

Abstract
Background
Prior studies report anomalous cause of death patterns for adults with Down syndrome, but do not provide comparison of age trends for specific causes of death between adults with and without Down syndrome, or explore biological sex and racial-ethnic differences in causes of death among adults with Down syndrome.
Objective
To better understand cause of death trends for adults, age 18 and over, with Down syndrome.
Methods
Cross-sectional data were from the 2013–2017 US Multiple Cause of Death Mortality files. Adjusted odds ratios were utilized to compare cause of death trends overall, and by age, between adults with (N=9,870) and without (N=13,323,001) Down syndrome. We also analyzed biological sex and race-ethnic differences in cause of death solely among adults with Down syndrome.
Results
Although heart disease, dementia and Alzheimer’s disease, and cancer were common among adults all adults, death from these diseases was more prominent at younger ages for adults with Down syndrome. Adults with Down syndrome were also more likely to die from influenza and pneumonia, pneumonitis, respiratory failure, and choking at all ages. Distinct biological sex and racial-ethnic differences were present in causes of death among adults with Down syndrome.
Conclusions
While efforts to reduce premature mortality for adults with Down syndrome should attend to common risk factors such as heart disease, dementia and Alzheimer’s disease, and cancer, it is imperative to afford increased attention to earlier onset of these diseases, as well as increased risk of death from respiratory and swallowing/choking related disorders at all ages.
Keywords: Down syndrome, mortality, cause of death, age, biological sex
Introduction
Down syndrome is a genetic disorder resulting in a full or partial extra copy of chromosome 21. In the US, it is estimated that there are 8.27 individuals with Down syndrome per 10,000 of the population.1 Based upon the 2018 US population size, this would mean 270,600 individuals with Down syndrome live in the US. People with Down syndrome often experience developmental delays, neurological and anatomical linked cognitive impairment, and increased prevalence of medical conditions such as congenital heart disease and early-onset Alzheimer’s disease.2,3
On average, people with Down syndrome die at younger ages than those without this disorder. However, due to deinstitutionalization, increased access to needed medical care, advances in medical technology and surgical interventions, and general improvements in population health, the mortality disadvantage for individuals with Down syndrome decreased considerably during the 20th century.1,2,4–6 While the average lifespan of an individual with Down syndrome was only 12 years in 1940,7 a recent study of US death certificate data reported the average age at death for adults with Down syndrome was 55 years in 2012–2016.8
Though a vast improvement, on average, adults with Down syndrome are still dying at ages 19 years younger than their peers without Down syndrome,8 with mortality risk increasing substantially after age 40.8,9 This differential may be explained by variation between adults with and without Down syndrome in age at and rates of death from common causes of death such as heart disease,6,9–11 dementia or Alzheimer’s disease,7,9,12–15 respiratory disease,6,16,17 or cancer,6,16,17 or more uncommon causes of death, such as a congenital heart formation for children or young adults with Down syndrome.2,6,7
While prior studies are helpful in understanding causes of death among adults with Down syndrome, they are often based upon small sample sizes, do not distinguish age trends for specific causes of death, and do not attend to possible biological sex and racial-ethnic differences. In addition, studies from the US are dated, with the most recent population-based study utilizing data from 1997.6 We build on the insights of earlier studies by analyzing comparative causes of death between the US population of adults, age 18 and over, with and without Down syndrome recorded on their death certificate between 2013 and 2017. Based upon prior studies, we expect that, compared to adults without Down syndrome, adults with Down syndrome will have increased risk of death from dementia and Alzheimer’s disease, infectious respiratory diseases, and congenital heart disease, and lower rates of death from cancer. As causes of death vary by biological sex and by race-ethnicity in the US general population,18 we also expect to see biological sex and racial-ethnic variation in causes of death among adults with Down syndrome.
Methods
We utilized cause of death data from the National Vital Statistics System 2013–2017 US Multiple Cause-of-Death Mortality files. We limit our primary analysis in this paper to the 9,870 adults, age 18 and over, with Down syndrome (ICD-10 code Q90) indicated on their death certificate, and the 13,323,001 adults without Down syndrome reported on their death certificate. The age range for the entire sample was 18–126, with a top end age of 96 for adults with Down syndrome. Thus, all results describe mortality trends only for those individuals who lived past the age of 18.
The practice of coding Down syndrome as the underlying cause of death “obscures” mortality trends for adults in this population.19–21 Individuals with Down syndrome may have a higher prevalence of specific medical conditions that contribute to earlier deaths such as Alzheimer’s disease or congenital heart disease. However, researchers investigating mortality among those with Down syndrome increasingly argue Down syndrome should not be recorded as the underlying cause of death as it is does little to inform public health and preventive care efforts for this population.20 Thus, prior to analysis, we utilized a sequential revision process fully detailed in a previous study20 to select a valid underlying cause of death on the 62% of death certificates that had Down syndrome coded as the underlying cause of death. Age was coded in continuous years; biological sex was dichotomously coded female and male; and race-ethnicity included the categories Non-Hispanic White, Non-Hispanic Black, Hispanic, and Non-Hispanic Other.
To identify the leading causes of death for adults with Down syndrome, we calculated prevalence rates for 23 causes of death inclusive of the 15 leading causes of death in the US during 2016,22 as well as eight additional causes of death reported as more prevalent among adults with developmental disability in general and/or Down syndrome specifically:3,23 1) choking - aspiration, ingestion, or inhalation of gastric contents, food, or other objects; 2) respiratory failure, not elsewhere classified; 3) intestinal obstruction, or Gastro Esophageal Reflux Disease (GERD); 4) seizure disorders; 5) protein/calorie malnutrition, or volume depletion; 6) dementia; 7) congenital heart defects; and 8) other congenital anomalies. Based upon this analysis, we identified and focus on the 10 leading causes of death, as well as an additional category for unknown/unspecified causes of death. The cause of death was identified as ‘unknown’ when decedents had only Down syndrome coded on their death certificate. The cause of death was identified as ‘unspecified’ when the underlying cause of death was an R-code, indicative of symptoms, signs and abnormal clinical and laboratory findings, not elsewhere classified.24 Dementia and Alzheimer’s disease were combined into one category for analysis. A list of the 10 leading causes of death and their corresponding ICD-10 codes is included in Table 1.
