

Abstract
This scientific statement summarizes the current state of knowledge related to interstage home monitoring for infants with shunt‐dependent single ventricle heart disease. Historically, the interstage period has been defined as the time of discharge from the initial palliative procedure to the time of second stage palliation. High mortality rates during the interstage period led to the implementation of in‐home surveillance strategies to detect physiologic changes that may precede hemodynamic decompensation in interstage infants with single ventricle heart disease. Adoption of interstage home monitoring practices has been associated with significantly improved morbidity and mortality. This statement will review in‐hospital readiness for discharge, caregiver support and education, healthcare teams and resources, surveillance strategies and practices, national quality improvement efforts, interstage outcomes, and future areas for research. The statement is directed toward pediatric cardiologists, primary care providers, subspecialists, advanced practice providers, nurses, and those caring for infants undergoing staged surgical palliation for single ventricle heart disease.
Keywords: AHA Scientific Statements, cardiovascular abnormalities, caregivers, infant, univentricular heart
In the recent era of congenital heart disease management, no defect has undergone more dramatic improvement in outcomes than hypoplastic left heart syndrome (HLHS) and related variants that require staged palliation for single ventricle heart disease (SVHD) with aortic hypoplasia. Stage 1 palliation (S1P) includes the surgical Norwood procedure or the hybrid alternative. The Norwood procedure consists of atrial septectomy, Damus‐Kaye Stansel connection of pulmonary and aortic roots, aortic arch reconstruction, ligation of the ductus arteriosus, and placement of a modified Blalock‐Taussig shunt or right ventricle to pulmonary artery shunt. The hybrid procedure includes stenting of the ductus arteriosus, pulmonary artery banding, and balloon atrial septostomy. Also included in the group of shunt‐dependent SVHD patients are single ventricle lesions that require surgical systemic‐to‐pulmonary shunt placement or stenting of the ductus arteriosus. Advancements in care span operative, postoperative, and interstage management. Before 2000, the postdischarge care provided after Norwood S1P, lacked the level of surveillance needed to manage this high‐risk population. Due to published mortality rates as high as 16% between discharge after S1P and stage 2 palliation (S2P), Ghanayem and colleagues (2003) developed an innovative home monitoring strategy.1, 2 The foundations of interstage home monitoring (IHM) are routine caregiver home surveillance of oxygen saturations, enteral intake, and weight change during the interstage period; early healthcare team notification of any abnormal parameters labeled as “red flags”; or other changes in clinical condition. This heightened in‐home surveillance augments conventional outpatient management to detect physiologic changes that may precede hemodynamic decompensation in high‐risk infants with shunt‐dependent SVHD. IHM programs, using family and healthcare provider engagement, have led to improved survival to S2P for infants who have undergone either Norwood procedure or hybrid procedure S1P, for HLHS and related variants.3, 4, 5
Shunt‐Dependent Physiology and Associated Interstage Risk Factors
The physiologic challenge associated with shunt‐dependent single ventricle, also referred to as functionally univentricular heart disease, is the persistence of parallel circulation that extends beyond the surgical hospitalization to shunt takedown at S2P. Inherent to parallel circulation are critical relationships between oxygen consumption, pulmonary blood flow, systemic blood flow, partially oxygenated arterial blood (Sao 2), systemic venous saturation, and pulmonary venous saturation. Sao 2 depends on the balance between systemic and pulmonary flow, lung health, and systemic venous saturation. The most life‐threatening risk associated with shunt‐dependent SVHD, particularly with a modified Blalock‐Taussig shunt or ductus arteriosus stent, is an abrupt reduction in pulmonary blood flow, thus highlighting the importance of monitoring Sao 2 trend during the interstage period. A more gradual reduction in pulmonary blood flow or pulmonary venous desaturation will also lead to a fall in Sao 2. This reduction in Sao 2 is dependent on an ability to increase systemic blood flow to maintain tissue oxygen delivery. Inability to augment systemic blood flow will result in lower systemic venous saturation and further reduce Sao 2. The inefficiency of parallel circulation combined with cyanosis, limited myocardial reserve, and autonomic responses to stress, places the infant with shunt‐dependent circulation at risk for critical impairment of oxygen delivery.
Multiple cardiac and noncardiac causes have been implicated in interstage death. Most common are residual or recurrent lesions and development of intercurrent childhood illness. Restrictive atrial communication, arch obstruction, obstructed shunt flow, pulmonary artery distortion, atrioventricular valve insufficiency, and arrhythmias have each been associated with interstage mortality (Figure 1).1, 4, 6, 7 Of the ≈2000 infants with shunt‐dependent SVHD enrolled in the National Pediatric Cardiology Quality Improvement Collaborative (NPC‐QIC) Phase 1 registry, 17% had at least 1 unplanned interstage intervention with the majority being catheter‐based. The most common surgical reintervention was modified Blalock‐Taussig shunt revision or placement, and the most common catheter intervention was on the aortic arch.6 The Congenital Heart Surgeons’ Society identified a 25% incidence of arch reintervention at a median age of 4.3 months in those who had Norwood palliation.7 Single center reports and the multicenter Pediatric Heart Network Single Ventricle Reconstruction trial report a higher incidence of interstage mortality in infants who underwent modified Blalock‐Taussig shunt compared with the right ventricle‐to‐pulmonary artery shunt.8 Whether the mechanism of increased mortality with the modified Blalock‐Taussig shunt is predominantly because of impairment of coronary perfusion or shunt obstruction remains unknown. Noncardiac causes such as poor feeding and acquired childhood gastrointestinal or respiratory illnesses that result in hypovolemia or acute hypoxemia have also been implicated as causes for interstage death.9, 10 Any of the aforementioned processes may critically influence systemic vascular resistance, increase metabolic demands, and potentiate progressive hypoxia or shock, either hypovolemia or cardiogenic, in the infant with S1P physiology.
Figure 1. Pathophysiology associated with changes in oxygen saturation for shunt‐dependent single ventricle heart defects.
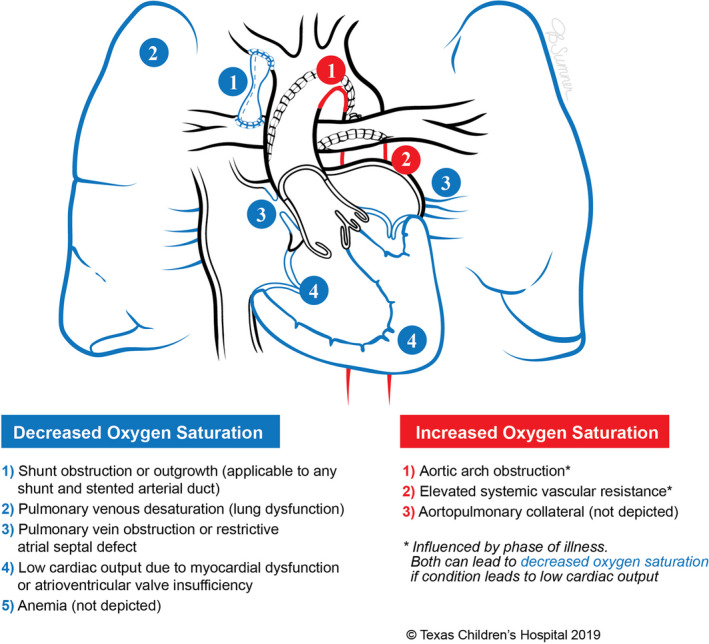
The figure illustrates differential diagnoses to consider when oxygen saturation thresholds are breached after Norwood palliation with a modified Blalock‐Taussig shunt for hypoplastic left heart syndrome. Similar pathophysiologic considerations are applicable to the right ventricle to pulmonary artery shunt, hybrid palliation, and other shunt‐dependent single ventricle variants. Used with permission from Texas Children's Hospital. Copyright © 2019 Texas Children's Hospital.
