

Abstract
Coronavirus disease 2019 is a global pandemic affecting >3 million people in >170 countries, resulting in >200 000 deaths; 35% to 40% of patients and deaths are in the United States. The coronavirus disease 2019 crisis is placing an enormous burden on health care in the United States, including residency and fellowship training programs. The balance between mitigation, training and education, and patient care is the ultimate determinant of the role of cardiology fellows in training during the coronavirus disease 2019 crisis. On March 24, 2020, the Accreditation Council for Graduate Medical Education issued a formal response to the pandemic crisis and described a framework for operation of graduate medical education programs. Guidance for deployment of cardiology fellows in training during the coronavirus disease 2019 crisis is based on the principles of a medical mission, and adherence to preparation, protection, and support of our fellows in training. The purpose of this review is to describe our departmental strategic deployment of cardiology fellows in training using the Accreditation Council for Graduate Medical Education framework for pandemic preparedness.
Keywords: COVID‐19, education, fellows in training, health education
Subject Categories: Health Services
Nonstandard Abbreviations and Acronyms
- ACGME
Accreditation Council for Graduate Medical Education
- CC
COVID‐19 cardiology consultation team
- C‐FIT
cardiology fellows in training
- COVID‐19
coronavirus disease 2019
- ICU
intensive care unit
- IM
internal medicine
- PES
pandemic emergency status
- PPE
personal protective equipment
Forces beyond your control can take away everything you possess except one thing, your freedom to choose how you will respond to the situation.
When we are no longer able to change a situation, we are challenged to change ourselves.
—Viktor E. Frankl, Man's Search for Meaning
Goals and Vision of the Program
Coronavirus disease 2019 (COVID‐19) is a global pandemic affecting >3 million people in >170 countries, causing >200 000 deaths; 35% to 40% of patients and deaths are in the United States. The COVID‐19 crisis places an enormous burden on patient care and graduate medical education; there are no guidelines for deploying cardiology fellows in training (C‐FIT).1 The purpose of this review is to describe our strategic deployment of C‐FIT using the Accreditation Council for Graduate Medical Education (ACGME) framework for pandemic preparedness (Figure 1).
Figure 1. Graphic representation of the number (N) of positive coronavirus disease 2019 (COVID‐19) patients in Beaumont Health (y axis) as a function of the day of crisis (x axis).
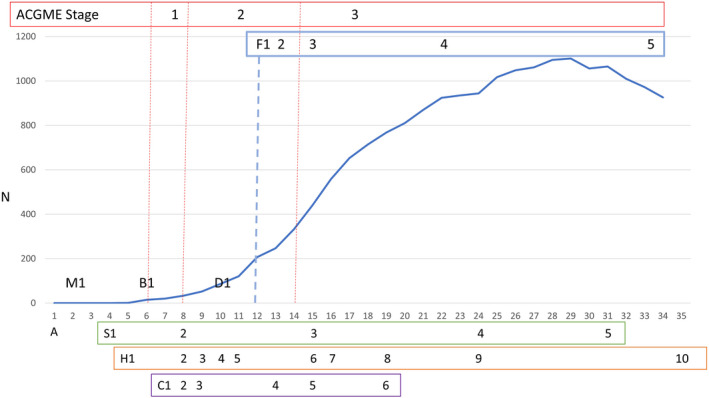
Layered on the graph are the Accreditation Council for Graduate Medical Education (ACGME) stages (red), deployment of cardiology fellows (F; blue), and mitigation strategies used by the state of Michigan (S; green), Beaumont Hospital–Royal Oak (H; orange), and the Department of Cardiovascular Medicine (C; purple). Statewide mitigation strategies include school closures (S1), prohibit public gathering >50 people (S2), orders to shelter at home (S3), permanent school closure (S4), and extend order to shelter at home (S5). Hospital mitigation strategies include cancel conferences, impose travel and visitor restrictions (H1), curbside testing (H2), on‐site testing, no meetings >10 people, cancel medical school rotations (H3), test hospitalized patients (H4), close outpatient offices (H5), suspend outpatient testing (H6), consolidate “clean” intensive care unit (ICU) (H7), expand personal protective equipment availability (H8), implement serologic testing (H9), and implement clinical study of serologic testing for employees (H10). Department mitigation strategies include cancel elective procedures and off‐site electives, change physician rounding to minimize patient contact (C1), nonessential fellows shelter at home (C2), COVID‐19 echocardiographic studies performed as “limited studies” (C3), develop acute coronary syndrome algorithm for COVID‐19 patients (C4), reduce outpatient noninvasive testing (C5), and implement telemedicine (C6). Deployment of cardiology fellows in training to COVID‐19 units include consultation service (F1), expand consultation service to 2 teams (F2), ICU‐line service (F3), internal medicine service (F4), and hybrid ICU service (F5). A indicates cancel the annual session of the American College of Cardiology; B1, first COVID‐19 patient in Beaumont Health; D1, first COVID‐19 death in Beaumont Health; and M1, first COVID‐19 patient in Michigan.
