

Abstract
Large and persistent obesity disparities exist in the US by socioeconomic status (SES) and race/ethnicity, and weight loss interventions have traditionally been less effective in these populations. Thus, a better understanding is needed of the behavioral, economic, and geographic factors that influence obesity risk factors such as eating behaviors. We used a discrete choice experiment to evaluate the impact of different meal attributes on meal choice and to test whether the relative importance of these attributes varied by SES and race/ethnicity. Study participants (n=228) were given a series of 10 choice tasks and asked to choose among 4 meals, each rated based on the following attributes: taste; healthfulness; preparation time; travel time to food outlet for meal/ingredients; and price. SES was measured using education and self-reported difficulty paying for basics. Race/ethnicity was categorized as Hispanic/Latina, non-Hispanic black, non-Hispanic white, and non-Hispanic other. Data were analyzed using mixed logit regression models with interaction terms to determine whether meal attributes influenced meal choices differentially by SES and race/ethnicity. Healthfulness and taste were the most important attributes for all participants. Price was a more important attribute among those in the lowest SES group compared with those in the higher SES groups. Travel was the least important attribute for low SES participants, and it was not significantly related to meal choice in these groups. Discrete choice experiments as illustrated here may help pinpoint the most salient targets for interventions to improve eating behaviors and reduce obesity disparities. Specifically, our findings suggest interventions should incorporate strategies to target the pricing of healthy and unhealthy food options.
Keywords: socioeconomic status, race/ethnicity, discrete choice experiment, diet
Introduction
The limited success of education programs and behavioral interventions to improve healthy eating in low-income and minority populations (Fitzgibbon et al., 2012; Lindberg & Stevens, 2007; Lindberg, Stevens, & Halperin, 2013; Tussing-Humphreys, Fitzgibbon, Kong, & Odoms-Young, 2013) has prompted an increased interest in the role of the food environment. In particular, lower access to healthy foods in minority and low-income neighborhoods is believed to be a major contributor to the persistent disparities seen in diet and obesity in the US (Walker, Keane, & Burke, 2010). As such, increasing geographic access to healthy foods has been a national and local goal of numerous public and private initiatives in the US (Block & Subramanian, 2015).
However, evidence from several recent evaluations of these initiatives suggests increasing geographic access alone may be insufficient to promote healthful behavior change. A number of studies have compared food shopping and eating behaviors of individuals living in two neighborhoods without a supermarket before and after one of the neighborhoods gets one, with mixed results. Two studies evaluated the same new supermarket that opened in the Bronx, NY. One focused on children and found no significant differences in household food availability or dietary intake between the two neighborhoods under study (Elbel et al., 2015). The other focused on adults and found increased availability of both healthy and unhealthy foods in the neighborhood where the new supermarket was introduced, but also greater consumption of healthy foods coupled with lower consumption of unhealthy foods (Rogus, Athens, Cantor, & Elbel, 2017). A study in Philadelphia, PA found significant increases in perceived healthy food access but not in diet (Cummins, Flint, & Matthews, 2014), while a Pittsburgh, PA study found improvements in diet but not due to use of the supermarket (Dubowitz, Ghosh-Dastidar, et al., 2015). These largely null findings suggest a better understanding of the relative importance of geographic access and other characteristics related to meal choices is vital for the development of more effective diet interventions, particularly in low-socioeconomic status (SES) and racial/ethnic minority populations who carry the larger burden of obesity.
One way to capture this type of information is through a discrete choice experiment. Discrete choice experiments are attribute-based approaches to collecting data on a participant’s stated preferences. This approach is appealing because it allows for an assessment of the relative importance of different characteristics, or attributes, of meals without directly asking participants to rank them. The technique was developed in marketing and has been applied in a growing number of health care studies to assess various health policy-related issues (de Bekker-Grob, Ryan, & Gerard, 2012). Discrete choice experiments have the potential to inform interventions designed to reduce disparities in eating behaviors and obesity by assessing variation in preferences by factors like race/ethnicity and SES. However, while several discrete choice experiments have examined attributes that influence meal selections in a restaurant setting (Clemes, Gan, & Sriwongrat, 2013; Jeffries, Lee, Frick, & Gittelsohn, 2013; Kim, Lee, & Yoon, 2012; Myung, McCool, & Feinstein, 2008; Stierand & Wood, 2012), few have assessed factors that influence eating behaviors more broadly (Kamphuis, de Bekker-Grob, & van Lenthe, 2015). Thus, the goal of this study was to determine the relative influence of different meal attributes (taste, healthfulness, price, preparation time, and travel time to buy meal/ingredients) on meal choices and to assess whether the impact of these attributes varied by SES and race/ethnicity.
Materials and methods
Study population
Data for this study came from the Chicago Healthy Eating Environments and Resources Study (CHEERS). The goal of CHEERS is to understand how women of childbearing age use their environments, knowledge, and each other to make eating decisions. Non-proportional quota sampling was used to recruit 228 women aged 18–44 years from four racially, ethnically, and socioeconomically diverse Chicago neighborhoods. Recruitment methods included mailings using commercially available address lists, flyers posted in stores located in the four neighborhoods, and presentations to parent organizations at schools in the target neighborhoods. The study was restricted to women ages 18–44 who could understand Spanish or English. The study focused on women based on the large racial/ethnic obesity disparities that exist in women and the fact that women are often responsible for the food preparation and purchasing for their families. The study focused on this age group because it is a critical period of increased weight due to various factors including post-pregnancy weight retention and declining muscle mass and muscle strength (Doherty, 2001).