Table 1:
Comparative description of all study variables for adults with and without Down syndrome, 2013–2017 US Multiple Cause-of-Death Mortality files (N=13,332,871)
| Down syndrome (N=9,870) | No Down syndrome (N=13,323,001) | |
|---|---|---|
| Age - Mean(SD) | 55.51 (.10) | 74.09 (.00) |
| Female | 48.45% | 49.32% |
| Race-ethnicity | ||
| Non-Hispanic White | 82.47% | 78.91% |
| Non-Hispanic Black | 8.66% | 11.57% |
| Hispanic | 7.11% | 6.45% |
| Non-Hispanic Other | 1.75% | 3.07% |
| Year - Mean(SD) | 2015.07 (.01) | 2015.04 (.00) |
| Cause of death | ||
| Dementia/Alzheimer’s (ICD-10 codes F03, G30) | 20.70% | 8.17% |
| Diseases of the Heart (ICD-10 codes I00-I09, I11, I13, I20-I51) | 13.12% | 23.61% |
| Influenza and Pneumonia (ICD-10 codes J09-J18) | 11.85% | 2.07% |
| Pneumonitis due to solids and liquids (ICD-10 code J69) | 10.00% | 0.73% |
| CVA - Cerebrovascular Diseases (ICD-10 codes I60-I69) | 3.01% | 5.18% |
| Respiratory failure, not elsewhere classified (ICD-10 code J96) | 2.40% | 0.35% |
| Genitourinary diseases - Nephritis, nephrotic syndrome and nephrosis, urinary tract infection (ICD-10 codes N00-N07, N17-N19, N25-N27, N39) | 2.38% | 2.29% |
| Choking - Aspiration, ingestion, or inhalation of gastric contents, food, or other objects (ICD-10 codes W78-W80) | 2.21% | 0.19% |
| Congenital Heart Defect (ICD-10 codes Q20-Q28) | 2.14% | 0.05% |
| Malignant Neoplasms (ICD-10 codes C00-C97) | 2.05% | 22.26% |
| Unknown/unspecified (No ICD-10 code, R-codes) | 9.02% | 1.16% |
After presenting a description of all study variables for adults with and without Down syndrome, we compare overall risk of dying from specific causes of death between adults with and without Down syndrome utilizing adjusted odds ratios (AOR) from logistic regression models. Similar to standardized mortality odds ratios,6,25,26 adjusted odds ratios estimate the risk of dying from a specific cause of death as opposed to dying from all other causes of death. This analytic strategy is useful for groups, such as adults with Down syndrome, for whom we do not have a reliable population estimate needed as the denominator to calculate standardized mortality rates. For ease of interpretation, we use language of comparative risk when describing adjusted odds ratios. Having confirmed overall differences in causes of death, we then compare the predicted probabilities of dying from specific causes of death for adults with and without Down syndrome by age. Finally, we utilize odds ratios to assess whether there were biological sex and racial-ethnic differences in causes of death among adults with Down syndrome.
Results
Comparisons between adults with and without Down syndrome
The prevalence of Down syndrome on the death certificates of adults who died in the US between 2013 and 2017 was 7.40 per 10,000, which was slightly lower than, but within the 90% confidence interval reported by Presson et al.1 Compared to adults without Down syndrome (Table 1), adults with Down syndrome had an overall 18.6 year lower mean age at death. The biological sex distribution of decedents was similar for adults with and without Down syndrome. A higher percentage of adults with Down syndrome were Non-Hispanic White, coinciding with lower percentages among Non-Hispanic Blacks and Non-Hispanic Others. Distinct differences were also apparent in the unadjusted percentage of adults with and without Down syndrome who died from each of the causes of death except for genitourinary disease.
Differences in causes of death between adults with and without Down syndrome were also apparent in the adjusted odds ratios (Table 2). All odds ratios were adjusted for age and year of death. Compared to adults without Down syndrome, comparative risk of death for adults with Down syndrome was substantially higher for pneumonitis (AOR=28.0; 95% CI=26.2, 29.9); dementia/Alzheimer’s disease (AOR=24.8; 95% CI=23.6, 24.1) congenital heart defect (AOR=21.7; 95% CI=18.8, 24.9); and choking (AOR=11.8; 95% CI=10.3, 13.5). In contrast, comparative risk of death was substantially lower for adults with Down syndrome for malignant neoplasms (AOR=0.05). Though not as pronounced, risk of death was higher for adults with Down syndrome for all other causes of death except for diseases of the heart, which was lower for adults with Down syndrome (AOR=0.7; 95% CI=0.6, 0.7), and for cerebrovascular disease, which was similar for adults with and without Down syndrome (AOR=0.9; 95% CI= 0.8, 1.0).
Table 2:
Adjusted odds ratios of causes of death for adults with Down syndrome compared to adults without Down syndrome, 2013–2017 US Multiple Cause-of-Death Mortality files (N=13,332,871)
| Cause of death | AOR | 95% CI |
|---|---|---|
| Dementia/Alzheimer’s | 24.84*** | (23.60, 24.14) |
| Diseases of the Heart | 0.68*** | (0.64, 0.72) |
| Influenza and Pneumonia | 9.93*** | (9.34, 10.56) |
| Pneumonitis | 27.97*** | (26.16, 29.92) |
| CVA - Cerebrovascular Diseases | 0.93 | (0.83, 1.04) |
| Respiratory failure | 8.13*** | (7.14, 9.25) |
| Genitourinary diseases | 1.46*** | (1.28, 1.66) |
| Choking | 11.78*** | (10.29, 13.49) |
| Congenital Heart Defect | 21.66*** | (18.84, 24.90) |
| Malignant Neoplasms | 0.05*** | (0.05, 0.07) |
| Unknown/unspecified | 8.96*** | (8.36, 9.60) |
Note: AOR=adjusted odds ratio; all AORs adjusted for age and year of death
In order to further refine our understanding of whether these differential cause of death risks are stable or fluctuate across the life course, we estimated adjusted odds ratios for each specific cause of death utilizing an age and age-squared measure for adults with and without Down syndrome (Appendix 1). All models also control for year of death. We then calculated and report in Figure 1 the predicted probabilities of dying for each cause of death for both groups by age, as well as the mean age at death. Though to varying degrees, adults with Down syndrome had consistently higher risk of death from four causes of death across all ages - influenza and pneumonia, respiratory failure, choking, and unknown/unspecified causes. Increased risk of death from pneumonitis was also apparent across all age groups for adults with Down syndrome, but steadily increased through age 60, then slightly decreased into older age. Differences in risk of death from cerebrovascular disease or genitourinary diseases were not remarkable. Mean ages at death for adults with and without Down syndrome who died from these seven causes of death were fairly similar.
