

Abstract
Purpose of Review
Irreparable subscapularis tears represent a challenging entity, especially when they occur in younger patients with high functional demands. Tendon transfers are one of the options considered for surgical management for this pathology. The purpose of this article is to review the surgical technique and outcome of the two most common tendon transfers considered for irreparable subscapularis tears: pectoralis major and latissimus dorsi.
Recent Findings
Transfer of the pectoralis major has been considered for decades the transfer of choice for irreparable subscapularis tears. Recently, a series with long-term follow-up (over 18 years) supported the reduction in pain and improvement in functional scores and patient satisfaction after pectoralis major transfer. However, the range of motion and the force in internal rotation were not maintained over time. Transfer of the latissimus dorsi to the lesser tuberosity has been recently described as an alternative with a sound biomechanical rationale and encouraging short-term results.
Summary
Transfer of the pectoralis major and the transfer of latissimus dorsi to the lesser tuberosity are the two transfers most commonly considered for patients with irreparable subscapularis tears. Transfer of the pectoralis major has a much longer track record. Both procedures seem to improve outcomes. Comparative studies are needed to determine the relative indications of these two procedures.
Keywords: Anterosuperior rotator cuff tear, Irreparable rotator cuff tear, Latissimus dorsi transfer, Massive rotator cuff tear, Pectoralis major transfer, Shoulder tendon transfer, Subscapularis tendon tear
Introduction
Rotator cuff pathology remains one of the most common shoulder conditions treated surgically [1]. The rotator cuff muscles include the supraspinatus, the infraspinatus, the teres minor, and the subscapularis muscle. In association with the periscapular muscles, the rotator cuff plays a critical role in the balance of shoulder biomechanics. A primary function of the rotator cuff is to dynamically maintain the center of rotation of the glenohumeral joint and avoid superior subluxation of the humeral head by resisting the upward vector of the deltoid muscle [2, 3]. As a consequence, tears of the rotator cuff may result in disruption of this balance and lead to abnormal shoulder function secondary to proximal humeral head migration, oftentimes pain and loss of motion, and ultimately cuff tear arthropathy [4].
Depending on the extent of involvement of the rotator cuff, various joint-preserving operative procedures can be considered for repair or reconstruction of an irreparable rotator cuff tear, as long as the articular cartilage glenohumeral joint is preserved. These include partial repair [5], biological augmentation [6], implantation of a subacromial balloon [7], superior capsular reconstruction [8], and tendon transfers [9, 10]. Reverse shoulder arthroplasty is another option to restore shoulder function in an irreparable cuff tear, and a discussion regarding arthroplasty must always be considered, as the postoperative management is often easier and shorter than for cuff repair or tendon transfer. However, in young and active patients, reverse shoulder arthroplasty may have an unacceptably high revision rate. Recent advancements in anatomical and biomechanics knowledge of periscapular muscles have allowed the development of techniques for muscle transfer for posterosuperior but also anterosuperior RCT insufficiency [11]. Although few studies were initially devoted to developing tendon transfers for anterosuperior cuff deficiency, there is recent interest in the development of novel transfers specifically for subscapularis insufficiency [12].
The subscapularis is considered by some the most important musculotendinous unit of the rotator cuff [13, 14]. An irreparable subscapularis tendon results in anteroposterior imbalance of the force couple in the transverse plane, with pain and loss of strength internal rotation [15]. If concomitant supraspinatus tendon insufficiency occurs, this results in anterosuperior migration of the humeral head secondary to the vertical imbalance of the glenohumeral joint. As a consequence, clinical symptoms of anterosuperior rotator cuff tear range from anterior shoulder pain with dysfunction, weakness, and eventually anterior instability [16, 17] to a complete loss of function leading to a so-called pseudoparalytic shoulder. Irreparable anterosuperior tear tears are less common than posterosuperior cuff tears, ranging from approximately 5 to 20% of all rotator cuff tear patterns [13, 18]. Compared with the number of different tendon transfers described for irreparable posterosuperior rotator cuff tear, only a few tendon transfers have been described to treat anterosuperior rotator cuff insufficiency. These have included the pectoralis major, pectoralis minor, and more recently latissimus dorsi [16, 19, 20••].
