

Key Points
Question
What is the diagnostic accuracy of the red reflex test for detecting ocular pathologies in infants?
Findings
In this systematic review and meta-analysis including 5 studies of 8713 patients, the red reflex test had a low sensitivity and a high specificity for detecting ocular pathologies.
Meaning
When screening infants, an abnormal red reflex test result is highly indicative of an ocular pathology, but a normal red reflex result does not rule out ocular pathologies.
Abstract
Importance
Red reflex testing is a simple and inexpensive method implemented in many countries as an important part of infant screening for ocular pathologies.
Objectives
To review the literature on the diagnostic accuracy of the red reflex test in infant screening for ocular pathologies and to perform meta-analyses to provide summary estimates.
Data Sources
The following literature databases were searched for English-language, peer-reviewed literature, published until April 19, 2020: Cochrane Central, PubMed/MEDLINE, Embase, Web of Science Core Collection, BIOSIS Previews, Current Contents Connect, Data Citation Index, Derwent Innovations Index, KCI-Korean Journal Database, Russian Science Citation Index, SciELO Citation Index, CINAHL (Cumulative Index to Nursing and Allied Health Literature), and ClinicalTrials.gov.
Study Selection
Eligibility criteria were defined according to population (studies of consecutively screened infants), exposure (red reflex or Brückner test as the index test), comparator (any ophthalmological examination), and study type (any study with diagnostic test accuracy data).
Data Extraction and Synthesis
The Preferred Reporting Items for Systematic Reviews and Meta-Analysis of Diagnostic Test Accuracy Studies (PRISMA-DTA) guidelines were followed. Data were extracted independently by 2 authors. For summary estimates of diagnostic test accuracy, the hierarchical summary receiver operating characteristics curve was used. Prevalence of ocular pathologies was introduced for a prevalence meta-analysis, which was then used in calculations of diagnostic accuracy of the red reflex test when applied in infant screening.
Main Outcomes and Measures
True-positive, false-positive, true-negative, and false-negative findings; sensitivity; specificity; and positive and negative predictive values.
Results
In this meta-analysis, 8713 unique infants from 5 unique studies were eligible for qualitative and quantitative review. All studies used the red reflex test without pupillary dilation and were compared with a reference test performed with pupillary dilation. For any ocular pathology, an estimated sensitivity of 7.5% (95% CI, 7.4%-7.5%) and specificity of 97.5% (95% CI, 97.5%-97.5%) was found. Focusing on ocular pathologies that required a medical or surgical intervention, sensitivity improved to 17.5% (95% CI, 0.8%-84.8%) and specificity remained high at 97.6% (95% CI, 87.7%-99.6%).
Conclusions and Relevance
These findings suggest that an abnormal red reflex finding most likely reflects an underlying ocular pathology. However, a normal red reflex finding during screening does not exclude ocular disease.
This systematic review and meta-analysis reviews the literature on diagnostic accuracy of the red reflex test in infant screening for ocular pathologies and provides summary estimates of sensitivity and specificity.
Introduction
“Red reflex testing is an essential component of the neonatal, infant, and child physical examination,” according to a joint policy statement by the American Academy of Pediatrics, American Association for Pediatric Ophthalmology and Strabismus, the American Academy of Ophthalmology, and the American Association of Certified Orthoptists.1(p1401) During red reflex testing, the reflection of light from the posterior segment of the eye is observed through an ophthalmoscope, and the pupil will appear red. Anything that blocks the passage of light through the eye will be observed as a duller red reflex, or the red reflex may be entirely blocked, making the pupil appear dark. In addition, structural abnormalities of the posterior pole will change the reflection of light and can be detected during the examination. Finally, large refractive errors may be observed as changes in the red reflex because the passage of light through the eye depends on the bending (refraction) of light by the optical media.
The aim of red reflex testing in infants is to ensure early detection of ocular diseases that will impair visual development (eg, congenital cataracts, vitreous masses, retinoblastoma, or other congenital abnormalities, such as chorioretinal coloboma). Congenital cataracts are rare (annual incidence, 18 to 36 per 100 000 population), but they are an important cause of avoidable blindness.2,3 Retinoblastoma (approximately 5 per 100 000 population) is seen even less frequently but is an important disease in which early detection prevents loss of vision or early death.4
Given the rarity of the conditions that the red reflex test in infants is aimed at detecting, a large number of infants and children needs to be screened to detect those with disease. From a practical point of view, clinicians need insight into the test’s diagnostic accuracy. The aim of this systematic review and meta-analysis was to examine the diagnostic test accuracy of red reflex screening.
Methods
Protocol and Registration
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis of Diagnostic Test Accuracy Studies (PRISMA-DTA).5 Our protocol was submitted prospectively to PROSPERO.6
Eligibility Criteria
We defined our eligibility criteria according to population, exposure, comparator, and study type. Studies in a setting of consecutively screened infants (aged <1 year) who are not a priori diagnosed with a certain disease were eligible. We restricted to studies that only considered infants or studies that included infants as a subset of the study population where data from such a subset could be extracted.
