

Abstract
BACKGROUND AND PURPOSE: The techniques of preoperative embolization of hypervascular spinal tumors, which has been known to be helpful for completing tumor resection, have not been described in detail. The purpose of this study was to analyze the technique and to evaluate the safety and value of preoperative transarterial embolization of hypervascular spinal tumors.
METHODS: Eighteen patients with hypervascular spinal tumors underwent transarterial embolization before surgery. The lesions were located between the upper cervical and lower lumbar spine: C1–T1 (n = 6), T5–L3 (n = 11), and L5 (n = 1); they arose intradurally in six patients and extradurally in 12. Thirty-one arteries were embolized with polyvinyl alcohol (PVA) particles (150–500 μm), and, in 18 of these, pieces of gelatin sponge were added for proximal pedicular embolization. The criteria for judging the effectiveness of embolization were completeness of tumor removal and estimated blood loss during surgery.
RESULTS: Tumor embolization was total in eight patients, nearly total in seven, subtotal in one, and partial in two. There were no symptomatic complications associated with embolization. Tumors were totally removed in 17 patients and nearly totally removed in one. The average estimated blood loss during surgery was 1100 mL (range, 200–6000 mL) for all 18 patients, and 1540 mL in patients with extradural tumors.
CONCLUSION: Preoperative embolization of hypervascular spinal tumors is safe and effective. It can make complete resection of a tumor possible and can make an unresectable tumor resectable. Superselection or flow control is necessary to achieve effective devascularization and to avoid complications.
Although the decision to perform surgery in patients with vertebral tumors that cause pain or neurologic deficit is somewhat controversial, it still is the best option (1–4). Surgical management can maintain spinal stability and relieve or prevent compression of the spinal cord and nerve roots. Resection of hypervascular spinal tumors may be hazardous or require termination owing to the possibility of excessive intraoperative bleeding; but, while preoperative embolization has been known to devascularize effectively hypervascular spinal tumors (1–5), the technical aspects of this procedure have not been described in detail. Although superselection of feeders is important to obliterate a hypervascular tumor bed, superselective embolization is sometimes difficult and dangerous in the treatment of spinal body tumors because of the numerous vascular channels around the vertebral column. In addition, preoperative embolization of intradural spinal tumors has rarely been reported in the literature (6, 7).
Methods
We retrospectively reviewed the records of 18 consecutive patients (10 men and eight women, 16 to 62 years old; mean age, 42 years) with hypervascular spinal tumors who had undergone preoperative transarterial embolization since 1993. The tumors were intradural in six cases and extradural in 12. The intradural tumors included three meningiomas, one schwannoma, one meningiopericytoma, and one hemangioblastoma. The extradural tumors, all of which involved vertebral bodies, consisted of three giant cell tumors, three multiple myelomas, two metastases from renal cell carcinoma, one metastasis from a hepatocellular carcinoma, one paraganglioma, one aneurysmal bone cyst, and one hemangioma. The vertebral body tumors compressed the spinal cord in eight patients, expanded to the pedicle in 11, and caused vertebral compression fracture in six. The levels of tumor involvement ranged from the upper cervical to the lower lumbar spine: C1–T1 (n = 6), T5–L3 (n = 11), and L5 (n = 1). Pain was the presenting symptom in 10 of the patients with extradural lesions, and was the only symptom in six cases. Symptoms referable to the lower limbs, ranging from minimal weakness at physical examination to gross motor weakness, spasticity, and sensory changes, were present in six of the 12 patients with extradural tumors. Among the six patients with intradural tumors, three had quadriparesis and three had lower extremity weakness.
A diagnosis of spinal tumor was made on the basis of findings at MR imaging and other imaging studies in all patients. In three patients, embolization was performed for tumors recurring after partial or total removal by previous surgery. In three patients with vertebral body tumors (case 7, 11, and 12), surgery performed within 1 week before embolization had to be terminated with no or only partial tumor removal on account of excessive bleeding.