All participants provided informed consent. The study was approved by the Northwestern University Feinberg School of Medicine Institutional Review Board (study number STU00203035).
Study design
Participants completed a 1.5 hour in-person examination that included completing questionnaires, having physical measurements taken, and giving a small blood sample. They were paid $40 for their participation. During the visit, a discrete choice experiment was used to evaluate individual preferences that influence meal choices. Participants were given a series of 10 choice tasks. In each choice task, they were asked to select from 4 hypothetical meals rated based on a sample of all possible combinations of the following attributes: taste (very good, good, or OK); healthfulness (healthy, neutral, or unhealthy); preparation time (0, 15, 30, or 45 minutes); travel time to food outlet for meal/ingredients (5, 10, 20, or 30 minutes); and price ($2, $4, $6, or $8 per person). These attributes were selected a priori because they are all hypothesized to contribute to disparities in healthy eating behaviors (Aggarwal, Rehm, Monsivais, & Drewnowski, 2016; Darmon & Drewnowski, 2015; Dubowitz, Zenk, et al., 2015; Glanz, Basil, Maibach, Goldberg, & Snyder, 1998).
Participants were asked to consider all of the attributes and choose the meal they would prefer. They were also given the option of choosing none of the meals. Including this no-choice option rather than forcing participants to select from the available alternatives may improve the accuracy of our estimates, but it could limit our ability to answer our proposed research questions if too many people selecting this option in terms of answering the research question (Hensher, Rose, & Greene, 2015). The latter does not appear to be a concern in this study as participants selected the no-choice option for less than 10% of all choice sets (n=22 out of 2,280 choice tasks).
There are substantially more possible combinations of attributes than the 40 that were included in this discrete choice experiment, so we used the previously developed %choicEff SAS macro to use a D-efficient design to generate the optimal sample of alternatives to present to participants (Kuhfeld, 2010). The optimal choice set design was generated based on the following criteria: D-efficiency equals the number of choice sets (D-efficiency=9.6 for this choice set); D-error equals 1 / the number of choice sets (D-error=0.10); all of the variances equal 1 / the number of choice sets (variance ranged from 0.10–0.11); all of the covariances are 0 (covariances all ≤0.01); and the relative D-efficiency equals 100 (D-efficiency=96.4). Figure 1 shows an example choice task.
Figure 1:
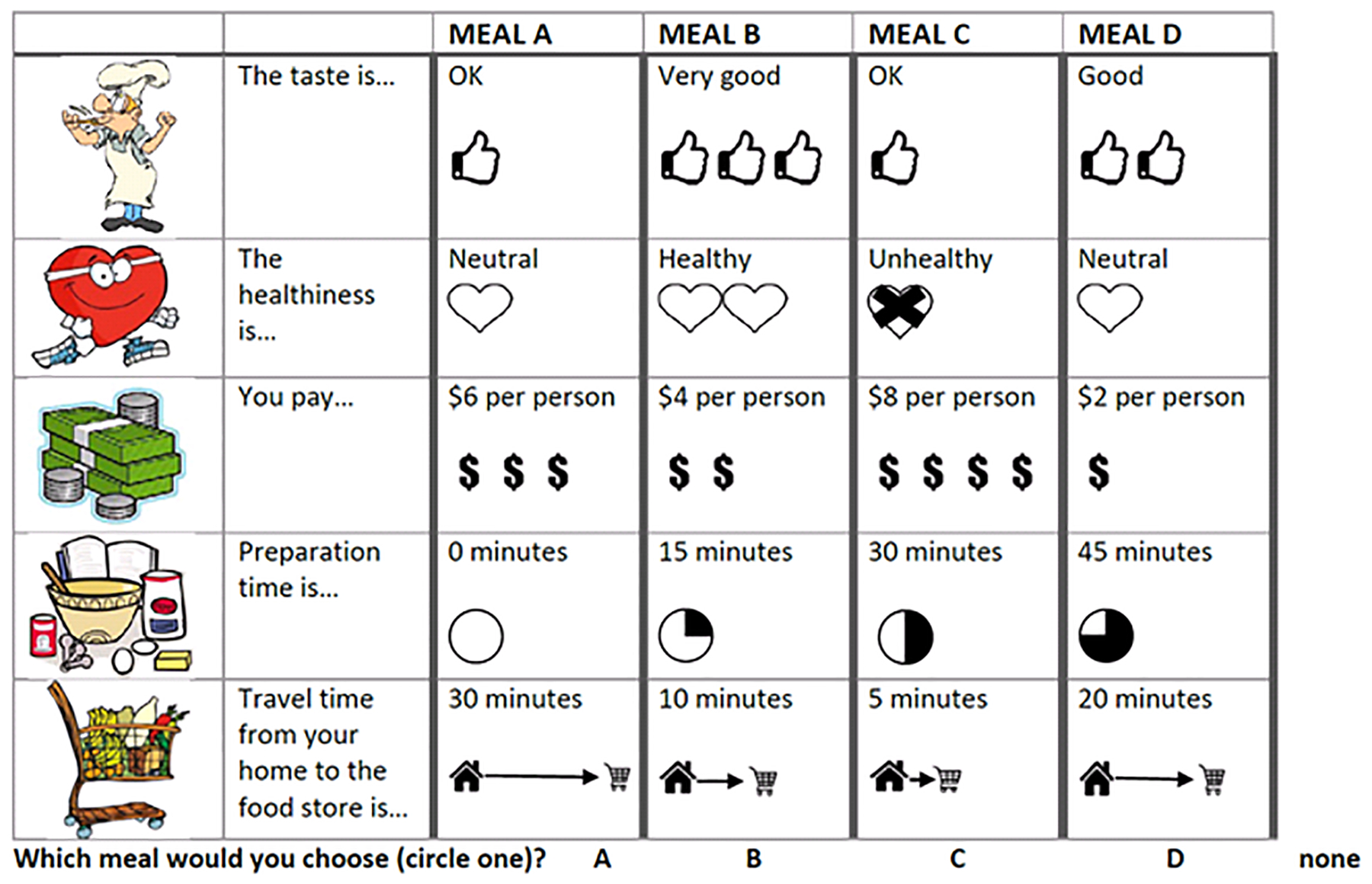
Example of a choice task administered to Chicago Healthy Eating Environments and Resources (CHEERS) study participants
Sociodemographic characteristics
Race/ethnicity was categorized as Hispanic/Latina, non-Hispanic white, non-Hispanic black, and non-Hispanic Asian/Pacific Islander/other. Education was defined as highest level completed and categorized as high school or less, some college or associate’s degree, and bachelor’s degree or higher. Financial burden was assessed by asking participants a single question on how difficult it was to pay for basics like food and heating (Matthews et al., 2002). Options ranged from very hard to not hard at all and were categorized as high (hard or very hard), medium (somewhat hard), and low (not hard at all).
Statistical analyses
Descriptive characteristics of CHEERS participants were generated using SAS 9.4 (SAS Institute; Cary, NC). The discrete choice data were analyzed using mixed logit models to account for within-subject correlation and unobserved preference heterogeneity. Models were estimated using NLogit 6.0 software (Econometric Software, Inc.; Plainview, NY). Taste and healthfulness were modeled as categorical variables with dummy coding. Price, preparation time, and travel time were modeled as a continuous variables. (Hauber et al., 2016)All attributes were included as random parameters. Random parameters were obtained from 100 repeated, Halton intelligent simulation draws using a normal distribution. Intelligent simulation draws reduce the computation time needed to achieve model convergence (compared to random draws) while maintaining the accuracy of the model results (Hensher et al., 2015). An alternative specific constant was added to the model to account for the no-choice option.