Local Challenges in Implementation
Several challenges had to be overcome to allow us to achieve our goals. These challenges relate to striking a balance between mitigation policies, the demands for patient care, and the needs of C‐FIT.
Mitigation Strategies
Mitigation strategies, mandated by federal, state, hospital, and departmental policies, are designed to attenuate the risk of exposure and transmission (Figure 1).
Demands for Patient Care
Beaumont Health in metropolitan Detroit, MI, has the highest volume of COVID‐19 patients in Michigan; the largest hospital is Beaumont Hospital–Royal Oak (≈1000 beds), which has >50% of the residents and fellows in training in the system. The Department of Cardiovascular Medicine (Royal Oak) has 23 C‐FIT, including 12 in clinical cardiology, 2 in clinical cardiac electrophysiology, 5 in interventional cardiology, 2 in cardiac imaging, and 2 in structural heart diseases.
Impact on Training and Education
On March 24, 2020, the ACGME proposed 3 stages for graduate medical education activities during the COVID‐19 pandemic (Table 1). In stage 3, institutions may declare pandemic emergency status (PES) under the extraordinary circumstances policy (Figure S1), allowing graduate medical education to increase the availability of residents and fellows in training for patient care by suspending traditional educational activities for 30 days.2 Most ACGME requirements are suspended, but there are 4 mandatory requirements for all residents and fellows in training: they must be trained in, and provided with, appropriate personal protective equipment (PPE); they must be supervised on the basis of the clinical situation and their level of experience; they must adhere to duty hour requirements; and they may function within their core specialty (C‐FIT who are board certified in cardiovascular diseases can function as independent cardiologists or internists; C‐FIT who are board certified in internal medicine [IM] can function as independent internists).
Table 1.
Description and Requirements During ACGME Stages of Pandemic Preparedness
| Stage | Description | ACGME Requirements |
|---|---|---|
| Stage 1 | “Business as usual”; no disruption of patient care and educational activities | Common and specialty‐specific requirements remain in effect |
| Stage 2 | Increased clinical need for care of COVID‐19 patients; some residents/FIT may need to shift to clinical activities; minimal disruption of educational activities | Common and specialty‐specific requirements remain in effect; programs may advance telemedicine initiatives and self‐study activities |
| Stage 3 | Most or all of residents/fellows will need to shift to patient care; educational activities will be severely disrupted | Requirements related to duty hours compliance, attending supervision remains in effect. FIT may function in core specialty, programs are required to supply proper PPE and adequate resources |
ACGME indicates Accreditation Council for Graduate Medical Education; COVID‐19, coronavirus disease 2019; FIT, fellows in training; and PPE, personal protective equipment.
Cardiology rotations are directly impacted by ACGME stage (Figure 2). Beginning in stage 2 and certainly by stage 3, our outpatient and inpatient imaging services were severely restricted. Elective procedures in the cardiac catheterization laboratory and clinical cardiac electrophysiology were canceled in stage 2. During the surge in stage 3, the number of hospitalized non–COVID‐19 patients declined, the geographic coronary care unit was converted to a COVID‐19 intensive care unit (ICU), and “usual” criteria for admission to the coronary care unit were modified to preserve all ICU beds for COVID‐19 patients. By stage 3, all C‐FIT in imaging and ECG rotations, clinical cardiac electrophysiology, inpatient service and coronary care unit were reassigned to COVID‐19 units; 2 interventional cardiology C‐FIT remained in the cardiac catheterization laboratory. All activities in the Continuity Clinic were suspended. Standard educational conferences were canceled early in stage 2, resulting from hospital mitigation policies to eliminate gatherings of >10 people, and for C‐FIT on nonessential rotations to shelter at home. Our daily noon teaching conference was replaced by daily virtual videoconferences to update C‐FIT and staff on new developments with COVID‐19 admissions, impact on ICU beds and ventilator requirements, and anticipated deployments of personnel into new areas of responsibility. Reduction in patient contact, elimination of teaching conferences, and restrictions on invasive and noninvasive services had profound impact on training and education.
