

Abstract
Background:
Early adversity consistently predicts youth psychopathology. However, the pathways linking unique dimensions of early adversity, such as deprivation, to psychopathology are understudied. Here, we evaluate a theoretical model linking early deprivation exposure with psychopathology prospectively through language ability.
Methods:
Participants included 2,301 youth (47.5% female) enrolled in the Fragile Families and Child Wellbeing Study. We include data from assessment points at ages 1, 3, 5, 9, and 15. Latent factors for deprivation and threat were modeled from multiple indicators at ages 1 and 3. Youth language ability was assessed at Age 5. Indicators of psychopathology were assessed at ages 5, 9, and 15. A structural equation model tested longitudinal paths to internalizing and externalizing psychopathology from experiences of deprivation and threat.
Results:
Deprivation from birth to Age 3 was associated with an indirect effect on internalizing and externalizing symptoms in early childhood (Age 5), later childhood (Age 9), and adolescence (Age 15) via language ability in early childhood (Age 5). Early threat exposure was associated with increased internalizing and externalizing psychopathology across all ages. There was no significant indirect effect from threat to psychopathology via language ability.
Conclusions:
The effects of deprivation on psychopathology during early childhood, late childhood, and adolescence are explained, in part, through early childhood language ability. Results provide insight into language ability as a possible opportunity for intervention.
Keywords: Deprivation, threat, language, adversity, internalizing psychopathology, externalizing psychopathology
Introduction
Early adversity affects an estimated 50% of all adults in the United States and increases psychopathology risk (Green et al., 2010; McLaughlin et al., 2012). Adolescents who experience early adversity are at higher risk for all types of psychopathology (Keyes et al., 2012). Importantly, early adversity accounts for nearly one third of all psychiatric disorder onsets in adolescence and up to 45% of childhood-onset disorders (Green et al., 2010; McLaughlin et al., 2012). While the association between early adversity exposure and psychopathology risk is well established, we know surprisingly little about the developmental paths linking early adversity to adolescent psychopathology. One potential path that we investigate here is the effect of early deprivation on language ability and subsequent psychopathology, indexed in the present study by internalizing and externalizing symptoms.
Cumulative risk models assume that the path linking early adversity with psychopathology risk is universal across adversity types and operate through changes in physiological responses to stress (Anda et al., 2005). Investigations adopting this model sum across types of adversity and find this predicts increased risk for psychopathology and other negative life outcomes. In one example of this approach, Schroeder et al (2020) recently found that more adversity exposure was associated with increased risk of behavior problems at Age 9 in the Fragile Families and Child Wellbeing Study (FFCWS). In a complementary model, the dimensional model of adversity and psychopathology (DMAP) differentiates between the developmental influences of deprivation and threat (Sheridan & McLaughlin, 2016). Deprivation is conceptualized as the absence of complexity in expected cognitive and social stimulation in infancy and early childhood (Sheridan & McLaughlin, 2014). Experiences on the deprivation dimension include parental separation and low cognitive and social stimulation in the home. Threatening experiences involve harm or threat of harm to the child or a close other (Sheridan & McLaughlin, 2014) and include physical and sexual abuse, domestic violence, or exposure to community violence. The DMAP proposes that deprivation and threat will influence psychopathology risk through distinct neurodevelopmental pathways. Specifically, experiences of deprivation are posited to influence psychopathology by altering early forms of learning that have lasting implications for cognitive development, particularly in the domains of language and executive function. In contrast, experiences of threat are thought to alter social-emotional development, such as emotional reactivity. While summing across experiences may predict psychopathology, DMAP argues this summation may miss distinct, malleable pathways.
Initial research demonstrates that deprivation has unique associations with markers of cognitive functioning. Controlling for threat, deprivation is associated with poor executive function, language development, and reading ability (e.g., Lambert et al., 2017; Machlin et al., 2019; Wolf & Suntheimer, 2019). In an initial test of the DMAP, early childhood deprivation, but not threat, was linked with late adolescent psychopathology via language ability in early adolescence (Miller et al., 2018). Here, we extend this initial test by examining whether language ability may link deprivation with psychopathology risk at earlier stages of development. This is critical as it may highlight earlier opportunities for intervention and prevention of later psychopathology (Forbes et al., 2019).
Prior research suggests that reduced language ability is associated with increased psychopathology risk, which may be due to language-associated difficulties with emotion regulation and social interactions (Carpenter & Drabick, 2011; Cohen et al., 2013; Helland et al., 2014; Salmon et al., 2016; Yew & O’Kearney, 2013). Available data suggest this relationship may strengthen with age (Salmon et al., 2016); language ability and future psychopathology are linked more strongly in later childhood and adolescence compared to early childhood (Bornstein et al., 2013; Petersen et al., 2013). These studies imply that lower early childhood language ability may not be immediately associated with psychopathology risk, but psychopathology risk increases with prolonged exposure to this language deficit. Thus, language ability may mediate associations with psychopathology only once sufficiently developed so that it can be used in the service of complex self-regulatory strategies such as cognitive reappraisal (Salmon et al., 2016).
