

Abstract
Purpose of Review
Lateral ankle ligament sprains are one of the most commonly reported injuries in high-level athletes and the general population. Unfortunately, up to 40% of these can go on to develop chronic lateral ankle instability which in the right circumstances requires surgical intervention. The purpose of this review is to present the gold standard surgical treatment for chronic lateral instability with anatomic ligament repair and to highlight the techniques, outcomes, and importance of anatomy when considering surgical treatment.
Recent Findings
Recent and remote literature agrees that the initial treatment for chronic ankle instability is non-operative rehabilitation. In the cases where this fails, the gold standard of surgical treatment is open anatomic repair using the Brostrom-Gould technique which stands out as having very good results over the course of time. Recent studies have shown equally good outcomes with arthroscopy as well as with internal brace devices, and both techniques show potential for earlier rehabilitation. In those with contraindications for anatomic repair including innate soft tissue laxity, high BMI, and in the revision setting, anatomic ligament reconstruction is an appropriate surgical option.
Summary
Open modified Brostrom lateral ligament repair continues to be the preferred method of surgical treatment for chronic lateral ligament instability. In the setting of new modifications and techniques, long-term outcome studies are necessary to identify both their usefulness in long term and to compare them to the open surgery outcomes. It would be useful to standardize rehabilitation protocols as well as return to sport metrics in order to better evaluate outcomes moving forward.
Keywords: Brostrom, Ankle instability, Lateral ligament repair, ATFL, Ankle sprain
Introduction
Ankle sprains remain one of the most commonly reported musculoskeletal injuries and occur across a wide variety of activities and sports [1, 2•]. Acute ankle sprains are generally the result of an inversion or eversion injury. Sprains of the lateral ligament complex are the most common [1]. Lateral ligament sprains are the most commonly reported injury in collegiate athletes in the USA [2•]. Initially, lateral ankle sprains can be successfully treated conservatively with rest, ice, non-steroidal anti-inflammatory drugs, and early mobilization [3•, 4]. Those with acute ankle instability benefit from a period of rest followed by functional rehabilitation to provide the strength and conditioning needed to return to sport or activities [3•, 5]. There is evidence that functional rehabilitation and bracing can prevent further instability events; however, 20–40% of patients diagnosed with acute ankle instability will go on to develop chronic ankle instability (CAI) [5–7].
CAI is diagnosed when patients present with recurrent ankle instability events, apprehension with activities oftentimes including ambulating over uneven surfaces, and ankle joint pain [6, 8, 9, 10•]. Bracing is unlikely to completely resolve their symptoms. Mechanical instability is generally caused by ligamentous rupture or laxity after an initial ankle sprain or as a culmination of multiple sprains. Targeted physical therapy with balance and strength training can address functional instability resulting from proprioceptive and strength deficits [11•]. If chronic instability is diagnosed and fails conservative therapies, it is more likely secondary to anatomic insufficiency. The most common surgical treatment for mechanical CAI that has failed functional rehabilitation is surgical anatomic repair or reconstruction of the lateral ligament complex [7]. Chronic painful instability of the ankle can lead to osteochondral lesions, synovitis, and post-traumatic arthritis if left untreated [12, 13].
In the setting of chronic lateral ankle instability, multiple surgical techniques have been described. The best outcomes historically have been seen with the ATFL primary repair technique described by Brostrom in 1966 and that technique’s subsequent modifications [14]. While there are many new techniques in the literature involving arthroscopic modifications, the excellent long-term outcomes for the open procedure ensure its current status as the gold standard of surgical care for chronic ankle instability. The purpose of this article is to review the current literature on the widely used open modified Brostrom technique for the surgical management of lateral ankle instability. We will also describe the technique in detail.
Anatomy and Injury Mechanism
Lateral ankle instability presents significant morbidity for those who fail non-operative interventions, and a clear understanding of the anatomy of these ligaments is paramount to the surgical management of these patients. There are three distinct ligaments which provide stability to the lateral ankle including the anterior talofibular, the calcaneofibular, and the posterior talofibular ligaments.
The anterior talofibular ligament (ATFL) functions to limit anterior translation of the talus as well as excessive plantarflexion and inversion of the talocrural joint. The ligament is most prone to injury when the ankle is in a plantarflexed position with an inversion moment and is the most frequently injured ligament during an ankle sprain. It originates on the anterior aspect of the lateral malleolus approximately 10 mm proximal to the fibular tip and continues anteromedially to its insertion point on the lateral talar body just anterior to the talofibular component of the ankle joint [15, 16]. The ATFL is most commonly composed of one or two separate bands with a close association to the joint capsule and is placed on the greatest tension in a plantarflexed and inverted position which is consistent with the mechanism of injury to this ligament [15, 17].
The calcaneofibular ligament (CFL) spans from the anterior distal fibula to the posterolateral calcaneus running in an anterior to posterior direction [16]. Upon initial surgical dissection, only approximately 1 cm of the ligament is visualized since it is located deep to the peroneal tendons [15]. The CFL is the only lateral ligament that spans both the talocrural and subtalar joints, and it functions in stabilizing both the talocrural and subtalar joints under multidirectional loads [18••]. It is the primary restraint during an inversion moment [19]. Injuries to this ligament most commonly occur with a concomitant ATFL tear and are extremely rare in isolation [20].
Finally, the posterior talofibular ligament (PTFL) runs in a horizontal pattern from the medial distal fibula to insert on the posterolateral talus. The PTFL is placed on tension during dorsiflexion and is rarely injured in an ankle sprain nor has it been found to contribute to ankle instability in isolation. Injuries to the PTFL generally only occur in high energy ankle injuries and are only identified in 5–10% of ankle sprains. Complete injuries to PTFL are more likely as a result of talar dislocation [21]. Due to these findings, the PTFL does not usually require surgical repair and is not part of the Brostrom technique for ankle instability [15].