Eligible studies used the red reflex as the index test. The Brückner test (a red reflex–like fundus reflection test that examines both eyes at the same time) was considered for this study if the test was used to identify ocular abnormalities. This is an important distinction because the Brückner test can also be used to identify ocular misalignment, which was not the aim of this review. Eligible studies provided data for diagnostic accuracy calculation for the index test. Therefore, studies using the index test as part of the screening or the diagnosis but without reporting any test specific data were not considered eligible for this study.
Any ophthalmological examination was considered the reference standard for the comparator. We did not restrict this definition further. Eligible studies tested all participants in the analysis with the reference standard. Therefore, studies only performing reference standard evaluation on participants with an abnormal red reflex finding would not be considered eligible, because such an approach would not allow calculation of diagnostic test accuracy.
Any prospective and retrospective studies with diagnostic test accuracy data, regardless of the study design, were eligible. We did not consider single case studies or case series. We did not use any date restrictions. We only considered studies published in English.
Information Sources, Search, and Study Selection
The search was conducted on April 19, 2020 (see eMethods 1 in the Supplement). The following literature databases were searched: Cochrane Central, PubMed/MEDLINE, Embase, Web of Science Core Collection, BIOSIS Previews, Current Contents Connect, Data Citation Index, Derwent Innovations Index, KCI-Korean Journal Database, Russian Science Citation Index, SciELO Citation Index, CINAHL (Cumulative Index to Nursing and Allied Health Literature), and ClinicalTrials.gov. One author (Y.S.) examined the title and abstracts of all identified records and removed duplicates and obviously irrelevant reports. Two authors (Y.S. and L.K.) screened the remaining references in full text. Any disagreements between the authors were discussed to reach consensus, and if consensus could not be reached, a third author (D.B.-H.) was invited for the final decision. Reference lists were reviewed to identify additional relevant studies.
Data Collection, Data Extraction, and Assessment of Risk of Bias
Using predesigned data extraction forms, we extracted data regarding study design, participant characteristics, methodological details regarding index test and reference standard, and results. Results of interest were data regarding diagnostic accuracy for detecting any ocular pathology and ocular pathology requiring further interventions. Ocular pathologies that required a medical or surgical intervention (hereinafter referred to as intervention demanding) were defined by a senior pediatric ophthalmologist (L.K.). We extracted information regarding any missing data from the analysis (participants included in the study but excluded from the analyses). Two authors (Y.S. and D.C.S.) extracted all data independently. Quality of eligible studies was assessed using the recommended revised tool for the quality assessment of diagnostic accuracy studies.7 Two authors (Y.S. and M.A-B.) evaluated risk of bias independently. Disagreements between the authors in data extraction and risk of bias assessment were discussed to reach consensus, and if consensus could not be reached, a third author (L.K.) was invited for final decision.
Diagnostic Accuracy Measures, Synthesis of Results, and Meta-analysis
All eligible studies were included for a qualitative synthesis. The main outcomes for this study were diagnostic test accuracy characteristics: true-positive, false-positive, true-negative, and false-negative findings; sensitivity; and specificity. For quantitative analyses, we followed the Cochrane Handbook for methodological guidance.8 Further details are specified in eMethods 2 in the Supplement.
Results
Study Selection
Among the 1215 records identified by the literature search, 530 were duplicates, 598 were obviously irrelevant, and 70 were non-English language records. The remaining 17 records were read in full text, and 5 of these were eligible for both the qualitative and the quantitative synthesis (Figure 1).
Figure 1. Flow Diagram of Study Selection Process.

Study Characteristics
The 5 studies included9,10,11,12,13 were reported as full-text articles and collectively summarized data on 8713 unique participants (Table 1). All were prospective single-center studies and recruited newborns. Collectively, studies included participants self-identified as mostly White and Asian (including Middle Eastern). In all studies, the red reflex (index) test was performed without pupillary dilation, and the ophthalmic examination (reference test) was performed with pupillary dilation. In 4 studies,9,10,11,12 the red reflex test was performed by a pediatrician, whereas in 1 study,13 an ophthalmologist performed a Brückner test (eTable 1 in the Supplement). The reference test was made using ophthalmological examination in 3 studies11,12,13 and using digital images for later interpretation by an ophthalmologist in 2 studies9,10 (eTable 1 in the Supplement).
Table 1. Characteristics of Included Studies.