Figure 1:
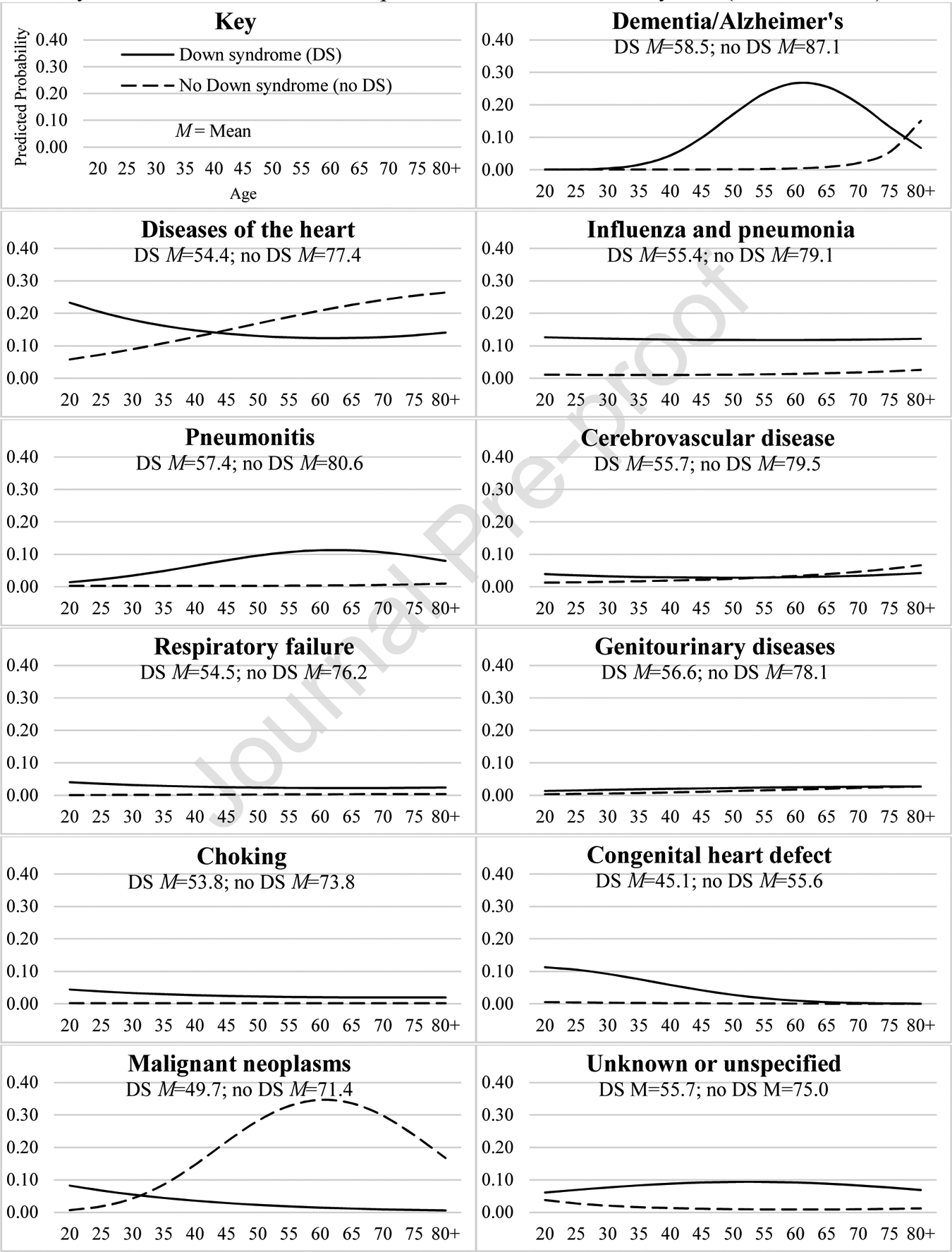
Predicted probabilities of specific causes of death by age for adults with and without Down syndrome, 2013–2017 US Multiple Cause-of-Death Mortality files (N=13,332,871)
The four other causes of death had distinct age trends. For dementia/Alzheimer’s disease, increased risk of death was apparent for adults with Down syndrome starting at age 35, grew substantially until age 60, then decreased in subsequent ages due to a drop in the predicted probability among adults with Down syndrome that occurred in tandem with a rise among adults without Down syndrome. Confirming the anomalous age trend for dementia/Alzheimer’s deaths, while age at death for adults without Down syndrome who died from dementia/Alzheimer’s was 13 years above the overall mean age at death for this group, it was only 3 years above the overall mean age at death for adults with Down syndrome.
Diseases of the heart showed a mid-life crossover trend, with a higher risk for adults with Down syndrome from ages 20 to 40, but lower risk from ages 45 to 80+ due to stability in the predicted probability for adults with Down syndrome in later ages that coincided with a steady rise for adults without Down syndrome. Mean age at death for adults with and without Down syndrome who died from heart disease were not remarkably different from the overall mean age at death for both groups.
Increased risk of death from a congenital heart defect was most pronounced for adults with Down syndrome at age 20, then decreased gradually in subsequent years to the point of having similar predicted probabilities to adults without Down syndrome by age 65. Further highlighting the risk for earlier age at death due to a congenital heart defect, mean age at death was at its lowest point for adults with and without Down syndrome who died from this specific cause of death.
Although risk of death from malignant neoplasms was slightly higher for adults with Down syndrome from ages 20 to 25, this was not the case past the age of 25. In contrast, the predicted probability of malignant neoplasms was similar for both groups at age 30, then diverged due to a severe climb for adults without Down syndrome that peaked at age 60, but a gradual decrease for adults with Down syndrome across subsequent ages. Mean age at death for those who died from cancer was lower than the overall mean age at death for both groups, but, due to the distinct differences in age trends, more pronounced for adults with Down syndrome.
Comparisons among adults with Down syndrome
Among adults with Down syndrome, age at death was similar for females (55.6 years) and males (55.5 years), but varied by race-ethnicity: Non-Hispanic Whites − 56.4 years; Non-Hispanic Blacks − 52.2 years; Hispanics − 50.6 years; and Non-Hispanic Others − 50.1 years.
To better understand possible biological sex and racial-ethnic differences, we analyzed whether these demographic characteristics had differential effects on the overall risk of dying from each specific cause of death among adults with Down syndrome (Appendix 2). As is apparent in Figure 2, compared to males, females with Down syndrome had increased risk of death from dementia/Alzheimer’s disease (AOR=1.2; 95% CI=1.1, 1.3) and congenital heart defect (AOR=1.7; 95% CI=1.2, 2.2), but decreased risk from influenza/pneumonia (AOR=0.8; 95% CI=0.7, 0.9) and pneumonitis (AOR=0.7; 95% CI=0.7, 0.9). Figure 3 provides comparisons of cause of death risk between each racial-ethnic minority group and Non-Hispanic Whites. Among those with Down syndrome, Non-Hispanic Blacks had higher risk of death from cerebrovascular disease (AOR=1.8; 95% CI=1.3, 2.5), and lower risk of death from dementia/Alzheimer’s disease (AOR=0.5; 95% CI=0.4, 0.7), pneumonitis (AOR=0.7; 95% CI=0.5, 0.9), and choking (AOR=0.5; 95% CI=0.3, 0.95). Hispanics had higher risk of death from respiratory failure (AOR=1.9; 95% CI=1.2, 2.8), genitourinary diseases (AOR=1.7; 95% CI=1.1, 2.6), and malignant neoplasms (AOR=2.5; 95% CI=1.7, 3.7), and lower risk of death from dementia/Alzheimer’s disease (AOR=0.5; 95% CI=0.4, 0.7). Non-Hispanic Others had higher risk of death from genitourinary diseases (AOR=3.0; 95% CI=1.6, 5.9).