Figure 2. Rotations of cardiology fellows in training (FIT) during stage 1 to 3 of the coronavirus disease 2019 (COVID‐19) crisis (as indicated by the red boxes).
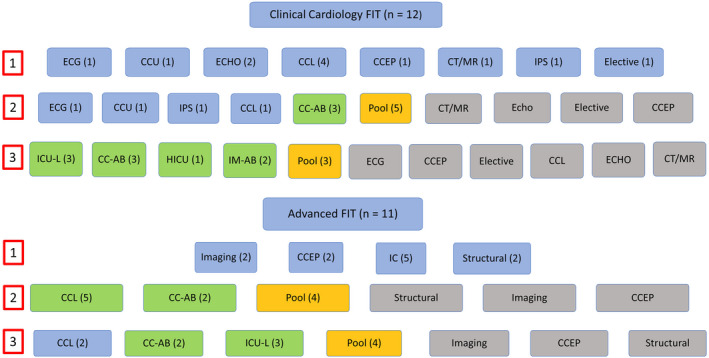
Stage 1 represents “business as usual.” Although stage 2 is characterized as minimal disruption of educational activities, hospital and departmental mitigation strategies required that FIT in “nonessential” activities shelter at home. Stage 3 is characterized by complete disruption of educational activities, mandated by the surge in COVID‐19 admissions that overwhelmed existing manpower. Cardiology FIT (C‐FIT) in the “pool” had several responsibilities, including backup for others in case of absence, remote services (adjudicate need for ECGs or echocardiograms and evaluate corrected QT interval for COVID‐19 patients), participate in C‐FIT deployment decisions, and participate in research or quality assurance projects. FIT assigned to coronary care unit (CCU) and inpatient service (IPS) were reassigned to COVID‐19 cardiology consultation teams (CCs) A and B. Blue indicates usual fellowship rotations; gray, inactive fellowship rotations; green, COVID‐19 patient care responsibilities; and yellow, pool. CCEP indicates clinical cardiac electrophysiology; CCL, cardiac catheterization laboratory; CT/MR, cardiac computed tomography/magnetic resonance imaging; ECHO, echocardiogram; HICU, hybrid intensive care unit; IC, interventional cardiology; ICU‐L, intensive care unit team for central lines (all intensive care units were COVID‐19 intensive care units); and IM‐AB, internal medicine teams A and B.
Other Considerations
C‐ FIT raised concerns about hazard pay. Although we support these concerns, lobbying for enhanced pay and benefits should begin with nurses and others on the “frontline.” However, we abide by the American Heart Association recommendations that C‐FIT should not be placed in direct COVID‐19 care without adequate PPE.3
Design of the Initiative
Although it is easy to understand the negative impact on learning activities, the crisis may create opportunities to enhance experience (Table 2). From the outset, our departmental approach was based on 2 principles: consider the care of our patients as a medical mission and advocate for our C‐FIT.
Table 2.
