

Abstract
Background:
There is a growing body of literature supporting the use of 5-aminolevulinic acid (5-ALA) in the pediatric population, however, its use is still considered “off label” in this setting. In this retrospective study, we report our experience using 5-ALA in pediatric patients with focal brainstem gliomas (BSGs).
Methods:
Patients younger than 16 years presenting with a newly diagnosed BSG that was focal in nature were considered suitable for treatment with 5-ALA-assisted surgery. Exclusion criteria included MRI features suggestive of a diffuse intrinsic pontine glioma. A single dose of 5-ALA was administered preoperatively. Intraoperative fluorescence was recorded as “solid,” “vague,” or “none.” The effectiveness of the fluorescence was graded as “helpful” or “unhelpful.”
Results:
Eight patients underwent 5-ALA-assisted surgery. There were four tumors located in the pons, two midbrain tumors, and two cervicomedullary tumors. Histological analysis demonstrated three diffuse astrocytomas, three pilocytic astrocytomas, and two anaplastic astrocytomas. Solid fluorescence was found in three of the eight cases, vague fluorescence was found in two cases, and no fluorescence was found in three cases. Fluorescence was useful in 3 (37%) cases. No patients experienced any complications attributable to the administration of the 5-ALA.
Conclusion:
With a total fluorescence rate of 62.5% but a subjectively assessed “usefulness” rate of only 37.5%, the role of 5-ALA in BSG surgery is limited. Given the toxicological safety, however, of the agent, caution is perhaps needed before dismissing the use of 5-ALA entirely.
Keywords: 5-aminolevulinic acid, Diffuse intrinsic pontine glioma, Focal brainstem tumors, Pediatric brain tumor

INTRODUCTION
Brainstem gliomas (BSGs) account for approximately 10–20% of brain tumors in children.[33] The management of BSGs in the past relied solely on nonoperative interventions and palliation.[33,81] Over the past three decades, however, the notion that these lesions are inoperable has shifted. With the advent of sophisticated neuronavigation, imaging technology, and neurophysiological monitoring, a group of these neoplasms has become amenable to surgery.[80] 5-aminolevulinic acid (5-ALA)-guided surgery has been proven to be a safe and effective adjuvant for the removal of malignant brain tumors[76] and its spectrum of use has been increasing with reported usage in low-grade lesions,[29] metastatic lesions,[41] and extra-axial lesions.[47] There is a growing body of literature supporting the use of 5-ALA in the pediatric population,[4,54,72] however, its use is still considered “off label”[89] in this setting. As far as, we are aware this is the first manuscript to address the use of 5-ALA specifically in the resection of pediatric focal BSGs.
In this retrospective study, we report our experience using 5-ALA in pediatric patients with focal BSGs. The aim of the report is to analyze the safety of its use, evaluate the intraoperative fluorescence rate and the “usefulness” of 5-ALA in this specific group of patients.
METHODS
Patient selection
Patients younger than 16 years presenting with a newly diagnosed, untreated BSG that was focal in nature were considered suitable for treatment with 5-ALA-assisted surgery. Exclusion criteria included MRI features suggestive of a diffuse intrinsic pontine glioma (DIPG), preexisting hepatic or renal disease, abnormal renal or hepatic function, any known cutaneous hypersensitivity, or a first degree relative with porphyria. Parents or guardians, after being informed about the potential benefit and risks derived from the existing adult data, were offered the treatment as an off-label use. Following an explanation regarding the lack of safety and efficacy data from clinical trials in the pediatric population and the character of an individual treatment attempt, written informed consent was obtained on behalf of the children from their parents or guardians. The Human Research Ethics Committee of the medical faculty of the University of the Witwatersrand approved the scientific analyses of these cases.
Operative protocol
Patients were treated according to the previously reported adult protocol of Stummer et al.[76] All patients received intravenous dexamethasone 0.25 mg/kg (body weight)/day in four divided doses for 2 days before the surgery. A single dose of 5-ALA (Gliolan®) 20 mg/kg suspended in 50 ml of tap water was administered orally 4 h before the predicted “cutting time” in the presence of medical personnel. All operations were performed with a microscope equipped with a fluorescent 400 nm UV light and filters (Zeiss, Kinevo 900, Carl Zeiss AG, Oberkochen, Germany). A neuronavigation system (STEALTH, Medtronic, Minneapolis, USA) was used for surgical planning and tumor localization. Intraoperative neurophysiological monitoring was employed in all cases. Intraoperative fluorescence was recorded as “solid,” “vague,” or “none” in accordance with previously described criteria.[75,78] The surgical procedures were performed by the same surgeon (J.L) who also judged the presence of 5-ALA fluorescence as “helpful” or “unhelpful.” The tumor was removed with standard microsurgical techniques. At the end of resection, the cavity was systematically checked in the violet-blue light mode for any residual tumor. Dissection was halted when we achieved a lack of tumoral tissue at white light together with a lack of fluorescent tissue at final blue light control. Anatomical localization of eloquent tissue such as brainstem nuclei or a significant change in neurophysiological parameters also resulted in aborting surgery regardless of the presence of residual tumor.
Clinical and radiological assessment
Patients were examined clinically during their postoperative course to assess for new neurological deficits or surgical complications. Patients were clinically assessed for signs of adverse drug reactions. The Lansky Performance Scale (LPS)[39] was used to evaluate general physical performance preoperatively, on discharge and at 3 months follow-up. Extent of resection was assessed on postoperative gadolinium-enhanced MRI obtained within 48 h of surgery and graded as either gross total resection (GTR), near-total resection (NTR), or subtotal resection (STR), which we defined as no evidence of residual tumor, greater than 90% excision, and less than 90% excision, respectively.
Statistical analysis
As the number of patients was small, the data presentation is mostly descriptive. Averages were expressed as means. Relationships between categorical variables were investigated by means of Fisher’s exact test. All statistics were performed using SSPS Version 25.0 for Windows (SPSS Inc., Chicago, IL, USA). P < 0.05 was considered statistically significant.
RESULTS
Demographics
Among the patients, six were male (75%) and 2 were female (25%). The mean age was 6.1 years old (range 1–13 years). There were four tumors located in the pons, two midbrain tumors, and two cervicomedullary tumors.