Interstage Home Monitoring Metrics and Red Flags
IHM was initially implemented for the purpose of reducing mortality, and this continues to be the most reported metric.3, 10, 11, 12 In‐home use of pulse oximetry to detect excessive hypoxia and infant scales to detect weight loss remain standards of monitoring. Tracking weight can identify dehydration as well as somatic growth failure which has been modifiable.12, 13 Additional interstage metrics include heart rate trends, adequate oral intake (≥100 mL/kg per day), and occurrence of major events with serious, or even fatal, consequences (eg, cardiac arrest, arrhythmias, sepsis, or thrombotic events).
Healthcare team consensus determined physiologic parameters to be monitored, and concerning changes in those parameters are denoted as “red flags” (Table 1). Any breach of these criteria detected by caregivers should trigger notification of the healthcare team. These parameters may vary somewhat based on infant‐specific physiology or program‐specific management but commonly caregivers are instructed to notify the healthcare team if any red flags or other unusual symptoms arise.
Table 1.
| Red Flags |
|---|
| Oxygen saturation ≤75%a |
| Failure to gain 20 g (=0.02 kg) in 3 d |
| Weight loss ≥30 g (=0.03 kg) |
| Enteral intake <100 mL/kg per d |
| Cyanosis, pallor |
| Irritable, fussy |
| Diarrhea or vomiting |
| Increased sweating |
| Respiratory changes (tachypnea, distress) |
| Temp >100.4°F |
Unanticipated increase in oxygen saturation from baseline (eg ≥90% in infant with Norwood physiology) should be considered a red flag.
Inpatient Preparation for Interstage Home Monitoring
Medical Readiness for Discharge
Criteria for discharge to IHM vary by institution and some infants may not be candidates for home management. At a minimum, infants should demonstrate cardiac stability with acceptable oxygen saturations, adequate weight gain on a stable feeding regimen, and no inpatient breach of red flag criteria for monitored metrics. Before discharge echocardiography should be completed to assess for known risk factors for adverse outcomes such as tricuspid regurgitation and ventricular dysfunction,1 as well as residual lesions such as aortic coarctation, atrial septal restriction, and shunt or branch pulmonary artery stenosis.16, 17 Knowledge of the infant's hospital course is also critical to determine readiness for discharge. A history of genetic abnormality or preterm gestation, extracardiac abnormalities, arrhythmias, prolonged dependence on inotropic support, and the need for extracorporeal membrane oxygenation, have all been associated with adverse outcomes following S1P.4, 9, 10, 16 Thus, selective inpatient interstage management has been proposed and is a strategy used at some centers for infants considered high risk.18
Home Equipment
In preparation for discharge caregivers are taught the necessary skills to care for and monitor their infant at home.19, 20 Essential IHM equipment includes a portable pulse oximeter with infant‐appropriate probes and a digital infant scale sensitive to weight changes of ≤10 g.21 Assistance with obtaining equipment and other home supplies or services can be provided by a case manager. In some regions, the cost of pulse oximeters and scales may be covered by insurance and provided by suppliers of durable medical equipment. Occasionally a letter of medical necessity stating the high risk of morbidity and mortality is needed. At some centers equipment or tablet‐based devices are purchased using charitable donations or by the institution and loaned to families for the duration of the interstage period. Provision of equipment and resources needed to support IHM may prove challenging and cost prohibitive at any given center.
Caregiver Education
Caregivers require training in equipment use, daily measurements, recording (eg, binder with paper logs, home telemedicine system, cellular phone application), and interpreting data (eg, oxygen saturation, heart rate, weight, nutritional intake) based on infant–specific parameters and previous trends.10, 14, 22, 23, 24, 25 Beginning this education early in the inpatient stay allows time for caregivers to become competent and confident in their ability to perform IHM tasks. They must learn to accurately calculate daily nutritional intake and weight changes.4, 10, 12, 24 Depending on the recording application used, selected programs can electronically calculate these changes, follow trends and provide automatic red flag notifications.22, 23, 24 In addition, medical knowledge of their infant's condition, medication administration, general infant care, preparation of calorically enhanced formula, feeding administration (eg, oral, nasogastric, or gastrostomy tube), schedules for follow‐up appointments, and IHM team contacts must be provided in writing (Table 2).14, 25, 26
Table 2.
| Topic | Content | Resources/Evaluation Method |
|---|---|---|
| Individualized cardiac defecta | [ ] Review diagram of cardiac defect, surgical interventions, oxygen saturations, and future surgeries |
[ ] Written material/diagrams [ ] Peer‐reviewed web links for CHD information |
| IHM equipment and plan of carea |
[ ] Explain IHM program purpose, goals, and participation requirements[ ] Review IHM team members and contact information [ ] Review equipment use (eg, scales, pulse oximeter, oxygen—if needed)[ ] Review clinical data entry system (eg, paper or web‐based with technical support)[ ] Red flag list and action plan[ ] Emergency department plan |
[ ] Written material and demonstration of equipment use with teach back[ ] Recording saturation, heart rate, weight change, and intake volume total[ ] Verbalize red flags [ ] Store a copy of the emergency action plan in IHM binder and/or cellular phone |
| General postoperative carea |
[ ] Medication list and schedule [ ] Written nutrition plan [ ] Enteral feeding supplies [ ] Activity/sternal precautions [ ] Incisional care [ ] Infection prevention [ ] Immunization plan (include Synagis) [ ] Infectious endocarditis prophylaxis [ ] Infant CPR training [ ] General newborn care (eg, bathing, cord care, temperature, normal development, car seat test) |
[ ] Written material on content listed and other infant care [ ] Demonstration of preparing correct dosing of medication[ ] Preparation of calorically enhanced breast milk or formula[ ] Demonstrate feeding tube care and pump use [ ] Demonstrate normal infant care and verbalize when to call the provider |
| Scheduled appointmentsa (goal of infant seeing a provider within 72 h of discharge) |
[ ] Primary care provider [ ] Pediatric cardiologist [ ] IHM clinic [ ] Other subspecialist (eg, genetics, GI, ENT, general surgery, neurology)[ ] Cardiac neurodevelopmental clinic |
[ ] Written material with contact Information for all providers/clinics telephone numbers[ ] IHM contact information on emergency card and stored in IHM binder or cellular phone |
| Discharge Materialsa | [ ] Caregiver keeps a copy of discharge instructions, medication list, hospital discharge summary in accessible locations such as diaper bag, IHM binder, or cellular phone | [ ] Written material (copy of discharge summary) |
| Support group informationa | [ ] Provide local, and national CHD support group websites | [ ] Written material with downloadable links |
| Competency in care | [ ] Caregiver rooms in for 24 h (minimum) to demonstrate independent care before discharge | [ ] Nursing staff and IHM team determination of safe and competent care |
CHD indicates congenital heart disease; CPR, cardiopulmonary resuscitation; ENT, ears, nose, and throat; GI, gastrointestinal; and IHM, interstage home monitoring.
Provide information in family/caregiver's native language.