Evaluation and Diagnosis
Patients presenting with CAI consistently report a sensation of ankle instability over a long period of time. Initial evaluation must include a detailed history including prior injuries, history of multiple instability events, and any previous surgeries. Multiple ankle sprains, elevated BMI, female gender, intrinsic foot or ankle deformity, and generalized ligamentous laxity are all factors that can predispose patients to CAI [10]. Those with poor dynamic control and slow recovery to previous function following an acute lateral ankle sprain are at higher risk for developing CAI [22].
Evaluation of patients with CAI should include a typical exam of the foot and ankle with examination of the contralateral extremity utilized as the “normal” control. Initially, inspection of alignment, deformity, swelling, or areas of point tenderness should be addressed. On physical exam, it is important to observe the alignment of the foot and ankle as hindfoot varus is a known risk factor for CAI and lateral ligament instability [23, 24]. In the cavovarus foot, the vector of pull of the Achilles tendon at heel strike causes increased stress in the lateral ligamentous structures, placing them at risk for failure during an inversion moment [24]. Ligament competency is evaluated using the anterior drawer test for the ATFL and talar tilt test for the CFL. The neurovascular status should be carefully evaluated as proprioceptive deficits and peroneal weakness can contribute significantly to the development of CAI. It should be noted that physical exam findings, especially when related to laxity, must be viewed as a whole. There is no single test for the diagnosis of CAI [25, 26•].
Imaging
As with most orthopedic evaluations, plain radiographs are important when evaluating CAI. Typically these are performed with the subject weight bearing. Identification of deformity or evidence of old avulsion fractures can provide valuable details for surgical planning. Stress radiographs can also be utilized in identifying pathologic instability which leads to alterations in the talar tilt or in anterior talar translation on the tibia. This test can be performed under x-ray or live fluoroscopic examination. The resulting images can confirm the diagnosis of ankle, and subtalar, instability, and aid in surgical decision-making. Pathologic instability is typically diagnosed with talar tilt greater than 6 degrees and anterior translation greater than 5 mm [27]. While stress radiographs are an inexpensive and straightforward test to perform, a positive test does not necessarily correlate with a difference in patient outcome scores after an open Brostrom procedure; however, they can be helpful in differentiating function and mechanical instability [28].
In situations where physical exam is ambiguous, MRI and ultrasound can be employed to diagnose ATFL and CFL tears in a non-invasive manner [29•] (Fig. 1). MRI is frequently utilized to identify co-existing intra-articular pathology prior to surgical intervention (Fig. 2) as the treatment of osteochondral lesions, for example, will alter the postoperative rehab protocol. While this can be helpful, arthroscopy remains the gold standard for identification of osteochondral lesions, loose bodies, tendinopathy, and additional ligamentous injuries when compared to MRI [30•].
Fig. 1.
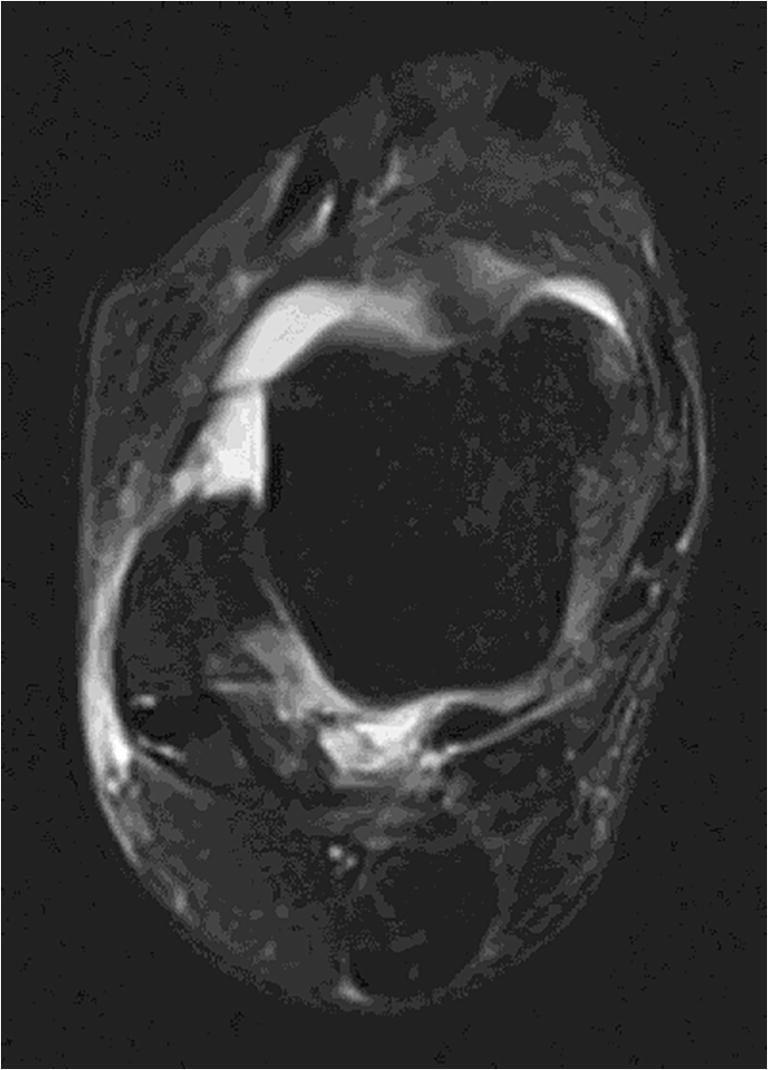
ATFL tear on MRI
Fig. 2.