Histology and fluorescence patterns
Histological analysis demonstrated three diffuse astrocytomas (WHO Grade II), three pilocytic astrocytomas (PCAs) (WHO Grade I), and two anaplastic astrocytomas (WHO Grade III). Solid fluorescence was found in three of the eight cases, vague fluorescence was found in two cases, and no florescence was found in three cases. The sample size is too small to make meaningful commentary regarding correlation of fluorescence to tumor histology or the WHO Grade, but 2 of the 3 (66%) cases of solid fluorescence were anaplastic astrocytomas (WHO Grade III). In two of the three cases in which there was solid, and hence potentially useful fluorescence, the surgical resection was halted due to a significant change in neurophysiological parameters occurring with extensive tumor fluorescence still visible in the surgical bed. As the presence of fluorescence did not alter the surgery in these cases, we, by definition, needed to grade them as “nonuseful.” The rate of “useful” fluorescence was thus reduced to 3 (37%) cases. Strong fluorescence or the determination of “usefulness” by the surgeon did not correlate with resection rate. [Table 1] summarizes the demographics, tumor classification, and intraoperative outcomes. [Figure 1] demonstrates a case with solid fluorescence, however due to identification of cranial nerve nuclei within the tumor bed, surgery needed to be halted, despite residual fluorescent tissue still identifiable within the tumor bed. We found no false-positive fluorescent tissue, that is, all tissues sent for histology confirmed tumor cells, irrespective of intraoperative vague, or solid fluorescence.
Table 1:
Demographics, classification, and intraoperative findings.
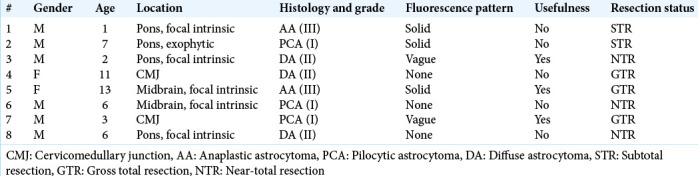
Figure 1:
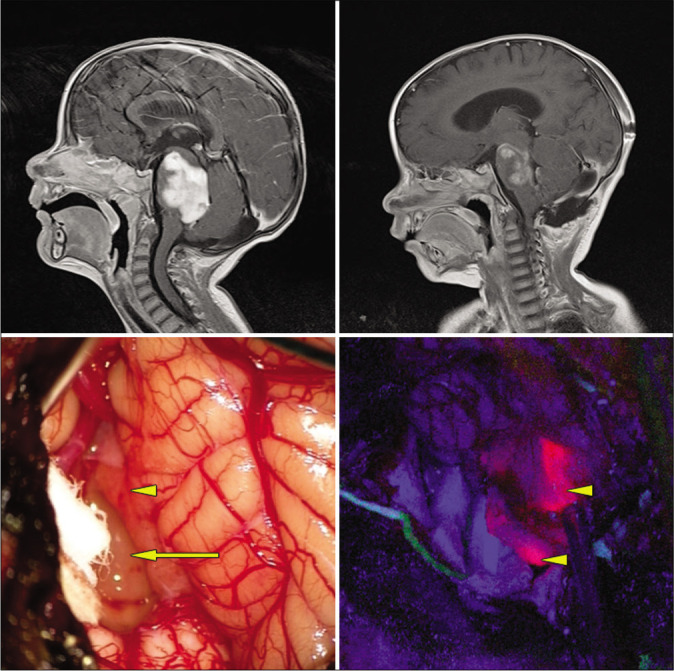
Exophytic pontine pilocytic astrocytoma. Top left: preoperative, postgadolinium-enhanced sagittal MRI. Top right: postoperative gadolinium-enhanced MRI revealing subtotal resection. Bottom left: intraoperative white light microscopic view. Arrow: obvious tumor under white light microscopy. Arrowhead: normal appearing tissue under white light microscopy. Bottom right: arrow heads: blue light mode reveals solid fluorescence of both obvious tumor and normal appearing area under white light mode.
Adverse events, neurological sequelae, and outcome
No patients experienced any complications directly attributable to the administration of the 5-ALA. We achieved GTR in three cases, NTR in three cases, and STR in two cases. Five patients experienced postoperative complications, including one case of postoperative hydrocephalus requiring a permanent ventriculoperitoneal shunt, two cases of worsening ataxia, and two cases of diplopia. With rehabilitation, there were no permanent neurological deficits at 3 months follow-up in any of the patients. There were no significant differences between the presurgical and direct postsurgical (P = 0.12) or 3 months follow-up (P = 0.55) LPS results.
DISCUSSION
BSGs account for 25% of posterior fossa tumors and 10–20% of all CNS tumors in children.[33,59] The advent of modern-day neuroimaging has brought about a realization that brainstem tumors are not a distinct entity, but a heterogeneous collection of tumor types and locations.[14,25] Many classification systems have been proposed for these lesions, incorporating features such as size, location, and imaging characteristics.[2,9,15,43,59,73] Epstein and McCleary[14] grouped intrinsic nonexophytic tumors as focal, diffuse, or cervicomedullary. In this report, we have used the classification system of Choux et al.:[9] Type1 I, diffuse BSG; Type II, focal intrinsic tumor; Type II, exophytic; and Type IV, cervicomedullary. From a surgical perspective, the most important differentiator of BSGs is between diffuse lesions and all other tumors.[10,17]
In our unit, we follow the treatment algorithm outlined by Pincus et al.[52] in dealing with BSGs. Based on MRI imaging, tumors that are believed to be resectable with acceptable risk are tackled surgically, lesions that are found to be consistent with diffuse pontine gliomas are treated empirically while lesions with an atypical appearance, which are not likely to benefit from resection, are candidates for stereotactic biopsy sampling and histological examination. Although by no means universally accepted,[79] the utility and efficacy of obtaining a histological diagnosis in atypical lesions have been validated by several centers.[12,13,48,57]
Although there are no sanctioned radiological guidelines for the diagnosis of a DIPG,[22] in the current series, we relied on the classic features[18,88] ascribed to typical DIPGs: (1) an intrinsic, central location involving more than 50% of the axial diameter of the pons; (2) diffuse infiltration with indistinct tumor margins; (3) hypointensity on T1-weighted MR imaging sequences; (4) hyperintensity on T2-weighted sequences; (5) no or minimal contrast enhancement after the administration of gadolinium; (6) the absence of cystic or exophytic components; and (7) encasement of the basilar artery, as exclusion criteria for resective surgery.
While there are proponents of surgery for diffuse BSGs,[37,43,80] surgical resection of these lesions carries a high morbidity and mortality, and radiation therapy is generally considered the primary therapy.[30,59,87] Conversely, the therapeutic goal of focal BSGs is safe and total surgical removal.[14,30,42,53] In most cases, a well-defined interface between the tumor and neural tissue indicates a GTR or STR resulting in a favorable prognosis.[1,41,63,85] Although not universal, several groups have found that the extent of resection is an important prognostic factor[35,51,68,69] for survival and some groups have advocated relook surgery[30] for recurrent lesions or if primary surgery needs to be halted prematurely because of a transient intraoperative injury. We elected not to perform any relook/second surgeries in the two cases that needed to be terminated prematurely due to alterations in intraoperative neurophysiology, but instead referred these children for radiotherapy.