| Source (country) | Study design | Population source | Population recruitment | Population characteristics | Race/ethnicity | Funding |
|---|---|---|---|---|---|---|
| Ludwig et al,9 2018 (US) | Prospective, cohort, single center | Consecutive newborns | 830 Approached, 202 recruited, and RRT conducted in 194 | 47% Female; 7% BW <2.5 kg; 61% VD | 55% White; 37% Asian; 1% Black; 7% Native Hawaiian | Grants from university, private and public foundations |
| Ma et al,10 2018 (China) | Prospective, cross-sectional, single center | Consecutive newborns approached 6 wk after birth | 1785 Approached, 481 recruited, and RRT conducted in 481 | 47% Female; 10% BW <2.5 kg; 57% VD | Not specified, but population from Beijing, where most identify as Han Chinese | Grants from hospital and public foundations |
| Mussavi et al,11 2014 (Iran) | Prospective, cross-sectional, single center | Consecutive newborns | Number approached was unclear, and RRT conducted in 255 | 45% Female; BW not reported; 43% VD | Not specified, but population from Ilam, where almost 100% identify as Middle Eastern origin | Grants from hospital |
| Sun et al,12 2016 (China) | Prospective, cross-sectional, single center | Consecutive newborns not preterm, not admitted to ICU, not with ocular deformities noticed without screening | 9985 Approached, 8497 eligible for study, 7641 gave consent, and RRT conducted in 7641 | 48% Female; mean (SD) BW, 3.4 (0.4) kg; 52% VD | Not specified, but population from Jinan, where most identify as Han Chinese | Grants from hospital and public foundations |
| Viquez and Wu,13 2020 (Costa Rica) | Prospective, cross-sectional, single center | Consecutive newborns not critically ill but who required monitoring | 71 Approached, 71 eligible and gave consent, and RRT conducted in 71 | 42% Female; mean (SD) BW, 2.9 (0.5) kg; 27% VD | Not specified, but population from San José, where population is highly diverse; most individuals identified as White, Asian, and Hispanic | No funding for the study, but travel grant from a pharmaceutical company for presentation |
Abbreviations: BW, birth weight; ICU, intensive care unit; RRT, red reflex test; VD, vaginal delivery.
Results of Individual Studies, Risk of Bias Within Studies, and Applicability
Ludwig et al9 screened 194 newborns and found no abnormal red reflex, leading to a sensitivity of 0% and a specificity of 100% (95% CI, 97%-100%). Ma et al10 screened 481 infants at 6 weeks of age and found an abnormal red reflex in 2 cases (0.4%), leading to a sensitivity of 1% (95% CI, 0%-4%) and specificity of 100% (95% CI, 99%-100%). Sun et al12 screened 7641 newborns, of whom 570 (7.5%) had an abnormal red reflex, which led to a sensitivity of 14% (95% CI, 13%-15%) and a specificity of 95% (95% CI, 95%-96%). Viquez and Wu13 screened 142 eyes of 71 newborns, among whom 31 eyes (21.8%) had an abnormal red reflex, leading to a sensitivity of 23% (95% CI, 11%-40%) and a specificity of 88% (95% CI, 81%-93%). Mussavi et al11 screened 255 newborns, with the pediatrician being asked to score the redness on a scale of 0 to 10 (10 indicates bold red) and where only 10 was accepted as a normal red reflex. Here, 168 screened newborns (65.9%) were deemed to have an abnormal red reflex, which led to a sensitivity of 85% (95% CI, 74%-92%) and a specificity of 40% (95% CI, 33%-47%).11 For comparison, the authors also asked ophthalmologists to perform the red reflex test as usual, where the sensitivity was 12% and the specificity 93%.11
Risk of bias within individual studies showed that patient selection was the most challenged domain (eTable 2 in the Supplement). Three studies9,10,12 highlighted an important discrepancy between the number of parents approached and the number of participants with consent and data (Table 1), which likely reflects difficulties in conducting a comprehensive screening study in newborns.
Identified Ocular Pathologies in Screened Infants
The prevalence of any ocular pathology in infants was estimated to be 27.3% (95% CI, 24.0%-30.9%) (eFigure 1 in the Supplement). Ocular pathologies identified with the reference test are summarized in Table 2. A small number of these cases were deemed to require follow-up or intervention (Table 2). Such pathologies had an estimated prevalence of 0.9% (95% CI, 0.2%-2.0%) (eFigure 2 in the Supplement). Because of the small number of studies in these prevalence meta-analyses, we refrained from commenting on measures of heterogeneity and risk of bias across studies (eFigures 1 and 2 in the Supplement). Sensitivity analyses showed robustness of these calculations; pooled prevalence ranged from 25.8% to 28.2% for any pathology and from 0.8% to 1.3% for intervention-demanding pathology (eFigures 1 and 2 in the Supplement).
Table 2. Ocular Pathologies Identified in Included Studies Using the Reference Test.