Pectoralis Major Transfer for Subscapularis Insufficiency
The pectoralis major (PM) consists of two heads: the clavicular head originates on the medial aspect of the clavicle and the sternal head originates from the upper portion of the sternum and the second through four ribs. The PM adducts, flexes, and internally rotates the humerus. Among musculotendinous transfers for irreparable anterosuperior rotator cuff tear, PM has been the most commonly described in various forms, including passage of the sternal or clavicular head, superficial, or deep to the conjoint tendon. Similarly, a biomechanical analysis identified a superior effect of the PM transferred underneath instead of above the conjoint tendon [21]. Furthermore, routing the pectoralis tendon deep to the conjoint tendon may have a theoretical advantage of providing an anterior buttress between the coracoid process and the humeral head [22].From a biomechanical standpoint, it has been reported that the sternal head is better for restoring internal rotation but, regardless of the repair technique, the pectoralis major does not exactly replicate the vector of the subscapularis. The subscapularis is located posterior to chest wall, while the PM is anterior to the chest wall.
Gerber et al. originally described the transfer of the pectoralis major tendon from the humeral shaft to the lesser tuberosity to repair the lower portion of the subscapularis [23]. This tendon transfer was initially described anterior to the conjoint tendon (Fig. 1). Gerber and colleagues recently reported their results with the longest follow-up outcome of pectoralis major tendon transfer for irreparable rotator cuff tears [24]. In a series of 22 patients, many achieved satisfactory long-term outcomes of PM transfer for irreparable subscapularis deficiency. At a mean follow-up of 19.7 years (minimum 18 years), they reported significantly improved functional scores (Constant score and SSV) with all shoulders rated good or excellent. Despite this satisfactory functional outcome, objective measurements were less encouraging. Both active internal and external rotation decreased significantly from the short-term (32 months) follow-up to the time of the latest follow-up (p = 0.005 and p = 0.002, respectively).
Fig. 1.

Illustrations depict transfer of the sternal head of the pectoralis major muscle deep to the clavicular head (A) or deep to the conjoint tendon (B) to reconstruct a subscapularis tear (Reproduced with permission from the Mayo Foundation for Medical Education and Research, Rochester, MN)
Based on biomechanical considerations [21], Resch et al [16] modified the original technique and reported transfer of the superior one-half to two-third of the PM tendon between the musculocutaneous nerve and the conjoint tendon (Fig. 2). In a series of 12 patients with short-term follow-up (mean, 28 months), these authors reported reduced pain and improvement of both subjective and objective scores. All four preoperatively unstable shoulders were considered stable at the latest follow-up. They did not encounter any musculocutaneous nerve dysfunction. However, the shoulders included in this study included isolated rupture of the subscapularis in 8 patients and only partial or complete concomitant rupture of the supraspinatus in 4 patients.
Fig. 2.

Illustrations depict transfer of the pectoralis minor muscle superficially (A) and deep (B) to the conjoint tendon to reconstruct a subscapularis tear. (Reproduced with permission from the Mayo Foundation for Medical Education and Research, Rochester, MN)
Using the same technique [16], Moroder et al. recently reported satisfactory midterm outcomes in a cohort of 27 patients with irreparable anterosuperior rotator cuff tears [25]. This series included anterosuperior rotator cuff tear in 45%, while a combination of posterosuperior and anterosuperior rotator cuff tears was noted in 32% of patients. Pain relief was maintained at an average of 10 years (range, 9 to 11 years) follow-up, but the initial postoperative increase in strength returned to the preoperative level, and improvements in range of motion diminished over time, especially with regard to internal rotation. Despite this worsening in certain outcomes, 77% of patients remained very satisfied at 10 years follow-up, and at final follow-up, only one patient had undergone revision surgery to a reverse shoulder arthroplasty.
Gavriilidis et al. reported a series of 15 patients either with only anterosuperior rotator cuff tear that means involving both the subscapularis and the supraspinatus [26]. They excluded patients with infraspinatus tear. They performed a tendon transfer of the clavicular part of the pectoralis major passed behind the conjoint tendon and fixed to the lesser tuberosity and to the anterior part of the greater tuberosity. The transferred tendon was either sutured to the remnants of subscapularis and the anterior part of the supraspinatus or fixed with anchors or transosseous sutures. No significant increase in range of motion was reported in these 15 patients at a mean follow-up of 37 months [26]. According to postoperative MRI findings, nine patients (70%) had an intact transferred PM tendon. Two patients had a complete tear and two patients had an intact but very thin tendon. One patient developed advanced cuff tear arthropathy (Hamada grade 4) [4]. Despite improvements in pain and Constant score, they suggested that a subscapularis tear combined with a supraspinatus tear was not a good indication for pectoralis major transfer.