The role of 5-ALA assistance in high-grade glioma surgery is well established with increased GTR resection rates and 6-month progression-free survival rates benefitting HGG patients receiving 5-ALA.[76] Reliable fluorescence rates approach 100% in both the adult and pediatric population.[54,75] More recently, the role of 5-ALA in low-grade glioma (LGG) surgery,[29] extra-axial,[47] and metastatic disease[41] has been advocated. The use of 5-ALA in the pediatric group is gaining popularity, although still considered as off label.[89] The literature regarding the use of 5-ALA in the pediatric population is largely restricted to supratentorial tumors and the frequently occurring posterior fossa tumors, namely, medulloblastomas and ependymomas.[3,54,72] Very little data are available regarding its use for brainstem lesions.[41,55]
The histopathology of DIPG represents a spectrum with grade not predictive of survival.[6] Focal BSGs, however, are commonly low grade (WHO I or II), with PCAs and diffuse astrocytoma/LGG[4,30,33,38] being the most commonly reported pathologies. It is important, therefore, to explore the value of 5-ALA-assisted surgery for these pathologies in locations outside of the brainstem. The value of 5-ALA in surgery for PCAs is generally accepted to be quite low.[72,89] Only 3 of the 21 PCAs in children reported in the literature displayed unequivocal and useful fluorescence.[7,54,77] Stummer et al.[77] hypothesized that the benign nature of PCAs prevents PpIX accumulation in these tumors and they are hence invisible to fluorescence. We found a global fluorescence rate (solid and vague florescence, across the entire cohort) of 62.5%, while two out of the three PCAs (66%) demonstrated fluorescence. As previously described[3] for posterior fossa lesions, contrast enhancement on MRI is not consistently predictive of malignant histopathology with two of the three PCAs in our group demonstrating vivid preoperative contrast enhancement on MRI. Likewise, for HGG, contrast enhancement appears to have a linear, but not identical correlation with 5-ALA fluorescence, whereas in PCAs and LGGs, there appears to be a very poor correlation.[16,46,66,86] The value of 5-ALA in LGG surgery appears to be variable. In the five largest studies to date of 5-ALA-assisted surgery in LGG, the fluorescence rates have been reported as extremely variable, ranging between 8 and 52%.[16,19,29,83,86] In the study by Goryaynov et al.,[19] in which they found 52% positive fluorescence rate they noted a significant difference in visible fluorescence, depending on the preoperative use of antiepileptic drugs (AEDs). Of the 15 patients with preoperative AED intake, 4 patients (27%) displayed visible fluorescence, whereas in the 12 patients without prior AED usage, 10 (83%) displayed visible fluorescence. Our relatively high percentage, of 62.5% of fluorescence across the cohort, may in part be due to the fact that none of our patients had received AEDs preoperatively. In vitro studies[24,40] have demonstrated a reduction of PpIX of up to 45% in glioma cells by phenytoin and valproates, which may account for the clinically observed phenomenon of diminished intraoperative fluorescence in these patients.
Potentially of greater significance than histological diagnosis, tumor grade, or markers of proliferation[45,47,56] in predicting fluorescence may be the distinct genetic expression profile of the tumor.[5] In both glioma[1] and nonglioma CNS neoplasms,[61,70,71] differing molecular metabolism has been shown to be predictive of fluorescence rate. Saito et al.[65] demonstrated that with multivariate analysis, isocitrate dehydrogenase 1 status of diffuse gliomas was the only independent, statistically significant factor related to 5-ALA fluorescence. Of particular, interest would be to determine if the histone H3 mutation (H3K27M) that is found in greater than 80% of diffuse midline gliomas[26] would or would not be correlated with 5-ALA fluorescence. Although in this series, only focal tumors were included, it is a limitation of the study that we could not perform molecular subtyping as in up to 35% of tumors not considered to be typical DIPGs on MRI imaging, the H3K27M mutation has been found.[8] Since the presence of the H3K27M mutation carries a uniformly fatal prognosis independent of tumor grade,[6] location or extent of tumor resection[34] stereotactic biopsy of both focal and diffuse lesions may be warranted to direct clinical decision-making.[20,21,27]
One of the limitations of 5-ALA-assisted surgery of lesions located in the brainstem is the impaired reliability of fluorescence in this area. Reliable fluorescence requires a sufficient exposure to fluorescent light at a perpendicular perspective to the operating microscope.[55,58] Given the depth, small operating field, and possible “blind spots” inherent to brainstem surgery, fluorescence may be impaired. In our experience, this was not a problem. The cases of poor fluorescence we felt were due to the inherent biology of the tumor cells and 5-ALA metabolism, rather than technical shortcomings. Having said that however, it is interesting to note that protoporphyrin IX fluorescence can be measured ex vivo in LGG tissue[28] and intraoperative confocal microscopy has been found to reliably identify tumor fluorescence in both Grade I and Grade II gliomas, in which standard microscopic tumor fluorescence had failed to identify histopathological proven tumorous tissue.[67] The addition of intraoperative confocal microscopy,[28] wavelength-specific lighted suction units,[46] or neuroendoscopes equipped with fluorescence capabilities[58,60] may in due course increase the 5-ALA florescence rate of tumors with inherently low fluorescence or those in poorly “visible” locations.
In HGG surgery, the 5-ALA fluorescence pattern is not homogenous throughout the tumor tissue. A three-tier grading system described by Stummer et al.[75] defines three different fluorescence entities: deep red fluorescence of the vital core of glioma tissue – labeled as “solid” – is distinguished from a more “vague” fluorescence zone, which was defined as a “transition zone with clearly discernible, but lighter pink fluorescence” and a nonfluorescing zone, described as a blue color after violet-blue light excitation. This spectrum of fluorescence is seen less commonly in non-HGG lesions[32] with most non-HGG tumors displaying partial fluorescence.[3,31,47,67,72] We chose to report our intraoperative findings using this three-tier system, we did not, however, find an infiltrative zone of “vague” fluorescence around the “solidly” fluorescing lesions. We also determined if the visible florescence was “useful,” which was defined by Stummer et al.[77] as “leading to changes in surgical strategy or identification of residual tumor.” In five of our eight cases, the addition of 5-ALA to the surgical procedure was not considered to be useful, in three cases, this was due to no florescence being visible, and in two cases, despite “solid” fluorescence, the surgery was halted with visible fluorescence in the tumor bed due to changes in neurophysiological parameters. In the three cases, in which fluorescence was deemed “useful,” it allowed for visualization of tumor that appeared normal under white light microscopy, however under blue light mode, fluorescence was still visible. This allowed for a greater extent of resection in all three of these cases, obtaining a GTR in two of the cases and a NTR in one. In two of the three cases, the fluorescence was considered “useful” despite the fluorescence being only “vague” in nature as it still allowed for visualization of residual tumor not identifiable under white light alone. [Figure 2] demonstrates a case of vague but still useful fluorescence in which additional tumor tissue was identified, not visualized by white light microscopy alone.
