMTL= too many to list where a single number is not available and aggregate numbers for entire region are too numerous. No matches = no available NYU Number corresponding to the new term.
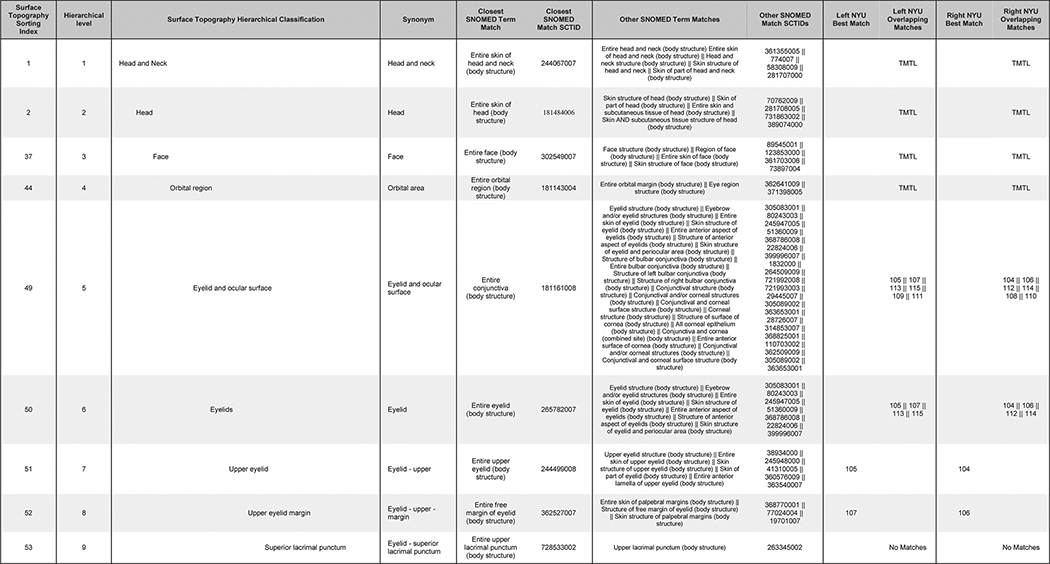 |
Table III.
Example of proposed hierarch with correlated SNOMED terms with associated SCTIDs and NYU numbers for the ear. TMTL= too many to list where a single number is not available and aggregate numbers for entire region are too numerous. No matches = no available NYU Number corresponding to the new term.
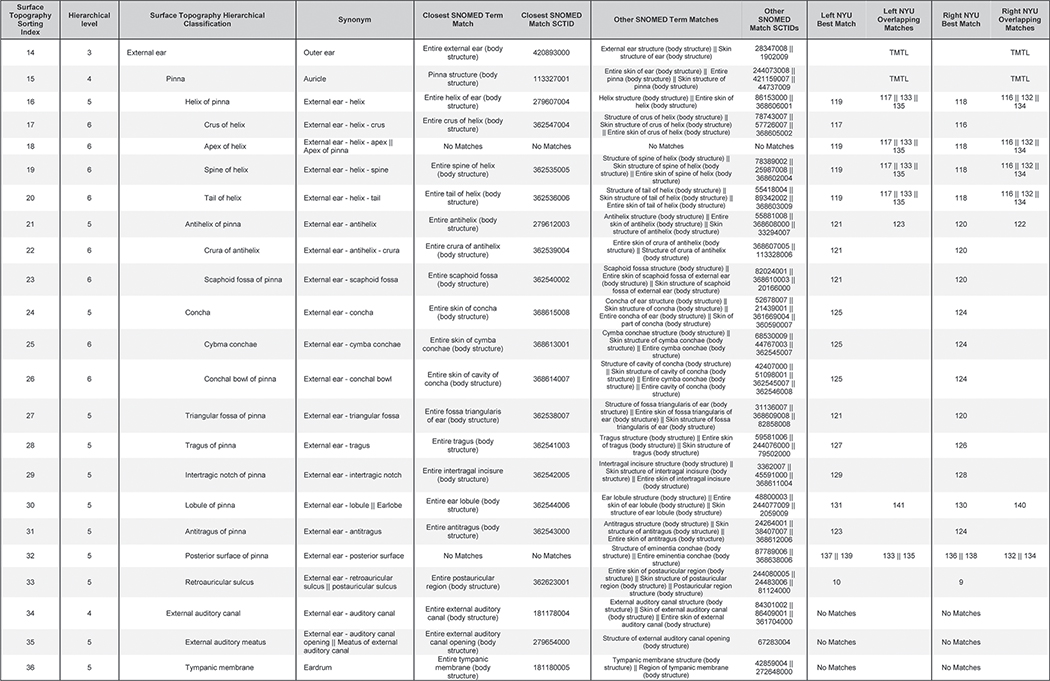 |
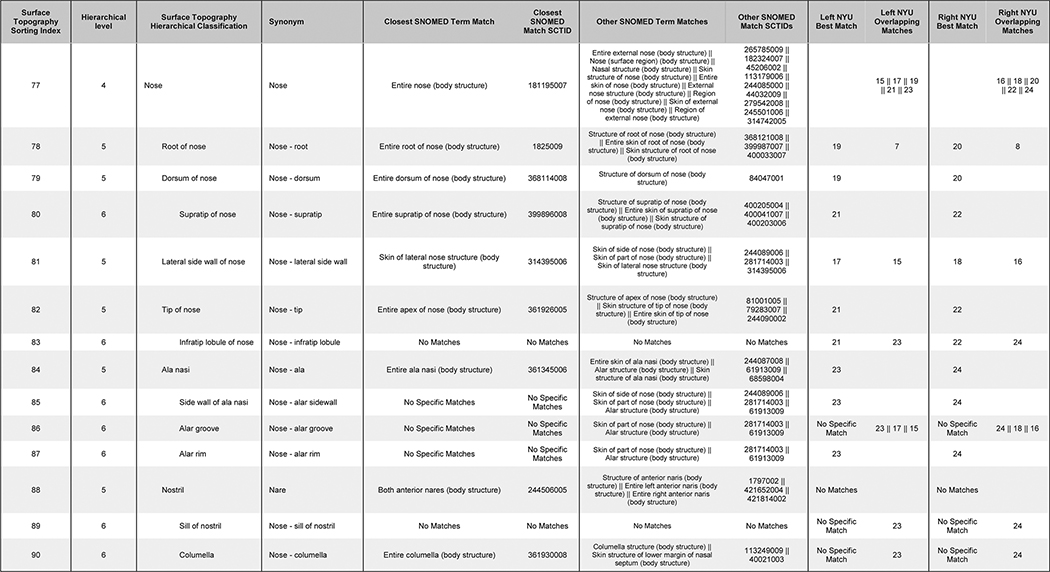
Table IV.
Example of proposed hierarchy with correlated SNOMED terms with associated SCTIDs and NYU numbers for the nose. TMTL= too many to list where a single NYU Number is not available and aggregate numbers for entire region are too numerous. No matches = no available NYU Number corresponding to the new term.
 |
To complement our cross-mapping and for historical reference, we have generated an interactive NYU Numbers map with the most precise anatomical terms possible linked to each of the numbered and bordered regions, which can be accessed at http://anatomymapper.com/nyu.10 Also included on this site are the best match anatomical descriptors for all NYU Numbers: as previously noted, not all NYU Numbers have clearly defined or anatomically correct borders. Terms were generated to best describe the NYU Number regions and thus they are not identical to the proposed 512 proposed terms.