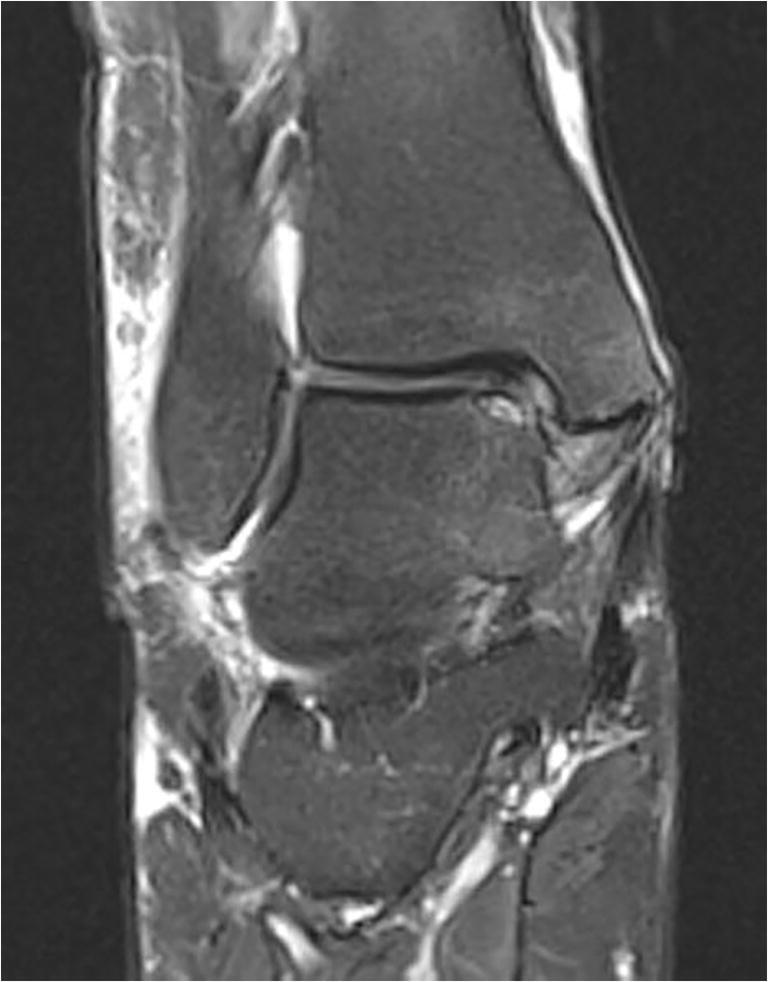
CFL tear with osteochondral lesion of the talar dome on MRI
Surgical Technique
The technique initially described by Brostrom included the anatomic repair and imbrication of the ATFL as well as the CFL when needed. Gould has since modified the technique with the use of the extensor retinaculum as an additional reinforcement repaired superficially to the primary repair of the CFL and ATFL [31]. While techniques can vary by surgeon, the general principles for open Brostrom-Gould anatomic repairs for lateral ankle ligament instability remain consistent.
The following is the technical description of the author’s preference when performing open lateral ligament repairs. The patient is positioned in a supine position with a bump under the ipsilateral hip, and general anesthesia can be used. A tourniquet is placed on the proximal thigh, and perioperative antibiotics are administered. If arthroscopy is indicated prior to open repair, an ankle distractor is applied (GUHL (Smith & Nephew) or other), and the superficial peroneal nerve is identified and marked. Standard anteromedial and anterolateral arthroscopic portals are established for examination of the joint. Following intra-articular examination and identification of any intra-articular pathology needing to be addressed, the open portion of the case begins. A curvilinear incision is made over the distal fibula and extending inferiorly towards the sinus tarsi. This incision allows access to both the ATFL and CFL for repair. If peroneal tendon pathology is present, the incision can be moved more posteriorly for better access to those tendons. Dissection is carried down through the skin and subcutaneous tissue exposing the anterolateral joint capsule as well as the inferior extensor retinaculum. Care is taken to avoid damaging any branches of the superficial peroneal nerve. The inferior extensor retinaculum is mobilized and protected inferiorly, while the peroneal tendon sheath is retracted posteriorly to access the CFL.
The ATFL footprint is incised at the distal fibula, and the ATFL ligament is isolated distally. The proximal periosteum is elevated (Fig. 3). A rongeur is used to decorticate the surrounding bone to promote healing. If CFL laxity is suspected from pre-operative examination and this is correlated in the operating room, the CFL can be directly repaired in a pants over vest fashion with suture or a suture anchor that can be drilled and placed in the CFL fibular footprint and the ligament stump advanced to the fibula. The ATFL footprint on the distal tibia is then exposed with subperiosteal dissection. The authors’ preference is to drill and place one or two suture anchors into the ATFL footprint on the distal fibula. (It is also possible to perform the repair with 2–3 pants-over-vest sutures). The ATFL is repaired to the footprint using two pants-over-vest sutures from inferior to superior. First, the sutures are passed through the ATFL ligament (Fig. 4). Next, they are passed underneath the periosteum exiting superficially (Fig. 5). The repair is over-sewn with 0 Vicryl suture to reinforce the ligament repair. The inferior retinaculum is then advanced over the ATFL repair and sutured to the remaining periosteal flap proximally (Fig. 6). During the repairs of both ligaments, it is important that the ankle is held in neutral with full eversion. The subcutaneous and skin layers are closed in the standard layered technique, and a sterile dressing is placed. A well-padded 3-way short leg plaster splint with appropriate neutral ankle position is applied.