Elhassan and Warner reported outcomes of PM transfer by passing the sternal head of the pectoralis major beneath its clavicular head to create a fulcrum for the sternal head in an attempt to be more in line with the vector of subscapularis [27•]. Similar to the technique described by Resch et al., their technique requires to pass the muscle beneath the conjoint tendon, thus placing the musculocutaneous nerve at risk. The PM tendon transfer was performed in 11 patients with an isolated subscapularis tendon tear (group I) and 11 patients with a more extensive irreparable rotator cuff tear (group III). Despite improvements in pain and functional outcomes, they reported failure of the tendon transfer in 3 cases in group I at a mean follow-up of 49 months (range, 25 to 68) and 4 cases in group III at a mean follow-up of 57 months (range, 44 to 82).
Interestingly, despite the proximity of the musculocutaneous nerve, the overall reported incidence of postoperative nerve palsy is low. A recent literature review reported only one transient musculocutaneous nerve palsy and one axillary nerve dysfunction out of 195 cases [28].
Based on this review of the literature, it would seem that transfer of the PM provides the best results for patients with isolated irreparable subscapularis tears in the absence of anterior instability or static anterior subluxation.
Latissimus Dorsi
The latissimus dorsi is a powerful thoracohumeral muscle. It originates from the inferior angle of the scapula, the 9th to 12th ribs, the spinous process of the 7th to 12th thoracic vertebrae, the thoracolumbar fascia, and the posterior one-third of the iliac crest. It inserts just inferior to the lesser tuberosity. Its contraction results in extension, adduction, and internal rotation of the arm. It is innervated by the middle subscapularis nerve or thoracodorsal nerve. This particular anatomical aspect is highly interesting when transferring the latissimus dorsi in place of the subscapularis, since this nerve rises from the posterior cord, as does the upper and lower subscapular nerves. Thereby, transferring the latissimus dorsi to compensate for subscapularis insufficiency has the potential of being particularly synergistic.
The latissimus dorsi is a well-known and studied muscle for transfers at the shoulder. It was first described in obstetrical brachial plexus palsies sequelae to reanimate or reinforce forward elevation and external rotation in Erb palsies. Gerber extended its indication to use it for irreparable posterosuperior cuff tears [10]. When considering transfer of the latissimus dorsi for posterosuperior irreparable cuff tears, adding a combined transfer of the teres major is controversial, and the debate remains open. However, the excursion of these two musculotendinous units is different, with more excursion for latissimus than the teres major. Moreover, the bulkiness of the transfers is significantly increased when both muscles are kept together, which may lead to impingement on the brachial plexus or axillary nerve when transferred together to the anterior aspect of the shoulder [29••]. For these reasons, for anterosuperior irreparable cuff tears, most would recommend transferring only the latissimus dorsi to the lesser tuberosity.
The surgical technique for anterior transfer of the latissimus dorsi to the lesser tuberosity has evolved, and may be performed with open techniques, with arthroscopic assistance, or completely arthroscopically. Any of these techniques provide benefits and disadvantages. Arthroscopic harvest of the latissimus dorsi clearly allows to specifically identify the latissimus dorsi tendon and separate it from the teres major tendon in an easier manner than when harvested through an axillary open approach. However, the dissection between the bellies of the two muscles, mandatory in order to obtain a sufficient excursion of the transfer, is difficult and technically demanding under arthroscopy, when more easily performed open.
First described by Elhassan in an anatomical feasibility study, the latissimus dorsi transfer for irreparable subscapularis requires awareness of the surrounding nerves, particularly the axillary and radial nerves, and in a broader level, the posterior cord of the brachial plexus. Different scenarios were studied in the anatomy lab to evaluate which route would create less impingement on the previously cited nerves, and the best configuration is the isolated transfer of the latissimus dorsi, separated from the teres major, when transferred to the upper half of the lesser tuberosity [29••]. The tendon must remain lateral and superior to the axillary and radial nerves and to the brachial plexus. In scenarios where both the muscles were transferred, the bulkiness of the transfer created a major impingement on the posterior cord. Consequently, the gold standard latissimus dorsi transfer to the lesser tuberosity for irreparable subscapularis is an isolated tendon transfer from the lower to the upper half of the lesser tuberosity, leaving the axillary nerve medial and posterior to the tendon.