| Source | Total No. | Pathology, No. (%) | No. identified pathologies in the anterior segment | Posterior segment pathology, No. (%) | No. identified pathologies in the posterior segment | Any medical or surgical intervention–demanding pathology, No. (%) | No. medical or surgical intervention–demanding pathologies | |
|---|---|---|---|---|---|---|---|---|
| Any ocular | Anterior segment | |||||||
| Ludwig et al,9 2018 | 194 | 49 (25) | 0 | 0 | 49 (25) | 36 Retinal HM, 31 macular HM, 26 optic nerve flame HM, 4 grouped pigmentation, 6 choroidal nevus, 1 choroidal pigmentation, 1 albinotic choroid, 1 polar bear tracks, 1 pigmentary retinopathy, 1 focal depigmentation of the RPE | 0 | 0 |
| Ma et al,10 2018 | 481 | 162 (34) | 4 (1) | 2 Corneal dermoid tumor, 1 cataract, 1 persistent pupillary membrane | 158 (33) | 85 Retinal whites, 32 retinal HM, 16 retinal pigmentation, 9 ROP, 8 albinismlike fundus, 2 FEVR, 2 immature retina, 2 large physiologic cupping of optic disc, 1 vitreous HM, 1 choroidal nevus | 12 (2) | 9 ROP, 2 FEVR, 1 cataract |
| Mussavi et al,11 2014 | 255 | 60 (24) | 0 | 0 | 60 (24) | 44 Retinal HM, 10 vessel reduction, 6 salt-and-pepper retinopathy, 5 retinal color change | 0 | 0 |
| Sun et al,12 2016 | 7641 | 2178 (29) | 223 (3) | 218 Persistent membranes or pigment granule, 2 cataract, 2 floaters in aqueous humor, 1 coloboma iridis, 1 corneal nebulaa | 1955 (26) | 1680 Retinal HM, 118 abnormal pigmentation, 51 peripheral subretinal exudative change, 38 FEVR, 17 medullated fibers, 12 persistent hyaloid artery, 11 vitreous opacity, 9 vascular abnormalities, 7 severe optic nerve cupping, 6 choroidal coloboma, 1 retinoblastoma, 1 persistent fetal vasculature, 1 oculocutaneous albinism, 1 nevus of Ota, 1 morning glory disc anomaly, 1 intravitreous masses with persistent hyaloid artery | 108 (1) | 51 Peripheral subretinal exudative change, 38 FEVR, 12 persistent hyaloid artery, 2 cataract, 2 floaters in aqueous humor, 1 retinoblastoma, 1 persistent fetal vasculature, 1 intravitreous masses with persistent hyaloid artery |
| Viquez and Wu,13 2020b | 142 | 31 (22) | 2 (1) | 2 Cataract | 29 (20) | 27 Retinal HM, 2 optic nerve coloboma | 2 (1) | 2 cataract |
Abbreviations: FEVR, familial exudative vitreoretinopathy; HM, hemorrhage; ROP, retinopathy of prematurity; RPE, retinal pigment epithelium.
One individual has more than 1 diagnosis.
Data extraction was only possible per eye.
Diagnostic Test Accuracy of the Red Reflex
True-positive (0%-20.0%; summary estimate, 2.0%) and false-positive (range, 0%-45.9%; summary estimate, 1.8%) findings were largely comparable; that is, approximately half of those identified as having an abnormal red reflex had any ocular pathology (Table 3). False-negative findings ranged from 3.5% to 33.3% (summary estimate, 25.3%); hence, the test did not identify an important proportion of those with any ocular pathology (Table 3). A normal red reflex correctly identified those with no ocular pathology (true-negative findings) in 30.6% to 74.7% (summary estimate, 70.9%) (Table 3). Bivariate meta-analysis of studies estimated sensitivity at 7.5% (95% CI, 7.4%-7.5%) and specificity at 97.5% (95% CI, 97.5%-97.5%). Sensitivity analyses showed robustness of calculations (eTable 3 in the Supplement). Based on the calculated diagnostic test accuracy estimates and the prevalence estimate, it was possible to calculate that 53% of those with abnormal red reflex findings would have any ocular pathology (the positive predictive value [PPV]), and 74% of those with a normal red reflex finding would be disease free (the negative predictive value [NPV]).
Table 3. Diagnostic Test Accuracy of the Red Reflex Test for Detecting Ocular Pathologies.
| Source | Total No. | No. (%) of patients | Sensitivity, % (95% CI) | Specificity, % (95% CI) | |||||
|---|---|---|---|---|---|---|---|---|---|
| Disease prevalence | Abnormal red reflex | True-positive finding | False-positive finding | False-negative finding | True-negative finding | ||||
| Any ocular pathology | |||||||||
| Ludwig et al,9 2018 | 194 | 49 (25.3) | 0 | 0 | 0 | 49 (25.3) | 145 (74.7) | 0 (0-7) | 100 (97-100) |
| Ma et al,10 2018 | 481 | 162 (33.7) | 2 (0.4) | 2 (0.4) | 0 | 160 (33.3) | 319 (66.3) | 1 (0-4) | 100 (99-100) |
| Mussavi et al,11 2014 | 255 | 60 (23.5) | 168 (65.9) | 51 (20.0) | 117 (45.9) | 9 (3.5) | 78 (30.6) | 85 (74-92) | 40 (33-47) |
| Sun et al,12 2016 | 7641 | 2178 (28.5) | 570 (7.5) | 303 (4.0) | 267 (3.5) | 1875 (24.5) | 5196 (68.0) | 14 (13-15) | 95 (95-96) |
| Viquez and Wu,13 2020a | 142 | 31 (21.8) | 20 (14.1) | 7 (4.9) | 13 (9.2) | 24 (16.9) | 98 (69.0) | 23 (11-40) | 88 (81-93) |
| Summary estimate, % (95% CI) | 27.3 (24.0-30.9) | 2.0 | 1.8 | 25.3 | 70.9 | 7.5 (7.4-7.5) | 97.5 (97.5-97.5) | ||
| Medical or surgical intervention–demanding ocular pathology | |||||||||
| Ludwig et al,9 2018 | 194 | 0 | 0 | 0 | 0 | 0 | 194 (100) | NaN | 100 (98-100) |
| Ma et al,10 2018 | 481 | 12 (2.5) | 2 (0.4) | 1 (0.2) | 1 (0.2) | 11 (2.3) | 468 (97.3) | 8 (1-35) | 100 (99-100) |
| Mussavi et al,11 2014 | 255 | 0 | 168 (65.9) | 0 | 168 (65.9) | 0 | 87 (34.1) | NaN | 34 (28-40) |
| Sun et al,12 2016 | 7641 | 108 (1.4) | 570 (7.5) | 5 (0.1) | 565 (7.4) | 103 (1.3) | 6968 (91.2) | 5 (2-10) | 98 (97-98) |
| Viquez and Wu,13 2020a | 142 | 2 (1.4) | 20 (14.1) | 2 (1.4) | 18 (12.7) | 0 | 122 (85.9) | 100 (34-100) | 87 (81-92) |
| Summary estimate, % (95% CI)b | 0.9 (0.2-2.0) | 0.2 | 2.4 | 0.7 | 96.7 | 17.5 (0.8-84.8) | 97.6 (87.7-99.6) | ||
Abbreviation: NaN, not a number, due to division by zero.