Figure 2:
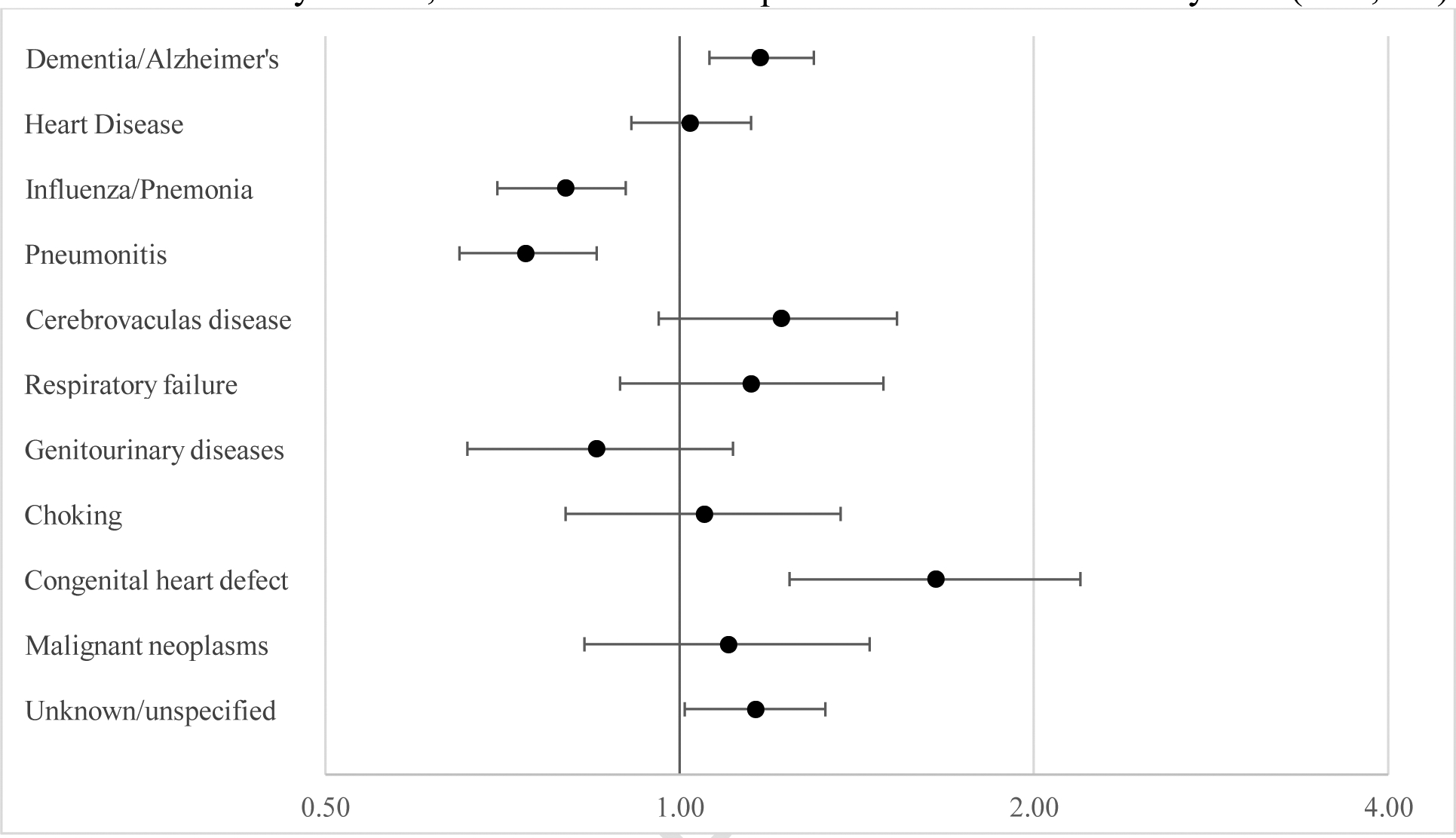
Adjusted odds ratios (AORs) for causes of death for females compared to males for adults with Down syndrome, 2013–2017 US Multiple Cause-of-Death Mortality files (N=9,870)
Figure 3:
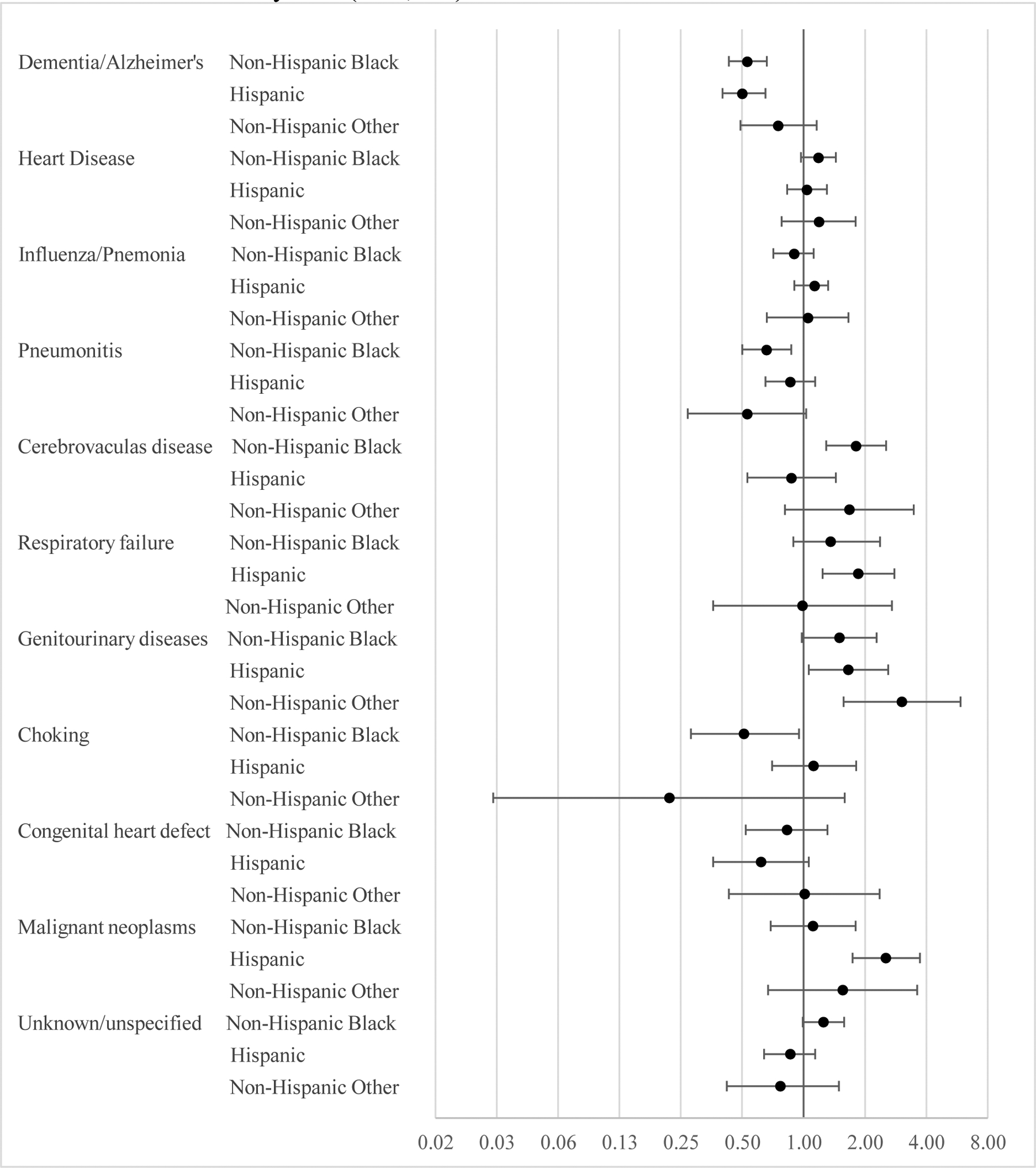
Adjusted odds ratios (AORs) for causes of death for racial-ethnic minority groups compared to Non-Hispanic Whites for adults with Down syndrome, 2013–2017 US Multiple Cause-of-Death Mortality files (N=9,870)
Discussion
This study utilized data from the National Vital Statistics System 2013–2017 US Multiple Cause of Death Mortality files to provide empirical evidence of comparatively distinct causes of death for adults, age 18 and over, who had Down syndrome indicated on their death certificate. Analysis of these mortality trends support our hypotheses and highlights the need for those who provide medical care for adults with Down syndrome to attend to health risk related to causes of death common in the general population, such as heart disease, cancer, and dementia and Alzheimer’s disease.3 However, providers should be aware of anomalous age-related trends in these more common causes of death. While correctly considered primarily middle- to older-age related mortality risks for the general population, this is not the case for adults with Down syndrome. Instead, the highest risk of death from heart disease, cancer, and dementia and Alzheimer’s disease occurs at earlier ages for adults with Down syndrome. In addition to differences in age trends among common causes of death, providers also need to attend to signs and symptoms of influenza and pneumonia, pneumonitis or choking, and congenital heart defects.
These results confirm the findings from prior studies that report earlier age of onset of dementia and Alzheimer’s disease among adults with Down syndrome.7,9,12–15 For adults with Down syndrome in this study, higher rates of death from dementia and Alzheimer’s disease became apparent around age 35, then increased precipitously to a spike at age 60. Providers should ensure that their patients with Down syndrome are regularly screened for dementias, and associated conditions,27 starting at least by age 35.
It is important to note that we chose to include dementia and Alzheimer’s disease as causes of death in our analysis. We are aware that some scholars argue that identifying either as underlying cause of death may reduce the ability to understand the ways in which these often chronic conditions are accompanied by a multi-faceted array of comorbidities that may just as easily be identified as the underlying cause of death.28,29 We agree that analysis of multiple-causes of death may be more appropriate to best understand the role that dementia and Alzheimer’s disease play in mortality trends for adults with Down syndrome, and think this an important topic for future research. Yet, as our focus in this study is comparing cause of death trends between those with and without Down syndrome, and these are typically reported as single causes of death by organizations such as the CDC,18,22 we chose to follow the traditional method of analysis which includes dementia and Alzheimer’s disease as causes of death.
