

Abstract
Aims
The aim of this paper is to describe the impact of COVID-19 on spine surgery services in a district general hospital in England in order to understand the spinal service provisions that may be required during a pandemic.
Methods
A prospective cohort study was undertaken between 17 March 2020 and 30 April 2020 and compared with retrospective data from same time period in 2019. We compared the number of patients requiring acute hospital admission or orthopaedic referrals and indications of referrals from our admission sheets and obtained operative data from our theatre software.
Results
Between 17 March to 30 April 2020, there were 48 acute spine referrals as compared to 68 acute referrals during the same time period last year. In the 2019 period, 69% (47/68) of cases referred to the on-call team presented with back pain, radiculopathy or myelopathy compared to 43% (21/48) in the 2020 period. Almost 20% (14/68) of spine referrals consisted of spine trauma as compared to 35% (17/48) this year. There were no confirmed cases of cauda equine last year during this time. Overall, 150 spine cases were carried out during this time period last year, and 261 spine elective cases were cancelled since 17 March 2020.
Recommendations
We recommend following steps can be helpful to deal with similar situations or new pandemics in future:
24 hours on-call spine service during the pandemic.
Clinical criteria in place to prioritize urgent spinal cases.
Pre-screening spine patients before elective operating.
Start of separate specialist trauma list for patients needing urgent surgeries.
Conclusion
This paper highlights the impact of COVID-19 pandemic in a district general hospital of England. We demonstrate a decrease in hospital attendances of spine pathologies, despite an increase in emergency spine operations.
Cite this article: Bone Joint Open 2020;1-6:281–286.
Keywords: COVID-19, OARS, IPASS, Major trauma centre
Introduction
Emerging and re-emerging pathogens are global challenges for public health.1 The current COVID-19 pandemic is the biggest challenge faced by national health systems in a century.2 A cluster of pneumonia of unknown origin identified in Wuhan, China, in December 20193 was termed severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2)4 or coronavirus disease 2019 (COVID-19). On 12 March, the World Health Organization (WHO) declared COVID-19 as a pandemic.5
On 17 March, NHS England released a statement to postpone all non-urgent operations for at least three months to expand critical care capacity to the maximum.6 Such an announcement has had an effect on all the provision of elective and trauma orthopaedic services in the UK, including spinal services. It is not known, however, how to best optimize the provision of surgical services to meet the changing demand during such a pandemic (Figure 1).
Fig. 1.
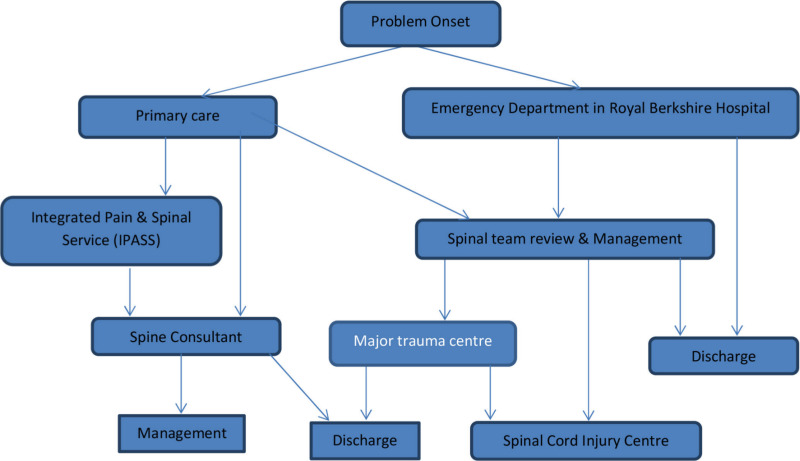
Spine pathway in Royal Berkshire Hospital.
Our hospital is a district general hospital consisting of three spine surgeons. Before the pandemic, our acute spinal pathway involved patients presenting to the emergency department (ED) for assessment by ED doctors and referred accordingly to the on-call orthopaedic team. Patients were referred directly from primary care to the on-call team. We accept and manage almost all of the spine emergencies except unstable spine injuries at any level, open spine fractures and spine injuries with neurology. Complex cases are referred to our major trauma centre (Oxford, UK). Cases involving spinal cord injuries are referred to spinal cord injury centre (Stoke Mandeville, UK) for further rehabilitation. Overall, we manage most of the patients presenting with spine conditions are managed by our spine service. If spine consultants are not available, then patients can be discussed with Oxford spine team via online referral system i-e Oxford Acute Referral System (OARS).