Potential Learning Opportunities in the ACGME Core Competencies During C‐FIT Deployment During the COVID‐19 Crisis
| Competency | Description | Learning Opportunity |
|---|---|---|
| Patient care and procedural skills | Compassionate and effective care, perform all procedures considered essential for the area of practice | New aspects of critical care, ventilator management, MOSF, central line placement, infection control; enhance understanding of end‐of‐life issues |
| Medical knowledge | Cognitive understanding and application to care | Cardiac complications of COVID‐19, use of PPE, inflammatory components to acute cardiopulmonary failure |
| Practice‐based learning and improvement | Investigate and evaluate care of patients, assimilate scientific evidence, continuously improve patient care | New applications for telemedicine, videoconferencing, experiential learning, simulation; understanding the use of novel and nonapproved therapies during a pandemic; prioritizing care and resources |
| Interpersonal skills and communication | Effective interpersonal and communication skills with patients, families, and healthcare team | Collaborative team‐based care with critical care, emergency medicine, nursing staff, hospice, and palliative care services; end‐of‐life discussions and decisions; learn to deal with personal stress and anxiety as they impact your behavior |
| Professionalism | Adhere to ethical principles and be sensitive to diversity | Understanding patient and family isolation; willingness to take on unexpected responsibilities and clinical roles; understanding the needs of others during a pandemic, including nursing staff and others |
| System‐based practice | Awareness and responsiveness to the larger healthcare system, ability to call on other resources to provide optimal care | The role of cardiology in a larger system of care, adapt to disruption of systems of care and organizational structure; need for team work to understand how to improve the system of care, effacement of differences between specialties to solve problems in logistics and patient care, emergency preparedness, understand available resources to enhance well‐being; learn to adapt to change |
ACGME indicates Accreditation Council for Graduate Medical Education; C‐FIT, cardiology fellows in training; COVID‐19, coronavirus disease 2019; MOSF, multiorgan system failure; and PPE, personal protection equipment.
The Department as a Medical Mission
The spirit of selflessness applies to care of our patients, without expectation of special benefits. Although the ACGME Extraordinary Circumstances policy provides hospitals with the authority to reassign C‐FIT to roles outside our specialty, our approach was to solicit volunteers and to assign these individuals into areas in which their skills were matched with specific needs for patient care. All 23 C‐FIT volunteered to participate in the medical mission.
Prepare, Protect, and Support Our C‐FIT
Preparation for the COVID‐19 pandemic requires careful planning and flexibility because of rapid changes on the ground. Such planning should start before stage 1, if possible. All C‐FIT express fear of infection and transmission; strategies for protection are to minimize direct contact between patients and C‐FIT and to train C‐FIT in the use of PPE (Table 3). Stress and anxiety are fundamentally related to fear, which can be ameliorated by education and learning; online resources are available to C‐FIT to provide general and specific information on safety, family and mental health, patient care, and adapting clinical care to the COVID‐19 environment (Table S1). These efforts lead to personal growth and deeper satisfaction about being involved in this medical mission.
Table 3.
Departmental Responsibilities for C‐FIT
| Responsibility | Description |
|---|---|
| Patient care | Provide appropriate supervision to ensure optimal patient care. |
| Prepare | Preparation should start at least 3 wk before initiation of stage 3; organize and implement planning strategies for FIT. Work with hospital to identify specific needs, and match needs with skills of FIT. |
| Protect | Maintain social distance, assume each patient is COVID‐19 positive, wear appropriate PPE, one‐to‐one training on use of PPE by experienced staff, maintain emergency “backup” supply of PPE for FIT. |
| Support | Stress and anxiety are fundamentally related to fear, which can be attenuated by education and learning. Establish effective protocols for “virtual” communication and rapid dissemination of information using web‐based systems. Program directors must be available 24/7 during pandemic to ensure adequate resources to support the mental and physical well‐being of their FIT. |
C‐FIT indicates cardiology FIT; COVID‐19, coronavirus disease 2019; FIT, fellows in training; and PPE, personal protection equipment.
Implementation of the Initiative
The rapid increase in demand for patient care mandated early identification of a strategic group to identify the hospital's needs and to match those needs by strategic deployment of C‐FIT on the basis of individual expertise and skills.
Leadership Group in Cardiology
The leadership role was held by the program director (M.J.G.), who maintained direct communication with the hospital's residency redeployment team and graduate medical education director 3 to 4 times daily. The chief fellow (R.B.) and the clinical chief (A.D.B.) ensured coordination of responsibilities between C‐FIT and cardiology attendings. Incorporation of advanced C‐FIT was facilitated by the program directors of clinical cardiac electrophysiology (B.D.W.) and interventional cardiology (R.D.S.), and all activities were supervised by the chairman (S.R.D.). Strategy meetings occurred 1 to 2 times daily by telephone conference or Zoom (Zoom Video Communications, San Jose, CA). Depending on severity of illness, patients were assigned by the residency redeployment team to regular medical floors, progressive care units, or ICUs. In early stage 3, all ICU beds (100 beds, >80% on ventilators) and half of non‐ICU beds were occupied by COVID‐19 patients. On March 25, 2020, the hospital requested a declaration of PES, followed by widespread deployment of residents and C‐FIT to COVID‐19 units.