All patients underwent angiography and embolization under local anesthesia and with intravenous sedation. Embolization was performed after diagnostic angiography or a few days later. A 4F or 5F catheter was used for diagnostic angiography. The angiographic protocol included the vertebral arteries, thyrocervical trunks, costocervical trunks, and external carotid arteries on both sides for cervical lesions; the vertebral arteries, thyrocervical trunks, costocervical trunks, and supreme intercostal arteries for upper thoracic lesions; the segmental arteries within at least two levels above and below the tumor site for thoracic and upper lumbar lesions; and the lower lumbar arteries, medial sacral artery, and internal iliac arteries for lower lumbar lesions. Selective angiography of the suspicious arterial branches supplying the tumor was then performed. No provocative testing was attempted. In total, 32 arteries were embolized. All materials for embolization were injected via a microcatheter coaxially inserted through the angiographic catheter. Polyvinyl alcohol (PVA) particles ranging in size from 150 to 500 μm were used in 31 arteries, and, in 18 of these, pieces of gelatin sponge (Gelfoam) were added for proximal pedicular embolization. N-butyl cyanoacrylate (NBCA) was injected into a single feeder.
The PVA particles were injected by means of a variety of methods. The first choice for the use of particles was direct infusion into the branch supplying the tumor via the superselectively introduced microcatheter (Figs 1 and 2). If superselective catheterization was not available, or if multiple small branches supplied the tumor, the normal branches distal to the tumor feeder were catheterized and embolized with Gelfoam strips or coils for protection, and then particles were infused proximal to the feeders (Fig 3). Flow control techniques, using preferential flow or flow reversal, were used to make particles flow into the feeding branches to the tumors rather than into the normal branches when particles were infused proximal to the tumor branches (Figs 3 and 4). A repeat angiogram was obtained immediately after embolization. Based on residual tumor staining, embolization was categorized as total (none), nearly total (<10%), subtotal (10% to 30%), and partial (>30%).
fig 1.
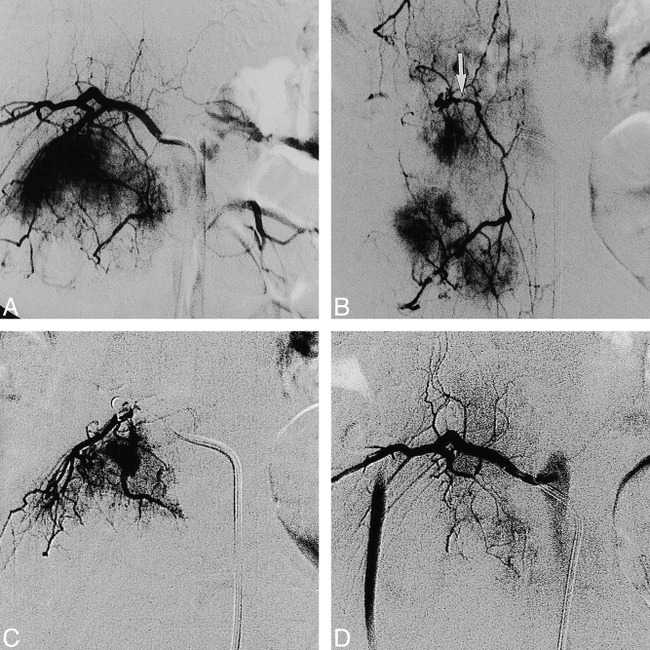
Case 7: 27-year-old woman with a giant cell tumor in the L3 vertebral body who underwent embolization 2 days before surgery.
A, Preembolization angiogram of the right second lumbar artery shows hypervascular supply to the tumor.
B, Selective injection of the dorsispinal artery at L2 (arrow) shows the extraspinal longitudinal anastomoses from L1 to L4 with tumor supply by L2 and L3.
C, Superselective injection of the feeding artery near the dorsispinal branch was followed by infusion of PVA particles.