The elective spine referral involves either a direct referral to spinal team or via the integrated pain and spinal service (IPASS) which provides multi-disciplinary specialist assessments and treatments for patients with back and generalized persistent pain. The multidisciplinary team (MDT) is able to educate and discuss with patients the most effective treatment for the individual with options including, psychological, pharmacological, physical and invasive treatments.7 IPASS then can refer the patients to spinal team for further management.
During the pandemic, guidelines for managing spine patients issued by the British Orthopaedic Association (BOA) and British Orthopaedic Association of Spine Surgeons (BASS) states that the movement of patients should be minimized to only those requiring specialist input or urgent /emergency spinal surgery. In the situation where capacity across the network becomes a specific issue, a dedicated single unit will be identified as the overarching spinal hub centre (Figure 2).8
Fig. 2.
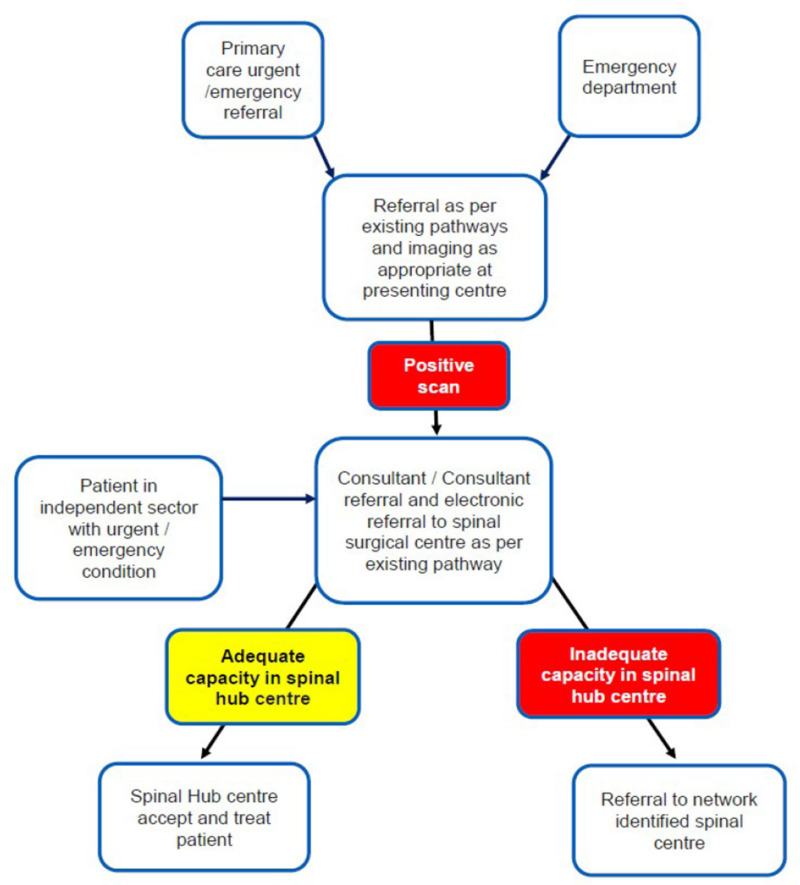
NHS Spine pathway during COVID-19 pandemic.
Our spine services adapted to these guidelines by managing most of spine emergencies requiring surgical intervention. Our consultants were available out of hours to operate and hence decreasing the patients’ movement to major trauma centre. All elective operative cases were cancelled and patients’ in need of urgent surgeries are prioritized. All face-to-face elective clinics have been moved to telephone clinics and the IPASS pathway is closed to decrease the influx of patients.
The aim of this paper is to describe the impact of COVID-19 on spine surgery services in a district general hospital in the UK in order to understand the spinal service provisions that may be required during a pandemic.
Methods
A prospective cohort study was undertaken between 17 March 2020 and 30 April 2020 during which elective operations were cancelled and compared with retrospective data from same time period in 2019. We compared the number of patients requiring acute hospital admission or orthopaedic referrals and indications of referrals from our admission sheets and obtained operative data from our theatre software. We included all spine patients referred to our on-call team and discussed in our trauma meetings. We also compared elective operations performed during this time last year to the number of cases cancelled due to COVID-19 pandemic.