Fig. 3.

Tibial anchor placed for ATFL repair
Fig. 4.
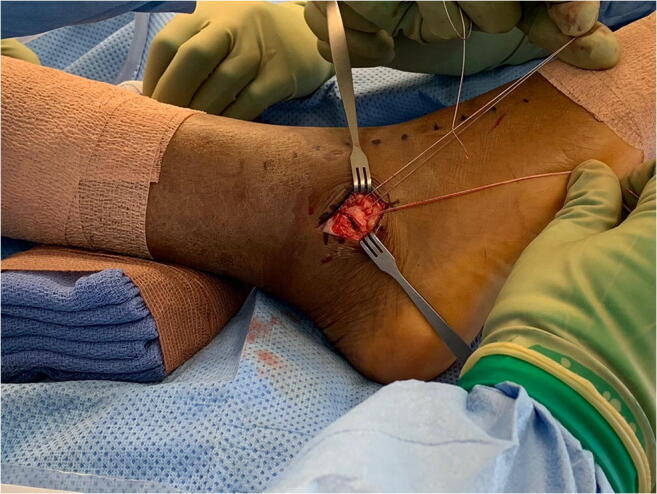
Repair of the ATFL to tibial anchor (author’s preferred technique for operative open lateral ligament repair)
Fig. 5.
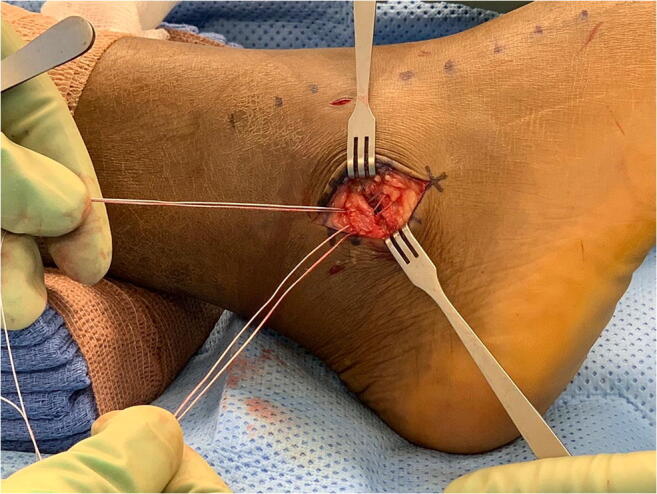
Repair of the ATFL to tibial anchor with ligament imbrication and periosteal reinforcement (author’s preferred technique for operative open lateral ligament repair)
Fig. 6.

Repaired ATFL (author’s preferred technique for operative open lateral ligament repair)
The classic Brostrom-Gould technique does not employ suture anchors but rather utilizes suture imbrication and repair of the ATFL and CFL in a pants-over-vest fashion with subsequent inferior retinacular reinforcement [31]. In cases where insufficient retinaculum is present for repair secondary to attrition of the tissues or anatomic variance, ligament repair can successfully be undertaken without reinforcement [32, 33].
Postoperative Rehabilitation
As in all other orthopedic procedures, adherence to a postoperative protocol is paramount to the success of a surgery for any patient. Following anatomic repair for chronic lateral ankle instability, the expert author’s preferred rehab protocol includes 2 weeks of non-weight bearing in a splint or brace with ankle in neutral dorsiflexion. For the following 4 weeks, weight bearing is allowed in a boot or brace. Range of motion (ROM) and strengthening are advanced between weeks 4–6 with absolutely no inversion, in order to protect the repair. ROM is continued with an emphasis on proprioceptive work for an additional 2 weeks, ensuring that inversion remains restricted throughout. Patients are placed in a lace up ankle brace for this phase of recovery. ROM with limited inversion, strengthening, and proprioceptive training are continued until 10 weeks at which time patients are allowed to return to full ROM and work towards return to sport-specific metrics after approximately 12–16 weeks.
Most modern rehabilitation programs call for similar early mobilization and range of motion depending on the strength of the ligamentous repair [34]. For lateral ligament repairs, it is generally accepted that the patient will be non-weight bearing for 7–10 days in a splint or boot for immobilization. From surgery to 6 weeks postoperatively, rehabilitation consists of slowly increasing range of motion with restrictions on plantarflexion and inversion in order to protect the ligament repair. In addition to range of motion, strengthening of dorsiflexion and eversion with emphasis on gait training is also encouraged. At 6 weeks postoperatively, range of motion is no longer restricted and proprioceptive, and balance are emphasized. A walking boot is employed until gait and balance are restored. Return to sport is not allowed until individuals can demonstrate 90% of pre-injury levels of strength, proprioception, and balance. Athletes must also meet sport-specific metrics that must be passed prior to return to sport [34, 35].
There is evidence that immediate postoperative weight bearing does not alter the outcomes of lateral ligament repair when range of motion was restricted [36]. In the protocol described by Petrera et al., initial ROM was restricted but weight bearing as tolerated was allowed in a boot. Range of motion was progressed during the third week postoperatively with full progression to active range of motion in all planes at 6 weeks. Strength, proprioception, and gait training were incorporated throughout the rehabilitation process. There was a 6% failure rate in this group which is comparable to the failure rate reported in other outcome studies for the modified Brostrom repair [36]. Return to play tends to be faster in the elite athlete population as they start off at a higher level of fitness and have access to physical therapy and other modalities that the general public may not be afforded. The average time to return to play is generally greater than 4 months post op, but this has been reported earlier in the athlete population [35, 37••]. Unfortunately there is a paucity of literature regarding standardized return to sport data [38••].