Arthroscopy Considerations
Arthroscopically assisted harvest of the latissimus dorsi was first performed and described by Laurent Lafosse in 2005, and has been recently updated by Kany [20••] The harvesting is identical when this transfer is used for irreparable posterosuperior or anterosuperior cuff tears).The scope is introduced in the subacromial space through a lateral portal (Fig. 3). A working portal is created anterolaterally (Fig. 4). A space is created between the humerus and the posterior aspect of the anterior deltoid and pectoralis major. The posterior face of the pectoralis major is dissected until the tendon and its insertion onto the humeral shaft is identified. Visualization is improved by placing the shoulder in forward flexion and slight internal rotation. A second working portal is created inferiorly to improve access to the humeral shaft. The insertion of the latissimus dorsi is identified medial to the long head of the biceps after the scope has been switched to the anterolateral portal (Fig. 5). A switching stick can be used at that step as a retractor to lift the pectoralis major and deltoid up and enlarge the working space. The radial nerve (specifically the branch to the long head of triceps) lies anterior to the latissimus dorsi tendon (Fig. 6), and should be identified and protected. Radiofrequency is used to detach the tendon. Sutures are then passed through the tendon with the help of antegrade or retrograde suture passing devices. This last step represents one of the major difficulties encountered during the arthroscopic technique. Once detached and loaded with traction sutures, the LD needs to be separated from the teres major and the many adhesions limiting its excursion (i.e., skin adhesion at its superficial layer, and bonny insertion on the scapula). Kany suggests and describes the use of endoscopy dissection scissors, long enough to push the dissection to the required level [20••]. Once released, the tendon is brought to its new insertion point (i.e., subscapularis footprint) and attached with conventional anchor-based arthroscopic techniques.
Fig. 3.
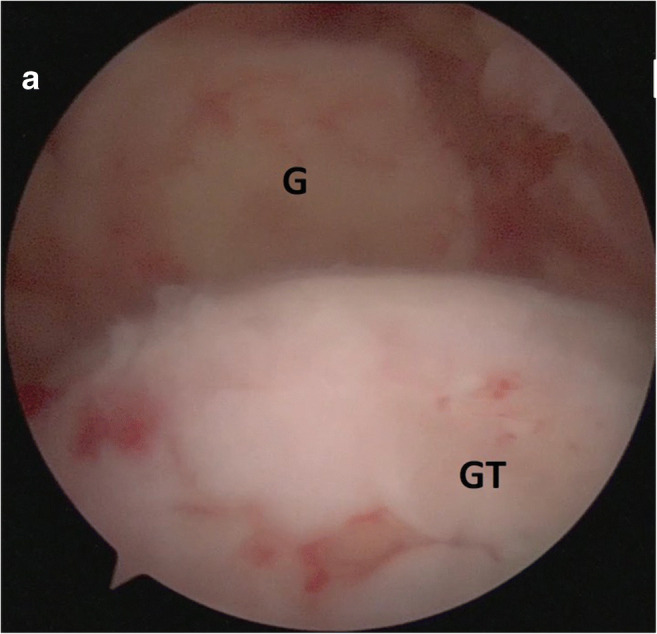
Exploration of a right shoulder through a lateral approach. G, glenoid; GT, greater tuberosity. The irreparable subscapularis tear is assessed. Complementary cuff repair can be performed arthroscopically
Fig. 4.
Creation of working portals. From a lateral visualization portal, more anterior portals are created, using needles
Fig. 5.

Latissimus dorsi exposition (right shoulder, visualization from anterolateral portal). From an anterolateral visualization, the space behind the pectoralis major is prepared, the conjoint tendon is dissected, and the latissimus (star) is exposed
Fig. 6.

Latissimus detachment (right shoulder; arm in forward flexion, internal rotation). Rn, radial nerve; LD, latissimus dorsi; BG, bicipital groove
Open Considerations
For an open transfer, the latissimus dorsi may be harvested and transferred using a one-incision or a two-incision technique. In the one-incision technique, the whole procedure (harvest and transfer) is performed through a deltopectoral approach. Harvest requires either partial detachment of the upper third of the pectoralis major tendon or an alternating retraction of its upper and lower borders, enabling to work on the latissimus dorsi tendon above or below the pectoralis major. The whole release of the LD is performed though this anterior approach, including the release of the belly of the muscle, but sometimes excursion of the tendon remains insufficient. Thereby, a separate axillary approach has the potential to provide a more complete the release of the muscle to facilitate its transfer from the humeral shaft to the lesser tuberosity.