Results
Between 17 March to 30 April 2020, there were 48 acute spine referrals since cancellation of elective operations as compared to 68 acute referrals during the same time period last year. In the 2019 period, 69% (47/68) of cases referred to the on-call team presented with back pain, radiculopathy, or myelopathy compared to 43% (21/48) in the 2020 period. Almost 20% (14/68) of spine referrals consisted of spine trauma as compared to 35% (17/48) this year. There were no confirmed cases of cauda equine last year during this time. There were four confirmed cases of cauda equine reported and operated on during the pandemic this year. Despite the reduction in acute referrals, there was an increase in emergency spine operations performed during the COVID-19 pandemic, with 13 operations carried out during this time.
Three spine cases were discussed with spine team in Oxford via OARS due to spine surgeons not on-call in our hospital in 2019 and one patient with spine trauma was transferred to Oxford. Following the new BOA and BASS guidelines issues during pandemic, all the cases were discussed and managed by our spine team during the pandemic.
Overall, 150 spine operations were carried out in our hospital by three spine consultants last year from 17 March to 30 April. The breakdown of cases is explained in Table I. As of 17 March 2020, due to the cancellation of non-urgent cases, 261 spine cases were cancelled (Table II, Figure 3, Tables II and III).
Table I.
Elective operations from 17 March to 30 April 2020.
| Elective operations | Done in 2019 | Cancelled in 2020 |
|---|---|---|
| Nerve root injections | 60 | 105 |
| Caudal injections | 46 | 86 |
| Discectomy | 6 | 24 |
| Decompression | 26 | 32 |
| Disc arthroplasty | 2 | |
| Anterior cervical decompression and fusion (ACDF) | 5 | 8 |
| Posterior or transformainal lumbar interbody fusion (PLIF/TLIF) | 4 | 2 |
| Foraminotomies | 3 | 2 |
| Total | 150 | 261 |
Table II.
Acute spine referrals from 17 March to 30 April 2020.
| Diagnosis | 2019 | 2020 | OARS 2019 | OARS 2020 |
|---|---|---|---|---|
| Spine trauma | 14 | 17 | ||
| Confirmed CES | 0 | 4 | ||
| Abscess/discitis | 4 | 4 | 1 | |
| Metastatic lesions | 3 | 2 | 1 | |
| Prolapse/stenosis | 17 | 5 | 1 | |
| Back pain | 30 | 16 | 1 | |
| Total | 68 | 48 | 4 | 0 |
Fig. 3.
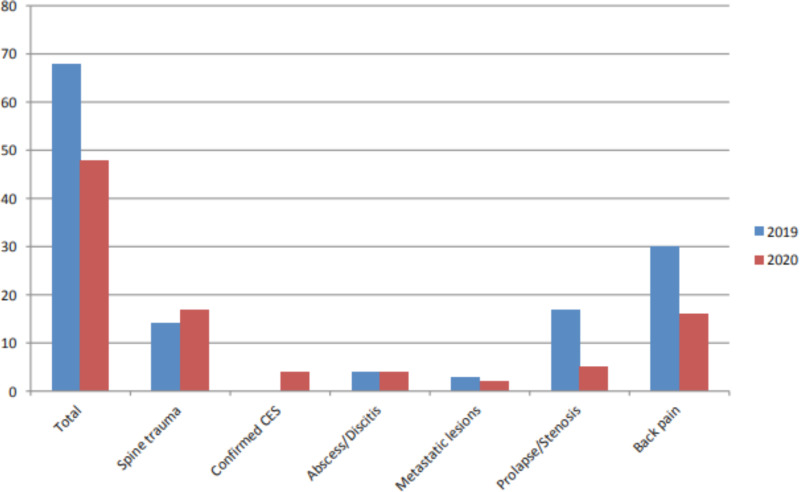
NHS Spine pathway during COVID-19 pandemic.
Table III.