Relative attribute importance proportions were also calculated to provide an indicator of which attributes were most important for participants (Louviere, Hensher, Swait, & Adamowicz, 2000). An estimate of the proportion of a participant’s preference for each attribute was calculated by dividing the difference in utility between the highest and lowest level of that attribute by the sum of the differences in utility of all attributes. The estimate for the highest level of the attribute was generated by running a model with all attributes included as categorical variables.
Variation in mean preference coefficients by race/ethnicity and SES were evaluated by using the ;rpl command line in Nlogit to include and test interactions of these factors with each attribute. Interactions with race/ethnicity and SES were first tested individually and then together in a single model. The main effect estimates and interaction terms were used to generate race/ethnicity and SES-specific preference estimates. The relative importance of each attribute by SES and race/ethnicity was calculated as well, using the approach described above. Interactions of the “other” race/ethnic group with the meal attributes were tested in the models but they are not presented in the table because the group is very small.
Results
The mean age of study participants was 33.9 years (Table 1). Nearly half of the participants were Latina, and another 15% were non-Hispanic blacks. Around 15% of participants fell in the high financial burden category, and 36% had a high school degree or less.
Table 1:
Descriptive characteristics of Chicago Healthy Eating Environments and Resources Study (CHEERS) participants
| Participants (n=228) | |
|---|---|
| Age, years (SD) | 33.9 (7.0) |
| Race/ethnicitya, % | |
| Hispanic/Latina | 48.7 |
| Non-Hispanic White | 35.1 |
| Non-Hispanic Black | 14.9 |
| Non-Hispanic Asian, Pacific Islander, or Other | 1.3 |
| Education, % | |
| High school or less | 36.0 |
| Some college or associate’s degree | 15.8 |
| Bachelor’s degree or higher | 48.2 |
| Financial burdena, % | |
| High | 15.4 |
| Medium | 33.3 |
| Low | 51.3 |
Financial burden is defined based on the extent to which participants report having difficulty paying for basics like food and heating: high=hard or very hard; medium=somewhat hard; low=not hard at all
All attributes were significantly associated with meal choice (Table 2; log likelihood = −2286.8, K=15; pseudo R2=0.38). These relationships were all in the expected direction. Very good tasting meals were significantly more preferable to participants than OK meals (mean=1.16; 95% confidence interval (CI)=0.97, 1.34), and healthy meals were more preferable than unhealthy ones (mean=2.35; 95% CI=2.12, 2.58). Participants also preferred meals that were less expensive (mean=−0.18; 95% CI=−0.24, −0.12), and those that required shorter preparation times (mean=−0.20; 95% CI=−0.26, −0.15) and travel times (mean=−0.14; 95% CI=−0.20, −0.09). The calculation of relative importance revealed that healthfulness was the most important attribute, followed by taste and preparation time. The standard deviation preference estimates were significant for price and travel time, suggesting there was significant preference heterogeneity around those means. Table 3 (log likelihood = −2152.6, K=29; pseudo R2=0.41) shows mean preference estimates and relative attribute importance proportions by education level. The preference estimates for taste and healthfulness were significantly weaker among participants with less than a bachelor’s degree, but those were still the most important two attributes for all three education categories. The other three attributes had similar relative importance proportions for participants with some college or associate’s degree and those with a bachelor’s degree or higher, but there were notable differences between those two groups and the participants with a high school degree or less. Specifically, price was a more important attribute to participants with a high school degree or less than those with a bachelor’s degree or more. In addition, the preference estimates for preparation time and travel time were not significant for participants in the lowest education category.