Figure 2:
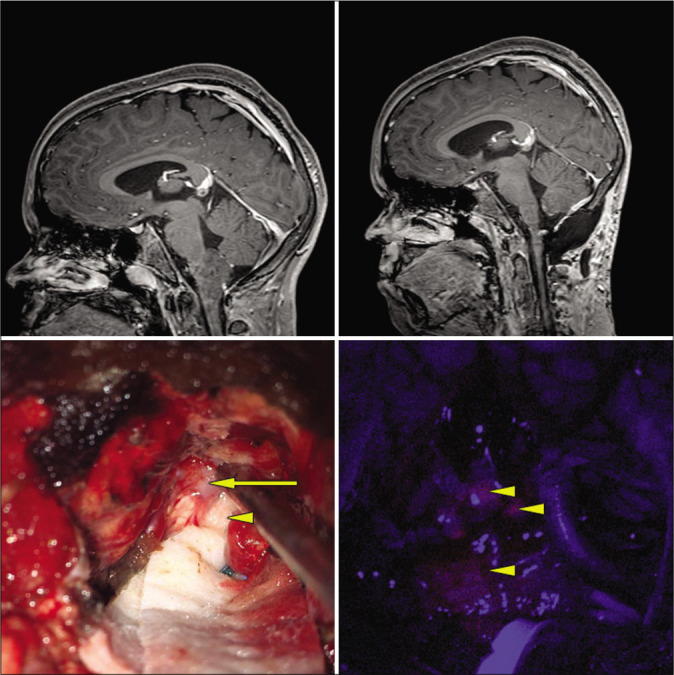
Cervicomedullary pilocytic astrocytoma. Top left: preoperative, postgadolinium-enhanced sagittal MRI. Top right: postoperative gadolinium-enhanced MRI revealing GTR. Bottom left: intraoperative white light microscopic view. Arrow: obvious tumor under white light microscopy. Arrowhead: normal appearing tissue under white light microscopy. Bottom right: arrow heads: blue light mode reveals vague fluorescence of both obvious tumor and normal appearing area under white light mode.
The phenomenon of ventricle wall 5-ALA-induced fluorescence has been well described[44] and this may serve as a confounder when operating in the brainstem/fourth ventricle.[56] In four of the six cases, in which we did enter the fourth ventricle as part of our surgical approach to the brainstem lesion, we did observe very vague fluorescence of the ventricular floor/ependyma beyond the area of solid tumor. This did not seem to correlate with the degree of tumor florescence. We did not find this to be problematic during the microsurgical resection. Given the eloquence of this area, we could not perform biopsies in this region to determine if these areas of enhancement did indeed harbor tumor cells or other reactive changes as found in the 5-ALA-induced fluorescing ependyma of the lateral ventricles.[44,50,62,82]
Unlike supratentorial malignant tumors, for which the extent of tumor resection (EOR) has a predictive value for outcome,[11,49,75,76] the goal for BSG will always be maximal safe resection, seeking a balance between GTR and postoperative neurological function.[87] We attained a GTR in 3 (37%) cases, NTR in 3 cases (37%), and STR in 2 cases (25%). In two of our cases, despite solid fluorescent tissue still visible in the surgical field, we needed to abort surgery due to abnormalities on neurophysiological monitoring. We only found the 5-ALA to be useful in 3 cases (37%) and conclude that 5-ALA is not routinely beneficial in BSG surgery. We concur with Roth and Constantini’s[62] summary that there is probably a “limited and selective role” for the use of 5-ALA in the resection of pediatric brain tumors and in particular the BSG group.
We experienced no complications due to the administration of 5-ALA. All our postoperative deficits had resolved by the 3 months follow-up, and there were no significant changes in our postoperative LPS scores. It appears that the complication rate of 5-ALA in children is very low, with isolated reports of increased transaminases being the only complication directly attributable to 5-ALA administration.[3]
Limitations
The most significant limitation to our study was the unavailability of molecular testing as molecular subtyping is more likely to be predictive of fluorescence than any other single variable.[65] In particular not being able to test for the H3K27M mutation is a significant limitation of the study given the clinical significance of a positive H3K27M mutation.
An additional limitation inherent in our methodology is the considerable interobserver variability, discrepancies, and inconsistencies demonstrated by both radiologists and pediatric neurosurgeons in diagnosing DIPGs based on MRI imaging alone.[22,23]
At present, most studies quantify intraoperative fluorescence levels subjectively and suffer from intraobserver and interobserver variability.[64] Multiple classification systems of 5-ALA fluorescence exist[32] and there is no standard of reporting on diagnostic accuracy and clinical utility.[74] A consensus on reporting is needed and the addition of quantitative spectrometric analysis or high-resolution microscopy should be considered.[36,84]
CONCLUSION
The extent of resection is an important prognostic factor[35,51,68,69] in focal BSG surgery, however, a balance between GTR and postoperative neurological function[87] must be maintained. With a combined fluorescence rate of 62.5% but a subjectively assessed “usefulness” rate of only 37.5%, the role of 5-ALA in BSG surgery is limited. Given the very low complication rate/toxicological safety of the agent, however, caution is perhaps needed before dismissing the use of 5-ALA entirely.[89] Well-designed pediatric clinical trials utilizing 5-ALA for not only BSGs but also all pediatric brain tumors are needed.
Footnotes
How to cite this article: Labuschagne J. 5-aminolevulinic Guided Surgery for Focal Pediatric Brainstem Gliomas: A Preliminary study. Surg Neurol Int 2020;11:334.
Declaration of patient consent
Institutional Review Board permission obtained for the study.
Financial support and sponsorship
Nil.
Conflicts of interest
There are no conflicts of interest.