Care demands and other family stressors, may impair or delay caregiver learning and possibly delay discharge.19, 26, 27, 29 The healthcare team should allow adequate time for training and monitor for any indications that the caregivers may require additional support or retraining. Training >1 caregiver is preferable and allows support and respite for the primary caregiver. Caregivers should repeatedly practice these skills before discharge and be able to verbalize a stepwise process for action should a red flag or concerning symptom be identified that requires reporting. A “rooming in” period for 24 to 48 hours in the hospital is often encouraged to assess the caregiver's ability to independently perform all aspects of care.15 This experience allows caregivers to imitate a home environment with the healthcare team available for support and can ease the transition to home. Various institutional‐specific educational forms or tools have been developed to assist families with identifying red flags and infant‐specific parameters and have been translated into multiple languages.15, 27 NPC‐QIC has also developed comprehensive standardized clinical care processes, resources, and tools for IHM education.28, 30
Coordination With Healthcare Providers
Well‐coordinated, comprehensive communication of the hospitalization, surgical palliation, and IHM plan of care between all healthcare providers is vital for effective management of the highly complex, fragile infant in the outpatient setting.10, 14, 17, 25, 30 Building a close, multidisciplinary collaboration between the caregivers, the IHM team, and healthcare providers in the medical home is advantageous in facilitating a supportive network for the IHM period.19, 25 In addition to sharing a written discharge plan of care17 with all healthcare providers, the NPC‐QIC recommends IHM programs incorporate a predischarge team conference call to communicate and coordinate an effective care transition (Table 3). Call participants should include the caregivers, outpatient primary care providers, and local pediatric cardiologists, along with the inpatient healthcare team to allow for review of the plan of care and to establish open communication.30 Close communication between the IHM team and local cardiologists and primary care providers can foster timely evaluation and management of medical concerns.
Table 3.
| Communication Topics | Content |
|---|---|
| Review diagnosis, interventions or procedures, and postoperative course |
[ ] Provide copy of discharge summary [ ] Review diagnosis, surgical intervention and shunt site, residual defects or concerns, baseline vital signs, oxygen saturation and weight, and any extracardiac anomalies (eg, genetic syndrome, neurologic issues, heterotaxy, asplenia, and dysphasia) |
| IHM team and management plan |
[ ] Introduce IHM, team members, and 24‐h access [ ] Identify best contact numbers for pediatrician and IHM team to communicate during the interstage[ ] Discuss what will be monitored, goal parameters, review “red flag symptoms” and communication needs across all specialties during the interstage period[ ] Discuss the nutrition and medication plan, growth parameter goals, who will provide weekly growth and nutrition evaluation with feeding plan advancements[ ] Discuss any social concerns or barriers to access care |
| Appointments |
[ ] Primary cardiologist [ ] Primary care provider [ ] Interstage clinic [ ] Specialty medical clinics (eg, general surgery, genetics, neurology) [ ] Therapies (physical, speech, and occupational) [ ] Neurodevelopmental clinic follow‐up (referral to local early intervention programs) [ ] Cardiac catheterization date (if known) [ ] Monthly palvizumab (RSV season only) [ ] Any follow‐up outpatient diagnostic or laboratory tests |
| Emergency plan | [ ] Identify the closest, equipped emergency department with guidelines on oxygenation and hydration, and urgent contact with IHM team and primary cardiologists |
| Caregiver/family resources and support groups | [ ] Social worker, psychologist/mental health, discharge planner, or case manager contact number[ ] Local and national family support groups |
| Share documents | [ ] Center specific forms—Medical identification tools, wallet identification cards, red flag action plans, interstage visit appointment summary, or NPC‐QIC templates |
IHM indicates interstage home monitoring; NPC‐QIC, National Pediatric Cardiology Quality Improvement Collaborative; and RSV, respiratory syncytial virus.
Interstage Medical Home
A collaborative, specialized multidisciplinary team to provide coordinated interstage management has been successfully and widely adopted at multiple centers.4, 10, 21, 23, 31 The IHM team typically consists of pediatric cardiologists, nurses, advanced practice providers, dieticians, occupational and physical therapists, and/or speech‐language pathologists knowledgeable in inpatient and outpatient management of infants with shunt‐dependent SVHD. The concept for the interstage medical home is consistent with the US Department of Health and Human Services Healthy People 2010 and 2020 goals and objectives for all children with special medical needs to have access and receive ongoing, comprehensive care.32 Establishing a medical home can optimize the use of medical resources, expand the competence of involved providers, increase caregiver satisfaction, and improve interstage outcomes.10 An important aspect of this medical home is neurodevelopmental surveillance through specialized cardiac neurodevelopmental clinics and state‐provided early intervention services for high risk infants. Medical home surveillance is advocated by national organizations (eg, NPC‐QIC, American Heart Association, American Academy of Pediatrics, and Cardiac Neurodevelopment Outcome Collaborative) to reduce potential developmental delays associated with chronic congenital cardiac conditions.33, 34
Caregiver Support: Transition From Hospital to Home
Thoughtful preparation can make the transition from hospital to home less stressful. Caregivers have shown higher confidence and knowledge after discharge when actively participating in the care of their infant while in the hospital.26 Despite this increased competence, many caregivers still feel anxious with the transition from inpatient to home.35 Stress, anxiety, and depression may increase when barriers to education are present and resources are low. These may include language barriers, low literacy, cultural barriers, single or teenage caregivers, lack of family or financial support, limited access to transportation, or lack of insurance. Socioeconomic factors have been shown to be associated with early mortality after S1P.36 The IHM team can lessen these factors through anticipating home needs and validating with caregivers stable trends in the infant's monitored parameters before discharge. An early postdischarge follow‐up phone call by the IHM team and home nursing visits can provide additional valuable support to caregivers.
The high‐risk nature of the interstage period and rigorous daily care requirements not only affects the caregivers but the entire family system, including siblings.27, 37, 38 Whether a first‐time or experienced caregiver, interstage management is complex and beyond the typical care of an infant without congenital heart disease. Caregivers have expressed feelings of social isolation and relied on close family and friends for support during this period.19 Thus, caregiver support must continue after discharge with 24‐hour access to the IHM team and the ability to communicate with the IHM team in their primary language. Caregivers need support and training to become an active member of the medical team. A parent perspective on interstage home monitoring is provided in the supplemental materials available with this article. This includes the capability to assess for red flags, report breaches to the healthcare team, share any parental concern and access the emergency department or primary care setting to ensure care is provided without delay. The transition to home is a pivotal step in fulfilling the caregiver's goal of “becoming a family,” which has been reported as an important coping strategy during this time.19
Nutritional Management
Risk factors for growth failure during the interstage period include inadequate caloric intake, increased metabolic demands of heart failure, gastrointestinal dysfunction, or noncardiac comorbidities. Poor feeding and decreased weight gain can be signs of hemodynamic instability after S1P and have been associated with more complex postoperative course at S2P.11, 39 Regular assessment of caloric intake and weight gain is needed throughout the interstage period to allow early identification of feeding difficulties or inadequate growth. NPC‐QIC efforts identified processes common to centers with positive interstage weight gain and adoption of these strategies is vital during IHM28, 30 (Table 4). Targeted weight gain during the interstage period is 20 to 30 g per day and often requires enteral intake goals of 120 to 140 mL/kg per day and 120 to 150 kcal/kg per day.40 Infant formula or expressed breast milk often requires concentration to 22 to 30 calories/oz.40 Feeding routes used after S1P include oral, tube, or a combination of these, including breastfeeding, if the infant's clinical condition allows. Each infant's home nutrition plan should include type and route of enteral support needed to promote growth and neurodevelopment.
Table 4.