Conclusion
The need for a standardized, widely utilized surface anatomy terminology is evident. None of the currently available terminologies is ideally suited for universal adoption. In creating a more complete, precise, yet concise set of surface anatomy terms, we have sought to create a language to facilitate improved inter-provider communication, generation of a rich dataset which may be used for clinical and epidemiological research, quality monitoring, recurrence monitoring and to assure correct treatment site. The proposed terminology set of 512 non-lateralized terms incorporates the strengths of existing systems while avoiding excessive granularity, a factor which could inhibit adoption. We recognize that this proposed set of terms will require further validation and consensus building to achieve universal adoption. We further anticipate that more granularity, including lateralization, will be added as electronic documentation becomes ubiquitous, making such granularity broadly practical.
The fact that ICD-ST has been accepted by the World Health Organization and is incorporated into the recently released Eleventh Revision of The International Classification of Diseases (ICD-11) should prove a spur to its wider adoption by clinicians. Furthermore, by crosslinking the NYU Numbers map and SNOMED-CT terms to our terminology, we hope to facilitate the transition to ICD-ST for institutions using NYU Numbers and SNOMED-CT-based systems. Finally, the proposed terminology set is freely available for open access online in the public domain in the hopes of promoting adoption and providing a foundation for the generation of increasingly practical systems of accurate, consistent, and precise anatomic labeling.
Capsule summary.
There is no standardized universal surface topography term set available.
We propose a hierarchically arranged set of 512 surface anatomy terms as an initial step toward international adoption.
It is vital that anatomic sites in dermatology are precise and accurate for correct site treatment, epidemiological tracking and interprovider communication
Acknowledgments
The research presented in this manuscript has not previously been published or presented.
Funding is provided by the P30 Cancer Center Support Grant (CCSG) (P30 CA008748).
Footnotes
Conflict of Interest:
Matthew Molenda is the developer and owner of Anatomymapper.com referenced in this manuscript.
Peter Soyer is a Shareholder and Consultant for e-derm GmbH, a Shareholder and Consultant for MoleMap by Dermatologists Pty Ltd. and a Consultant for Canfield Scientific.
Allan Halpern is an Advisory Board Member for Syneos Health.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- 1.The IHTSDO SNOMED CT Browser. The International Health Terminology Standards Development Organisation. http://browser.ihtsdotools.org. Published 2015. Accessed November 2017.
- 2.FMA browser. Structural Informatics Group at the University of Washington. http://xiphoid.biostr.washington.edu/fma/fmabrowser-hierarchy.html. Published 2008. Accessed February 2, 2018.
- 3.World Health Organization, International Agency for Research on Cancer. International Classification of Diseases for Oncology ICD-O-3 online. http://codes.iarc.fr. Published September 2011. Updated 2013. Accessed February 2, 2018.
- 4.Chalmers RJG, Molenda M, Soyer HP, Weichenthal M. Surface Topography Workshop Manchester January 2014, University of Manchester, Manchester, UK: January 13–16, 2014. [Google Scholar]
- 5.About DataDerm. https://www.aad.org/practicecenter/quality/dataderm/about-dataderm. Published 2016. Accessed February 3, 2018.
- 6.Kopf A. NYU Numbers. New York City, New York: The New York University Melanoma Cooperative Group; 1972. [Google Scholar]
- 7.Molenda M, Palmer M, Sachdeva K, Kenneweg K. Human Surface Anatomy Labeling System. http://www.anatomymapper.com. Published August 1, 2015. Accessed February 2, 2018.
- 8.Gueld MO, Kohnen M, Keysers D et al. Quality of DICOM header information for image categorization Medical Imaging 2002: PACS and Integrated Medical Information Systems: Design and Evaluation; 2002: 4685. [Google Scholar]
- 9.Pianykh OS. Digital imaging and communication in medicine (DICOM): A practical introduction and survival guide. (2nd ed.). Berlin: Springer; 2012. [Google Scholar]
- 10.Molenda M, Kenneweg K. Online NYU Labeling System. http://www.anatomymapper.com/nyu/# Published March 2016. Updated 2017. Accessed February 2, 2018