Strategic Deployment of C‐FIT
Our department began to deploy C‐FIT ≈48 hours before the PES declaration. Cardiologists have unique expertise that make us superbly qualified to serve during the COVID‐19 crisis (Table 4, Figure 3).
Table 4.
Specific Roles of C‐FIT During the COVID‐19 Crisis
| Role | Description |
|---|---|
| Consultant | C‐FIT managed cardiology consultations for all COVID‐19 units (ICU, PCU, RMF). Reasons include ACS, ↑biomarkers, AF, CHF, MOSF, VDRF, AKI, VTE, ↑QT. Rely on chart review, telephone contact with the patient, and direct communication with primary service. The consultation teams consisted of ≥1 cardiology attendings and ≥1 C‐FIT. |
| ICU‐L | C‐FIT placed central and arterial lines; participated in daily rounds with the ICU team and provided collaborative critical care management of ICU patients. C‐FIT assisted critical care teams with management of cardiovascular comorbidities, emergency procedures, and handheld portable echocardiography when necessary. C‐FIT were supervised by critical care attendings. C‐FIT also responded to cardiac emergencies in non–COVID‐19 patients (especially during night shift). |
| Medical service | C‐FIT function as a member of the primary IM hospitalist team for the general medical COVID‐19 services. The teams consisted of 1 cardiology attending, 1 C‐FIT, and physician extenders. |
| CCU | Non–COVID‐19 cardiac ICU patients are managed by the COVID‐19 cardiology consultation teams during the day and covered by the C‐FIT on the ICU‐L team at night. |
| Other | C‐FIT performed remote ECG interpretation and assessment of QT intervals; adjudicated need for echocardiography and 12‐lead ECGs on COVID‐19 patients, assisted with “virtual” COVID‐19 consultations to support on‐site CCs, participated in research and quality assurance projects as permissible. |
ACS indicates acute coronary syndrome; AF, atrial fibrillation; AKI, acute kidney injury; CC, COVID‐19 cardiology consultation team; CCU, coronary care unit; C‐FIT, cardiology fellows in training; CHF, congestive heart failure; COVID‐19, coronavirus disease 2019; ICU, intensive care unit; ICU‐L, ICU team for central lines; IM, internal medicine; MOSF, multiorgan system failure; PCU, progressive care unit; RMF, regular medical floor; VDRF, ventilator‐dependent respiratory failure; and VTE, venous thromboembolism.
Figure 3. Deployment of cardiology attendings and fellows in training (FIT) during stages 2 and 3 of the coronavirus disease 2019 (COVID‐19) crisis.
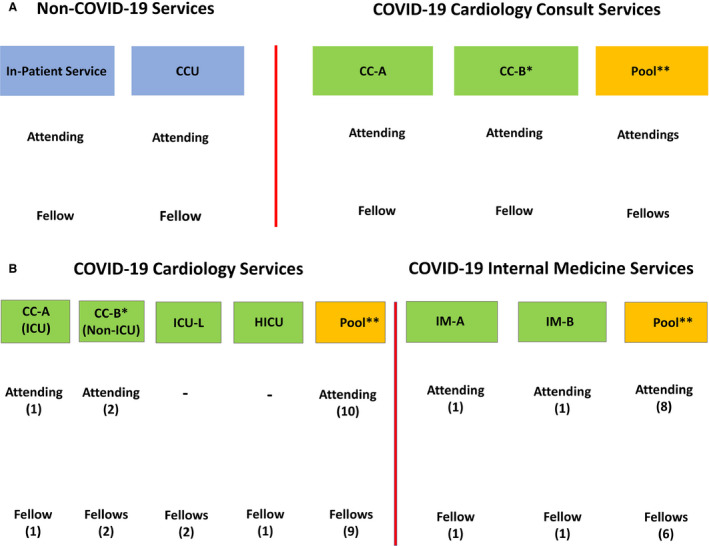
A, “Usual” non–COVID‐19 cardiology services and new COVID‐19 cardiology consultation services (consultation teams A and B) during stage 2. Each service was assigned 1 cardiology attending and 1 FIT. B, Deployment of cardiology attendings and FIT during stage 3 of the COVID‐19 crisis. At this point, there was complete disruption of all usual cardiology rotations, and all 23 fellows had assigned roles on COVID‐19 services. By the peak of stage 3, cardiology attendings and FIT were assigned to roles on 1 of 4 COVID‐19 cardiology services or 1 of 2 COVID‐19 internal medicine services. The numbers in parentheses represent the number of physicians assigned to the rotation. *The attending and FIT on team B were fully deployed when the census on team A approached 25 patients. Before that time, team B was available as “backup.” **The pool included attendings and FIT who were not assigned to one of these clinical services, to serve as additional clinical needs or to replace others who were ill. Unlike the consultation services, members of internal medicine teams A and B had primary responsibility for the care of COVID‐19 patients. CC‐A and CC‐B indicate COVID‐19 cardiology consultation teams A and B; and CCU, coronary care unit.