Acute spine operations from 17 March to 30 April 2020.
| Procedures | 2019 | 2020 |
|---|---|---|
| Revision lumbar decompression and discectomy | 1 | |
| Lumbar nerve root injection | 1 | |
| Lumbar decompression | 2 | 5 |
| Cervical decompression | 1 | |
| Lumbar micro discectomy | 2 | |
| Thoracic corpectomy and fusion | 1 | |
| Lumbar stabilization | 2 | |
| Anterior cervical decompression and fusion (ACDF) | 1 | |
| Total | 3 | 13 |
Discussion
Overall, we have demonstrated during the COVID-19 pandemic there was a decrease in the number of ED referrals to the acute spinal service at our district general hospital; however, despite this there was an increase in emergency spinal operations. This could be due to fact that only patients with serious conditions are presenting to the ED during the lockdown and patients with more minor conditions are self-managing at home. Also, with the announcement of cancellation of elective services our spine team prioritized patients requiring urgent spinal decompressions and were given place on trauma lists. It is expected that for many spine patients, a significant delay in care may result in the progression of symptoms in terms of weakness and pain with possibly less predictable improvements after surgery. Furthermore, in many conditions, such as myelopathy, delaying surgical decompression may allow for neurological deterioration and irreversible patient harm.
Spain and Italy were among the first countries in Europe to be affected by the pandemic and, as such, they implemented new care pathways to manage the changing requirements of the orthopaedic services. Giorgi et al9 proposed a care pathway for emergency spinal surgery in Italy. Their goal was to reduce the time to surgery with the ultimate aim of reducing the overall length of hospital stay for the patients. In order to reach their goals, they made a multidisciplinary team of spinal surgeons and a dedicated theatre and staff. In our approach, to minimize the travel of patients between different hospitals and reduce hospital stay, our spine surgeons worked out of their on-call rota to help with patients’ management and discharge. It is depicted in our results, by an increase in spine cases performed in emergency during COVID-19 pandemic compared to same time last year. Also, no spine referral was made to spine team in major trauma centre during the pandemic as compared to three cases which were online referred last year due to non-availability of our spine service out of hours.
Chang Liang et al10 recently reported the organizational experience in Singapore. Patients who needed urgent care of their injuries were still admitted to hospital and treated in the same way as usual. Moreover, and more interestingly, they reported that day cases were also managed as usual, since the required hospital stay was less than 23 hours. The rationale was that the short hospital stay does not pose a major drain on healthcare resources and does not carry a high risk of nosocomial COVID-19 infection. In our approach, we managed all spine emergencies as usual by ensuring spine surgeon review and surgical intervention done within 24 hours of admission and aim to discharge most spine emergency operations the following day if there is a smooth recovery.
Our study shows a decrease of nearly 21% in spine referrals during the pandemic despite cancellation of all elective operations during this time period. In contrast, there happens to be an increase in the spine operations done in emergency due to few cases done on urgent bases due to cancellation of elective lists and also due to cancellation of routine appointments for spine surgeons leading to an increased availability of surgeons for patients requiring urgent care. Our results are in line with the regional study done by Long et al11 stating a 57% decrease in dental referrals during the pandemic and national data available showing a decrease of 29% in emergency department attendances in March 2020 as compared to March last year.12 There is 23% decrease in emergency admissions reported during March 2020 as compared to March 2019.13
Back pain is one of the common presenting symptom to emergency departments spine referrals. Due to the cancellation of nerve injections and caudal epidural, we expected to see an increase in emergency attendances with these symptoms but our results show 13 cases with back pain referred to the orthopaedic team during pandemic as compared to 30 cases referred last year. There were 60 nerve root injections and 46 caudal injections performed on elective lists by our three spine surgeons. During the pandemic, 105 nerve root injections and 86 caudal injections were cancelled. Despite a large number of injection cases cancelled and community spine services not available, fewer patients presented to ED demonstrating that either patients’ are cautious not to overburden the health system unless absolutely necessary or the fear of catching virus is keeping them away.
Plans are in place to start elective spine surgery in accordance with the new guidelines released by the British Association of Spine Surgeons (BASS).14,15 Like other domains, the pandemic will have a lasting effect on both acute and elective services in future. All patients cancelled during the pandemic will be prioritised and counselled16 for COVID-19 risks. Steroid injections for back pain are deemed not clinically urgent by BASS and advised not to be performed at this time. As such, other options to manage pain need to be explored and discussed with patients.15
Recommendations
We recommend following steps can be helpful to deal with similar situations or new pandemics in future:
24 hours on-call spine service during the pandemic.