Nutrition Bundlea
| Standard post‐S1P feeding evaluation (eg, clinical, endoscopic, or swallow evaluation |
| Home scale for interstage weight monitoring |
| Specific weight gain/loss “red flags” to identify patients with growth failure in the interstage |
| Regular telephone contact with families during the interstage about nutrition and growth |
| Dietitian available for each cardiology outpatient visit during the interstage |
Modified from the National Pediatric Cardiology Quality Improvement Collaborative ( http://npcqic.org) Nutrition Bundle.28, 30
Additional Interstage Surveillance Strategies
Interstage surveillance strategies have evolved over the past decade.10, 29 Center variations occur based on staff, resources, and access or distance to a cardiac center. Despite center differences in surveillance, common strategies include weekly communication with families, interstage specialty clinics, and telehealth modalities.
Weekly communication between caregivers and the IHM team provides an opportunity to review physiologic and growth trends, update feeding plans, validate caregiver observations, provide anticipatory guidance, and addresses any concerns. Algorithms to facilitate direct and frequent communication between the caregiver and IHM care team, referring cardiologist, and pediatrician have been developed by some centers.25, 41, 42
Interstage specialty clinics have evolved to meet the multidisciplinary needs of infants after S1P, and care is often provided by cardiology nurse practitioners, cardiologists, dieticians, and social workers. Interstage clinic visits vary depending on distance from center and type of monitoring (eg, telehealth). Clinic visits afford the IHM team an opportunity to validate weight trends and oxygen saturations using clinic equipment, review data trends recorded by caregivers, confirm medication dosages, review red flags and how to reach IHM team, observe enteral feeding, perform a comprehensive physical assessment, obtain diagnostic imaging if warranted, and assess the emotional and social state of caregivers. Other services that may be provided include speech, occupational, and physical therapy to assess and address developmental needs.
Currently, telehealth platforms are being used at some centers for interstage surveillance through telephone or tablet‐based applications including some with real‐time image and video transfer capabilities. The proliferation of consumer‐grade mobile devices and secure, cloud‐based services has laid the foundation for automated real‐time analytics and notifications to the healthcare team.22, 43 Programs that integrate IHM with clearly defined, automatic thresholds for notification of the healthcare team have demonstrated improvements in survival, weight gain, and shorter interstage intensive care unit length of stay.22, 43 These technologies may help address socioeconomic disparities in interstage survival and potentially alleviate some parental stress.22, 35, 43 Systematic analysis of daily videos of the infant may provide important insights. Mobile technologies offer an ever‐evolving continuum of IHM and care in the outpatient setting. However, consideration of the caregiver's comfort level with digital technology, access to wireless connectivity, and potential preference for traditional IHM strategies should be acknowledged.
Progression to Stage 2 Palliation
Timing of elective S2P is variable but is typically performed between 3 and 6 months after S1P.44, 45 One of the effects of IHM has been a progression to earlier S2P to mitigate risk in those infants with multiple breaches of red flag criteria or those who fail to progress.46 Early S2P may be more feasible as interstage weight gain has improved in the era of IHM.9 Outcomes of S2P, even when done at an early age, are comparable to S2P done at standard age.47 A decision algorithm for progression to S2P based on clinical markers is shown in Figure 2.
Figure 2. Decision Algorithm for Progression to Stage 2 Palliation.
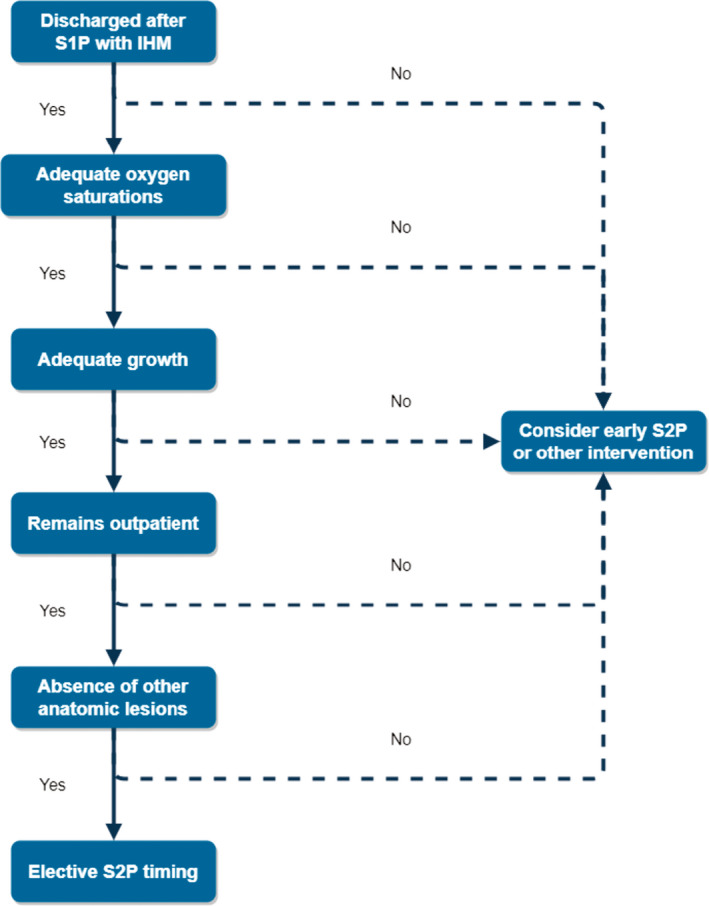
IHM indicates interstage home monitoring; S1P, stage 1 palliation; and S2P, stage 2 palliation.
Transition ON Completion of Interstage Home Monitoring
The completion of IHM marks a major care transition for caregivers and usually occurs after the completion of S2P or a cardiac procedure (surgical or catheter‐based) deemed to reduce an infant's risk of acute decompensation at home. Caregivers have expressed great relief around normalizing family routines and the ability to focus on the infant's developmental progress once discharged after S2P.19 However, others shared feelings of stress, anxiety and a heightened sense of vigilance about caring for their infant without the aid of home monitoring and frequent contact with the healthcare team.20 The healthcare team should be sensitive to caregiver needs and priorities when preparing for IHM completion. Assurance of ongoing support during the transition of cardiac care from the IHM team to potentially new cardiology providers or location is critical along with reinforcing the caregiver's ability to assess their infant without the use of monitoring equipment. The completion of IHM should be viewed in a positive light and caregivers should be praised for reaching the S2P milestone.
Expansion of IHM to Other High‐Risk Infants With Congenital Heart Disease
Hypoplastic left heart syndrome is considered to be among the highest risk of early mortality, even after successful S1P and early IHM programs focused primarily on infants who had undergone S1P.2 More recently, single center reports have identified non‐HLHS single ventricle defects to also be at high risk for interstage mortality (eg, heterotaxy anatomic substrates, pulmonary atresia with intact ventricular septum, or other defects with shunt‐dependent pulmonary blood flow, and balanced circulation) supporting the expansion of IHM to all types of SVHD both with and without a systemic‐to‐pulmonary shunt.14, 31, 48 The potential to include biventricular shunt‐dependent defects that require an initial palliative procedure could be another area of inclusion. Surgical practices such as primary transplant for high‐risk lesions or neonatal complete repair of previously palliated Congenital Heart Disease and center resources may limit this expansion of IHM to additional lesions.