D, Postembolization angiogram shows nearly total occlusion of the feeding artery and patency of the normal branches.
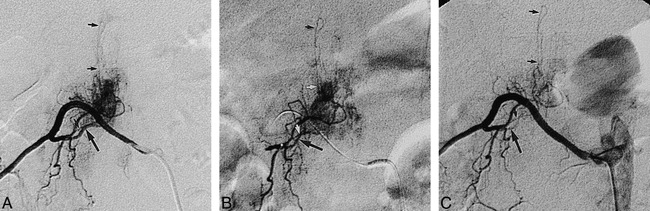
fig 3.

Case 6: 31-year-old man with an intramedullary hemangioblastoma at T8–T9 who underwent embolization the day before surgery.
A, Preembolization angiogram shows that the posterior radiculomedullary artery (arrow), mainly supplying the intradural tumor, originates from the right ninth intercostal artery.
B, Angiogram after embolization with coils (large arrow) shows occlusion of the intercostal artery distal to the feeder, and the presence of another normal branch originating just distal to the feeder. Infusion of PVA particles with preferential flow and infusion of Gelfoam was then performed through the microcatheter (small arrow) close to the feeder.
C, Postembolization angiogram shows complete occlusion of both the feeder and the normal branch.
Surgical procedures were performed within 12 days (mean, 3 days) after embolization. The blood loss estimated by the anesthesiologists and surgeons at the time of the procedure was obtained from the surgical records. Clinical outcome was evaluated in the outpatient clinic approximately 3 months after surgery. Excellent indicated no neurologic symptoms; good, minor neurologic symptoms; fair, mild or moderate neurologic symptoms; and aggravated, more severe symptoms than before embolization.
Results
The clinical data and embolization results are shown in the Table. In the six patients with lesions at C1–T1, the arteries supplying the tumors originated from the vertebral arteries in four, from the costocervical trunk in one, and from the vertebral artery and thyrocervical trunk in another. All feeding arteries to tumors from T5–L3 arose from the intercostal or lumbar arteries. The feeder originated in the iliolumbar artery in one patient with a lesion at L5 (case 17). Thirty-two of 34 feeding arteries were embolized. NBCA was injected into a superselectively catheterized feeder from the right vertebral artery at the C1–C2 interspace in the patient with the intradural lesion (case 3). The PVA particles were directly infused into the feeders after superselective catheterization in 13 arteries (Figs 1 and 2). Flow control was used for infusion of the particles in most cases, even after superselective catheterization. The normal branches were embolized with Gelfoam strips in 11 arteries and with coils in three. The particles were then infused into 10 of 14 arteries in which there was no evidence of normal branches around the feeders. The PVA particles were injected into eight arteries in which there were still normal branches around the feeders. The majority of PVA particles flowed into the feeders when the particles were infused slowly in a diluted solution, because there was much more blood flow into the feeders than into the normal branches in that case (Fig 3). In three cases, there was reversal of flow in a normal branch from a collateral after the pedicle was wedged by the guiding catheter (two arteries) or by the microcatheter (one artery, Fig 4). Two arteries were not embolized owing to their particular anatomic status. In a patient with intradural tumor at C1–C2 (case 2), a feeder inferiorly arising from the left vertebral artery at C3 failed to be superselectively catheterized after another feeder from the same vertebral artery was embolized. In another patient with a vertebral body tumor (case 7), multiple small branches from the right vertebral artery remained to supply the lesion while the major feeder from the left thyrocervical trunk was embolized. Therefore, the tumors were only partially (50% to 70%) devascularized in these two cases. Tumor embolization was total in eight patients, nearly total in seven, and subtotal in one.