C‐FIT as Consultants
Cardiovascular complications occur in 25% to 50% of COVID‐19 patients, and the need for cardiology consultants requires more resources than any other cardiology activity. Cardiology consultations were performed by the COVID‐19 cardiology consultation teams (CCs). When possible, consultations were performed by chart review and telephone contact with the patient; the attending may examine the patient without the C‐FIT, if needed. The consultation report is generated by the C‐FIT; reasons for consultation are similar to non–COVID‐19 patients (acute coronary syndromes, asymptomatic increase in cardiac biomarkers, rapid atrial fibrillation, other arrhythmias, and assessment of congestive heart failure superimposed on a background of pulmonary infiltrates and dyspnea). In the ICUs, more complex assessments are required (multiorgan failure, respiratory failure, shock, renal injury, and venous or arterial thrombosis). QT prolongation emerged as a frequent issue for patients on hydroxychloroquine and azithromycin.
C‐FIT in the COVID‐19 ICUs
The need for central and arterial lines in the ICUs led to the formation of the ICU team for central lines. C‐FIT were selected on the basis of their skill in rapid placement of central lines. Additional daytime responsibilities included rounds and assisting in critical care management. After hours, the C‐FIT responded to cardiac emergencies anywhere in the hospital. Full PPE was required when entering patient rooms, and N95 masks were required while on the units. Attending supervision was provided by pulmonary or surgical critical care.
C‐FIT on IM Services
In contrast to consultants, there was an expanding need for attending cardiologists and C‐FIT as IM hospitalists. These IM teams included 1 attending cardiologist, 1 C‐FIT, 1 to 2 physician extenders, and nursing staff. Although the ACGME provided guidance to allow C‐FIT to serve as IM attendings, we used C‐FIT as supervising residents. Their strong base of knowledge in IM and their exceptional supervisory and organizational skills were ideally suited to lead a team of physician extenders and non‐IM residents. This strategy allowed them to focus on patient management and communication with patients and families while minimizing their direct exposure to COVID‐19 patients. The cardiology attending was the primary physician for these COVID‐19 patients (requiring full PPE for each patient encounter); C‐FIT did not enter patient rooms. N95 masks were required for all C‐FIT on IM units. The C‐FIT determined treatment plans, triaged admissions and transfers, wrote notes, and managed consultants; physician extenders may assist. Daily communication with the patient and families was by telephone or FaceTime (Apple, Inc, Cupertino, CA).
C‐FIT in the Hybrid ICU
Because of 100% occupancy of ICUs by COVID‐19 patients, contingency plans required conversion of progressive care units to hybrid ICUs to accommodate patients on ventilators. C‐FIT shared night coverage with fellows in training from other specialties. C‐FIT had direct patient exposure, so full PPE was required.
C‐FIT and Cardiovascular Emergencies
There is an absolute need to maintain an immediate response to cardiovascular emergencies, whether arising from the emergency department or the hospital, irrespective of COVID‐19 status (Table 5). Guidelines for management of acute cardiovascular emergencies were developed by the department chair in collaboration with department leaders (Figures S2 through S4).
Table 5.