Surgical Techniques and Outcomes
The open Brostrom procedure for lateral ligament incompetency remains the gold standard for the surgical treatment of CAI. Outcome studies since the original introduction of the modification have shown excellent results [31, 39, 40••]. As techniques utilizing arthroscopy as well as anchors and suture reinforcement are frequently being utilized, there are multiple studies comparing and contrasting the outcomes of these new and modified techniques to the open Brostrom-Gould technique. Many surgeons are now utilizing anchors to reinforce the imbrication and repair described by Brostrom-Gould. Rigby et al. found no significant difference in outcome when comparing their modified Brostrom-Gould which included anchor reinforcement at the distal end of the fibula to an all inside arthroscopic repair of the ATFL. There was no significant difference in outcome noted despite differences in intra-articular pathology as well as postoperative rehab protocol in the two different groups. The arthroscopic repair group was allowed to weight bear earlier than the open group. There was a rate of 97% return to activities including sport for athletes across both groups [41].
When it comes to the open versus arthroscopic Brostrom-Gould techniques, both have excellent patient outcome scores regardless of which technique is used [40••, 42•]. Nevertheless, there is a slightly higher reported reoperation rate in the arthroscopic group [43•]. It is important to also consider concomitant pathology at the time of ligament repair as the literature reports a rate of greater than 50% [44]. A recent retrospective study looking at arthroscopic evaluation and treatment of intra-articular pathology at time of lateral ligament repair or reconstructive surgery did result in fewer ankle arthrodesis cases as well as less wound complications when compared to the lateral ligament procedure alone. It should be noted that arthroscopy did not decrease the overall reoperation rate [44].
Biomechanical studies comparing the arthroscopic versus open modified Brostrom also showed no difference in torque to failure on cadaver specimens [45]. Additionally, in cases where an internal brace was utilized for reinforcement of the ATFL repair, Schuh et al. found that the torque to failure as well as inversion angle at time of failure was actually greater for the group with the internal brace [46]. The most common mode of failure for primary repair of the ATFL as well as the repair of the ATFL to bone utilizing a suture anchor occurred at the ligament to suture interface. This is consistent with other biomechanical investigations [47]. When suture anchor repair techniques were reinforced with the internal brace, the failure at that interface decreased significantly which could potentially accelerate rehabilitation protocols [46]. While short-term outcomes look promising for internal brace reinforcement of repairs, long-term studies are needed [48•].
Regardless of the technique for ligament repair, consideration of the anatomy is essential. While the ATFL is the classically repaired ligament for lateral CAI, it is important to consider CFL repair when performing lateral ankle stabilization. A recent biomechanical study found significantly increased tibiotalar contact pressures and greater inversion of both the talus and the calcaneus with sectioning of the CFL indicative of the importance of a competent CFL for success of stabilization [18••]. Despite this finding, there are multiple studies showing excellent outcomes with isolated ATFL repairs, and as such CFL repair can be left to surgeon discretion [41, 42•]. Park et al. reported that the presence or absence of the ATFL remnant did not negatively impact the clinical outcome of patients undergoing a modified Broström procedure as described by Gould [49••]. In this study, the ATFL was evaluated on MRI, ultrasound, and arthroscopically with absence of or differences in ATFL morphology having no significant effect on the Foot and Ankle Outcome Scores (FAOS). Maffulli et al. reported a 9-year follow-up for 38 patients who underwent open modified Brostrom surgery addressing only the ATFL with 58% continuing at pre-injury sporting level. There was a 16% failure rate in this group at 9 years [50].
Functional chronic ankle instability is most often attributed to an imbalance of muscular control in addition to deficits in proprioception and oftentimes co-exists with mechanical instability [11•]. After ligament repair and restoration of mechanical stability to the ankle, it is important to address the functional instability factors with therapy as the patient recovers. Cho et al. found that at intermediate follow-up (2 years) following modified open Brostrom, peroneal strength was restored to 82.6% compared to the contralateral side. Despite the importance of peroneal strength in the conservative management of CAI, the outcomes of the open Brostrom were not significantly affected by peroneal muscle recovery, and all patients reported an FAOS score of greater than 90 at 2-year follow-up [40••]. 4.9% of the patients reported recurring instability.
Anatomic repair remains the most common treatment for chronic lateral ankle instability with the gold standard of the Brostrom-Gould technique. There are instances, however, where direct repair is contraindicated including those patients with significant generalized ligamentous laxity, prior unsuccessful anatomic repair, or secondary reconstructions and those with high body mass index. Beighton scores greater than or equal to 4 have been associated with higher failure rates after anatomic repair surgery [36, 51]. In these cases, as described in other chapters in this text, anatomic ligament reconstruction or augmented repair is an excellent option for stabilization and has been found to have similar outcomes to the Brostrom-Gould technique [52, 53••]. It is important to identify hindfoot or tibia vara during physical and imaging evaluation as the cavovarus foot can independently lead to failure of the ligament repair [23].
Conclusion
The open modified Brostrom lateral ligament repair remains the gold standard for surgical treatment of chronic lateral ankle instability. The outcomes for patients who undergo this procedure are excellent and have passed the test of time. As new techniques, including arthroscopic repairs, as well as reinforcement techniques are being utilized, long-term studies are needed to truly investigate how the outcomes compare to the open procedure. These newer methods may in fact lead to better results if reinforcement and minimally invasive techniques can lead to faster and more aggressive rehabilitation protocols.
Compliance with Ethical Standards
Conflict of Interest
Rebecca Griffith declares that she has no conflict of interest.