Data extraction was only possible per eye.
We then focused on medical or surgical intervention–demanding ocular pathologies (Table 3). True-positive findings ranged from 0% to 1.4%, which was generally lower than the false-positive findings ranging from 0% to 65.9%. False-negative findings were low (0%-2.3%) and true-negative findings were high (34.1%-100%). For this subgroup meta-analysis, we were only able to include 3 studies, because Ludwig et al9 and Mussavi et al11 did not have any cases with medical or surgical intervention–demanding ocular pathologies that would lead to division by 0 in analyses (Table 3). Bivariate meta-analysis of studies found estimates of sensitivity at 17.5% (95% CI, 0.8%-84.8%) and specificity at 97.6% (95% CI, 87.7%-99.6%). Sensitivity analyses showed that excluding the smaller study of Viquez and Wu13 did not affect the overall conclusion of the test (sensitivity, 6.1%; 95% CI, 2.0%-17.3%), but that excluding Ma et al10 (sensitivity, 62.1%; 95% CI, 0.2%-99.9%) or Sun et al12 (sensitivity, 55.9%; 95% CI, 0.7%-99.5%) would significantly increase the sensitivity of the test (eTable 4 in the Supplement).
The hierarchical summary receiving operating characteristic curve was depicted to show the association between sensitivity and specificity for the red reflex test in detecting any ocular pathology and in detecting any medical or surgical intervention–demanding ocular pathology (eFigure 3 in the Supplement). Based on the calculated diagnostic test accuracy estimates and the prevalence estimate, it was possible to calculate that 6.2% of those with abnormal red reflex findings would have a medical or surgical intervention–demanding ocular pathology (the PPV), and 99.2% of those with a normal red reflex finding would be free of having such condition (the NPV).
Performance of the Red Reflex Test in Infant Eye Screening
Given the calculated summary estimates of the diagnostic accuracy of the red reflex test for detecting any ocular pathology and for detecting any medical or surgical intervention–demanding ocular pathology, the association between disease prevalence and the PPV and the NPV for the red reflex test can be depicted (Figure 2). These models highlight the performance of the red reflex test when applied in populations with lower or higher disease prevalence. In a pediatric ophthalmologist clinic where the prevalence of ocular diseases would be high, the red reflex as a test has a high PPV and a low NPV (Figure 2). However, when the test is applied in a nonselected infant population, where the prevalence of ocular diseases would be low, the red reflex test has a low to moderate PPV and a high NPV (Figure 2).
Figure 2. Performance Evaluation of the Red Light Reflex for Detection of Ocular Pathologies.