Multicenter Interstage Quality Improvement Efforts
The NPC‐QIC was established in 2008 to improve outcomes of HLHS during the interstage period with an emphasis on reducing mortality and improving quality of life.49 Initial NPC‐QIC publications reported significant practice variation with regards to care during the interstage period.17, 41, 50 In a comparison of data from 2 eras, there were significant changes in infant‐specific risk factors, surgical strategy, discharge communication, and interstage care as measured by discharge processes, nutrition support, interstage monitoring, and surgical timing of S2P.51 The work of this multicenter quality improvement collaborative resulted in improved knowledge about best practices to manage interstage infants and led to the development of an Interstage Change Package, a resource containing multiple interstage improvement strategies.28 NPC‐QIC's Phase 1 efforts led to a decrease in interstage mortality by >40% (9.5%–5.5%) and a decrease in growth failure by 28% (18.6%–13.1%).30
Interstage Home Monitoring Outcomes
Improved Survival
Data from single centers with IHM programs report success in reducing interstage mortality to as low as 2%.1, 10, 14, 25, 42, 46, 52 The NPC‐QIC reported a decrease in interstage mortality by >40% between 2008 and 2016.30 Although multiple factors likely contributed to the decline, the widespread adoption of IHM strategies at >50 cardiac centers participating in the collaborative was thought to be the most impactful. Other variations in practice and programmatic changes such as earlier catheterization and S2P or hospitalization of high‐risk infants throughout the interstage period or following a readmission may have also contributed to differences in survival outcomes.30
Decreased Major Event Readmissions
Decreased readmissions for major events such as cardiac arrest, shunt thrombosis, arrhythmias, systemic infections, aspiration, stroke, or seizures was a desired outcome of IHM.42 In contrast, readmissions prompted by red flags or concerning symptoms were anticipated to increase as they were considered important in allowing for prompt assessment and prevention of major events. A recent study found infants with IHM were more likely to be admitted than historical controls.42 Although the IHM group had more readmissions, the duration was shorter compared with controls with the majority being observational and requiring minimal or no interventions. Analysis of the NPC‐QIC registry data revealed unanticipated interstage readmissions occurred in 66% of 815 infants at 50 centers.53 The median readmission length of stay was 2 days. Most readmissions were prompted by minor clinical changes (eg, red flags). Only 6% were major adverse event readmissions. Given the lack of previous data, it is difficult to determine whether IHM itself has increased or decreased the frequency and type of readmissions. However, it seems likely that early readmissions based on red flag events identified by IHM may prevent major adverse events.53 In support of this scenario, 1 study noted the percentage of IHM infants in their cohort requiring major interventions such as emergent surgery or an unscheduled interventional catheterization, was similar to their previously reported interstage mortality rates indicating these interventions may possibly represent “near‐miss deaths.”25
Improved Growth
Although it was widely believed the complex medical problems of infants with HLHS would not allow normal weight gain, an unexpected but welcomed outcome of IHM was improved weight gain during the interstage period.3 NPC‐QIC data demonstrated use of a nutrition bundle (Table 4) and home monitoring of weight was associated with a 28% reduction in interstage growth failure.30 Further analyses revealed that with appropriate caloric goals and IHM, adequate growth could be achieved regardless of feeding modality.18 Others have reported improved interstage weight gain31 and normal interstage growth velocity of 26 g/d during the period associated with IHM.9 Frequent weight monitoring provides more opportunities for clinicians to detect growth failure early and intervene to optimize the nutritional plan of care. Interstage growth failure has been linked to a more complex postoperative course and longer hospital length of stay at the time of S2P.39, 49, 54 Furthermore, early growth failure in complex congenital heart disease is associated with worse early developmental outcomes.55, 56
Gaps in Knowledge and Goals
The major research gap associated with IHM is the lack of a randomized controlled trial to assess the role it plays in improvement in interstage mortality and morbidity. IHM may be only one component, particularly because IHM use is concomitant with improved discharge processes, care coordination, and nutrition bundles, which are all linked to better outcomes.3 Additional understanding of key drivers of improvement can allow resources to be targeted more effectively. It is unlikely a randomized trial will be performed because of the wide acceptance of the benefits of IHM. Rather, further research exploring the use of novel statistical techniques can assist in predicting which infants with a single ventricle are most at risk for sudden death, inform future interstage care, and define who may benefit from remaining inpatient interstage.9, 18 Use of multilanguage, low literacy, affordable telehealth and social media options for monitoring and communicating with families requires further investigation. The ultimate goal would be to lift the burden of caregiver‐driven data collection and assessments of deterioration onto the care coordination team.23 In addition, there is limited research examining the psychological effects of IHM on caregivers.19 The interstage period is often perceived as a highly stressful and anxious time. Future qualitative studies to address the interstage experience may prove useful to address caregiver and family needs and identify ways to improve IHM programs.26 With caregiver education, nutritional management and care coordination being key elements in IHM, there remain many opportunities for ongoing quality improvement and research. The development of national quality improvement collaboratives such as NPC‐QIC, offer excellent forums for determining best practices and establishing benchmarks. Through collaboration and transparency across centers, there is a continued effort to reach 100% survival in the population of infants with SVHD.
Summary
Infants with shunt‐dependent SVHD pose unique challenges during the interstage period for caregivers and the healthcare team related to potential sudden acute hemodynamic decompensation, hypoxia, feeding difficulties, and somatic growth failure. IHM is an innovative strategy developed to augment conventional outpatient management and to assist with early detection of physiologic changes associated with morbidity and mortality following successful S1P. There is overwhelming evidence of improvement in single ventricle infant survival and growth outcomes with IHM programs. This surveillance strategy has become the standard of care for most pediatric cardiac programs and continues to evolve using telehealth platforms such as phone technology and tablet‐based real‐time video encounters in an effort to optimize data collection and visual assessment of the infant at home. The initial multisite examination of IHM effectiveness by NPC‐QIC has laid the groundwork for determining best practices and establishing benchmarks for care. Together with improved care coordination, discharge planning, and nutritional management bundles, IHM is a key component in optimizing outcomes in these high‐risk infants. Future collaborative research and quality improvement efforts should address the psychosocial needs of caregivers to improve the IHM experience and further investigate additional key drivers impacting mortality and morbidity in the SVHD population.
Disclosures
Writing Group Disclosures
| Writing Group Member | Employment | Research Grant | Other Research Support | Speakers’ Bureau/Honoraria | Expert Witness | Ownership Interest | Consultant/Advisory Board | Other |
|---|---|---|---|---|---|---|---|---|
| Nancy A. Rudd | Children's Hospital of Wisconsin | None | None | None | None | None | None | None |
| Nancy A. Pike | University of California, Los Angeles School of Nursing | NIH R01* | None | None | None | None | None | None |
| Nancy S. Ghanayem | Texas Children's Hospital; Baylor College of Medicine | None | None | None | None | None | None | None |
| Garick D. Hill | Cincinnati Children's Hospital Medical Center | None | None | None | None | None | None | None |
| Linda M. Lambert | University of Utah and Primary Children's Hospital | None | None | None | None | None | None | None |
| Kathleen A. Mussatto | Children's Hospital of Wisconsin Herma Heart Center | None | None | None | None | None | None | None |
| Jo Ann Nieves | Nicklaus Children's Hospital | None | None | None | None | None | None | None |
| Sarah Robinson | Self‐Employed | None | None | None | None | None | None | None |
| Girish Shirali | Children's Mercy Hospitals and Clinics The Ward Family Heart Center | None | None | None | None | None | None | None |
| Michelle M. Steltzer | Ann and Robert Lurie Children's Hospital of Chicago | None | None | None | None | None | None | None |
| Karen Uzark | University of Michigan, Women's Hospital | None | None | None | None | None | None | None |
This table represents the relationships of writing group members that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all members of the writing group are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives ≥$10 000 during any 12‐month period, or ≥5% of the person's gross income; or (2) the person owns ≥5% of the voting stock or share of the entity, or owns ≥$10 000 of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
Significant.