Kenneth Hunt declares that he has no conflict of interest.
Human and Animal Rights and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Management of Ankle Instability
Publisher’s note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Contributor Information
Kenneth J. Hunt, Email: kenneth.j.hunt@cuanschutz.edu
Rebecca Griffith, Email: Rebecca.griffith@cuanschutz.edu.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- 1.Doherty C, Delahunt E, Caulfield B, Hertel J, Ryan J, Bleakley C. The incidence and prevalence of ankle sprain injury: a systematic review and meta-analysis of prospective epidemiological studies. Sports Med. 2014;44:123–140. doi: 10.1007/s40279-013-0102-5. [DOI] [PubMed] [Google Scholar]
- 2.Roos KG, Kerr ZY, Mauntel TC, Djoko A, Dompier TP, Wikstrom EA. The epidemiology of lateral ligament complex ankle sprains in National Collegiate Athletic Association sports. Am J Sports Med. 2017;45:201–209. doi: 10.1177/0363546516660980. [DOI] [PubMed] [Google Scholar]
- 3.Doherty C, Bleakley C, Delahunt E, Holden S. Treatment and prevention of acute and recurrent ankle sprain: an overview of systematic reviews with meta-analysis. Br J Sports Med. 2017;51:113–125. doi: 10.1136/bjsports-2016-096178. [DOI] [PubMed] [Google Scholar]
- 4.Shawen SB, Dworak T, Anderson RB. Return to play following ankle sprain and lateral ligament reconstruction. Clin Sports Med. 2016;35:697–709. doi: 10.1016/j.csm.2016.05.012. [DOI] [PubMed] [Google Scholar]
- 5.Chen H, Li HY, Zhang J, Hua YH, Chen SY. Difference in postural control between patients with functional and mechanical ankle instability. Foot Ankle Int. 2014;35:1068–1074. doi: 10.1177/1071100714539657. [DOI] [PubMed] [Google Scholar]
- 6.Knupp M, Lang TH, Zwicky L, Lötscher P, Hintermann B. Chronic ankle instability (medial and lateral) Clin Sports Med. 2015;34:679–688. doi: 10.1016/j.csm.2015.06.004. [DOI] [PubMed] [Google Scholar]
- 7.McCriskin BJ. Management and prevention of acute and chronic lateral ankle instability in athletic patient populations. World J Orthop. 2015;6:161–171. doi: 10.5312/wjo.v6.i2.161. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Al-Mohrej O, Al-Kenani N. Chronic ankle instability: current perspectives. Avicenna J Med. 2016;6:103–108. doi: 10.4103/2231-0770.191446. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Kobayashi T, Gamada K. Lateral ankle sprain and chronic ankle instability: a critical review. Foot Ankle Spec. 2014;7:298–326. doi: 10.1177/1938640014539813. [DOI] [PubMed] [Google Scholar]
- 10.Vuurberg G, Hoorntje A, Wink LM, BFW VDD, Van Den Bekerom MP, Dekker R, et al. Diagnosis, treatment and prevention of ankle sprains: Update of an evidence-based clinical guideline. Br J Sports Med. 2018;52:956. doi: 10.1136/bjsports-2017-098106. [DOI] [PubMed] [Google Scholar]
- 11.Miklovic TM, Donovan L, Protzuk OA, Kang MS, Feger MA. Acute lateral ankle sprain to chronic ankle instability: a pathway of dysfunction. Phys Sportsmed. 2018;46:116–122. doi: 10.1080/00913847.2018.1409604. [DOI] [PubMed] [Google Scholar]
- 12.Odak S, Ahluwalia R, Shivarathre DG, Mahmood A, Blucher N, Hennessy M, et al. Arthroscopic evaluation of impingement and osteochondral lesions in chronic lateral ankle instability. Foot Ankle Int. 2015;36:1045–1049. doi: 10.1177/1071100715585525. [DOI] [PubMed] [Google Scholar]
- 13.Delco ML, Kennedy JG, Bonassar LJ, Fortier LA. Post-traumatic osteoarthritis of the ankle: a distinct clinical entity requiring new research approaches. J Orthop Res. 2017;35:440–453. doi: 10.1002/jor.23462. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Broström L. Sprained ankles. V. Treatment and prognosis in recent ligament ruptures. Acta Chir Scand. 1966;132:537–550. [PubMed] [Google Scholar]
- 15.Golanó P, Vega J, de Leeuw PAJ, Malagelada F, Manzanares MC, Götzens V, et al. Anatomy of the ankle ligaments: a pictorial essay. Knee Surg Sports Traumatol Arthrosc. 2016;18:557–569. doi: 10.1007/s00167-010-1100-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Clanton TO, Campbell KJ, Wilson KJ, Michalski MP, Goldsmith MT, Wijdicks CA, et al. Qualitative and quantitative anatomic investigation of the lateral ankle ligaments for surgical reconstruction procedures. J Bone Jt Surg Am. 2014;96:e98. doi: 10.2106/JBJS.M.00798. [DOI] [PubMed] [Google Scholar]
- 17.Khawaji B, Soames R. The anterior talofibular ligament: a detailed morphological study. Foot. 2015;25:141–147. doi: 10.1016/j.foot.2015.05.004. [DOI] [PubMed] [Google Scholar]
- 18.Hunt KJ, Pereira H, Kelley J, Anderson N, Fuld R, Baldini T, et al. The role of calcaneofibular ligament injury in ankle instability: implications for surgical management. Am J Sports Med. 2019;47:431–437. doi: 10.1177/0363546518815160. [DOI] [PubMed] [Google Scholar]