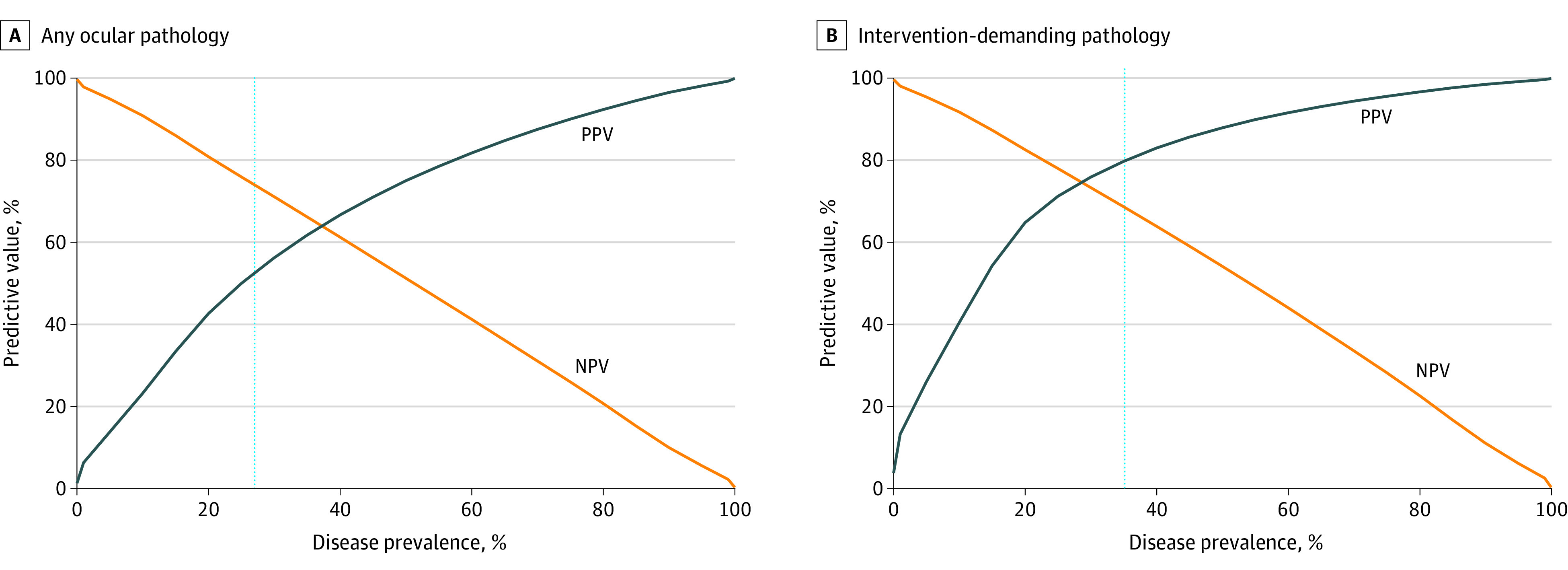
Based on summary estimates of the diagnostic test accuracy, we plotted the association between the disease prevalence (x-axis) and the positive predictive value (PPV, ie, percentage with disease given that the test result is positive) and the negative predictive value (NPV, ie, percentage not having disease given that the test result is negative) (y-axis). The dotted line shows the calculated prevalence among infants of any ocular pathology (A) and any medical or surgical intervention–demanding ocular pathology (B).
Discussion
We identified 5 studies9,10,11,12,13 in which red reflex testing without pupillary dilation was compared with standard ophthalmological examination performed after pupil dilation in a total of 8642 consecutively recruited newborns. The rate of false-positive findings (ie, abnormal red reflex test result without underlying ocular abnormality) was 1.8%. False-positive findings may lead to parental anxiety and will result in overreferral of healthy infants to ophthalmological evaluation. The true challenge, however, lies in the number of false-negative findings (ie, those infants with severe ocular disease who will be missed because of a normal red reflex test result), which was 25.3%. When interpreting these diagnostic accuracy measures in the context of screening, it is important to consider the population in question and the expected disease prevalence. For any ocular pathology, we calculated the NPV to be 74%. However, ophthalmological findings requiring medical follow-up or surgical intervention are significantly rarer, and here we calculated an NPV of 99.2%.
Red reflex testing will only identify those changes that lie within the passage of light, that is, retinal changes that are restricted to the peripheral retina and do not affect the central part that reflects the light will not be detected by the test. The 2 studies from China10,12 described a surprisingly large number of infants with familial exudative vitreoretinopathy (2 of 481 [0.4%] and 38 of 7641 [0.5%]) or peripheral subretinal exudation (51 of 7641 [0.7%]). These findings can be devastating to visual function, but as expected, they were not detected by the red reflex test, because they mainly involve the peripheral retina. The missed cases that should have been detected by red reflex screening included 1 case of congenital cataract and 1 case of intravitreous masses with persistent hyaloid artery. Thus, of a reported total of 5 infants with congenital cataract, 4 were correctly detected by red reflex testing results. The missed cases that would have been likely to be detected depending on retinal location and size of the lesion included retinoblastoma (n = 1), vitreous opacities (n = 11), persistent hyaloid artery (n = 11), choroidal coloboma (n = 6), and macular hemorrhages (n = 31).
None of the studies used pupil dilation for red reflex testing. Newborns and infants have smaller pupils,14 and because the test depends on the amount of light passing through the pupil, a small pupil may theoretically decrease the validity of the test. Mussavi et al11 demonstrated that the diagnostic threshold of the test could be altered by changing the testing conditions. Medical pupil dilation can be associated with risk of adverse effects, including tachycardia and cardiac arrythmia, which should be weighed against the benefits of detecting severe ocular disease on a case-by-case basis, but pupil size can be increased by performing the test in a dark room. The red reflex may disappear when the visual axis of the eye overlaps with the light from the ophthalmoscope and conversely, the color of the reflex improves as the angle of incoming light deviates slightly from the center of fixation.15 This effect is used in the Brückner test to assess for ocular misalignment, and slightly deviating the angle of illumination may improve visualization of the red reflex if the infant focuses directly on the light source.16
Several factors may influence the quality or redness of the red reflex. The red reflex depends on the reflection of light from the posterior segment of the eye.17 Incoming light is to some extent absorbed by the retinal pigment epithelium, and retinal pigment epithelium layer thickness varies significantly between different races/ethnicities, with White, Asian, and Chinese individuals having significantly thinner retinal pigment epithelium than Black individuals.18 We found no studies evaluating the accuracy of red reflex testing across ethnicity. Most infants included in our meta-analyses were Asian, Chinese, or White. The accuracy of red reflex testing in newborns with a high degree of pigmentation is uncertain.