Table 2:
Mixed logit model for Chicago Healthy Eating Environments and Resources (CHEERS) participant meal preferences
| Attribute | Preference estimates | Relative attribute importancea | ||
|---|---|---|---|---|
| Taste | Coefficient | 95% CI | 23.3% | |
| Very good | Mean | 1.16b | (0.97, 1.34) | |
| SD | 0.02 | (−0.59, 0.63) | ||
| Good | Mean | 0.52b | (0.35, 0.68) | |
| SD | 0.15 | (−0.70, 1.00) | ||
| OK | Mean | Reference | ||
| SD | Reference | |||
| Healthiness | 48.6% | |||
| Healthy | Mean | 2.35b | (2.12, 2.58) | |
| SD | 0.02 | (−0.55, 0.59) | ||
| Neutral | Mean | 1.53b | (1.34, 1.72) | |
| SD | 0.06 | (−0.57, 0.69) | ||
| Unhealthy | Mean | Reference | ||
| SD | Reference | |||
| Price | 9.3% | |||
| $2 increase | Mean | −0.18b | (−0.24, −0.12) | |
| SD | 0.26b | (0.01, 0.51) | ||
| Preparation time | 13.1% | |||
| 15 minute increase | Mean | −0.20b | (−0.26, −0.15) | |
| SD | 0.04 | (−0.26, 0.35) | ||
| Travel time | 5.7% | |||
| 5–10 minute increase | Mean | −0.14b | (−0.20, −0.09) | |
| SD | 0.25b | (0.004, 0.49) | ||
| Constant | Mean | −3.23b | (−4.02, −2.44) | |
Relative attribute importance was calculated by dividing the difference in utility between the highest and lowest level of a single attribute by the sum of the differences of all attributes
Attributes or attribute levels with this superscript had a significant impact on meal preferen
Table 3:
Mixed logit model for Chicago Healthy Eating Environments and Resources (CHEERS) participant mean meal preference estimates by level of education
| Attribute | HS or less | Some college | Bachelor’s degree or more | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% CI | Relative attribute importancea | Coefficient | 95% CI | Relative attribute importancea | Coefficient | 95% CI | Relative attribute importancea | |
| Taste | 27.0% | 19.0% | 23.5% | ||||||
| Very good | 0.78b,c | (0.56, 1.00) | 0.79b,c | (0.48, 1.09) | 1.94b | (1.59, 2.28) | |||
| Good | 0.05c | (−0.24, 0.33) | 0.07c | (−0.31, 0.46) | 1.09b | (0.79, 1.39) | |||
| OK | Reference | Reference | Reference | ||||||
| Healthfulness | 62.3% | 50.6% | 44.9% | ||||||
| Healthy | 1.70b,c | (1.41, 1.98) | 1.84b,c | (1.44, 2.24) | 3.84b | (3.28, 4.40) | |||
| Neutral | 1.19b,c | (0.94, 1.45) | 1.28b,c | (0.90, 1.67) | 2.37b | (1.94, 2.79) | |||
| Unhealthy | Reference | Reference | Reference | ||||||
| Price (per $2 increase) | −0.09b,c | (−0.17, −0.01) | 9.8% | −0.10 | (−0.22, 0.02) | 5.5% | −0.25b | (−0.35, −0.14) | 4.9% |
| Preparation time (per 15 minute increase) | −0.02c | (−0.10, 0.05) | 0.2% | −0.18b,c | (−0.30, −0.06) | 16.4% | −0.48b | (−0.61, −0.35) | 18.5% |
| Travel time (per 5–10 minute increase) | −0.04c | (−0.12, 0.03) | 0.8% | −0.16b | (−0.29, −0.04) | 8.6% | −0.29b | (−0.39, −0.20) | 8.1% |
Relative attribute importance was calculated by dividing the difference in utility between the highest and lowest level of a single attribute by the sum of the differences of all attributes
Attributes or attribute levels with this superscript had a significant impact on meal preference
Statistically significant heterogeneity compared with referent category (bachelor’s degree or more) based on p-value for interaction terms
Findings were similar by financial burden category (Table 4; log likelihood = −2224.4, K=29; pseudo R2=0.39). Healthfulness and taste were the most important attributes for all 3 groups. Preparation time was the next most important attribute for participants in the low and medium financial burden categories, whereas price was for those in the high burden category. In addition, preparation time and travel time were not significantly associated with meal choice.