Coverage for Cardiovascular Emergencies and Urgent Patient Evaluations
| Area | Shift | First‐Degree Contact | Second‐Degree Contact |
|---|---|---|---|
| ED | 7 am–7 pm | ACS team | STEMI: F‐IC; other: F‐CC |
| 7 pm–7 am | F‐ICU‐L or F‐HICU | STEMI: F‐IC; other: attending | |
| Hospital | 7 am–7 pm | F‐CC | STEMI: F‐IC; other: attending |
| 7 pm–7 am | RRG | STEMI: F‐IC; other: F‐ICU‐L or F‐HICU |
ACS indicates team of nurse clinicians to evaluate patients with acute coronary syndromes and other cardiac emergencies; ED, emergency department; F‐CC, cardiology fellows on the coronavirus disease 2019 consultation services; F‐HICU, cardiology fellows on the hybrid intensive care unit; F‐IC, interventional fellows in the cardiac catheterization laboratory; F‐ICU‐L, fellow on ICU line team; RRG, rapid response group consisting of nurse clinicians and physician extenders; and STEMI, ST‐segment–elevation myocardial infarction.
Other Activities
C‐FIT had brief periods of “downtime” between shifts. Even at home, C‐FIT were engaged in ECG interpretation by Skype Communications (Microsoft Corporation, Palo Alto, CA), screening the need for ECGs and echocardiograms, obtaining measurement of QT intervals, or performing research or quality assurance projects. It is possible to adapt the educational environment by incorporating virtual learning and telemedicine.4, 5
Summary of C‐FIT Assignments by Stage
Stage 1 only lasted 2 days (Figure 1); we maintained the usual structure of our clinical services (Figures 2 and 3, Table 6). Stage 2 only lasted 6 days, which was characterized by a rapidly increasing demand for cardiology consultations. During this stage, most activities were disrupted by mitigation strategies, rather than by C‐FIT redeployments. We anticipated additional demands for cardiology consultations, so we created 2 consultation teams (CC‐A and CC‐B) and pools of attendings and C‐FIT in case of unexpected illness. CC‐A (ICU consultations) and CC‐B (non‐ICU consultations) were deployed within 24 hours of each other. Our entry into stage 3 occurred when residency redeployment team requested immediate deployment of C‐FIT to provide coverage on ICU team for central lines; this request was 24 hours before the ACGME framework was announced and 48 hours before approval of PES. By this time, C‐FIT educational programs were completely disrupted, and except for 2 interventional cardiology C‐FIT in the cardiac catheterization laboratory, all C‐FIT were assigned to COVID‐19 units. Additional C‐FIT were assigned to CC‐B to meet growing needs for consultations. The IM department was overwhelmed, so 2 IM teams (IM‐A and IM‐B) were each assigned to a cardiology attending and C‐FIT to serve as the “primary” hospitalists. There was 100% occupancy of the ICUs, so C‐FIT were assigned to cover hybrid ICU patients, including those on ventilators. By the peak in stage 3, all C‐FIT were covering the COVID‐19 unit.
Table 6.
Deployment Requirements at Peak of COVID‐19
| Rotation | Cardiology Attending | Cardiology FIT | Shiftsa | Duration, d | Responsibility | ||
|---|---|---|---|---|---|---|---|
| On Service | Poolb | On Service | Poolb | ||||
| CC‐AB | 2 | 8 | 3 | 8 | 7 am–7 pm | 7 | Cardiology consultations on COVID‐19 patients in ICU and medical units; manage CCU patients |
| ICU‐L | ··· | ··· | 1 | 6 | 7 am–7 pm | 4 | Manage COVID‐19 ICU patients, lines, rounds |
| ··· | ··· | 1 | 6 | 7 pm–7 am | 4 | Cover COVID‐19 ICU patients and lines, cover cardiac emergencies | |
| IM‐AB | 2 | 8 | 2 | 8 | 7 am–7 pm | 7 | Primary care of COVID‐19 units |
| HICU | ··· | ··· | 1 | 4 | 7 pm–7 am | 4 | Primary care of HICU patients; cover cardiac emergencies |
| CCL | 2 | 22 | 2 | 5 | 7 am–7 pm | 7 | Only IC FIT; emergency and urgent procedures |
| 1 | 22 | 1 | 5 | 7 pm–7 am | 7 | Only IC FIT; emergency procedures | |
CC‐AB indicates COVID‐19 cardiology consultation teams A and B; CCL, cardiac catheterization laboratory; CCU, coronary care unit; COVID‐19, coronavirus disease 2019; FIT, fellows in training; HICU, hybrid ICU (non‐ICU setting includes sick patients on and off ventilators); IC, interventional cardiology; ICU, intensive care unit; ICU‐L, ICU team for central lines; and IM‐AB, internal medicine teams A and B.