Reviewer Disclosures
| Reviewer | Employment | Research Grant | Other Research Support | Speakers’ Bureau/Honoraria | Expert Witness | Ownership Interest | Consultant/Advisory Board | Other |
|---|---|---|---|---|---|---|---|---|
| Lori A. Erickson | Children's Mercy Hospitals and Clinics | None | None | None | None | None | None | None |
| Patricia O'Brien | Children's Hospital, Boston | None | None | None | None | None | None | None |
| James S. Tweddell | Cincinnati Children's Hospital Medical Center | None | None | None | None | None | None | None |
| Gail Wright | Stanford University | None | None | None | None | None | None | None |
This table represents the relationships of reviewers that may be perceived as actual or reasonably perceived conflicts of interest as reported on the Disclosure Questionnaire, which all reviewers are required to complete and submit. A relationship is considered to be “significant” if (1) the person receives ≥$10 000 during any 12‐month period, or ≥5% of the person's gross income; or (2) the person owns ≥5% of the voting stock or share of the entity, or owns ≥$10 000 of the fair market value of the entity. A relationship is considered to be “modest” if it is less than “significant” under the preceding definition.
Supporting information
Supinfo
Acknowledgments
The authors would like to acknowledge Dr Nancy Ghanayem for the development of Figure 1 and Dr Garick Hill for the development of Figure 2. The authors would also like to acknowledge Ashley Ziedler, MLIS, of the Medical College of Wisconsin for her assistance with the literature review and reference management.
(J Am Heart Assoc. 2020;9:e014548 DOI: 10.1161/JAHA.119.014548.)
The American Heart Association makes every effort to avoid any actual or potential conflicts of interest that may arise as a result of an outside relationship or a personal, professional, or business interest of a member of the writing panel. Specifically, all members of the writing group are required to complete and submit a Disclosure Questionnaire showing all such relationships that might be perceived as real or potential conflicts of interest.
This statement was approved by the American Heart Association Science Advisory and Coordinating Committee on April 16, 2020, and the American Heart Association Executive Committee on May 5, 2020. A copy of the document is available at https://professional.heart.org/statements by using either “Search for Guidelines & Statements” or the “Browse by Topic” area.
Supplemental material is available with this article at https://www.ahajournals.org/doi/suppl/10.1161/JAHA.119.014548
The American Heart Association requests that this document be cited as follows: Rudd NA, Ghanayem NS, Hill GD, Lambert LM, Mussatto KA, Nieves JA, Robinson S, Shirali G, Steltzer MM, Uzark K, Pike NA; on behalf of the American Heart Association Council on Cardiovascular and Stroke Nursing; Council on Lifelong Congenital Heart Disease and Heart Health in the Young; Council on Arteriosclerosis, Thrombosis and Vascular Biology; Council on Clinical Cardiology; and Council on Lifestyle and Cardiometabolic Health. Interstage home monitoring for infants with single ventricle heart disease: education and management: a scientific statement from the American Heart Association. J Am Heart Assoc. 2020;9:e014548. doi: 10.1161/JAHA.119.014548
The expert peer review of AHA‐commissioned documents (eg, scientific statements, clinical practice guidelines, systematic reviews) is conducted by the AHA Office of Science Operations. For more on AHA statements and guidelines development, visit https://professional.heart.org/statements. Select the “Guidelines & Statements” drop‐down menu, then click “Publication Development.”
References
- 1. Furck AK, Uebing A, Hansen JH, Scheewe J, Jung O, Fischer G, Rickers C, Holland‐Letz T, Kramer HH. Outcome of the Norwood operation in patients with hypoplastic left heart syndrome: a 12‐year single‐center survey. J Thorac Cardiovasc Surg. 2010;139:359–365. [DOI] [PubMed] [Google Scholar]
- 2. Ghanayem NS, Hoffman GM, Mussatto KA, Cava JR, Frommelt PC, Rudd NA, Steltzer MM, Bevandic SM, Frisbee SS, Jaquiss RD, et al. Home surveillance program prevents interstage mortality after the Norwood procedure. J Thorac Cardiovasc Surg. 2003;126:1367–1377. [DOI] [PubMed] [Google Scholar]
- 3. Oster ME, Ehrlich A, King E, Petit CJ, Clabby M, Smith S, Glanville M, Anderson J, Darbie L, Beekman RH 3rd. Association of interstage home monitoring with mortality, readmissions, and weight gain: a multicenter study from the National Pediatric Cardiology Quality Improvement Collaborative. Circulation. 2015;132:502–508. [DOI] [PubMed] [Google Scholar]
- 4. Hehir DA, Ghanayem NS. Single‐ventricle infant home monitoring programs: outcomes and impact. Curr Opin Cardiol. 2013;28:97–102. [DOI] [PubMed] [Google Scholar]
- 5. Galantowicz M, Cheatham JP. Lessons learned from the development of a new hybrid strategy for the management of hypoplastic left heart syndrome. Pediatr Cardiol. 2005;26:190–199. [DOI] [PubMed] [Google Scholar]
- 6. Castellanos DA, Ocampo EC, Gooden A, Wang Y, Qureshi AM, Heinle JS, Mery CM, Hill GD, Ghanayem NS. Outcomes associated with unplanned interstage cardiac interventions following Norwood palliation. Ann Thorac Surg. 2019;108:1423–1429. [DOI] [PubMed] [Google Scholar]
- 7. Devlin PJ, McCrindle BW, Kirklin JK, Blackstone EH, DeCampli WM, Caldarone CA, Dodge‐Khatami A, Eghtesady P, Meza JM, Gruber PJ, et al. Intervention for arch obstruction after the Norwood procedure: prevalence, associated factors, and practice variability. J Thorac Cardiovasc Surg. 2019;157:684–695.e688. [DOI] [PubMed] [Google Scholar]
- 8. Ohye RG, Sleeper LA, Mahony L, Newburger JW, Pearson GD, Lu M, Goldberg CS, Tabbutt S, Frommelt PC, Ghanayem NS, et al; Pediatric Heart Network Investigators . Comparison of shunt type in the Norwood procedure for single‐ventricle lesions. N Engl J Med. 2010;362:1980–1992. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Hehir DA, Rudd N, Slicker J, Mussatto KA, Simpson P, Li SH, Frommelt MA, Tweddell JS, Ghanayem NS. Normal interstage growth after the Norwood operation associated with interstage home monitoring. Pediatr Cardiol. 2012;33:1315–1322. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10. Rudd NA, Frommelt MA, Tweddell JS, Hehir DA, Mussatto KA, Frontier KD, Slicker JA, Bartz PJ, Ghanayem NS. Improving interstage survival after Norwood operation: outcomes from 10 years of home monitoring. J Thorac Cardiovasc Surg. 2014;148:1540–1547. [DOI] [PubMed] [Google Scholar]