REFERENCES
- 1.Alvisi C, Cerisoli M, Maccheroni ME. Long-term results of surgically treated brainstem gliomas. Acta Neurochir (Wien) 1985;76:12–7. doi: 10.1007/BF01403823. [DOI] [PubMed] [Google Scholar]
- 2.Barkovich AJ, Krischer J, Kun LE, Zimmerman RA, Freeman CR, Wara WM, et al. Brain stem gliomas: A classification system based on magnetic resonance imaging. Pediatr Neurosurg. 1990;91:73–83. doi: 10.1159/000120511. [DOI] [PubMed] [Google Scholar]
- 3.Beez T, Sarikay-Seiwert S, Steiger HJ, Hänggi D. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of brain tumors in children a technical report. Acta Neurosurg. 2014;156:597–604. doi: 10.1007/s00701-014-1997-9. [DOI] [PubMed] [Google Scholar]
- 4.Behnke J, Christen HJ, Mursch K, Markakis E. Intra-axial endophytic tumors in the pons and/or medulla oblongata. Childs Nerv Syst. 1997;13:135–46. doi: 10.1007/s003810050059. [DOI] [PubMed] [Google Scholar]
- 5.Bonnin DA, Havrda MC, Lee MC, Evans L, Ran C, Qian DC, et al. Characterizing the heterogeneity in 5-aminolevulinic acid-induced fluorescence in glioblastoma. J Neurosurg. 2019;1:1–9. doi: 10.3171/2019.2.JNS183128. [DOI] [PubMed] [Google Scholar]
- 6.Buczkowicz P, Bartels U, Bouffet E, Becher O, Hawkins C. Histopathological spectrum of pediatric diffuse intrinsic pontine glioma: Diagnostic and therapeutic implications. Acta Neuropathol. 2014;128:573–81. doi: 10.1007/s00401-014-1319-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Burford C, Kayal N, Pandit A, Tailor J, Lavrador J, Bravo A. PP39. 5-Aminolevulinic acid aided resection of pediatric brain tumours: The UK’s first case series. Neuro Oncol. 2017;19:i11. [Google Scholar]
- 8.Chiang J, Diaz AK, Makepeace L, Li X, Han Y, Li Y, et al. Clinical, imaging, and molecular analysis of pediatric pontine tumors lacking characteristic imaging features of DIPG. Acta Neuropathol Commun. 2020;8:57. doi: 10.1186/s40478-020-00930-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Choux M, Lena G, Do L. Brainstem tumors. In: Choux M, Di Rocco C, Hockley A, editors. Pediatric Neurosurgery. New York: Churchill Livingstone; 2000. pp. 471–91. [Google Scholar]
- 10.Constantini S, Epstein F. Surgical Indication and Technical considerations in the management of benign brain stem gliomas. J Neurooncol. 1996;28:193–205. doi: 10.1007/BF00250199. [DOI] [PubMed] [Google Scholar]
- 11.De Bonis P, Anile C, Pompucci A, Florentino A, Balducci M, Chiesa S, et al. The influence of surgery on recurrence pattern of glioblastoma. Clin Neurol Neurosurg. 2013;115:37–43. doi: 10.1016/j.clineuro.2012.04.005. [DOI] [PubMed] [Google Scholar]
- 12.Dellaretti M, Câmara BB, Ferreira PH, da Silva Júnior JB, Arantes RM. Impact of histological diagnosis on the treatment of atypical brainstem lesions. Sci Rep. 2020;10:11065. doi: 10.1038/s41598-020-68063-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Dellaretti M, Touzet G, Reyns N, Dubois F, Gusmão S, Pereira JL, et al. Correlation among magnetic resonance imaging findings, prognostic factors for survival, and histological diagnosis of intrinsic brainstem lesions in children. J Neurosurg Pediatr. 2011;8:539–43. doi: 10.3171/2011.9.PEDS1167. [DOI] [PubMed] [Google Scholar]
- 14.Epstein F, McCleary EL. Intrinsic brain-stem tumors of childhood: Surgical indications. J Neurosurg. 1986;64:11–5. doi: 10.3171/jns.1986.64.1.0011. [DOI] [PubMed] [Google Scholar]
- 15.Epstein FJ, Framer JP. Brain-stem glioma growth patterns. J Neurosurg. 1993;78:408–12. doi: 10.3171/jns.1993.78.3.0408. [DOI] [PubMed] [Google Scholar]
- 16.Ewelt C, Floeth FW, Felsberg J, Steiger HJ, Sabel M, Langen KJ, et al. Finding the anaplastic focus in diffuse gliomas: The value of Gd-DTPA enhanced MRI, FET-PET, and intraoperative, ALA-derived tissue fluorescence. Clin Neurol Neurosurg. 2011;113:541–7. doi: 10.1016/j.clineuro.2011.03.008. [DOI] [PubMed] [Google Scholar]
- 17.Fisher PG, Breiter SN, Carson BS, Wharam MD, Williams JA, Weingart JD, et al. A clinicopathologic reappraisal of brain stem tumor classification. Cancer. 2000;89:1569–76. doi: 10.1002/1097-0142(20001001)89:7<1569::aid-cncr22>3.0.co;2-0. [DOI] [PubMed] [Google Scholar]
- 18.Frazier JL, Lee J, Thomale UW, Noggle JC, Cohen KJ, Jallo GI. Treatment of diffuse intrinsic brainstem gliomas: Failed approaches and future strategies. J Neurosurg Pediatr. 2009;3:259–69. doi: 10.3171/2008.11.PEDS08281. [DOI] [PubMed] [Google Scholar]
- 19.Goryaynov SA, Widhalm G, Goldberg MF, Chelushkin D, Spallone A, Chernyshove KA, et al. The role of 5-ALA in low grade gliomas and the influence of antiepileptic drugs on intraoperative fluorescence. Front Oncol. 2019;9:1–7. doi: 10.3389/fonc.2019.00423. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Grill J, Puget S, Andreiuolo F, Philippe C, MacConaill L, Kieran MW. Critical oncogenic mutations in newly diagnosed pediatric diffuse intrinsic pontine glioma. Pediatr Blood Cancer. 2012;58:489–91. doi: 10.1002/pbc.24060. [DOI] [PubMed] [Google Scholar]
- 21.Gupta N, Goumnerova LC, Manley P, Chi SN, Neuberg D, Puligandla M, et al. Prospective feasibility and safety assessment of surgical biopsy for patients with newly diagnosed diffuse intrinsic pontine glioma. Neuro Oncol. 2018;20:1547–55. doi: 10.1093/neuonc/noy070. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hankinson TC, Campagna EJ, Foreman NK, Handler MH. Interpretation of magnetic resonance images in diffuse intrinsic pontine glioma: A survey of pediatric neurosurgeons. J Neurosurg Pediatr. 2011;8:97–102. doi: 10.3171/2011.4.PEDS1180. [DOI] [PubMed] [Google Scholar]
- 23.Hayward RM, Patronas N, Baker EH, Vézina G, Albert PS, Warren KE. Inter-observer variability in the measurement of diffuse intrinsic pontine gliomas. J Neurooncol. 2008;90:57–61. doi: 10.1007/s11060-008-9631-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24.Hefti M, Albert I, Luginbuelli V. Phenytoin reduces 5-aminolevulinic acid-induced protoporphyrin IX accumulation in malignant glioma cells. J Neurooncol. 2012;108:443–50. doi: 10.1007/s11060-012-0857-9. [DOI] [PubMed] [Google Scholar]