Clinical data and results in 18 patients treated with preoperative transarterial embolization
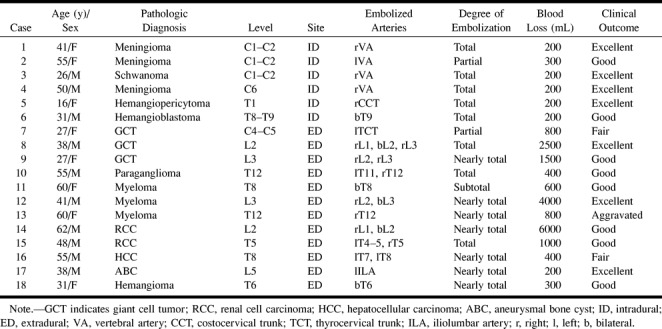
fig 4.
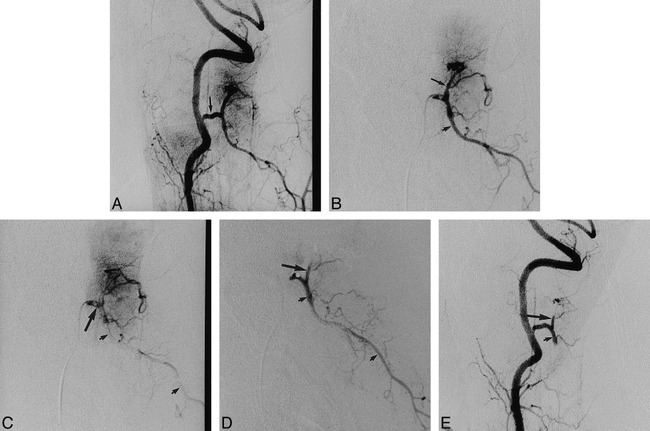
Case 1: 41-year-old woman with a meningioma at C1–C2 who underwent embolization the day before surgery.
A, Right vertebral angiogram before embolization shows a C2 branch supplying the intradural tumor (arrow).
B, Selective microcatheter injection of the common trunk of the feeder (large arrow) and the normal branch (small arrow) is performed before embolization.
C, Late arterial phase of selective injection shows that most of the contrast medium in the normal branch is washed out (small arrows) because the wedged microcatheter caused flow reversal in the branch. Note that dense contrast medium remains in the trunk (large arrow) just distal to the tip of the microcatheter.
D, Injection after infusion of PVA particles in the trunk shows almost complete occlusion of the feeder (large arrow) and patency of the normal branch (small arrows).
E, Right vertebral angiogram after embolization with Gelfoam pieces shows complete occlusion of both the feeder (large arrow) and the normal branch (small arrow).
Anterior spinal arteries were found in 10 patients, none of which arose from the same pedicle as the tumor feeders. They originated at the cervical level in three cases, at T5–T12 in six cases, and at L2 in one case. Nine posterior spinal arteries were seen in six patients. Among five posterior spinal arteries originating from the common trunks with feeding arteries, two were not affected after superselective catheterization into the feeders (Fig 2), one was embolized with Gelfoam for protection before the PVA was infused, and two were feeders supplying the intramedullary tumor (case 6) and embolized with PVA particles via superselective catheterization or via preferential flow after protection of the main normal branch (Fig 3). There were no complications within 24 hours after embolization. MR imaging, performed the day after embolization in a case of giant cell tumor in the vertebral body (case 9), showed extensive tumor necrosis.
fig 2.
Case 10: 55-year-old man with a paraganglioma in the T12 vertebral body who underwent embolization 7 days before surgery.
A and B, Angiogram of the right segmental artery at T12 (A) and selective angiogram with microcatheter (B) show the posterior radiculomedullary artery (small arrows) originating from the same trunk as the feeding artery (large arrow) to the tumor.
C, Pedicular injection after superselective catheterization and infusion of PVA particles and Gelfoam pieces in the feeder show complete occlusion of the feeder (large arrow) and patency of the posterior radiculomedullary artery (small arrows).