Table 4:
Mixed logit model for Chicago Healthy Eating Environments and Resources (CHEERS) participant mean meal preference estimates by financial burden category
| Attribute | Hard or very hard to pay for basics | Somewhat hard to pay for basics | Not hard at all to pay for basics | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% CI | Relative attribute importancea | Coefficient | 95% CI | Relative attribute importancea | Coefficient | 95% CI | Relative attribute importancea | |
| Taste | 15.3% | 23.8% | 24.7% | ||||||
| Very good | 0.45b,c | (0.17, 0.73) | 0.95b,c | (0.71, 1.19) | 1.63b | (1.36, 1.90) | |||
| Good | −0.15c | (−0.47, 0.17) | 0.36b,c | (0.12, 0.60) | 0.93b | (0.68, 1.17) | |||
| OK | Reference | Reference | Reference | ||||||
| Healthfulness | 72.2% | 50.9% | 44.0% | ||||||
| Healthy | 1.76b,c | (1.39, 2.13) | 1.98b,c | (1.69, 2.28) | 2.88b | (2.55, 3.22) | |||
| Neutral | 1.24b,c | (0.87, 1.61) | 1.40b | (1.13, 1.68) | 1.73b | (1.44, 2.02) | |||
| Unhealthy | Reference | Reference | Reference | ||||||
| Price (per $2 increase) | −0.06c | (−0.18, 0.05) | 12.9% | −0.12b,c | (−0.21, −0.04) | 8.3% | −0.24b | (−0.33, −0.16) | 8.6% |
| Preparation time (per 15 minute increase) | −0.06c | (−0.17, 0.05) | 2.7% | −0.15b,c | (−0.23, −0.06) | 11.1% | −0.29b | (−0.38, −0.20) | 15.5% |
| Travel time (per 5–10 minute increase) | −0.03c | (−0.14, 0.09) | −3.1% | −0.14b | (−0.23, −0.06) | 5.9% | −0.20b | (−0.28, −0.13) | 7.2% |
Relative attribute importance was calculated by dividing the difference in utility between the highest and lowest level of a single attribute by the sum of the differences of all attributes
Attributes or attribute levels with this superscript had a significant impact on meal preference
Statistically significant heterogeneity compared with referent category (not hard at all to pay for basics) based on p-value for interaction terms
Healthfulness and taste were the most important attributes for all three race/ethnic groups (Table 5; log likelihood = −2162.8, K=36; pseudo R2=0.41). Price was the next most important attribute for Hispanic/Latina participants, but preparation time was ranked third among non-Hispanic black and white participants. Preparation time was not a significant attribute among Hispanic/Latina participants; neither price nor travel time were significantly related to meal choice in non-Hispanic black participants. All attributes were significantly associated with meal choice in non-Hispanic whites.
Table 5:
Mixed logit model for Chicago Healthy Eating Environments and Resources (CHEERS) participant mean meal preference estimates by race/ethnicity
| Attribute | Hispanics/Latinas | Non-Hispanic Blacks | Non-Hispanic Whites | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Coefficient | 95% CI | Relative attribute importancea | Coefficient | 95% CI | Relative attribute importancea | Coefficient | 95% CI | Relative attribute importancea | |
| Taste | 21.9% | 23.7% | 24.7% | ||||||
| Very good | 0.74b,c | (0.55, 0.94) | 1.26b,c | (0.90, 1.62) | 2.14b | (1.75, 2.52) | |||
| Good | 0.19c | (−0.03, 0.41) | 0.035c | (−0.05, 0.75) | 1.27b | (0.92, 1.62) | |||
| OK | Reference | Reference | Reference | ||||||
| Healthfulness | 59.4% | 46.8% | 42.3% | ||||||
| Healthy | 1.83b,c | (1.57, 2.09) | 2.46b,c | (1.98, 2.94) | 3.74b | (3.19, 4.28) | |||
| Neutral | 1.32b,c | (1.09, 1.55) | 1.58b | (1.11, 2.04) | 2.16b | (1.72, 2.61) | |||
| Unhealthy | Reference | Reference | Reference | ||||||
| Price (per $2 increase) | −0.11b,c | (−0.18, 0.04) | 10.2% | −0.08c | (−0.22, 0.05) | 4.2% | −0.28b | (−0.40, −0.16) | 6.5% |
| Preparation time (per 15 minute increase) | −0.05c | (−0.11, 0.02) | 3.2% | −0.40b | (−0.55, −0.25) | 22.1% | −0.45b | (−0.58, −0.32) | 15.7% |
| Travel time (per 5–10 minute increase) | −0.10b,c | (−0.16, −0.03) | 5.4% | −0.07c | (−0.20, 0.06) | 3.2% | −0.33b | (−0.44, −0.22) | 10.8% |
Relative attribute importance was calculated by dividing the difference in utility between the highest and lowest level of a single attribute by the sum of the differences of all attributes
Attributes or attribute levels with this superscript had a significant impact on meal preference
Statistically significant heterogeneity compared with referent category (non-Hispanic whites) based on p-value for interaction terms
When interactions of race/ethnicity, financial burden, and education with meal attributes were included in a single model, many of the interaction coefficients for race/ethnicity and financial burden were attenuated (Supplemental Table; log likelihood = −2105.4, K=64; pseudo R2=0.43). The preference estimates for taste and healthfulness were weaker for participants in the high financial burden group compared with the low group. Taste was weaker for Hispanic/Latina participants, and healthfulness was weaker for non-Hispanic other race participants, compared with non-Hispanic white participants. There was no other significant variation by financial burden or race/ethnicity. In contrast, significant heterogeneity by education level remained for every attribute except price.