Shifts on CC‐AB and IM‐AB were staggered between the attending physician and the FIT, to ensure continuity of care and to avoid situations where the attending and FIT were changing service on the same day.
Pools of physicians were selected to ensure continuity of service, rather than include all attendings and FIT for all services.
Translation to Other Settings
The COVID‐19 pandemic has created a crisis of extraordinary proportions that has never been witnessed during our lifetimes. The pandemic has impacted the lives of millions of people around the world and is still spreading across the United States. We wanted to take a deep dive into the impact on our C‐FIT. We recognize that each program has its own unique profile, but we hope that this document provides useful insights and a template for action, particularly as C‐FIT are deployed into areas of unexpected responsibility. It is essential for programs to define their leadership structure, objectives, and priorities, to ensure a flexible response with appropriate contingency plans. We hope it is possible to look at this crisis as a life‐changing experience, including many things we would like to forget, but also some things that have allowed us to grow as humans and as physicians.
Summary of the Experience, Future Directions, and Challenges
It appears that we have passed the peak of the COVID‐19 crisis; 4 C‐FIT and 3 cardiology attendings developed illnesses consistent with coronavirus, although none required hospitalization and all tested negative. The prospect for returning our fellowship to normal is an unrealized dream, and there are new and persistent challenges ahead. The hospital plans to renew our PES for another 30 days, and the pace of unwinding will differ for cardiology compared with other specialties. We anticipate a “new normal,” which may include retaining several mitigation strategies, incorporating telemedicine into our clinical and educational practices, modifying how we conduct interviews and recruitment for new C‐FIT, and encouraging patients and families to return to our hospital, despite the magnitude of the crisis we face.
Sources of Funding
None.
Disclosures
None.
Supporting information
Table S1 Figures S1–S4
Acknowledgments
We would like to acknowledge the selflessness and dedication of our cardiology fellows: postgraduate year (PGY)‐4: Andres Palomo, MD, Akash Rusia, MD, Adam Tawney, DO, and Amit Vira, MD; PGY‐5: Travis Tagami, DO, Richard Gaines, MD, Thomas O'Connell, MD, and Daniel Tim, MD; PGY‐6: Richard Bloomingdale, MD*, Ashish Chaddha, MD, Amy Mertens, DO, and Jason Schott, DO; PGY‐7: Michael Ashbrook, MD*, Shengchuan Dai, MD, Korey Haddox, DO, Jay Mohan, DO, Sara Karnib, MD, Amit Sharma, MD, Dinesh Sharma, DO, and Craig Tucker, MD; PGY‐8: Christopher Bradley, DO, Jacob Goldstein, MD, and Daniel Rothschild, MD (*Chief Fellows). Drs Mertens, Mohan, and Bloomingdale kindly provided the list of resources in Table S1.
(J Am Heart Assoc. 2020;9:e017443 DOI: 10.1161/JAHA.120.017443.)
For Sources of Funding and Disclosures, see page 9.
References
- 1. Shashank SS, Sharma G, Cullen MW. The crucible of crisis: fellows’ in training and early career cardiologists’ responses to the COVID‐19 pandemic. J Am Coll Cardiol. 2020;75:2627–2629. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2. Three stages of GME during the COVID‐19 pandemic. Accreditation Council for Graduate Medical Education. https://acgme.org/COVID-19/Three-Stages-of-GME-During-the-COVID-19-Pandemic. Accessed April 30, 2020.
- 3. Harrington RA, Elkind MSV, Benjamin IJ. Protecting medical trainees on the COVID‐19 frontlines saves us all. Circulation. 2020;141:e775–e777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. DeFillippis EM, Schmidt S, Reza N. Adapting the educational environment for cardiovascular fellows‐in‐training during the COVID‐19 pandemic. J Am Coll Cardiol. 2020;75:2630–2634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Almarzooq Z, Lopes M, Kochar A. Virtual learning during the COVID‐19 pandemic: a disruptive technology in graduate medical education. J Am Coll Cardiol. 2020;75:2635–2638. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Table S1 Figures S1–S4