Tumors were totally removed in 17 patients and nearly totally in one patient (case 6). Estimated blood loss during the surgical procedure wasbetween 200 and 6000 mL, with an average of 1100 mL. Blood loss was from 200 to 300 mL in the patients with intradural tumors. In those with extradural lesions, the average blood loss was1540 mL. Although there was blood loss of 4000 mL or more in two patients, their tumors were totally resected. Clinical outcome 3 months after surgery was excellent in seven cases, good in eight, fair in two, and aggravated by tumor recurrence in one.
Discussion
Several investigators have reported their results with preoperative endovascular embolization of spinal tumors (1–5, 8–10). Surgery in patients with hypervascular tumors is frequently complicated by excessive intraoperative blood loss. Preoperative tumor embolization facilitates surgical resection primarily by reducing intraoperative bleeding, ensuring an unimpeded view of the surgical field, and shrinking the tumor, thus making complete tumor resection more likely (5). Total tumor removal was obtained after embolization in almost all the patients in our series. The median estimated intraoperative blood loss in patients with vertebral tumors was 1540 mL, which was less than or similar to the previously reported estimates, with averages from 1600 mL to 2200 mL (1–5, 8). In contrast, previous attempts at resection before embolization were unsuccessful because of excessive bleeding in three of our first five patients with vertebral body tumors.
Preoperative embolization of intradural spinal tumors has rarely been reported in the literature. Hypervascular intradural tumors consist of intramedullary tumors, such as hemangioblastoma, and extramedullary tumors, including meningioma and schwannoma. Berenstein and Lasjaunias (6) presumed that angiography and embolization of intradural spinal tumors would be limited to hemangioblastomas, as they are the only truly hypervascular spinal cord tumors. Eskridge et al (7) reported preoperative endovascular embolization of craniospinal hemangioblastomas in nine patients, including two with spinal lesions. These two patients, who had first undergone surgical resection, had repeat surgery after embolization, which rendered the tumor nidus avascular. In our series, preoperative embolization of intradural spinal tumors was performed in six patients, including one with an intramedullary tumor and five with an extramedullary tumor. In every patient with an intradural tumor, preoperative embolization was requested by the surgeons, who believed that tumor resection would be easier and safer after embolization as compared with surgery without embolization. The decreased intraoperative bleeding after embolization clarified the surgical field, and the increased cleavage between tumor and spinal cord, which resulted from tumor shrinkage, permitted easier resection.
Various embolic materials are available for the embolization of vessels supplying spinal tumors. Although Gelfoam has been used in the past, proximal occlusion of large vessels without penetration into the tumor architecture results in ineffective embolization with very early recanalization through enzymatic resorption of the material. Absolute ethanol has also been used for preoperative embolization of spinal metastases from renal cancer. No complications were found in the 17 patients reported by Sundaresan et al (4), who felt that ethanol was a superior embolic agent because of its deep penetration and intimal sclerosis with inflammatory reaction. Breslau et al (2) described a vertebral artery that was occluded with a detachable balloon in order to simplify the surgical approach in a case of cervical vertebral tumor. However, the most frequently used embolic agent reported in the literature, and the one used in our series, is PVA particles. These particles are nonbiodegradable (11). PVA particles of 150- to 250-μm diameter allow relatively distal embolization with occlusion at the capillary level, because the capillaries within the tumor are usually about 200 μm in diameter. If normal branches or important anastomoses are seen in the preliminary superselective study or during the course of embolization, the use of larger particles, such as 250 to 350 μm or 350 to 500 μm, is safe in order to avoid normal tissue ischemia. Then the same arteries can be occluded proximally by using Gelfoam. Such proximal Gelfoam occlusion may produce a transient devascularization of the region adjacent to the tumor as well as augment the distal thrombosis within the tumor itself.