Discussion
In this discrete choice experiment participants reported that healthfulness and taste were the most important attributes influencing meal choices. Although the strength of these associations varied significantly such that these attributes were more weakly associated with meal choice in minorities and low SES groups, these rankings were consistent across race/ethnic and socioeconomic groups. There was substantial heterogeneity in the contributions of the other three meal attributes to meal choice. In particular, price was more important among those in the lowest SES categories and Hispanics/Latinas, while preparation time was a stronger predictor for those in the higher SES categories and non-Hispanic blacks and whites. In addition, travel time was not significantly associated with meal choice in low SES and non-Hispanic black participants.
Our findings for healthfulness and taste are consistent with the results from a previous study that used a discrete choice experiment to identify determinants of meal choice (Kamphuis et al., 2015). Participants in the low-SES group rated healthiness (by both income and education) and taste (only by income) as less important than their high SES counterparts. This study did not present relative importance scores or rankings by SES, so it is not clear whether or not healthfulness and taste remained the most important attributes for all participants. Our findings are also consistent with an observational study that used NHANES to relate perceived importance of several food attributes to diet (Aggarwal et al., 2016). They found taste and nutrition were the two most important factors for all socioeconomic and race/ethnic groups included in the study. Our finding that price was a more important attribute among low SES participants is consistent with several studies in the literature. The influence of price on food choice has been shown to be stronger in low income participants compared with their higher income counterparts (Darmon & Drewnowski, 2015; Glanz et al., 1998; Steptoe, Pollard, & Wardle, 1995). Previous studies have also shown low SES populations are more sensitive to changes in food prices (Green et al., 2013; Ni Mhurchu et al., 2013). For example, a US multi-site cohort study found increases in fast food pricing led to sharper decreases in fast food consumption in participants in the lowest education and income groups compared with their higher SES counterparts (Meyer et al., 2014). This price sensitivity may explain why placing restrictions on unhealthy foods (e.g., through taxes) tend to be a more successful strategy for promoting healthier eating behaviors than alternatives like menu labeling or opening new supermarkets (Mayne, Auchincloss, & Michael, 2015).
Travel time was one of the least important attributes among all participants, and it was unassociated with meal choice among participants in the lowest education and highest financial burden categories. This is consistent with recent studies that have suggested that many individuals, even low-income individuals with more limited access to transportation, frequently shop outside their neighborhoods (Dubowitz, Zenk, et al., 2015; Ver Ploeg, Mancino, Todd, Clay, & Scharadin, 2015). This is also supported by a discrete choice analysis of the National Household Food Acquisition and Purchase Survey that found participants of all income groups preferred superstores and supermarkets to farmers markets and smaller grocery stores, even if they were farther away (Taylor & Villas-Boas, 2016). Our findings have important implications for interventions designed to promote healthful eating in low-SES populations. Specifically, efforts designed to increase geographic access may not be sufficient to promote healthful behavior change without also changing taste preferences and making healthy foods more affordable. Previous research shows healthier diets (e.g., those higher in fruit, vegetables, and lean meat/fish) are more expensive than unhealthy diets (Darmon & Drewnowski, 2015). There is some evidence suggesting it is possible to eat meals that are both healthy and affordable, but it may require compromises in taste and convenience (Darmon & Drewnowski, 2015).
The strength of association and relative importance of price, preparation time, and travel time on meal choice all varied by race/ethnicity. Price was the least important attribute for non-Hispanic whites, but the third most important attribute for Hispanics/Latinas (after healthfulness and taste). Preparation time was not associated with meal choice in Hispanics/Latinas, but it was the third most important attribute among non-Hispanic blacks and whites. Travel time was unrelated to meal choice in non-Hispanic blacks, and the relationship was significantly weaker in Hispanics/Latinas compared with non-Hispanic whites. All of these interactions lost statistical significance when interactions between the attributes and SES indicators were included, which may indicate that these race/ethnic differences may have been driven by differences in education or income.
This study has several strengths and limitations. The use of a discrete choice experimental design is a key strength of this study, as it allowed for an implicit examination of food choices. In addition, the use of pictures in the discrete choice experiment made the options more easily understood regardless of education of literacy level (Mangham & Hanson, 2008). One limitation is that we were only able to include a limited number of attributes, and in doing so, we may have missed other, potentially important determinants of meal choice. Qualitative data collection approaches in diverse populations may help shed light on other important determinants of meal choice that could be incorporated into future discrete choice experiments in this area. Also, our non-proportional sampling approach may limit the generalizability of our findings. In addition, as described above, since discrete choice experiments identify stated preferences (rather than revealed preferences or actual choices made), they are susceptible to hypothetical bias.