- 11. Hehir DA, Cooper DS, Walters EM, Ghanayem NS. Feeding, growth, nutrition, and optimal interstage surveillance for infants with hypoplastic left heart syndrome. Cardiol Young. 2011;21(suppl 2):59–64. [DOI] [PubMed] [Google Scholar]
- 12. Menon SC, McCandless RT, Mack GK, Lambert LM, McFadden M, Williams RV, Minich LL. Clinical outcomes and resource use for infants with hypoplastic left heart syndrome during bidirectional Glenn: summary from the Joint Council for Congenital Heart Disease National Pediatric Cardiology Quality Improvement Collaborative registry. Pediatr Cardiol. 2013;34:143–148. [DOI] [PubMed] [Google Scholar]
- 13. Feinstein JA, Benson DW, Dubin AM, Cohen MS, Maxey DM, Mahle WT, Pahl E, Villafane J, Bhatt AB, Peng LF, et al. Hypoplastic left heart syndrome: current considerations and expectations. J Am Coll Cardiol. 2012;59:S1–S42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Dobrolet NC, Nieves JA, Welch EM, Khan D, Rossi AF, Burke RP, Zahn EM. New approach to interstage care for palliated high‐risk patients with congenital heart disease. J Thorac Cardiovasc Surg. 2011;142:855–860. [DOI] [PubMed] [Google Scholar]
- 15. Nieves JA, Uzark K, Rudd NA, Strawn J, Schmelzer A, Dobrolet N. Interstage home monitoring after newborn first‐stage palliation for hypoplastic left heart syndrome: family education strategies. Crit Care Nurse. 2017;37:72–88. [DOI] [PubMed] [Google Scholar]
- 16. Buelow MW, Rudd N, Tanem J, Simpson P, Bartz P, Hill G. Reintervention following stage 1 palliation: a report from the NPC‐QIC registry. Congenit Heart Dis. 2018;13:919–926. [DOI] [PubMed] [Google Scholar]
- 17. Schidlow DN, Anderson JB, Klitzner TS, Beekman RH 3rd, Jenkins KJ, Kugler JD, Martin GR, Neish SR, Rosenthal GL, Lannon C. Variation in interstage outpatient care after the Norwood procedure: a report from the Joint Council on Congenital Heart Disease National Quality Improvement Collaborative. Congenit Heart Dis. 2011;6:98–107. [DOI] [PubMed] [Google Scholar]
- 18. Hill GD, Tanem J, Ghanayem N, Rudd N, Ollberding NJ, Lavoie J, Frommelt M. Selective use of inpatient interstage management after Norwood procedure. Ann Thorac Surg. 2020;109:139–147. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19. Stoffel G, Spirig R, Stiasny B, Bernet V, Dave H, Knirsch W. Psychosocial impact on families with an infant with a hypoplastic left heart syndrome during and after the interstage monitoring period—a prospective mixed‐method study. J Clin Nurs. 2017;26:3363–3370. [DOI] [PubMed] [Google Scholar]
- 20. Meakins L, Ray L, Hegadoren K, Rogers LG, Rempel GR. Parental vigilance in caring for their children with hypoplastic left heart syndrome. Pediatr Nurs. 2015;41:31–41, 50. [PubMed] [Google Scholar]
- 21. Ghanayem NS, Cava JR, Jaquiss RD, Tweddell JS. Home monitoring of infants after stage one palliation for hypoplastic left heart syndrome. Semin Thorac Cardiovasc Surg Pediatr Card Surg Annu. 2004;7:32–38. [DOI] [PubMed] [Google Scholar]
- 22. Bingler M, Erickson LA, Reid KJ, Lee B, O'Brien J, Apperson J, Goggin K, Shirali G. Interstage outcomes in infants with single ventricle heart disease comparing home monitoring technology to three‐ring binder documentation: a randomized crossover study. World J Pediatr Congenit Heart Surg. 2018;9:305–314. [DOI] [PubMed] [Google Scholar]
- 23. Shirali G, Erickson L, Apperson J, Goggin K, Williams D, Reid K, Bradley‐Ewing A, Tucker D, Bingler M, Spertus J, et al. Harnessing teams and technology to improve outcomes in infants with single ventricle. Circ Cardiovasc Qual Outcomes. 2016;9:303–311. [DOI] [PubMed] [Google Scholar]
- 24. Black AK, Sadanala UK, Mascio CE, Hornung CA, Keller BB. Challenges in implementing a pediatric cardiovascular home telehealth project. Telemed J E Health. 2014;20:858–867. [DOI] [PubMed] [Google Scholar]
- 25. Siehr SL, Norris JK, Bushnell JA, Ramamoorthy C, Reddy VM, Hanley FL, Wright GE. Home monitoring program reduces interstage mortality after the modified Norwood procedure. J Thorac Cardiovasc Surg. 2014;147:718–723.e711. [DOI] [PubMed] [Google Scholar]
- 26. March S. Parents’ perceptions during the transition to home for their child with a congenital heart defect: how can we support families of children with hypoplastic left heart syndrome? J Spec Pediatr Nurs. 2017;22:e12185. [DOI] [PubMed] [Google Scholar]
- 27. Gaskin KL, Barron DJ, Daniels A. Parents’ preparedness for their infants’ discharge following first‐stage cardiac surgery: development of a parental early warning tool. Cardiol Young. 2016;26:1414–1424. [DOI] [PubMed] [Google Scholar]
- 28. National Pediatric Cardiology Quality Improvement Collaborative . Interstage change package. 2016. Available at: https://npcqic.org/sites/default/files/images/About/QI/Change%20Package/NPC-QIC%20Interstage%20Change%20Package_20160219.pdf. Accessed October 1, 2019.
- 29. Stewart J, Dempster R, Allen R, Miller‐Tate H, Dickson G, Fichtner S, Principe AJ, Fonseca R, Nicholson L, Cua CL. Caregiver anxiety due to interstage feeding concerns. Congenit Heart Dis. 2015;10:E98–E106. [DOI] [PubMed] [Google Scholar]
- 30. Anderson JB, Brown DW, Lihn S, Mangeot C, Bates KE, Van Bergen AH, Rudd NA, Hanke S, Tweddell J, Lannon C. Power of a learning network in congenital heart disease. World J Pediatr Congenit Heart Surg. 2019;10:66–71. [DOI] [PubMed] [Google Scholar]
- 31. Petit CJ, Fraser CD, Mattamal R, Slesnick TC, Cephus CE, Ocampo EC. The impact of a dedicated single‐ventricle home‐monitoring program on interstage somatic growth, interstage attrition, and 1‐year survival. J Thorac Cardiovasc Surg. 2011;142:1358–1366. [DOI] [PubMed] [Google Scholar]
- 32. US Department of Health and Human Services, Health Resources and Services Administration . Measuring success for healthy people 2010: national agenda for children with special health care needs. 1999. Available at: https://www.healthypeople.gov/2020/topics-objectives/topic/maternal-infant-and-child-health. Accessed September 19, 2001.