While accurately classified as a respiratory disease, pneumonitis as a cause of death among adults with developmental disabilities such as Down syndrome is more closely akin to choking, as both are likely related to a higher prevalence of dysphagia and swallowing disorders among this population.30 Although a common diagnosis for adults with Down syndrome, these disorders receive little to no attention in texts that discuss the health needs of this population.3,23 This is cause for concern, especially as adults with Down syndrome in this study were between 28 times more likely to die from pneumonitis, and 12 times more likely to die from choking, and risk of death from pneumonitis increased with age. Combined, pneumonitis and choking accounted for 12.2% of all deaths for adults with Down syndrome. Based upon these findings, it is critical for medical providers to consistently screen all adults for dysphagia and/or swallowing disorders, and ensure that people with Down syndrome, as well as their families and care staff, receive needed education regarding proper oral intake and swallowing.31 In addition, public health efforts should focus on raising awareness regarding the prevalence of aspiration and choking related deaths and highlight practical steps for assessing swallowing and oral intake dysfunction.
Results from this study also confirm that individuals with Down syndrome are less prone to death from malignant neoplasms. Yang, et al.6 suggest lower cancer rates among adults with Down syndrome may be due to less exposure to environmental risk, slower cell replication, or the presence of three copies of tumor-suppressing genes on the 21st chromosome. While lower risk of death from cancer may be attributable to this population having comparatively higher protection from hazardous environments and behaviors, or to physiological distinctions, it also may be related to shorter life spans, as the median age at death for adults with Down syndrome is 55,8 and the median age of cancer diagnoses in the US is 66.32
Finally, analysis of causes of death for adults with Down syndrome by biological sex and race-ethnicity revealed a few notable findings. Compared to males, females had increased risk of death from a congenital heart defect and from dementia/Alzheimer’s disease, but lower risk of death from influenza/pneumonia and pneumonitis. Distinct racial-ethnic differences were also present. Non-Hispanic Whites were more likely than Non-Hispanic Blacks and Hispanics to die from dementia or Alzheimer’s disease. In addition, Non-Hispanic Blacks were more likely to die from cerebrovascular disease than Non-Hispanic Whites, and Hispanics were more likely to die from cancer, respiratory failure, and genitourinary diseases than Non-Hispanic Whites. Although utilizing 5 years of mortality data, there were not enough cases to explore age trends in biological sex and racial-ethnic differences in cause of death. However, these overall demographic differences in mortality risk warrant further study.