Authors’ Preferred Technique
Currently, in our practice, we favor a combined open-arthroscopic approach, using an axillary open exposure to harvest and mobilize the latissimus dorsi and arthroscopic techniques for tendon fixation. This provides two potential benefits. First, the arthroscopic approach remains the best way to evaluate the glenohumeral joint and perform any partial rotator cuff repair. Second, the dissection, identification, and detachment of the latissimus dorsi tendon are actually easier to perform than from an open axillary approach, since separation of the latissimus dorsi from the teres major may be difficult with open techniques even in the most experienced hands. Fixation of the LD tendon, once prepared and loaded with traction sutures, is easily managed arthroscopically as a conventional subscapularis repair would be (Figs. 7 and 8). However, before tendon fixation, a complementary axillary approach is used, and the tendon is brought from its anterior insertion to the posterior aspect of the shoulder, where the axillary incision lies, in order to dissect the muscle belly and release its adhesions from the skin and scapula, to maximize excursion as previously mentioned (Fig. 9). In addition, suture placement in the tendon is easier in the axillary open approach, which allows placing sutures all the way to the musculotendinous junction if needed. An important maneuver that we recommend using in order not to lose the correct path of the tendon regarding the nerves is to place a suture in the tendon before bringing it from anterior to posterior. This suture will guide the traction sutures from the posterior space of the axillary dissection, back into the anterior aspect of the shoulder before attaching it back to the humerus at the level of the subscapularis footprint (Fig. 12). The transferred tendon should remain lateral and anterior to the axillary nerve (Figs. 10 and 11).
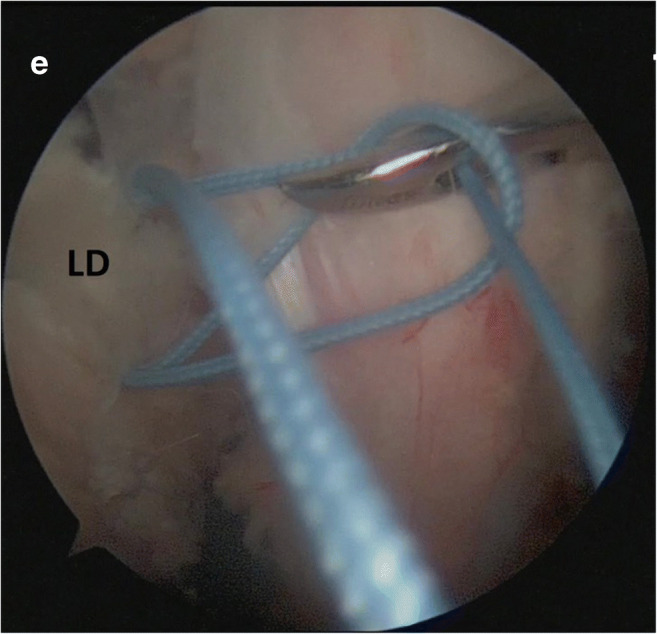
Fig. 7.

Latissimus dorsi brought back to the lesser tuberosity after traction sutures were loaded. LD, latissimus Dorsi; CT conjoint tendon
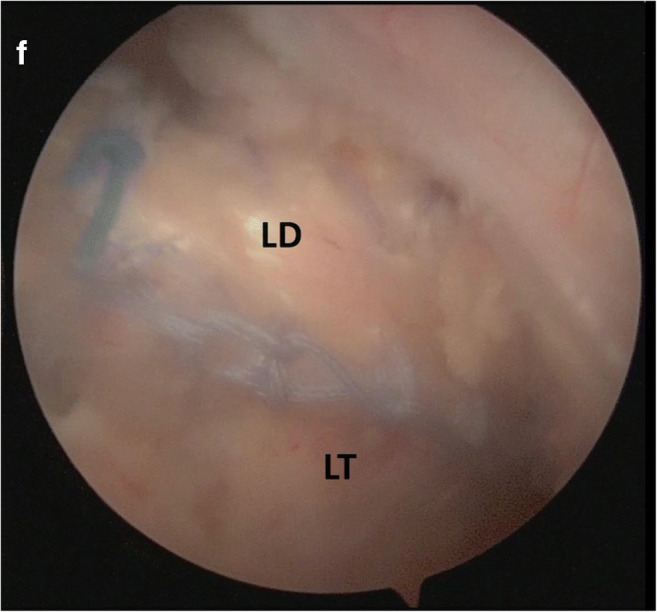
Fig. 8.