The embolization technique includes catheterization and infusion of embolic agent into the feeding arteries via the catheter. The objective is to infuse embolic agent only into the feeders, thus sparing normal, uninvolved arteries. Optimal catheterization is as superselectively into the tumor feeder as possible (Figs 1C and 2). In our series, all procedures were performed with a coaxial microcatheter technique using a Tracker-18 or Tracker-10 via a 4F or 5F catheter, which acted as a guide. Superselective catheterization was successfully performed in 14 of 32 arteries supplying the tumors. Reshaping of the microguidewire or microcatheter is usually necessary, depending on the course of the relevant vessels. High-resolution angiography with subtraction facilities the procedure, and road-mapping techniques are also necessary, especially for identifying spinal arteries. Even though superselective catheterization is available, attention should be given to injection of the embolic material in order to avoid reflex into the normal branches.
Superselective catheterization is sometimes difficult or impossible owing to the size and course of the feeders. To obtain efficient devascularization of tumors and avoid complications in such cases, blood flow control may be used to ensure that the blood with the embolic agent flows toward feeders rather than toward the normal vessels, once the hemodynamic characteristics of the relevant vessels have been evaluated. The technique most commonly used for flow control is to protect the vessels supplying the normal tissues by embolizing their proximal portions, which usually does not risk ischemia of normal tissue, because of the collaterals. Sufficient anastomoses exist among the adjacent structures, both on individual and consecutive levels (12). Within the spinal canal, anastomoses mostly transverse dorsally and ventrally to the dural sheath. From this extradural ring, several branches supply the adjacent bony structures. Extraspinal anastomoses are mainly longitudinal between two consecutive segmental arteries (Fig 1B). These longitudinal communications at the thoracolumbar level include the dorsal anastomoses around the midline and the pretransverse dorsal anastomoses and anastomoses originating from the lateral portions of the intercostal or lumbar arteries. Anastomoses outside the spinal canal at the cervical level are formed by the deep cervical, vertebral, and ascending cervical arteries. Therefore, after the normal branches are proximally embolized with Gelfoam strips or coils, infusion of PVA particles proximal to a feeder is functionally similar to superselective injection into a feeder, and normal tissues previously supplied by proximally occluded branches can immediately receive blood supply from anastomoses.
Preferential flow or flow reversal is also a useful method of flow control when superselective catheterization into feeders is unsatisfactory or impossible or when there are still branches supplying normal tissues although superselective catheterization is available or the main normal branch is embolized for protection (Fig 3). Test injection of contrast medium into a vessel proximal to a feeder in a manner similar to the infusion of particles is helpful in such cases. If almost all contrast medium is shown to preferentially flow toward a feeder, owing to the hypervascularity of the tumor, PVA particles can also be infused. Even if there is a small amount of flow into normal branches, PVA particles can still be used. Of course, a microcatheter should be positioned as close to the feeder as possible, and the infusion of the particles should be performed slowly and carefully, using a diluted solution. When increased flow into normal branches is noted during embolization, the injection of PVA particles should be stopped in order to avoid normal tissue ischemia. At this point, Gelfoam pieces can be used for embolization of the feeder even if it involves normal branches. In our series, no complications occurred after embolization was performed via this preferential flow method in five arteries in which normal branches were located distal to the microcatheter. In another three arteries, almost all contrast medium flowed into the feeders during a test injection after the 5F catheter or microcatheter had been wedged in the pedicle of the artery (Fig 4C). This wedged catheter temporally obstructed pedicular flow and probably reversed blood flow into the normal branch via the anastomosis; this then forced the emboli toward the feeders (Fig 4D), which were then completely embolized with particles.
Special attention should be paid to the identification of spinal arteries. Anterior spinal arteries were noted in 10 cases in our study, but none of them originated from the same arterial pedicle as the feeding artery to the tumor. The presence of an anterior spinal artery at the same pedicle is an obvious contraindication for embolization (1, 6, 10). The untoward embolization of an anterior spinal artery may injure the pyramidal tracts and cause a severe motor deficit (13). In addition, embolization of feeders in adjacent levels should be performed carefully because there are numerous collateral channels surrounding the vertebral column. No symptoms corresponding to spinal cord ischemia were observed after embolization of posterior spinal arteries with particles as feeders or with Gelfoam for protection in these cases.