This study improves our understanding of mortality trends for adults, age 18 and over, who had Down syndrome indicated on their death certificate in multiple ways. Our analysis provides a needed update on causes of death that eliminates the obscuring effect of coding Down syndrome as the underlying cause of death. The analysis also relies on census death certificate data, which unlike administrative data from private or state service providers used in previous studies, is inclusive of adults with Down syndrome who do and do not receive formal support services. As the prevalence of Down syndrome in this study was similar to population estimates, it is likely this study includes the majority of adults who died with Down syndrome in the US between 2013 and 2017. Consequently, results from this study are current, accurately reflect mortality trends for adults across the life course, and are representative of the population of adults with Down syndrome in the US. In addition, use of specific causes of death, as opposed to broader ICD-10 chapters, provides in a more refined understanding of specific diseases causing death in this population.
Endemic to all studies examining cause of death trends among adults with Down syndrome in the US, after revising death certificates that erroneously coded Down syndrome as cause of death,20 we could not identify a cause of death for 9.0% of adults with this disability, as their certificate only included an ICD-10 code for Down syndrome with or without an accompanying R-code. This limitation emphasizes the need to urge those certifying the death certificates of adults with Down syndrome to: 1) when possible, provide a thorough accounting of all causes of death on the death certificate inclusive of, but not limited to Down syndrome; and 2) unless medically justified as and an indispensable part of the causal sequence leading death,33 not record Down syndrome in Part I of the death certificate, but instead, record this disability in Part II of the death certificate.20 Per instructions from the Centers for Disease Control and Prevention (CDC), Part II of the death certificate is intended to include all “other important diseases or conditions that were present at the time of death and that may [italics added] have contributed to death.”34
Conclusion
Though sharing some similar causes of death with adults without Down syndrome, such as heart disease, dementia and Alzheimer’s disease, and cancer, adults with Down syndrome were more likely to die at younger ages from these diseases. In addition, adults with Down syndrome also were more likely to die in early adulthood from a congenital heart defect, and across all ages from influenza and pneumonia, respiratory failure, pneumonitis, and choking. Further research is needed to explore the biological sex and racial-ethnic differences in cause of death among adults with Down syndrome reported in this study. In addition, future studies should attempt to discern whether adults with Down syndrome are protected from risk factors that lead to death from cancer. It seems this may be likely for lung cancer as adults Down syndrome are less likely to work in hazardous occupations, and have access to cancer-causing drugs. Conversely, it is possible that lower overall cancer ratios may, at least partially, be informed by earlier deaths among adults with Down syndrome.
Funding:
Research reported in this publication was supported by the National Institute On Aging of the National Institutes of Health under Award Number R03AG065638. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Appendix 1:
Adjusted odds ratios for causes of death by age stratified by Down syndrome status, 2013–2017 US Multiple Cause-of-Death Mortality files (N=13,332,871)
| Adults with Down syndrome (N=9,870) |
Adults without Down syndrome (N=13,323,001) |
||||
|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | ||
| Dementia/Alzheimer’s | |||||
| Age | 1.75*** | (0.92, 0.98) | 0.85*** | (0.85, 0.86) | |
| Age2 | 1.00*** | (0.99, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.01 | (0.97, 1.04) | 0.99*** | (0.99, 1.00) | |
| Intercept | 0.00*** | (0.00, 0.00) | 0.01*** | (0.01. 0.01) | |
| Heart Disease | |||||
| Age | 0.95* | (0.92, 0.98) | 1.07*** | (1.07, 1.07) | |
| Age2 | 1.00* | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 0.97 | (0.93, 1.01) | 0.99*** | (0.99, 0.99) | |
| Intercept | 0.76 | (0.35, 1.61) | 0.02*** | (0.02, 0.02) | |
| InfluenzaPneumonia | |||||
| Age | 0.99 | (0.96, 1.03) | 0.97*** | (0.97, 0.97) | |
| Age2 | 1.00 | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 0.93* | (0.89, 0.97) | 0.97*** | (0.97, 0.97) | |
| Intercept | 0.16*** | (0.07, 0.39) | 0.02*** | (0.02, 0.02) | |
| Pneumonitis | |||||
| Age | 1.16*** | (1.10, 1.24) | 0.95*** | (0.95, 0.96) | |
| Age2 | 1.00*** | (0.99, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.00 | (0.95, 1.05) | 1.00 | (1.00, 1.01) | |
| Intercept | 0.00*** | (0.00, 0.01) | 0.01*** | (0.00, 0.01) | |
| CVA | |||||
| Age | 0.96 | (0.90, 1.02) | 1.01*** | (1.01, 1.01) | |
| Age2 | 1.00 | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.06 | (0.98, 1.15) | 1.01*** | (1.01, 1.02) | |