Elective services to be expanded to private hospitals to avoid postoperative complications.
Clinical criteria in place to prioritize urgent spinal cases.
Pre-screening spine patients before elective operating.
Start of separate specialist trauma list for patients needing urgent surgeries.
Conclusion
This paper highlights the impact of COVID-19 pandemic in a district general hospital of England. We demonstrate a decrease in hospital attendances of spine pathologies despite increase in emergency spine operations. This should help to guide hospitals in ensuring the availability of acute spinal emergency services during future pandemics. It can guide spine services to prepare for a change in the demands of the acute spinal services and plan to accommodate cancelled elective cases once the pandemic is settled.
Acknowledgements
The authors thank all the orthopaedic surgeons whose patients were included in this study.
Footnotes
Author contributions: W. Zahra: Designed the study, Carried out data collection and analysis, Wrote the manuscript.
M.Karia: Collected the data, Edited and reviewed the manuscript.
D. Rolton: Supervised study, Edited and reviewed the manuscript.
Funding statement: No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
ICMJE COI statement: D. Rolton reports consultancy from Nuvasive Educational Consultant, which is unrelated to this article.
References
- 1. Gao GF. From "A"IV to "Z"IKV: Attacks from Emerging and Re-emerging Pathogens. Cell. 2018;172(6):1157–1159. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Giorgi PD, Villa F, Gallazzi E, et al. The management of emergency spinal surgery during the COVID-19 pandemic in Italy. Bone Joint J. 2020;102-B(6):671–676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Wuhan City Health Committee (WCHC) Wuhan Municipal Health and Health Commission's briefing on the current pneumonia epidemic situation in our city 2019. http://wjw.wuhan.gov.cn/front/web/showDetail/2019123108989 (date last accessed 14 Jan 2020).
- 4. European Centre for Disease Prevention and Control (ECDC) Rapid Risk Assessment: Outbreak of acute respiratory syndrome associated with a novel coronavirus, Wuhan, China; first update – 22 January 2020. Stockholm: ECDC. 2020. https://www.ecdc.europa.eu/en/publications-data/risk-assessment-outbreak-acute-respiratory-syndrome-associated-novel-coronavirus
- 5. WHO Director-General's opening remarks at the Mission briefing on COVID-19. https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-mission-briefing-on-covid-19-12-march-2020 (date last accessed 12 March 2020).
- 6. https://www.hospitaltimes.co.uk/all-non-urgent-operations-in-england-postponed/
- 7. https://www.nice.org.uk/sharedlearning/the-integrated-pain-and-spinal-service-ipass-a-unique-integrated-and-collaborative-approach-to-persistent-pain-management
- 8. Clinical guide for the management of urgent and emergency spinal surgical patients during the coronavirus pandemic. 14 April 2020, Version 2.
- 9. Giorgi PD, Villa F, Gallazzi E, et al. The management of emergency spinal surgery during the COVID-19 pandemic in Italy. Bone Joint J. 2020;102-B(6):671–676. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Chang Liang Z, Wang W, Murphy D, Po Hui JH. Novel coronavirus and orthopaedic surgery: early experiences from Singapore. J Bone Joint Surg Am. 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11. Long L, Corsar K. The COVID-19 effect: number of patients presenting to The Mid Yorkshire Hospitals OMFS team with dental infections before and during The COVID-19 outbreak. 10.1016/j.bjoms.2020.04.030 [DOI] [PMC free article] [PubMed]
- 12. https://www.telegraph.co.uk/news/2020/04/09/ae-attendances-lowest-point-since-records-began-amid-coronavirus/
- 13. A&E Attendances and Emergency Admissions March 2020 Statistical Commentary. https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2020/04/Statistical-commentary-March-2020-jf8hj.pdf
- 14. Clinical guide for restoration of the spinal surgical services during & after the coronavirus pandemic – BASS.
- 15. https://spinesurgeons.ac.uk/resources/Documents/Member%20News/200514-InformationforPatientsundergoingSpinalInjectionsduringtheCoronaviruspandemic-Update-FINAL.pdf
- 16. https://spinesurgeons.ac.uk/resources/Documents/Member%20News/200514-BASS-ConsentCOVID.pdf