- 19.Kobayashi T, Yamakawa S, Watanabe K, Kimura K, Suzuki D, Otsubo H, et al. The in situ force in the calcaneofibular ligament and the contribution of this ligament to ankle joint stability. Clin Biomech. 2016;40:8–13. doi: 10.1016/j.clinbiomech.2016.10.009. [DOI] [PubMed] [Google Scholar]
- 20.Rigby R, Cottom JM, Rozin R. Isolated calcaneofibular ligament injury: a report of two cases. J Foot Ankle Surg. 2015;54:487–489. doi: 10.1053/j.jfas.2014.08.017. [DOI] [PubMed] [Google Scholar]
- 21.Khor YP, Tan KJ. The anatomic pattern of injuries in acute inversion ankle sprains: a magnetic resonance imaging study. Orthop J Sport Med. 2013;1:232596711351707. doi: 10.1177/2325967113517078. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Doherty C, Bleakley C, Hertel J, Caulfield B, Ryan J, Delahunt E. Recovery from a first-time lateral ankle sprain and the predictors of chronic ankle instability: a prospective cohort analysis. Am J Sports Med. 2016;44:995–1003. doi: 10.1177/0363546516628870. [DOI] [PubMed] [Google Scholar]
- 23.Krause F, Seidel A. Malalignment and lateral ankle instability: causes of failure from the varus tibia to the cavovarus foot. Foot Ankle Clin. 2018;23:593–603. doi: 10.1016/j.fcl.2018.07.005. [DOI] [PubMed] [Google Scholar]
- 24.Klammer G, Benninger E, Espinosa N. The varus ankle and instability. Foot Ankle Clin. 2012;17:57–82. doi: 10.1016/j.fcl.2011.11.003. [DOI] [PubMed] [Google Scholar]
- 25.Rosen AB, Ko J, Brown CN. Diagnostic accuracy of instrumented and manual talar tilt tests in chronic ankle instability populations. Scand J Med Sci Sports. 2015;25:e214–e221. doi: 10.1111/sms.12288. [DOI] [PubMed] [Google Scholar]
- 26.Doherty C, Bleakley C, Hertel J, Caulfield B, Ryan J, Delahunt E. Clinical tests have limited predictive value for chronic ankle instability when conducted in the acute phase of a first-time lateral ankle sprain injury. Arch Phys Med Rehabil. 2018;99:720–725. doi: 10.1016/j.apmr.2017.11.008. [DOI] [PubMed] [Google Scholar]
- 27.Dowling LB, Giakoumis M, Ryan JD. Narrowing the normal range for lateral ankle ligament stability with stress radiography. J Foot Ankle Surg. 2014;53:269–273. doi: 10.1053/j.jfas.2013.12.014. [DOI] [PubMed] [Google Scholar]
- 28.Jeong BO, Kim TY, Song WJ. Effect of preoperative stress radiographic findings on radiographic and clinical outcomes of the modified Broström procedure for chronic ankle instability. J Foot Ankle Surg. 2016;55:125–128. doi: 10.1053/j.jfas.2015.08.010. [DOI] [PubMed] [Google Scholar]
- 29.Cao S, Wang C, Ma X, Wang X, Huang J, Zhang C. Imaging diagnosis for chronic lateral ankle ligament injury: a systemic review with meta-analysis. J Orthop Surg Res. 2018;13:122. doi: 10.1186/s13018-018-0811-4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Staats K, Sabeti-Aschraf M, Apprich S, Platzgummer H, Puchner SE, Holinka J, et al. Preoperative MRI is helpful but not sufficient to detect associated lesions in patients with chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2018;26:2103–2109. doi: 10.1007/s00167-017-4567-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 31.Gould N, Seligson D, Gassman J. Early and late repair of lateral ligament of the ankle. Foot Ankle. 1980;1:84–89. doi: 10.1177/107110078000100206. [DOI] [PubMed] [Google Scholar]
- 32.Jeong BO, Kim MS, Song WJ, Soohoo NF. Feasibility and outcome of inferior extensor retinaculum reinforcement in modified broström procedures. Foot Ankle Int. 2014;35:1137–1142. doi: 10.1177/1071100714543645. [DOI] [PubMed] [Google Scholar]
- 33.Behrens SB, Drakos M, Lee BJ, Paller D, Hoffman E, Koruprolu S, et al. Biomechanical analysis of Brostrom versus Brostrom-Gould lateral ankle instability repairs. Foot Ankle Int. 2013;34:587–592. doi: 10.1177/1071100713477622. [DOI] [PubMed] [Google Scholar]
- 34.Pearce CJ, Tourné Y, Zellers J, Terrier R, Toschi P, Silbernagel KG. Rehabilitation after anatomical ankle ligament repair or reconstruction. Knee Surg Sports Traumatol Arthrosc. 2016;24:1130–1139. doi: 10.1007/s00167-016-4051-z. [DOI] [PubMed] [Google Scholar]
- 35.White WJ, McCollum GA, Calder JDF. Return to sport following acute lateral ligament repair of the ankle in professional athletes. Knee Surg Sports Traumatol Arthrosc. 2016;24:1124–1129. doi: 10.1007/s00167-015-3815-1. [DOI] [PubMed] [Google Scholar]
- 36.Petrera M, Dwyer T, Theodoropoulos JS, Ogilvie-Harris DJ. Short- to medium-term outcomes after a modified Broström repair for lateral ankle instability with immediate postoperative weightbearing. Am J Sports Med. 2014;42:1542–1548. doi: 10.1177/0363546514530668. [DOI] [PubMed] [Google Scholar]