The value of red reflex testing in a real-world scenario has been demonstrated in a study comparing age at diagnosis for congenital cataract in Denmark and Sweden, 2 neighboring countries that are socioeconomically and genetically comparable and with comparable health care systems. Red reflex testing is performed on all neonates in Sweden, whereas pencil light examination of the eyes is used in Denmark.19 This study demonstrated that congenital cataract is diagnosed later in Denmark compared with Sweden—possibly explained by the red reflex test not being used in Denmark. Age at diagnosis and early surgery is of extreme importance for visual outcome, and a mere 3-week delay in surgery decreases visual outcome by 1 line on a visual acuity chart at school age. Surgery after 14 weeks of age will—at best—result in permanent irreversible moderate visual impairment (Snellen 20/60 to 20/160).20
Limitations
Selection bias is likely to influence the results presented in this study. Four studies9,10,12,13 reported that they approached 12 671 newborns, but red reflex testing was only performed in 8387, and 1 study11 did not report on the number of families approached. Reasons for this discrepancy are well described, but families may have been more likely to agree to participate if they had reasons to suspect any eye disease, for example, owing to family history.
Conclusions
Finding a normal red reflex during screening does not exclude ocular disease, but finding an abnormal red reflex most likely reflects an underlying ocular pathology. The NPV of severe ocular disease was 99.2%, which means that 99 of 100 infants with a normal red reflex will have no ocular disease; the PPV of an abnormal red reflex was 7.7%, which means that the risk of severe ocular disease is increased more than 7-fold in these infants. Important findings, such as retinoblastoma and congenital cataracts, were occasionally missed, but as real-life data from Denmark and Sweden clearly demonstrate,19 not performing red reflex screening will have detrimental effects on ocular health and visual outcomes.
eMethods 1. Literature Search in Different Databases
eMethods 2. Details of Data Analysis
eTable 1. Methods for Index and Reference Test in Included Studies
eTable 2. Risk of Bias Within Individual Studies
eTable 3. Sensitivity Analyses of the Bivariate Meta-analysis of the Diagnostic Test Accuracy of the Red Reflex on Detecting Any Ocular Pathology
eTable 4. Sensitivity Analyses of the Bivariate Meta-analysis of the Diagnostic Test Accuracy of the Red Reflex on Detecting Any Medical or Surgical Intervention–Demanding Ocular Pathology
eFigure 1. Calculated Summary Prevalence Estimate of Any Ocular Pathology, Risk of Bias Across Studies, and Sensitivity Analyses
eFigure 2. Calculated Summary Prevalence Estimate of Medical or Surgical Intervention–Demanding Ocular Pathology, Risk of Bias Across Studies, and Sensitivity Analyses
eFigure 3. Hierarchical Summary Receiver Operating Characteristics Model (HSROC) Curve for Evaluating the Association Between Sensitivity and Specificity for the Red Reflex in Identifying Ocular Pathology
References
- 1.American Academy of Pediatrics; Section on Ophthalmology; American Association for Pediatric Ophthalmology and Strabismus; American Academy of Ophthalmology; American Association of Certified Orthoptists . Red reflex examination in neonates, infants, and children. Pediatrics. 2008;122(6):1401-1404. doi: 10.1542/peds.2008-2624 [DOI] [PubMed] [Google Scholar]
- 2.Sheeladevi S, Lawrenson JG, Fielder AR, Suttle CM. Global prevalence of childhood cataract: a systematic review. Eye (Lond). 2016;30(9):1160-1169. doi: 10.1038/eye.2016.156 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Gilbert C, Foster A. Childhood blindness in the context of VISION 2020—the right to sight. Bull World Health Organ. 2001;79(3):227-232. [PMC free article] [PubMed] [Google Scholar]
- 4.Dimaras H, Kimani K, Dimba EA, et al. Retinoblastoma. Lancet. 2012;379(9824):1436-1446. doi: 10.1016/S0140-6736(11)61137-9 [DOI] [PubMed] [Google Scholar]
- 5.McInnes MDF, Moher D, Thombs BD, et al. ; and the PRISMA-DTA Group . Preferred Reporting Items for a Systematic Review and Meta-analysis of Diagnostic Test Accuracy Studies: the PRISMA-DTA statement. JAMA. 2018;319(4):388-396. doi: 10.1001/jama.2017.19163 [DOI] [PubMed] [Google Scholar]
- 6.Subhi Y, Schmidt DC, Al-Bakri M, Bach-Holm D, Kessel L Diagnostic test accuracy of the red reflex for detecting ocular pathology in infants: a systematic review with meta-analysis. PROSPERO. CRD42020182397. Accessed July 5, 2020. https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42020182397