Latissimus dorsi is attached to the lesser tuberosity with a minimum of 3 anchors. The picture is showing the lasso loop suture being performed on the medial anchor. LD: Latissimus Dorsi
Fig. 9.

Latissimus dorsi is dissected and released from its adhesions on the skin and scapula. The picture is showing the latissimus belly, released from the surrounding adhesions, and the tendon loaded with sutures, which will be used for the fixation of the transfer on the lesser tuberosity thanks to knotless anchors
Fig. 12.
Latissimus dorsi transferred and fixed on the lesser tuberosity. The picture is showing the tendon attached to the lesser tuberosity. It is fixed on 3 anchors: two lateral row knotless anchors and one medial and superior anchor
Fig. 10.
Representation of the shuttle relay. The picture is showing the shuttle relay passed under the conjoint tendon, along the teres major to mark the course of the transfer.
Fig. 11.
Representation of the transfer of the latissimus dorsi. The picture is showing the transfer passed under the radial nerve, lateral to the axillary nerve
Conclusions
Irreparable anterosuperior cuff tears may be managed surgically by transferring to the lesser tuberosity either the whole pectoralis major or parts of it or the latissimus dorsi tendon. Long-term outcome studies have reported satisfactory results with transfer of the pectoralis major, particularly in patients with an isolated irreparable subscapularis tear and no static anterior subluxation. However, some studies have reported higher failure rates, and the ability of this transfer to maintain improvements in strength seems to be more limited. As such, it may be best to reserve this transfer for patients with low functional needs, with main focus on reducing pain and improving functional outcomes. Transfer of the latissimus dorsi to the lesser tuberosity is definitely attractive. However, there is very limited information in the peer reviewed literature on its outcome. Performing this transfer with arthroscopically assisted techniques is challenging, with a steep learning curve associated with the procedure. There is always risk of injury to major anatomical structures such as radial nerve, axillary nerve, or vascular structures during all phases of the surgery. However, with experience, we believe that this procedure can be performed safely provided a meticulous surgical technique is used.
Compliance with Ethical Standards
Conflict of Interest
The authors declare that they have no conflict of interest.
Human and Animal Right and Informed Consent
This article does not contain any studies with human or animal subjects performed by any of the authors.
Footnotes
This article is part of the Topical Collection on Surgical Management of Massive Irreparable Cuff Tears.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Marion Burnier and Thibault Lafosse equally contributed to the redaction of this Manuscript
Contributor Information
Marion Burnier, Email: marion.burnier@wanadoo.fr.
Thibault Lafosse, Email: thiblaff@gmail.com.