Conclusion
Preoperative transarterial embolization of hypervascular spinal tumors is safe. It appears to limit blood loss during surgery and to allow complete tumor resection, including of those tumors initially believed to be unresectable. Of course, appropriate techniques, such as superselective catheterization and blood flow control, including protection of the normal branches, preferential flow, and flow reversal, are necessary in order to achieve efficient devascularization and to avoid complications.
Acknowledgments
We thank Soon Ju Lee for preparing the manuscript, and Bonnie Hami, Department of Radiology, University Hospitals of Cleveland, for editorial assistance.
Footnotes
Address reprint requests to Hai Bin Shi, MD, Department of Radiology, First Affiliated Hospital of Nanjing Medical University, 300 Guangzhou Rd, Nanjing 210029, China.
References
- 1.Smith TP, Gray L, Weinstein JN, Richardson WJ, Payne CS, Preoperative transarterial embolization of spinal column neoplasms. J Vasc Interv Radiol 1995;6:863-869 [DOI] [PubMed] [Google Scholar]
- 2.Breslau J, Eskridge JM, Preoperative embolization of spinal tumors. J Vasc Interv Radiol 1995;6:871-875 [DOI] [PubMed] [Google Scholar]
- 3.Olerud C, Jonsson H, Lofberg AM, Lorelius LE, Sjostrom L, Embolization of spinal metastases reduces preoperative blood loss. Acta Orthop Scand 1993;64:9-12 [DOI] [PubMed] [Google Scholar]
- 4.Sundaresan N, Choi IS, Hughes JEO, Sachdev VP, Berenstein A, Treatment of spinal metastases from kidney cancer by presurgical embolization and resection. J Neurosurg 1990;73:548-554 [DOI] [PubMed] [Google Scholar]
- 5.Gellad JE, Sadato N, Numaguchi Y, Levine AM, Vascular metastatic lesions of the spine: preoperative embolization. Radiology 1990;176:683-686 [DOI] [PubMed] [Google Scholar]
- 6.Berenstein A, Lasjaunias P, Tumors of the spinal column and spinal cord. In: Surgical Neuroangiography. Berlin: Springer; 1992;5:111–147
- 7.Eskridge JM, McAuliffe W, Harris B, Kim DK, Scott J, Winn HR, Preoperative endovascular embolization of craniospinal hemangioblastomas. AJNR Am J Neuroradiol 1995;17:525-531 [PMC free article] [PubMed] [Google Scholar]
- 8.Hess T, Kramann B, Schmidt E, Rupp S, Use of preoperative vascular embolisation in spinal metastasis resection. Arch Orthop Trauma Surg 1997;116:279-282 [DOI] [PubMed] [Google Scholar]
- 9.Broaddus WC, Grady MS, Delashaw JB, Ferguson RDG, Jane JA, Preoperative superselective arteriolar embolization: a new approach to enhance resectability of spinal tumors. Neurosurgery 1990;27:755-759 [PubMed] [Google Scholar]
- 10.O'Reilly GV, Kleefield J, Klein LA, Blume HW, Dubuisson D, Cosgrove GR, Embolization of solitary spinal metastases from renal cell carcinoma: alternative therapy for spinal cord or nerve root compression. Surg Neurol 1989;31:268-271 [DOI] [PubMed] [Google Scholar]
- 11.Latchaw RE, Gold LHA, Polyvinyl foam embolization of vascular and neoplastic lesions of the head, neck, and spine. Radiology 1979;131:669-679 [DOI] [PubMed] [Google Scholar]
- 12.Lasjaunias P, Berenstein A, Spinal and spinal cord arteries and veins. In: Surgical Neuroangiography. Berlin: Springer; 1992;3: 15–87
- 13.Casasco AE, Houdart E, Gobin YP, Aymard A, Guichard JP, Rufenacht DA, Embolization of spinal vascular malformations. Neuroimaging Clin North Am 1992;2:337-358 [Google Scholar]