- 25.Hoffman HJ, Becker L, Craven MA. A clinically and pathologically distinct group of benign brain stem gliomas. Neurosurgery. 1980;7:243–8. doi: 10.1227/00006123-198009000-00007. [DOI] [PubMed] [Google Scholar]
- 26.Huang T, Garcia R, Qi J, Lulla R, Horbinski C, Behdad A, et al. Detection of histone H3 K27M mutation and post-translational modifications in pediatric diffuse midline glioma via tissue immunohistochemistry informs diagnosis and clinical outcomes. Oncotarget. 2018;9:37112–24. doi: 10.18632/oncotarget.26430. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Infinger LK, Stevenson CB. Re-examining the need for tissue diagnosis in pediatric diffuse intrinsic pontine gliomas: A review. Curr Neuropharmacol. 2017;15:129–33. doi: 10.2174/1570159X14666160425114024. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Ishihara R, Katayama Y, Watanabe T, Yoshino A, Fukushima T, Sakatani K. Quantitative spectroscopic analysis of 5 aminolevulinic acid induced protoporphyrin IX fluorescence intensity in diffusely infiltration astrocytomas. Neurol Med Chir. 2007;47:53–7. doi: 10.2176/nmc.47.53. [DOI] [PubMed] [Google Scholar]
- 29.Jaber M, Wölfer J, Ewelt C, Holling M, Hasselblatt M, Niederstadt T, et al. The value of 5-aminolevulinic acid in low-grade gliomas and high-grade gliomas lacking glioblastoma imaging features: An analysis based on fluorescence, magnetic resonance imaging, 18F-fluoroethyl tyrosine positron emission tomography, and tumor molecular factors. Neurosurgery. 2016;78:401–11. doi: 10.1227/NEU.0000000000001020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Jallo GI, Biser-Rohrbaugh A, Freed D. Brainstem gliomas. Childs Nerv Syst. 2004;20:143–53. doi: 10.1007/s00381-003-0870-6. [DOI] [PubMed] [Google Scholar]
- 31.Kamp MA, Grosser P, Felsberg J. 5-Aminolevulinic acid (5-ALA) induced fluorescence in intracerebral metastases: A retrospective study. Acta Neurochir. 2012;154:223–8. doi: 10.1007/s00701-011-1200-5. [DOI] [PubMed] [Google Scholar]
- 32.Kamp MA, Molle ZK, Munoz-Bendix C, Rapp M, Sabel M, Steiger HJ, et al. Various shades of red-A systematic analysis of qualitative estimation of ALA derived fluorescence in neurosurgery. Neurosurg Rev. 2018;41:3–18. doi: 10.1007/s10143-016-0745-4. [DOI] [PubMed] [Google Scholar]
- 33.Kaplan AM, Albright L, Zimmerman RA, Rorke LB, Li H, Moyett JM, et al. Brainstem gliomas in children. Pediatr Neurosurg. 1996;24:185–92. doi: 10.1159/000121036. [DOI] [PubMed] [Google Scholar]
- 34.Karremann M, Gielen GH, Hoffmann M, Wiese M, Colditz N, Warmuth-Metz M, et al. Diffuse high-grade gliomas with H3 K27M mutations carry a dismal prognosis independent of tumor location. Neuro Oncol. 2018;20:123–31. doi: 10.1093/neuonc/nox149. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Kestle J, Townsend JJ, Brockmeyer DL, Walker ML. Juvenile pilocytic astrocytoma of the brainstem in children. J Neurosurg Pediatr. 2014;101:1–6. doi: 10.3171/ped.2004.101.2.0001. [DOI] [PubMed] [Google Scholar]
- 36.Kim A, Khurana M, Moriyama Y, Wilson BC. Quantification of in vivo fluorescence decoupled from the effects of tissue optical properties using fiber-optic spectroscopy measurements. J Biomed Opt. 2010;15:067006. doi: 10.1117/1.3523616. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37.Klimo P, Nesvick CL, Broniscer A, Orr BA, Choudhri AF. Malignant brainstem tumors in children, excluding diffuse intrinsic pontine gliomas. J Neurosurg Pediatr. 2016;17:57–65. doi: 10.3171/2015.6.PEDS15166. [DOI] [PubMed] [Google Scholar]
- 38.Klimo P, Panandiker AS, Thompson CJ, Boop FA, Qaddoumi I, Gajjar A, et al. Management and outcome of focal low-grade brainstem tumors in pediatric patients: The St. Jude experience. J Neurosurg Pediatr. 2013;11:274–81. doi: 10.3171/2012.11.PEDS12317. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Lansky SB, List MA, Lanskey LL, Ritter-Sterr C, Miller DR. The measurement of performance in childhood cancer patients. Cancer. 1987;60:1651–6. doi: 10.1002/1097-0142(19871001)60:7<1651::aid-cncr2820600738>3.0.co;2-j. [DOI] [PubMed] [Google Scholar]
- 40.Lawrence JE, Steele CJ, Rovin RA, Belton RJ, Winn RJ. Dexamethasone alone and in combination with desipramine, phenytoin, valproic acid or levetiracetam interferes with 5 ALA mediated PpIX production and cellular retention in glioblastoma cells. J Neurooncol. 2016;127:15–21. doi: 10.1007/s11060-015-2012-x. [DOI] [PubMed] [Google Scholar]
- 41.Marbacher S, Klinger E, Schwyzer L, Fischer I, Nevzati E, Diepers M, et al. Use of fluorescence to guide resection or biopsy of primary brain tumors and brain metastases. Neurosurg Focus. 2014;36:1–10. doi: 10.3171/2013.12.FOCUS13464. [DOI] [PubMed] [Google Scholar]
- 42.Mauffrey C. Paediatric brainstem gliomas: Prognostic factors and management. J Clin Neurosci. 2006;13:431–7. doi: 10.1016/j.jocn.2005.05.015. [DOI] [PubMed] [Google Scholar]
- 43.Mehta VS, Chandra PS, Singh PK, Garg A, Rath GK. Surgical considerations for. “intrinsic” brainstem gliomas: Proposal of a modification in classification. Neurology India. 2009;57:274–81. doi: 10.4103/0028-3886.53272. [DOI] [PubMed] [Google Scholar]
- 44.Moon JH, Kim SH, Shim JK, Roh TH, Sung KS, Lee J. Histopathological implications of ventricle wall 5-aminolevulinic acid-induced fluorescence in the absence of tumor involvement on magnetic resonance images. Oncol Rep. 2016;36:837–44. doi: 10.3892/or.2016.4881. [DOI] [PubMed] [Google Scholar]
- 45.Moreno RG, García LM, Bastidas HI, Tirado CA, Flores AM, et al. Fluorescence guided surgery with 5-aminolevulinic acid for resection of spinal cord ependymomas. Asian Spine J. 2019;13:119–25. doi: 10.31616/asj.2018.0165. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Morshed RA, Han SJ, Lau D, Berger MS. Wavelength-specific lighted suction instrumentation for 5-aminolevulinic acid fluorescence-guided resection of deep-seated malignant glioma: Technical note. J Neurosurg. 2018;128:1448–53. doi: 10.3171/2017.1.JNS161949. [DOI] [PubMed] [Google Scholar]