| Intercept | 0.08* | (0.02, 0.38) | 0.01*** | (0.01, 0.01) | |
| Respiratory Failure | |||||
| Age | 0.96 | (0.90, 1.03) | 1.06*** | (1.05, 1.07) | |
| Age2 | 1.00 | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.11* | (1.02, 1.22) | 1.09*** | (1.09, 1.10) | |
| Intercept | 0.08* | (0.02, 0.43) | 0.00*** | (0.00, 0.00) | |
| Genitourinary diseases | |||||
| Age | 1.03 | (0.95, 1.12) | 1.07*** | (1.07, 1.08) | |
| Age2 | 1.00 | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.04 | (0.95, 1.14) | 1.00*** | (1.00, 1.00) | |
| Intercept | 0.01*** | (0.00, 0.08) | 0.00*** | (0.00, 0.00) | |
| Choking | |||||
| Age | 0.96 | (0.89, 1.03) | 0.99 | (0.99, 1.00) | |
| Age2 | 1.00 | (1.00, 1.00) | 1.00 | (1.00, 1.00) | |
| Year | 0.99 | (0.90, 1.08) | 1.00*** | (0.99, 1.00) | |
| Intercept | 0.10* | (0.02, 0.52) | 0.00 | (0.00, 0.00) | |
| Congenital Heart Defect | |||||
| Age | 1.05 | (0.97, 1.13) | 0.96*** | (0.95, 0.97) | |
| Age2 | 1.00* | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.00 | (0.90, 1.10) | 0.98 | (0.97, 1.00) | |
| Intercept | 0.09* | (0.02, 0.39) | 0.01*** | (0.01, 0.01) | |
| Malignant Neoplasms | |||||
| Age | 0.96 | (0.89, 1.03) | 1.37*** | (1.37, 1.38) | |
| Age2 | 1.00 | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 1.11* | (0.90, 1.08) | 0.98*** | (0.98, 0.98) | |
| Intercept | 0.21* | (0.05, 0.94) | 0.00*** | (0.00, 0.00) | |
| Unknown/Unspecified | |||||
| Age | 1.05* | (1.00, 1.10) | 0.90*** | (0.90, 10.90) | |
| Age2 | 1.00* | (1.00, 1.00) | 1.00*** | (1.00, 1.00) | |
| Year | 0.99 | (0.94, 1.04) | 0.95*** | (0.95, 0.95) | |
| Intercept | 0.03*** | (0.01, 0.10) | 0.24*** | (0.22, 0.25) | |
Note: AOR=adjusted odds ratio;
p<.001;
p<.05;
p<.05
Appendix 2:
Adjusted odds ratios for causes of death for adults with Down syndrome, 2013–2017 US Multiple Cause-of-Death Mortality files (N=9,870)
| Dementia/Alzheimer’s | Heart | Influenza/Pneumonia | Pneumonitis | |||||
|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Age | 1.04*** | (1.03, 1.05) | 0.99*** | (0.98, 1.00) | 1.00 | (0.99, 1.01) | 1.02*** | (1.01, 1.03) |
| Female | 1.17** | (1.06, 1.30) | 1.02 | (0.91, 1.15) | 0.80*** | (0.70, 0.90) | 0.74*** | (0.65, 0.85) |
| Race-ethnicity (Ref: Non-Hispanic White) | ||||||||
| Non-Hispanic Black | 0.53*** | (0.43, 0.66) | 1.18 | (0.97, 1.44) | 0.90 | (0.71, 1.12) | 0.66** | (0.50, 0.87) |
| Hispanic | 0.50*** | (0.40, 0.65) | 1.04 | (0.83, 1.30) | 1.13 | (0.90, 1.42) | 0.86 | (0.65, 1.14) |
| Non-Hispanic Other | 0.75 | (0.49, 1.14) | 1.19 | (0.78, 1.80) | 1.05 | (0.66, 1.66) | 0.53 | (0.27, 1.03) |
| Year | 1.01 | (0.97, 1.04) | 0.97 | (0.93, 1.01) | 0.93** | (0.89, 0.98) | 1.00 | (0.96, 1.05) |
| Intercept | 0.03*** | (0.02, 0.04) | 0.26*** | (0.19, 0.36) | 0.16*** | (0.10, 0.22) | 0.04*** | (0.03, 0.07) |
| Cerebrovascular disease | Respiratory failure | Genitourinary Diseases | Choking | |||||
|---|---|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Age | 1.00 | (0.99, 1.02) | 0.99 | (0.98, 1.01) | 1.02* | (1.00, 1.03) | 0.98** | (0.97, 1.00) |
| Female | 1.22 | (0.96, 1.53) | 1.15 | (0.89, 1.49) | 0.85 | (0.66, 1.11) | 1.05 | (0.80, 1.37) |
| Race-ethnicity (ref: Non-Hispanic White) | ||||||||
| Non-Hispanic Black | 1.81** | (1.29, 2.54) | 1.36 | (0.89, 2.07) | 1.50 | (0.98, 2.28) | 0.51* | (0.28, 0.95) |
| Hispanic | 0.87 | (0.53, 1.44) | 1.86** | (1.24, 2.79) | 1.66* | (1.06, 2.60) | 1.12 | (0.70, 1.81) |
| Non-Hispanic Other | 1.68 | (0.81, 3.47) | 0.99 | (0.36, 2.71) | 3.04** | (1.57, 5.89) | 0.22 | (0.03, 1.59) |
| Year | 1.06 | (0.97, 1.15) | 1.11* | (1.01, 1.22) | 1.03 | (0.94, 1.13) | 0.99 | (0.90, 1.09) |
| Intercept | 0.02*** | (0.01, 0.04) | 0.03*** | (0.01, 0.06) | 0.01*** | (0.00, 0.02) | 0.06*** | (0.03, 0.12) |
| Congenital Heart Defect | Malignant Neoplasms | Unspecified/Unknown | ||||
|---|---|---|---|---|---|---|
| AOR | 95% CI | AOR | 95% CI | AOR | 95% CI | |
| Age | 0.93*** | (0.92, 0.94) | 0.96*** | (0.95, 0.97) | 1.00 | (1.00, 1.01) |
| Female | 1.65** | (1.24, 2.19) | 1.10 | (0.83, 1.45) | 1.16* | (1.01, 1.33) |
| Race-ethnicity (Ref: Non-Hispanic White) | ||||||
| Non-Hispanic Black | 0.83 | (0.52, 1.31) | 1.11 | (0.69, 1.80) | 1.25 | (0.99, 1.58) |
| Hispanic | 0.62 | (0.36, 1.06) | 2.54*** | (1.74, 3.72) | 0.86 | (0.64, 1.14) |
| Non-Hispanic Other | 1.01 | (0.43, 2.36) | 1.56 | (0.67, 3.61) | 0.77 | (0.42, 1.39) |
| Year | 0.99 | (0.90, 1.09) | 1.11* | (1.01, 1.23) | 0.99 | (0.94, 1.04) |
| Intercept | 0.76 | (0.45, 1.30) | 0.14*** | (0.08, 0.27) | 0.08*** | (0.05, 0.12) |
Note: AOR=adjusted odds ratio;
p<.001;
p<.05;
p<.05
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of interests:
To the best of our knowledge, no conflict of interest, financial or other, exists.
Submission declaration: This manuscript is not under consideration for publication elsewhere, is approved by all authors, and, if accepted, will not be published elsewhere including electronically in the same form, in English or in any other language, without the written consent of the copyright-holder.
Prior presentation: Results for this study were presented at the 2019 Gerontological Society of America Annual Meeting.