- 33. Marino BS, Lipkin PH, Newburger JW, Peacock G, Gerdes M, Gaynor JW, Mussatto KA, Uzark K, Goldberg CS, Johnson WH Jr, et al; on behalf of the American Heart Association Congenital Heart Defects Committee of the Council on Cardiovascular Disease in the Young, Council on Cardiovascular Nursing, and Stroke Council . Neurodevelopmental outcomes in children with congenital heart disease: evaluation and management: a scientific statement from the American Heart Association. Circulation. 2012;126:1143–1172. [DOI] [PubMed] [Google Scholar]
- 34. Anderson JB, Beekman RH 3rd, Kugler JD, Rosenthal GL, Jenkins KJ, Klitzner TS, Martin GR, Neish SR, Brown DW, Mangeot C, et al. Improvement in interstage survival in a National Pediatric Cardiology Learning Network. Circ Cardiovasc Qual Outcomes. 2015;8:428–436. [DOI] [PubMed] [Google Scholar]
- 35. Caris EC, Dempster N, Wernovsky G, Butz C, Neely T, Allen R, Stewart J, Miller‐Tate H, Fonseca R, Texter K, et al. Anxiety scores in caregivers of children with hypoplastic left heart syndrome. Congenit Heart Dis. 2016;11:727–732. [DOI] [PubMed] [Google Scholar]
- 36. Bucholz EM, Sleeper LA, Newburger JW. Neighborhood socioeconomic status and outcomes following the Norwood procedure: an analysis of the Pediatric Heart Network Single Ventricle Reconstruction Trial public data set. J Am Heart Assoc. 2018;7:e007065 DOI: 10.1161/JAHA.117.007065. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 37. Bates KE, Yu S, Mangeot C, Shea JA, Brown DW, Uzark K. Identifying best practices in interstage care: using a positive deviance approach within the National Pediatric Cardiology Quality Improvement Collaborative. Cardiol Young. 2019;29:398–407. [DOI] [PubMed] [Google Scholar]
- 38. Dempster N, Cua CL, Wernovsky G, Caris E, Neely T, Allen R, Butz C. Children with hypoplastic left heart syndrome have lower quality of life than healthy controls and children with other illnesses. Cardiol Young. 2018;28:21–26. [DOI] [PubMed] [Google Scholar]
- 39. Anderson JB, Beekman RH 3rd, Border WL, Kalkwarf HJ, Khoury PR, Uzark K, Eghtesady P, Marino BS. Lower weight‐for-age z score adversely affects hospital length of stay after the bidirectional Glenn procedure in 100 infants with a single ventricle. J Thorac Cardiovasc Surg. 2009;138:397–404.e391. [DOI] [PubMed] [Google Scholar]
- 40. Slicker J, Hehir DA, Horsley M, Monczka J, Stern KW, Roman B, Ocampo EC, Flanagan L, Keenan E, Lambert LM, et al. Nutrition algorithms for infants with hypoplastic left heart syndrome; birth through the first interstage period. Congenit Heart Dis. 2013;8:89–102. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41. Brown DW, Connor JA, Pigula FA, Usmani K, Klitzner TS, Beekman RH 3rd, Kugler JD, Martin GR, Neish SR, Rosenthal GL, et al. Variation in preoperative and intraoperative care for first‐stage palliation of single‐ventricle heart disease: a report from the Joint Council on Congenital Heart Disease National Quality Improvement Collaborative. Congenit Heart Dis. 2011;6:108–115. [DOI] [PubMed] [Google Scholar]
- 42. Gardner MM, Mercer‐Rosa L, Faerber J, DiLorenzo MP, Bates KE, Stagg A, Natarajan SS, Szwast A, Fuller S, Mascio CE, et al. Association of a home monitoring program with interstage and stage 2 outcomes. J Am Heart Assoc. 2019;8:e010783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 43. Cross R, Steury R, Randall A, Fuska M, Sable C. Single‐ventricle palliation for high‐risk neonates: examining the feasibility of an automated home monitoring system after stage I palliation. Future Cardiol. 2012;8:227–235. [DOI] [PubMed] [Google Scholar]
- 44. Meza JM, Hickey EJ, Blackstone EH, Jaquiss RDB, Anderson BR, Williams WG, Cai S, Van Arsdell GS, Karamlou T, McCrindle BW. The optimal timing of stage 2 palliation for hypoplastic left heart syndrome: an analysis of the Pediatric Heart Network Single Ventricle Reconstruction Trial public data set. Circulation. 2017;136:1737–1748. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45. Hill GD, Rudd NA, Ghanayem NS, Hehir DA, Bartz PJ. Center variability in timing of stage 2 palliation and association with interstage mortality: a report from the National Pediatric Cardiology Quality Improvement Collaborative. Pediatr Cardiol. 2016;37:1516–1524. [DOI] [PubMed] [Google Scholar]
- 46. Hehir DA, Dominguez TE, Ballweg JA, Ravishankar C, Marino BS, Bird GL, Nicolson SC, Spray TL, Gaynor JW, Tabbutt S. Risk factors for interstage death after stage 1 reconstruction of hypoplastic left heart syndrome and variants. J Thorac Cardiovasc Surg. 2008;136:94–99.e3. [DOI] [PubMed] [Google Scholar]
- 47. Jaquiss RD, Ghanayem NS, Hoffman GM, Fedderly RT, Cava JR, Mussatto KA, Tweddell JS. Early cavopulmonary anastomosis in very young infants after the Norwood procedure: impact on oxygenation, resource utilization, and mortality. J Thorac Cardiovasc Surg. 2004;127:982–989. [DOI] [PubMed] [Google Scholar]
- 48. Ohman A, Stromvall‐Larsson E, Nilsson B, Mellander M. Pulse oximetry home monitoring in infants with single‐ventricle physiology and a surgical shunt as the only source of pulmonary blood flow. Cardiol Young. 2013;23:75–81. [DOI] [PubMed] [Google Scholar]
- 49. Kugler JD, Beekman RH 3rd, Rosenthal GL, Jenkins KJ, Klitzner TS, Martin GR, Neish SR, Lannon C. Development of a pediatric cardiology quality improvement collaborative: from inception to implementation. From the Joint Council on Congenital Heart Disease Quality Improvement Task Force. Congenit Heart Dis. 2009;4:318–328. [DOI] [PubMed] [Google Scholar]
- 50. Baker‐Smith CM, Neish SR, Klitzner TS, Beekman RH 3rd, Kugler JD, Martin GR, Lannon C, Jenkins KJ, Rosenthal GL. Variation in postoperative care following stage I palliation for single‐ventricle patients: a report from the Joint Council on Congenital Heart Disease National Quality Improvement Collaborative. Congenit Heart Dis. 2011;6:116–127. [DOI] [PubMed] [Google Scholar]
- 51. Carlo WF, Cnota JF, Dabal RJ, Anderson JB. Practice trends over time in the care of infants with hypoplastic left heart syndrome: a report from the National Pediatric Cardiology Quality Improvement Collaborative. Congenit Heart Dis. 2017;12:315–321. [DOI] [PubMed] [Google Scholar]
- 52. Hansen JH, Furck AK, Petko C, Buchholz‐Berdau R, Voges I, Scheewe J, Rickers C, Kramer HH. Use of surveillance criteria reduces interstage mortality after the Norwood operation for hypoplastic left heart syndrome. Eur J Cardiothorac Surg. 2012;41:1013–1018. [DOI] [PubMed] [Google Scholar]
- 53. Hanke SP, Joy B, Riddle E, Ravishankar C, Peterson LE, King E, Mangeot C, Brown DW, Schoettker P, Anderson JB, et al. Risk factors for unanticipated readmissions during the interstage: a report from the National Pediatric Cardiology Quality Improvement Collaborative. Semin Thorac Cardiovasc Surg. 2016;28:803–814. [DOI] [PubMed] [Google Scholar]
- 54. Kelleher DK, Laussen P, Teixeira‐Pinto A, Duggan C. Growth and correlates of nutritional status among infants with hypoplastic left heart syndrome (HLHS) after stage 1 Norwood procedure. Nutrition. 2006;22:237–244. [DOI] [PubMed] [Google Scholar]
- 55. Medoff‐Cooper B, Irving SY, Hanlon AL, Golfenshtein N, Radcliffe J, Stallings VA, Marino BS, Ravishankar C. The association among feeding mode, growth, and developmental outcomes in infants with complex congenital heart disease at 6 and 12 months of age. J Pediatr. 2016;169:154–159.e151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56. Mussatto KA, Hoffmann R, Hoffman G, Tweddell JS, Bear L, Cao Y, Tanem J, Brosig C. Risk factors for abnormal developmental trajectories in young children with congenital heart disease. Circulation. 2015;132:755–761. [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Supinfo