- 47.Motekallemi A, Jeltema HR, Metzemaekers JD, Van Dam GM, Crane LM, Groen RJ. The current status of 5-ALA fluorescence-guided resection of intracranial meningiomas a critical review. Neurosurg Rev. 2015;38:619–28. doi: 10.1007/s10143-015-0615-5. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 48.Ogiwara H, Morota N. The efficacy of a biopsy of intrinsic brainstem lesions for decision making of the treatments. Childs Nerv Syst. 2013;29:833–7. doi: 10.1007/s00381-013-2042-7. [DOI] [PubMed] [Google Scholar]
- 49.Orringer D, Lau D, Khatri S, Zamora-Berridi GJ, Zhang K, Wu C, et al. Extent of Resection in patients with glioblastoma: Limiting factors, perception of resectability, and effect of survival. J Neurosurg. 2012;117:851–9. doi: 10.3171/2012.8.JNS12234. [DOI] [PubMed] [Google Scholar]
- 50.Piccirillo SG, Spiteri I, Sottoriva A, Touloumis A, Ber S, Price SJ, Heywood R, et al. Contributions to drug resistance in glioblastoma derived from malignant cells in the subependymal zone. Cancer Res. 2015;75:194–202. doi: 10.1158/0008-5472.CAN-13-3131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Pierre-Kahn A, Hirsch JF, Vinchon MD, Rayan C, Saint-Rose C, Renier D, et al. Surgical management of brain-stem tumors in children results and statistical analysis of 75 cases. J Neurosurg. 1993;79:845–52. doi: 10.3171/jns.1993.79.6.0845. [DOI] [PubMed] [Google Scholar]
- 52.Pincus DW, Richter EO, Yachnis AT, Bennett J, Bhatti MT, Smith A. Brainstem stereotactic biopsy sampling in children. J Neurosurg. 2006;104:108–14. doi: 10.3171/ped.2006.104.2.108. [DOI] [PubMed] [Google Scholar]
- 53.Pollack IF, Hoffman HJ, Humphreys RP, Becker L. The long-term outcome after surgical treatment of dorsally exophytic brain-stem gliomas. J Neurosurg. 1993;78:859–63. doi: 10.3171/jns.1993.78.6.0859. [DOI] [PubMed] [Google Scholar]
- 54.Preuß M, Renner C, Krupp W, Christiansen H, Fischer L, Merkenschlager A, et al. The use of 5 aminolevulinic acid fluorescence guidance in resection of pediatric brain tumors. Childs Nerv Syst. 2013;29:1263–7. doi: 10.1007/s00381-013-2159-8. [DOI] [PubMed] [Google Scholar]
- 55.Puppa AD, Rustemi O, Gioffré G, Scienza R. Approaching a brainstem high-grade glioma (HGG) with the assistance of 5-aminolevulinic acid (5-ALA) technology: A new strategy for an old surgical challenge. Neurol Sci. 2014;36:797–9. doi: 10.1007/s10072-014-1901-7. [DOI] [PubMed] [Google Scholar]
- 56.Puppa AD, Rustemi O, Gioffrè G, Troncon I, Lombardi G, Rolma G, et al. Predictive value of intraoperative 5-aminolevulinic acid-induced fluorescence for detecting bone invasion in meningioma surgery. J Neurosurg. 2014;120:840–5. doi: 10.3171/2013.12.JNS131642. [DOI] [PubMed] [Google Scholar]
- 57.Rachinger W, Grau S, Holtmannspötter M, Herms J, Tonn JC, Kreth FW. Serial stereotactic biopsy of brainstem lesions in adults improves diagnostic accuracy compared with MRI only. J Neurol Neurosurg Psychiatry. 2009;80:1134–9. doi: 10.1136/jnnp.2009.174250. [DOI] [PubMed] [Google Scholar]
- 58.Rapp M, Kamp M, Steiger HJ, Sabel M. Endoscopic-assisted visualization of 5 aminolevulinic acid induced fluorescence in malignant glioma surgery: A technical note. World Neurosurg. 2014;82:1–3. doi: 10.1016/j.wneu.2013.07.002. [DOI] [PubMed] [Google Scholar]
- 59.Recinos PF, Sciubba DM, Jallo GI. Brainstem tumors: Where are we today? Pediatr Neurosurg. 2007;43:192–201. doi: 10.1159/000098831. [DOI] [PubMed] [Google Scholar]
- 60.Ritz R, Feigl GC, Schuhmann MU, Ehrhardt A, Danz S, Noell S, et al. Use of 5-ALA fluorescence guided endoscopic biopsy of a deep-seated primary malignant brain tumor. J Neurosurg. 2011;114:1410–3. doi: 10.3171/2010.11.JNS10250. [DOI] [PubMed] [Google Scholar]
- 61.Ritz R, Scheidle C, Noell S, Roser F, Schenk M, Dietz K, et al. In vitro comparison of hypericin and 5-aminolevulinic acid-derived protoporphyrin IX for photodynamic inactivation of medulloblastoma cells. PLoS One. 2012;7:e51974. doi: 10.1371/journal.pone.0051974. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 62.Roberts DW, Valdés PA, Harris BT, Fontaine KM, Hartov A, Fan X, et al. Coregistered fluorescence-enhanced tumor resection of malignant glioma: Relationships between 5-aminolevulinic acid induced protoporphyrin IX Fluorescence, magnetic resonance imaging enhancement, and neuropathological parameters. J Neurosurg. 2011;114:595–603. doi: 10.3171/2010.2.JNS091322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 63.Robertson PL, Allen JC, Abbott IR, Miller DC, Fidel J, Epstein FJ. Cervicomedullary tumors in children: A distinct subset of brainstem gliomas. Neurology. 1994;44:1798–803. doi: 10.1212/wnl.44.10.1798. [DOI] [PubMed] [Google Scholar]
- 64.Roth J, Constantini S. 5ALA in pediatric brain tumors is not routinely beneficial. Childs Nerv Syst. 2017:850–9. doi: 10.1007/s00381-017-3371-8. [DOI] [PubMed] [Google Scholar]
- 65.Saito K, Hirai T, Takeshima H, Kadota Y, Yamashita S, Ivanova A, et al. Genetic factors affecting intraoperative 5-aminolevulinic acid-induced fluorescence of diffuse gliomas. Radiol Oncol. 2017;51:142–50. doi: 10.1515/raon-2017-0019. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66.Samkoe KS, Gibbs-Strauss SL, Yang HH, Hekmatyar SK, Hoopes PJ, et al. Protoporphyrin IX Fluorescence contrast in invasive glioblastomas is linearly correlated with Gd enhanced magnetic resonance image contrast but has diagnostic accuracy. J Biomed Opt. 2011;16:096008. doi: 10.1117/1.3622754. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Sanai N, Snyder LA, Honea NJ, Coons SW, Eschbacher JM, Smith KA. Intraoperative confocal microscopy in the visualization of 5-aminolevulinic acid fluorescence in low-grade gliomas. J Neurosurg. 2011;115:740–8. doi: 10.3171/2011.6.JNS11252. [DOI] [PubMed] [Google Scholar]