References
Papers of particular interest, published recently, have been highlighted as: • Of importance •• Of major importance
- 1.Yamamoto A, Takagishi K, Osawa T, Yanagawa T, Nakajima D, Shitara H, Kobayashi T. Prevalence and risk factors of a rotator cuff tear in the general population. J Shoulder Elb Surg. 2010;19(1):116–120. doi: 10.1016/j.jse.2009.04.006. [DOI] [PubMed] [Google Scholar]
- 2.Paletta GA, Jr, Warner JJ, Warren RF, Deutsch A, Altchek DW. Shoulder kinematics with two-plane x-ray evaluation in patients with anterior instability or rotator cuff tearing. J Shoulder Elb Surg. 1997;6(6):516–527. doi: 10.1016/S1058-2746(97)90084-7. [DOI] [PubMed] [Google Scholar]
- 3.Lippitt SB, Vanderhooft JE, Harris SL, Sidles JA, Harryman DT, 2nd, Matsen FA., 3rd Glenohumeral stability from concavity-compression: a quantitative analysis. J Shoulder Elb Surg. 1993;2(1):27–35. doi: 10.1016/S1058-2746(09)80134-1. [DOI] [PubMed] [Google Scholar]
- 4.Hamada K, Fukuda H, Mikasa M, Kobayashi Y. Roentgenographic findings in massive rotator cuff tears. A long-term observation Clinical orthopaedics and related research. 1990;254:92–96. [PubMed] [Google Scholar]
- 5.Godeneche A, Freychet B, Lanzetti RM, Clechet J, Carrillon Y, Saffarini M. Should massive rotator cuff tears be reconstructed even when only partially repairable? Knee surgery, sports traumatology, arthroscopy : official journal of the ESSKA. 2017;25(7):2164–2173. doi: 10.1007/s00167-016-4105-2. [DOI] [PubMed] [Google Scholar]
- 6.Lewington MR, Ferguson DP, Smith TD, Burks R, Coady C, Wong IH. Graft utilization in the bridging reconstruction of irreparable rotator cuff tears: a systematic review. Am J Sports Med. 2017;45(13):3149–3157. doi: 10.1177/0363546517694355. [DOI] [PubMed] [Google Scholar]
- 7.Prat D, Tenenbaum S, Pritsch M, Oran A, Vogel G. Sub-acromial balloon spacer for irreparable rotator cuff tears: Is it an appropriate salvage procedure? Journal of orthopaedic surgery (Hong Kong) 2018;26(2):2309499018770887. doi: 10.1177/2309499018770887. [DOI] [PubMed] [Google Scholar]
- 8.Mihata T, Lee TQ, Watanabe C, Fukunishi K, Ohue M, Tsujimura T, Kinoshita M. Clinical results of arthroscopic superior capsule reconstruction for irreparable rotator cuff tears. Arthroscopy : the journal of arthroscopic & related surgery : official publication of the Arthroscopy Association of North America and the International Arthroscopy Association. 2013;29(3):459–470. doi: 10.1016/j.arthro.2012.10.022. [DOI] [PubMed] [Google Scholar]
- 9.Elhassan BT, Wagner ER, Werthel JD. Outcome of lower trapezius transfer to reconstruct massive irreparable posterior-superior rotator cuff tear. J Shoulder Elb Surg. 2016;25(8):1346–1353. doi: 10.1016/j.jse.2015.12.006. [DOI] [PubMed] [Google Scholar]
- 10.Gerber C, Hersche O. Tendon transfers for the treatment of irreparable rotator cuff defects. The Orthopedic clinics of North America. 1997;28(2):195–203. doi: 10.1016/S0030-5898(05)70279-0. [DOI] [PubMed] [Google Scholar]
- 11.Elhassan BT, Wagner ER, Bishop AT. Feasibility of contralateral trapezius transfer to restore shoulder external rotation: part I. J Shoulder Elb Surg. 2012;21(10):1363–1369. doi: 10.1016/j.jse.2011.10.031. [DOI] [PubMed] [Google Scholar]
- 12.Mun SW, Kim JY, Yi SH, Baek CH. Latissimus dorsi transfer for irreparable subscapularis tendon tears. J Shoulder Elb Surg. 2018;27(6):1057–1064. doi: 10.1016/j.jse.2017.11.022. [DOI] [PubMed] [Google Scholar]
- 13.Warner JJ. Management of massive irreparable rotator cuff tears: the role of tendon transfer. Instr Course Lect. 2001;50:63–71. [PubMed] [Google Scholar]
- 14.Gerber C, Krushell RJ. Isolated rupture of the tendon of the subscapularis muscle. Clinical features in 16 cases. The Journal of bone and joint surgery British volume. 1991;73(3):389–394. doi: 10.1302/0301-620X.73B3.1670434. [DOI] [PubMed] [Google Scholar]
- 15.Burkhart SS. Arthroscopic treatment of massive rotator cuff tears. Clinical results and biomechanical rationale Clinical orthopaedics and related research. 1991;267:45–56. [PubMed] [Google Scholar]