Conclusions
Healthfulness and taste were the most important attributes for all participants. However, the relative importance of the other meal attributes evaluated in this study varied significantly by participant SES, particularly education. Discrete choice experiments have the potential to help public health researchers and practitioners identify the most salient targets for interventions designed to improve eating behaviors and reduce obesity disparities. Our findings suggest policies directed at improving geographic access to food outlets may not be sufficient for addressing the unequal burden of obesity facing low-SES populations without targeting other factors like the pricing of healthy and unhealthy foods.
Funding:
The corresponding author and the data collection were funded by the National Institutes of Health/National Heart, Lung, and Blood Institute (K01-HL133531).
References
- Aggarwal A, Rehm CD, Monsivais P, & Drewnowski A (2016). Importance of taste, nutrition, cost and convenience in relation to diet quality: Evidence of nutrition resilience among US adults using National Health and Nutrition Examination Survey (NHANES) 2007–2010. Prev Med, 90, 184–192. doi: 10.1016/j.ypmed.2016.06.030 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Block JP, & Subramanian SV (2015). Moving Beyond “Food Deserts”: Reorienting United States Policies to Reduce Disparities in Diet Quality. PLOS Medicine, 12(12), e1001914. doi: 10.1371/journal.pmed.1001914 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Clemes MD, Gan C, & Sriwongrat C (2013). Consumers’ Choice Factors of an Upscale Ethnic Restaurant. Journal of Food Products Marketing, 19(5), 413–438. doi: 10.1080/10454446.2013.724364 [DOI] [Google Scholar]
- Cummins S, Flint E, & Matthews SA (2014). New neighborhood grocery store increased awareness of food access but did not alter dietary habits or obesity. Health Aff (Millwood), 33(2), 283–291. doi: 10.1377/hlthaff.2013.0512 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Darmon N, & Drewnowski A (2015). Contribution of food prices and diet cost to socioeconomic disparities in diet quality and health: a systematic review and analysis. Nutr Rev, 73(10), 643–660. doi: 10.1093/nutrit/nuv027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- de Bekker-Grob EW, Ryan M, & Gerard K (2012). Discrete choice experiments in health economics: a review of the literature. Health Econ, 21(2), 145–172. doi: 10.1002/hec.1697 [DOI] [PubMed] [Google Scholar]
- Doherty TJ (2001). The influence of aging and sex on skeletal muscle mass and strength. Curr Opin Clin Nutr Metab Care, 4(6), 503–508. [DOI] [PubMed] [Google Scholar]
- Dubowitz T, Ghosh-Dastidar M, Cohen DA, Beckman R, Steiner ED, Hunter GP, … Collins RL (2015). Diet And perceptions change with supermarket introduction in a food desert, but not because of supermarket use. Health Aff (Millwood), 34(11), 1858–1868. doi: 10.1377/hlthaff.2015.0667 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dubowitz T, Zenk SN, Ghosh-Dastidar B, Cohen DA, Beckman R, Hunter G, … Collins RL (2015). Healthy food access for urban food desert residents: examination of the food environment, food purchasing practices, diet and BMI. Public Health Nutr, 18(12), 2220–2230. doi: 10.1017/S1368980014002742 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Elbel B, Moran A, Dixon LB, Kiszko K, Cantor J, Abrams C, & Mijanovich T (2015). Assessment of a government-subsidized supermarket in a high-need area on household food availability and children’s dietary intakes. Public Health Nutr, 18(15), 2881–2890. doi: 10.1017/s1368980015000282 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fitzgibbon ML, Tussing-Humphreys LM, Porter JS, Martin IK, Odoms-Young A, & Sharp LK (2012). Weight loss and African-American women: a systematic review of the behavioural weight loss intervention literature. Obes Rev, 13(3), 193–213. doi: 10.1111/j.1467-789X.2011.00945.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Glanz K, Basil M, Maibach E, Goldberg J, & Snyder D (1998). Why Americans eat what they do: taste, nutrition, cost, convenience, and weight control concerns as influences on food consumption. J Am Diet Assoc, 98(10), 1118–1126. doi: 10.1016/s0002-8223(98)00260-0 [DOI] [PubMed] [Google Scholar]
- Green R, Cornelsen L, Dangour AD, Turner R, Shankar B, Mazzocchi M, & Smith RD (2013). The effect of rising food prices on food consumption: systematic review with meta-regression. Bmj, 346, f3703. doi: 10.1136/bmj.f3703 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hauber AB, Gonzalez JM, Groothuis-Oudshoorn CG, Prior T, Marshall DA, Cunningham C, … Bridges JF (2016). Statistical Methods for the Analysis of Discrete Choice Experiments: A Report of the ISPOR Conjoint Analysis Good Research Practices Task Force. Value Health, 19(4), 300–315. doi: 10.1016/j.jval.2016.04.004 [DOI] [PubMed] [Google Scholar]