- 68.Sandri A, Sardi N, Genitori L, Peretta P, Basson ME, Bertin D, et al. Diffuse and focal brain stem tumors in childhood: Prognostic factors and surgical outcome. Childs Nerv Syst. 2006;22:1127–35. doi: 10.1007/s00381-006-0083-x. [DOI] [PubMed] [Google Scholar]
- 69.Schild SE, Stafford SL, Brown PD, Wood CP, Scheithauer BW, Schomberg PJ, et al. The results of radiotherapy for brainstem tumors. J Neurooncol. 1998;40:171–7. doi: 10.1023/a:1006193306286. [DOI] [PubMed] [Google Scholar]
- 70.Schwake M, Günes D, Köchling M, Brentrup A. Kinetics of porphyrin fluorescence accumulation in pediatric brain tumor cells incubated in 5-aminolevulinic acid. Acta Neurochir (Wien) 2014;156:1077–84. doi: 10.1007/s00701-014-2096-7. [DOI] [PubMed] [Google Scholar]
- 71.Schwake M, Nemes A, Dondrop J, Schroeteler J, Schipmann S, Senner V, et al. In-vitro use of 5-ALA for photodynamic therapy in pediatric brain tumors. Neurosurgery. 2018;83:1328–37. doi: 10.1093/neuros/nyy054. [DOI] [PubMed] [Google Scholar]
- 72.Schwake M, Schipmann S, Müther M, Köchling M, Brentrup A, Stummer W. 5-ALA fluorescence-guided surgery in pediatric brain tumors a systematic review. Acta Neurochir. 2019;161:1099–108. doi: 10.1007/s00701-019-03898-1. [DOI] [PubMed] [Google Scholar]
- 73.Stroink AR, Harold MD, Hoffman J, Hendrick EB, Humphreys RP. Diagnosis and management of pediatric brainstem gliomas. J Neurosurg. 1986;65:745–50. doi: 10.3171/jns.1986.65.6.0745. [DOI] [PubMed] [Google Scholar]
- 74.Stummer W, Koch R, Valle RD, Roberts DW, Sanai N, Kalkanis S, et al. Intraoperative fluorescence diagnosis in the brain: A systematic review and suggestions for future standards on reporting diagnostic accuracy and clinical utility. Acta Neurochir (Wien) 2019;161:2083–98. doi: 10.1007/s00701-019-04007-y. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 75.Stummer W, Novotny A, Stepp H, Goetz C, Bise K, Reulen HJ. Fluorescence-guided resection of glioblastoma multiforme by using 5-aminolevulinic acid induced porphyrins: A prospective study in 52 consecutive patients. J Neurosurg. 2000;93:1003–13. doi: 10.3171/jns.2000.93.6.1003. [DOI] [PubMed] [Google Scholar]
- 76.Stummer W, Pichlmeier U, Meinel T, Wiestler OD, Zanella F, Reulan HJ, et al. Fluorescence-guided surgery with 5-aminolevulinic acid for resection of malignant glioma: A randomized controlled multicentre phase III trial. Lancet Oncol. 2006;7:392–401. doi: 10.1016/S1470-2045(06)70665-9. [DOI] [PubMed] [Google Scholar]
- 77.Stummer W, Rodriques F, Schucht P, Preuss M, Wiewrodt D, Nestler U, et al. Predicting the “usefulness” of 5-ALA derived tumor fluorescence for fluorescence guided resections in pediatric brain tumors: A European survey. Acta Neurochir. 2014;156:2315–24. doi: 10.1007/s00701-014-2234-2. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Stummer W, Tonn JC, Goetz C, Ullrich W, Stepp H, Bink A. 5 aminolevulinic acid derived tumor fluorescence: The diagnostic accuracy of visible fluorescence qualities as corroborated by spectrometry and histology and postoperative imaging. Neurosurgery. 2014;74:310–20. doi: 10.1227/NEU.0000000000000267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 79.Tejada S, Aquilina K, Goodden J, Pettorini B, Mallucci C, van Veelen ML, et al. Biopsy in diffuse pontine gliomas: Expert neurosurgeon opinion-a survey from the SIOPE brain tumor group. Childs Nerv Syst. 2020;36:705–11. doi: 10.1007/s00381-020-04523-8. [DOI] [PubMed] [Google Scholar]
- 80.Teo C, Siu TL. Radical resection of focal brainstem gliomas: Is it worth doing? Childs Nerv Syst. 2008;24:1307–14. doi: 10.1007/s00381-008-0647-z. [DOI] [PubMed] [Google Scholar]
- 81.Tomita T, McLone DG, Naidich TP. Brain stem gliomas in childhood. J Neuro Oncol. 1984;2:117–22. doi: 10.1007/BF00177896. [DOI] [PubMed] [Google Scholar]
- 82.Utsuki S, Oka H, Sato S, Shimizu S, Suzuki S, Tanizaki Y, et al. Histological examination of false positive tissue resection using 5 aminolevulinic acid-induced fluorescence guidance. Neurol Med Chir. 2007;47:210–4. doi: 10.2176/nmc.47.210. [DOI] [PubMed] [Google Scholar]
- 83.Valés PA, Jacobs V, Harris BT, Wilson BC, Leblond F, Paulson KD, et al. Quantitative fluorescence using 5-aminolevulinic acid induced protoporphyrin IX biomarker as a surgical adjunct in low-grade glioma surgery. J Neurosurg. 2015;123:771–80. doi: 10.3171/2014.12.JNS14391. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 84.Wei L, Fujita Y, Sanai N, Liu JT. Toward quantitative neurosurgical guidance with high-resolution microscopy of 5-aminolevulinic acid-induced protoporphyrin IX. Front Oncol. 2019;9:592. doi: 10.3389/fonc.2019.00592. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 85.Weiner HL, Freed D, Woo HH, Rezai AR, Kim R, Epstein FJ. Intra-axial tumors of the cervicomedullary junction: Surgical results and long term outcome. Pediatr Neurosurg. 1997;27:12–8. doi: 10.1159/000121219. [DOI] [PubMed] [Google Scholar]
- 86.Widhalm G, Kiesel B, Weshrer A, Weldinger TT, Preusser M, Marosi C, et al. 5-aminolevulinic acid induced fluorescence is a powerful intraoperative marker for precise histopathological grading of gliomas with non-significant contrast enhancement. PLoS One. 2013;8:1–8. doi: 10.1371/journal.pone.0076988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Xue Z, Kong L, Pan C, Wu Z, Zhang J, Zhang L. Fluorescein-guided surgery for pediatric brainstem gliomas: Preliminary study and technical notes. J Neurol Surg B. 2018;79:340–6. doi: 10.1055/s-0038-1660847. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 88.Yin L, Zhang L. Correlation between MRI findings and histological diagnosis of brainstem glioma. Can J Neurol Sci. 2013;40:348–54. doi: 10.1017/s0317167100014293. [DOI] [PubMed] [Google Scholar]
- 89.Zhang C, Boop FA, Ruge J. The use of 5-aminolevulinic acid in resection of pediatric brain tumors: A critical review. J Neurooncol. 2019;141:567–73. doi: 10.1007/s11060-018-03004-y. [DOI] [PubMed] [Google Scholar]