- 16.Resch H, Povacz P, Ritter E, Matschi W. Transfer of the pectoralis major muscle for the treatment of irreparable rupture of the subscapularis tendon. J Bone Joint Surg Am. 2000;82(3):372–382. doi: 10.2106/00004623-200003000-00008. [DOI] [PubMed] [Google Scholar]
- 17.Deutsch A, Altchek DW, Veltri DM, Potter HG, Warren RF. Traumatic tears of the subscapularis tendon. Clinical diagnosis, magnetic resonance imaging findings, and operative treatment. Am J Sports Med. 1997;25(1):13–22. doi: 10.1177/036354659702500104. [DOI] [PubMed] [Google Scholar]
- 18.Harryman DT, 2nd, Mack LA, Wang KY, Jackins SE, Richardson ML, Matsen FA., 3rd Repairs of the rotator cuff. Correlation of functional results with integrity of the cuff. J Bone Joint Surg Am. 1991;73(7):982–989. doi: 10.2106/00004623-199173070-00004. [DOI] [PubMed] [Google Scholar]
- 19.Paladini P, Campi F, Merolla G, Pellegrini A, Porcellini G. Pectoralis minor tendon transfer for irreparable anterosuperior cuff tears. J Shoulder Elb Surg. 2013;22(6):e1–e5. doi: 10.1016/j.jse.2012.12.030. [DOI] [PubMed] [Google Scholar]
- 20.Kany J, Guinand R, Croutzet P, Valenti P, Werthel JD, Grimberg J. Arthroscopic-assisted latissimus dorsi transfer for subscapularis deficiency. Eur J Orthop Surg Traumatol. 2016;26(3):329–334. doi: 10.1007/s00590-016-1753-3. [DOI] [PubMed] [Google Scholar]
- 21.Konrad GG, Sudkamp NP, Kreuz PC, Jolly JT, McMahon PJ, Debski RE. Pectoralis major tendon transfers above or underneath the conjoint tendon in subscapularis-deficient shoulders: an in vitro biomechanical analysis. J Bone Joint Surg Am. 2007;89(11):2477–2484. doi: 10.2106/JBJS.F.00811. [DOI] [PubMed] [Google Scholar]
- 22.Jennings GJ, Keereweer S, Buijze GA, De Beer J, DuToit D. Transfer of segmentally split pectoralis major for the treatment of irreparable rupture of the subscapularis tendon. J Shoulder Elb Surg. 2007;16(6):837–842. doi: 10.1016/j.jse.2007.03.030. [DOI] [PubMed] [Google Scholar]
- 23.Gerber C, Hersche O, Farron A. Isolated rupture of the subscapularis tendon. J Bone Joint Surg Am. 1996;78(7):1015–1023. doi: 10.2106/00004623-199607000-00005. [DOI] [PubMed] [Google Scholar]
- 24.Ernstbrunner L, Wieser K, Catanzaro S, Agten CA, Fornaciari P, Bauer DE, Gerber C. Long-term outcomes of pectoralis major transfer for the treatment of irreparable subscapularis tears: results after a mean follow-up of 20 years. J Bone Joint Surg Am. 2019;101(23):2091–2100. doi: 10.2106/JBJS.19.00172. [DOI] [PubMed] [Google Scholar]
- 25.Moroder P, Schulz E, Mitterer M, Plachel F, Resch H, Lederer S. Long-term outcome after pectoralis major transfer for irreparable anterosuperior rotator cuff tears. J Bone Joint Surg Am. 2017;99(3):239–245. doi: 10.2106/JBJS.16.00485. [DOI] [PubMed] [Google Scholar]
- 26.Gavriilidis I, Kircher J, Magosch P, Lichtenberg S, Habermeyer P. Pectoralis major transfer for the treatment of irreparable anterosuperior rotator cuff tears. Int Orthop. 2010;34(5):689–694. doi: 10.1007/s00264-009-0799-9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 27.Elhassan B, Ozbaydar M, Massimini D, Diller D, Higgins L, Warner JJ. Transfer of pectoralis major for the treatment of irreparable tears of subscapularis: does it work? The Journal of bone and joint surgery British volume. 2008;90(8):1059–1065. doi: 10.1302/0301-620X.90B8.20659. [DOI] [PubMed] [Google Scholar]
- 28.Shin JJ, Saccomanno MF, Cole BJ, Romeo AA, Nicholson GP, Verma NN. Pectoralis major transfer for treatment of irreparable subscapularis tear: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2016;24(6):1951–1960. doi: 10.1007/s00167-014-3229-5. [DOI] [PubMed] [Google Scholar]
- 29.Elhassan BT. Feasibility of latissimus and teres major transfer to reconstruct irreparable subscapularis tendon tear: an anatomic study. Journal of Shoulder and Elbow Surgery. 2015;24(4):e102–e103. doi: 10.1016/j.jse.2014.12.035. [DOI] [PubMed] [Google Scholar]