- Hensher DA, Rose JM, & Greene WH (2015). Applied choice analysis. Cambridge, UK: Cambridge University Press. [Google Scholar]
- Jeffries JK, Lee SH, Frick KD, & Gittelsohn J (2013). Preferences for Healthy Carryout Meals in Low-Income Neighborhoods of Baltimore City. Health Promotion Practice, 14(2), 293–300. doi: 10.1177/1524839912465290 [DOI] [PubMed] [Google Scholar]
- Kamphuis CB, de Bekker-Grob EW, & van Lenthe FJ (2015). Factors affecting food choices of older adults from high and low socioeconomic groups: a discrete choice experiment. Am J Clin Nutr, 101(4), 768–774. doi: 10.3945/ajcn.114.096776 [DOI] [PubMed] [Google Scholar]
- Kim HK, Lee TJ, & Yoon SH (2012). Factors affecting consumer’s choice of ethnic restaurants. Tourism Analysis, 17(3), 377–383. doi: 10.3727/108354212X13412775928104 [DOI] [Google Scholar]
- Kuhfeld WF (2010). Marketing research methods in SAS. SAS Technical Papers. Retrieved from http://support.sas.com/resources/papers/tnote/tnote_marketresearch.html [Google Scholar]
- Lindberg NM, & Stevens VJ (2007). Review: weight-loss interventions with Hispanic populations. Ethn Dis, 17(2), 397–402. [PubMed] [Google Scholar]
- Lindberg NM, Stevens VJ, & Halperin RO (2013). Weight-loss interventions for Hispanic populations: the role of culture. J Obes, 2013, 542736. doi: 10.1155/2013/542736 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Louviere JJ, Hensher DA, Swait JD, & Adamowicz W (2000). Stated choice models: Analysis and applications. Cambridge, UK; New York, NY: Cambridge University Pres. [Google Scholar]
- Mangham LJ, & Hanson K (2008). Employment preferences of public sector nurses in Malawi: results from a discrete choice experiment. Trop Med Int Health, 13(12), 1433–1441. doi: 10.1111/j.1365-3156.2008.02167.x [DOI] [PubMed] [Google Scholar]
- Matthews KA, Kiefe CI, Lewis CE, Liu K, Sidney S, & Yunis C (2002). Socioeconomic trajectories and incident hypertension in a biracial cohort of young adults. Hypertension, 39(3), 772–776. [DOI] [PubMed] [Google Scholar]
- Mayne SL, Auchincloss AH, & Michael YL (2015). Impact of policy and built environment changes on obesity-related outcomes: a systematic review of naturally occurring experiments. Obes Rev, 16(5), 362–375. doi: 10.1111/obr.12269 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Meyer KA, Guilkey DK, Ng SW, Duffey KJ, Popkin BM, Kiefe CI, … Gordon-Larsen P (2014). Sociodemographic differences in fast food price sensitivity. JAMA internal medicine, 174(3), 434–442. doi: 10.1001/jamainternmed.2013.13922 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Myung E, McCool AC, & Feinstein AH (2008). Understanding attributes affecting meal choice decisions in a bundling context. International Journal of Hospitality Management, 27(1), 119–125. doi: 10.1016/j.ijhm.2007.07.014 [DOI] [Google Scholar]
- Ni Mhurchu C, Eyles H, Schilling C, Yang Q, Kaye-Blake W, Genc M, & Blakely T (2013). Food prices and consumer demand: differences across income levels and ethnic groups. PLoS One, 8(10), e75934. doi: 10.1371/journal.pone.0075934 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Rogus S, Athens J, Cantor J, & Elbel B (2017). Measuring micro-level effects of a new supermarket: Do residents within 0.5 mile have improved dietary behaviors? J Acad Nutr Diet. doi: 10.1016/j.jand.2017.06.360 [DOI] [PubMed] [Google Scholar]
- Steptoe A, Pollard TM, & Wardle J (1995). Development of a measure of the motives underlying the selection of food: the food choice questionnaire. Appetite, 25(3), 267–284. doi: 10.1006/appe.1995.0061 [DOI] [PubMed] [Google Scholar]
- Stierand MB, & Wood RC (2012). Reconceptualising the commercial meal experience in the hospitality industry. Journal of Hospitality and Tourism Management, 19(1), 143–148. doi: 10.1017/jht.2012.16 [DOI] [Google Scholar]
- Taylor R, & Villas-Boas SB (2016). Food Store Choices of Poor Households: A Discrete Choice Analysis of the National Household Food Acquisition and Purchase Survey (Foodaps). American Journal of Agricultural Economics, 98(2), 513–532. doi: 10.1093/ajae/aaw009 [DOI] [Google Scholar]
- Tussing-Humphreys LM, Fitzgibbon ML, Kong A, & Odoms-Young A (2013). Weight loss maintenance in African American women: a systematic review of the behavioral lifestyle intervention literature. J Obes, 2013, 437369. doi: 10.1155/2013/437369 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ver Ploeg M, Mancino L, Todd JE, Clay DM, & Scharadin B (2015). Where do Americans usually shop for food and how do they travel to get there? Initial findings from teh National Household Food Acquisition and Purchase Survey. United States Department of Agriculture. [Google Scholar]
- Walker RE, Keane CR, & Burke JG (2010). Disparities and access to healthy food in the United States: A review of food deserts literature. Health Place, 16(5), 876–884. doi: 10.1016/j.healthplace.2010.04.013 [DOI] [PubMed] [Google Scholar]