REFERENCES
- 1.Presson AP, Partyka G, Jensen KM, et al. Current estimate of Down syndrome population prevalence in the United States. The Journal of Pediatrics. 2013;163(4):1163–1168. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Esbensen AJ, MacLean WE. Down syndrome In: Wehmeyer ML, ed. A comprehensive guide to intellectual and developmental disabilities. 2nd ed Baltimore, MD: Brookes Publishing; 2017:195–208. [Google Scholar]
- 3.Rubin IL, Crocker AC. Medical care for children & adults with developmental disabilities. Baltimore, MD: Paul H. Brookes Publishing; 2006. [Google Scholar]
- 4.Bittles AH, Bower C, Hussain R, Glasson EJ. The four ages of Down syndrome. European Journal of Public Health. 2006;17(2):221–225. [DOI] [PubMed] [Google Scholar]
- 5.Englund A, Jonsson B, Zander CS, Gustafsson J, Annerén G. Changes in mortality and causes of death in the Swedish Down syndrome population. American Journal of Medical Genetics Part A. 2013;161(4):642–649. [DOI] [PubMed] [Google Scholar]
- 6.Yang Q, Rasmussen SA, Friedman JM. Mortality associated with Down’s syndrome in the USA from 1983 to 1997: a population-based study. The Lancet. 2002;359(9311):1019–1025. [DOI] [PubMed] [Google Scholar]
- 7.Coppus A, Evenhuis H, Verberne G-J, et al. Dementia and mortality in persons with Down’s syndrome. Journal of Intellectual Disability Research. 2006;50(10):768–777. [DOI] [PubMed] [Google Scholar]
- 8.Landes SD, Stevens JD, Turk MA. Heterogeneity in age at death for adults with developmental disability. Journal of Intellectual Disability Research. 2019;63:1482–1487. [DOI] [PubMed] [Google Scholar]
- 9.Torr J, Strydom A, Patti P, Jokinen N. Aging in Down syndrome: Morbidity and mortality. Journal of Policy and Practice in Intellectual Disabilities. 2010;7(1):70–81. [Google Scholar]
- 10.Esbensen AJ, Seltzer MM, Greenberg JS. Factors predicting mortality in midlife adults with and without Down syndrome living with family. Journal of Intellectual Disability Research. 2007;51(12):1039–1050. [DOI] [PubMed] [Google Scholar]
- 11.Janicki MP, Dalton AJ, Henderson CM, Davidson PW. Mortality and morbidity among older adults with intellectual disability: health services considerations. Disability & Rehabilitation. 1999;21(5):284–294. [DOI] [PubMed] [Google Scholar]
- 12.Coppus AMW, Evenhuis HM, Verberne G-J, et al. Survival in elderly persons with Down syndrome. Journal of the American Geriatrics Society. 2008;56(12):2311–2316. [DOI] [PubMed] [Google Scholar]
- 13.Janicki MP, Dalton AJ. Prevalence of dementia and impact on intellectual disability services. Mental retardation. 2000;38(3):276. [DOI] [PubMed] [Google Scholar]
- 14.Strydom A, Shooshtari S, Lee L, et al. Dementia in older adults with intellectual disabilities—Epidemiology, presentation, and diagnosis. Journal of Policy and Practice in Intellectual Disabilities. 2010;7(2):96–110. [Google Scholar]
- 15.Uppal H, Chandran S, Potluri R. Risk factors for mortality in Down syndrome. Journal of Intellectual Disability Research. 2015;59(9):873–881. [DOI] [PubMed] [Google Scholar]
- 16.Hermon C, Alberman E, Beral V, Swerdlow AJ. Mortality and cancer incidence in persons with Down’s syndrome, their parents and siblings. Annals of Human Genetics. 2001;65(2):167–176. [DOI] [PubMed] [Google Scholar]
- 17.Hill DA, Gridley G, Cnattingius S, et al. Mortality and cancer incidence among individuals with Down syndrome. JAMA Internal Medicine. 2003;163(6):705–711. [DOI] [PubMed] [Google Scholar]
- 18.Heron MP. Deaths: Leading causes for 2016. National vital statistics reports. 2018;67(6). [PubMed] [Google Scholar]
- 19.Landes SD, Peek CW. Death by mental retardation? The influence of ambiguity on death certificate coding error for adults with intellectual disability. Journal of Intellectual Disability Research. 2013;57(12):1183–1190. [DOI] [PubMed] [Google Scholar]
- 20.Landes SD, Stevens JD, Turk MA. Obscuring effect of coding developmental disability as the underlying cause of death on mortality trends for adults with developmental disability: a cross-sectional study using US Mortality Data from 2012 to 2016. BMJ Open. 2019;9:e026614. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Trollor J, Srasuebkul P, Xu H, Howlett S. Cause of death and potentially avoidable deaths in Australian adults with intellectual disability using retrospective linked data. BMJ Open. 2017;7(2). [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Xu J, Murphy SL, Kochanek KDK, Bastian BB, Arias E. Deaths: Final Data for 2016. National Vital Statistics Reports. 2018;67(5). [PubMed] [Google Scholar]
- 23.Prasher VP, Janicki MP, eds. Physical health of adults with intellectual and developmental disabilities. 2nd ed. New York: Springer; 2019. [Google Scholar]
- 24.Naghavi M, Makela S, Foreman K, O’Brien J, Pourmalek F, Lozano R. Algorithms for enhancing public health utility of national causes-of-death data. Population Health Metrics. 2010;8(1):9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Smith KR, Kliewer EV. Estimating standardized mortality odds ratios with National Mortality Followback Data. Epidemiology. 1995;6(1):55–60. [DOI] [PubMed] [Google Scholar]
- 26.Miettinen OS, Wang J-D. An alternative to the proportionate mortality ratio. American Journal of Epidemiology. 1981;114(1):144–148. [DOI] [PubMed] [Google Scholar]
- 27.Kurrle S, Brodaty H, Hogarth R. Physical comorbidities of dementia. Cambridge University Press; 2012. [Google Scholar]
- 28.Brunnström HR, Englund EM. Cause of death in patients with dementia disorders. European Journal of Neurology. 2009;16(4):488–492. [DOI] [PubMed] [Google Scholar]
- 29.Park J Mortality from Alzheimer’s disease in Canada: A multiple-cause-of-death analysis, 2004 to 2011. Health Reports. 2016;27(5):17–21. [PubMed] [Google Scholar]
- 30.Samuels R, Chadwick DD. Predictors of asphyxiation risk in adults with intellectual disabilities and dysphagia. Journal of Intellectual Disability Research. 2006;50(5):362–370. [DOI] [PubMed] [Google Scholar]
- 31.Chadwick DD, Jolliffe J, Goldbart J, Burton MH. Barriers to caregiver compliance with eating and drinking recommendations for adults with intellectual disabilities and dysphagia. Journal of Applied Research in Intellectual Disabilities. 2006;19(2):153–162. [Google Scholar]
- 32.National Cancer Institute. Age and cancer risk. National Insitutes of Health. https://www.cancer.gov/about-cancer/causes-prevention/risk/age. Published 2015. Accessed February 8, 2019. [Google Scholar]
- 33.Office for National Statistics. Guidance for doctors completing Medical Certificates of Cause of Death in England and Wales. https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/757010/guidance-for-doctors-completing-medical-certificates-of-cause-of-death.pdf. Published 2018. Accessed December, 2019.
- 34.National Center for Health Statistics. Physicians’ handbook on medical certification of death Centers for Disease Control and Prevention. https://www.cdc.gov/nchs/data/misc/hb_cod.pdf. Published 2003. Accessed November 29, 2018. [Google Scholar]