- 37.Lee K, Jegal H, Chung H, Park Y. Return to play after modified broström operation for chronic ankle instability in elite athletes. CiOS Clin Orthop Surg. 2019;11:126–130. doi: 10.4055/cios.2019.11.1.126. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 38.Hunt KJ, Fuld RS, Sutphin BS, Pereira H, D’Hooghe P. Return to sport following lateral ankle ligament repair is under-reported: a systematic review. J ISAKOS Jt Disord Orthop Sport Med. 2017;2:5. [Google Scholar]
- 39.Hamilton WG, Thompson FM, Snow SW. The modified Brostrom procedure for lateral ankle instability. Foot Ankle. 1993;14:1–7. doi: 10.1177/107110079301400101. [DOI] [PubMed] [Google Scholar]
- 40.Cho BK, Park JK, Choi SM, SooHoo NF. The effect of peroneal muscle strength on functional outcomes after the modified Broström procedure for chronic ankle instability. Foot Ankle Int. 2018;39:105–112. doi: 10.1177/1071100717735838. [DOI] [PubMed] [Google Scholar]
- 41.Rigby RB, Cottom JM. A comparison of the “all-inside” arthroscopic Broström procedure with the traditional open modified Broström-Gould technique: a review of 62 patients. Foot Ankle Surg. 2019;25:31–36. doi: 10.1016/j.fas.2017.07.642. [DOI] [PubMed] [Google Scholar]
- 42.Li H, Hua Y, Li H, Ma K, Li S, Chen S. Activity level and function 2 years after anterior talofibular ligament repair: a comparison between arthroscopic repair and open repair procedures. Am J Sports Med. 2017;45:2044–2051. doi: 10.1177/0363546517698675. [DOI] [PubMed] [Google Scholar]
- 43.Guelfi M, Zamperetti M, Pantalone A, Usuelli FG, Salini V, Oliva XM. Open and arthroscopic lateral ligament repair for treatment of chronic ankle instability: a systematic review. Foot Ankle Surg. 2018;24:11–18. doi: 10.1016/j.fas.2016.05.315. [DOI] [PubMed] [Google Scholar]
- 44.Yasui Y, Murawski CD, Wollstein A, Kennedy JG. Reoperation rates following ankle ligament procedures performed with and without concomitant arthroscopic procedures. Knee Surg Sports Traumatol Arthrosc. 2017;25:1908–1915. doi: 10.1007/s00167-016-4207-x. [DOI] [PubMed] [Google Scholar]
- 45.Lee KT, Kim ES, Kim YH, Ryu JS, Rhyu IJ, Lee YK. All-inside arthroscopic modified Broström operation for chronic ankle instability: a biomechanical study. Knee Surg Sports Traumatol Arthrosc. 2016;24:1096–1100. doi: 10.1007/s00167-014-3159-2. [DOI] [PubMed] [Google Scholar]
- 46.Schuh R, Benca E, Willegger M, Hirtler L, Zandieh S, Holinka J, et al. Comparison of Broström technique, suture anchor repair, and tape augmentation for reconstruction of the anterior talofibular ligament. Knee Surg Sports Traumatol Arthrosc. 2016;24:1101–1107. doi: 10.1007/s00167-015-3631-7. [DOI] [PubMed] [Google Scholar]
- 47.Brown CA, Hurwit D, Behn A, Hunt KJ. Biomechanical comparison of an all-soft suture anchor with a modified Broström-Gould suture repair for lateral ligament reconstruction. Am J Sports Med. 2014;42:417–422. doi: 10.1177/0363546513517873. [DOI] [PubMed] [Google Scholar]
- 48•.Coetzee JC, Ellington JK, Ronan JA, Stone RM. Functional results of open Broström ankle ligament repair augmented with a suture tape. Foot Ankle Int. 2018;39:304–310. doi: 10.1177/1071100717742363. [DOI] [PubMed] [Google Scholar]
- 49.Park S, Kim T, Lee M, Park Y. Absence of ATFL remnant does not affect the clinical outcomes of the modified Broström operation for chronic ankle instability. Knee Surg Sports Traumatol Arthrosc. 2019;28:213–220. doi: 10.1007/s00167-019-05464-9. [DOI] [PubMed] [Google Scholar]
- 50.Maffulli N, Del Buono A, Maffulli GD, Oliva F, Testa V, Capasso G, et al. Isolated anterior talofibular ligament Broström repair for chronic lateral ankle instability: 9-year follow-up. Am J Sports Med. 2013;41:858–864. doi: 10.1177/0363546512474967. [DOI] [PubMed] [Google Scholar]
- 51.Park KH, Lee JW, Suh JW, Shin MH, Choi WJ. Generalized ligamentous laxity is an independent predictor of poor outcomes after the modified Broström procedure for chronic lateral ankle instability. Am J Sports Med. 2016;44:2975–2983. doi: 10.1177/0363546516656183. [DOI] [PubMed] [Google Scholar]
- 52.Matheny LM, Johnson NS, Liechti DJ, Clanton TO. Activity level and function after lateral ankle ligament repair versus reconstruction. Am J Sports Med. 2015;44:1301–1308. doi: 10.1177/0363546515627817. [DOI] [PubMed] [Google Scholar]
- 53.Vuurberg G, Pereira H, Blankevoort L, van Dijk CN. Anatomic stabilization techniques provide superior results in terms of functional outcome in patients suffering from chronic ankle instability compared to non-anatomic techniques. Knee Surg Sports Traumatol Arthrosc. 2018;26:2183–2195. doi: 10.1007/s00167-017-4730-4. [DOI] [PMC free article] [PubMed] [Google Scholar]