- 7.Whiting PF, Rutjes AW, Westwood ME, et al. ; QUADAS-2 Group . QUADAS-2: a revised tool for the quality assessment of diagnostic accuracy studies. Ann Intern Med. 2011;155(8):529-536. doi: 10.7326/0003-4819-155-8-201110180-00009 [DOI] [PubMed] [Google Scholar]
- 8.Higgins JPT, Thomas J, Chandler J, Cumpston M, Li T, Page MJ, Welch VA, eds. Cochrane Handbook for Systematic Reviews of Interventions, version 6.0. Updated July 2019. Accessed May 29, 2020. https://www.training.cochrane.org/handbook. [DOI] [PMC free article] [PubMed]
- 9.Ludwig CA, Callaway NF, Blumenkranz MS, Fredrick DR, Moshfeghi DM. Validity of the red reflex exam in the Newborn Eye Screening Test Cohort. Ophthalmic Surg Lasers Imaging Retina. 2018;49(2):103-110. doi: 10.3928/23258160-20180129-04 [DOI] [PubMed] [Google Scholar]
- 10.Ma Y, Deng G, Ma J, Liu J, Li S, Lu H. Universal ocular screening of 481 infants using wide-field digital imaging system. BMC Ophthalmol. 2018;18(1):283. doi: 10.1186/s12886-018-0943-7 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Mussavi M, Asadollahi K, Janbaz F, Mansoori E, Abbasi N. The evaluation of red reflex sensitivity and specificity test among neonates in different conditions. Iran J Pediatr. 2014;24(6):697-702. [PMC free article] [PubMed] [Google Scholar]
- 12.Sun M, Ma A, Li F, et al. Sensitivity and specificity of red reflex test in newborn eye screening. J Pediatr. 2016;179:192-196.e4. doi: 10.1016/j.jpeds.2016.08.048 [DOI] [PubMed] [Google Scholar]
- 13.Viquez MV, Wu L. Sensitivity and specificity of the red reflex in Costa Rican newborns [in Spanish]. Arch Soc Esp Oftalmol. 2020;95(1):4-8. doi: 10.1016/j.oftal.2019.10.007 [DOI] [PubMed] [Google Scholar]
- 14.MacLachlan C, Howland HC. Normal values and standard deviations for pupil diameter and interpupillary distance in subjects aged 1 month to 19 years. Ophthalmic Physiol Opt. 2002;22(3):175-182. doi: 10.1046/j.1475-1313.2002.00023.x [DOI] [PubMed] [Google Scholar]
- 15.de Groot MJ, van der Helm FC, Simonsz HJ. The mechanism underlying the Brückner effect studied with an automated, high-resolution, continuously scanning Brückner device. Strabismus. 2015;23(2):85-100. doi: 10.3109/09273972.2015.1036081 [DOI] [PubMed] [Google Scholar]
- 16.Roe LD, Guyton DL. The light that leaks: Brückner and the red reflex. Surv Ophthalmol. 1984;28(6):665-670. doi: 10.1016/0039-6257(84)90187-5 [DOI] [PubMed] [Google Scholar]
- 17.Mallmann MB, Tomasi YT, Boing AF. Neonatal screening tests in Brazil: prevalence rates and regional and socioeconomic inequalities. J Pediatr (Rio J). 2020;96(4):487-494. doi: 10.1016/j.jped.2019.02.008 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Ko F, Foster PJ, Strouthidis NG, et al. ; UK Biobank Eye and Vision Consortium . Associations with retinal pigment epithelium thickness measures in a large cohort: results from the UK Biobank. Ophthalmology. 2017;124(1):105-117. doi: 10.1016/j.ophtha.2016.07.033 [DOI] [PubMed] [Google Scholar]
- 19.Haargaard B, Nyström A, Rosensvärd A, Tornqvist K, Magnusson G. The Pediatric Cataract Register (PECARE): analysis of age at detection of congenital cataract. Acta Ophthalmol. 2015;93(1):24-26. doi: 10.1111/aos.12445 [DOI] [PubMed] [Google Scholar]
- 20.Birch EE, Cheng C, Stager DR Jr, Weakley DR Jr, Stager DR Sr. The critical period for surgical treatment of dense congenital bilateral cataracts. J AAPOS. 2009;13(1):67-71. doi: 10.1016/j.jaapos.2008.07.010 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eMethods 1. Literature Search in Different Databases
eMethods 2. Details of Data Analysis
eTable 1. Methods for Index and Reference Test in Included Studies
eTable 2. Risk of Bias Within Individual Studies
eTable 3. Sensitivity Analyses of the Bivariate Meta-analysis of the Diagnostic Test Accuracy of the Red Reflex on Detecting Any Ocular Pathology
eTable 4. Sensitivity Analyses of the Bivariate Meta-analysis of the Diagnostic Test Accuracy of the Red Reflex on Detecting Any Medical or Surgical Intervention–Demanding Ocular Pathology
eFigure 1. Calculated Summary Prevalence Estimate of Any Ocular Pathology, Risk of Bias Across Studies, and Sensitivity Analyses
eFigure 2. Calculated Summary Prevalence Estimate of Medical or Surgical Intervention–Demanding Ocular Pathology, Risk of Bias Across Studies, and Sensitivity Analyses
eFigure 3. Hierarchical Summary Receiver Operating Characteristics Model (HSROC) Curve for Evaluating the Association Between Sensitivity and Specificity for the Red Reflex in Identifying Ocular Pathology