Present study
The present study had three main aims. First, we assessed the underlying, latent dimensions of deprivation and threat in a large national sample. In prior work, we and others have primarily tested the DMAP using composite index scores for deprivation and threat (Machlin et al., 2019; Wolf & Suntheimer, 2019) because of the known co-occurrence of early adversity in the population. Here, we are able to test underlying latent dimensions given the size and diversity of the sample, and we hypothesized that we would find support for two, separable latent factors for deprivation and threat. Second, we tested the DMAP model using latent factors of deprivation and threat exposure. Consistent with the DMAP, we hypothesized that deprivation, but not threat, would be indirectly associated with internalizing and externalizing symptoms in adolescence via language ability. We hypothesized that threat would be directly associated with internalizing and externalizing symptoms in adolescence. We examined whether our findings held when controlling for income-to-needs, maternal education, and prenatal risk as these have been previously linked with psychopathology (Ashford et al., 2008; Bøe et al., 2014; Busso et al., 2017). Third, we examined whether the relationship between deprivation, threat, and internalizing and externalizing symptoms via language ability held across early childhood, late childhood, and adolescence. This extends our previous study, which only examined associations with psychopathology in late adolescence (Miller et al., 2018). We hypothesized that the indirect effect of deprivation on internalizing and externalizing symptoms via language ability would be present for late childhood and adolescence but not early childhood.
Methods
Data
Data were drawn from the FFCWS. The FFCWS is a population-based, birth cohort study of 4,898 children (born between 1998 and 2000) across 20 large cities in the United States. FFCSW oversampled for nonmarital births and includes a large, diverse sample of children from lower income families and neighborhoods. Detailed methodology is available in Reichman, Teitler, Garfinkel, and McLanahan (2001) and here: https://fragilefamilies.princeton.edu/documentation. For the present study, we included individuals if they had valid data on internalizing or externalizing variables at each ages 5, 9, and 15. In other words, each person in the sample had information about their internalizing or externalizing problems across all three years. This resulted in a sample of 2,301 (47% of the original sample). Of these, 1,092 of youth identified as female (47.5%). At Age 15, youth self-reported race/ethnicity with 384 White non-Hispanic/Latinx individuals (16.7%), 1,086 Black/ African American non-Hispanic (47.2%) individuals, 492 Hispanic/Latinx individuals (21.4%), 52 other non-Hispanic (2.3%), and 112 multiracial individuals (4.9%). Data from the ages 1, 3, 5, 9, and 15 assessments are used in the present analysis. All participants provided informed consent to participate, and all procedures were approved by the affiliated human subjects review board.
Measures
Detailed information about scoring and coding of each deprivation and threat indicators is available in Appendix S1 and Table S1.
Deprivation.
The latent construct of deprivation was modeled from seven manifest, categorical indicators comprised of both primary caregiver- and observational-report data from the Age 1 and Age 3 interviews (see Table 2 and Appendix S1). Consistent with DMAP (Sheridan & McLaughlin, 2014), and previous investigations of deprivation and threat (Machlin et al., 2019; Miller et al., 2018), these indicators were constructed to capture the absence of complexity in expected cognitive and social stimulation in infancy and early childhood. Indicators include frequent separations from primary caregivers that lasted a week or longer, the absence of cognitive stimulation in daily routines (e.g., playing imaginary games, reading), the number of developmentally appropriate books and toys available to the child, and observed positive parenting interactions during the in-home visit. Higher scores reflect greater exposure to deprivation.
Table 2.
Standardized latent factor loadings
| Age | Factor loading/beta | SE | |
|---|---|---|---|
| Deprivation | |||
| Frequency separations | 1 | 0.47*** | 0.09 |
| Cognitive stimulation | 1 | 0.37*** | 0.04 |
| Number of toys in the home+ | 3 | 0.50*** | 0.04 |
| Number of child books | 3 | 0.57*** | 0.05 |
| Positive parenting interactions | 3 | 0.50*** | 0.05 |
| Frequency of separations | 3 | 0.35*** | 0.09 |
| Cognitive stimulation | 3 | 0.38*** | 0.04 |
| Threat | |||
| Domestic violence exposure | 1 | 0.38*** | 0.05 |
| Mother spanking | 1 | 0.56*** | 0.04 |
| Father spanking | 1 | 0.37*** | 0.05 |
| Physical abuse+ | 3 | 0.60*** | 0.04 |
| Verbal abuse | 3 | 0.42*** | 0.04 |
| Domestic violence exposure | 3 | 0.29*** | 0.04 |
| Community violence | 3 | 0.37*** | 0.03 |
| Covariances between indicators | |||
| Separation Age 1 ↔ Age 3 | 0.48*** | 0.10 | |
| Cognitive stimulation Age 1 ↔ Age 3 | 0.25*** | 0.03 | |
| Spanking mother Age 1 ↔ father Age 1 | 0.61*** | 0.04 | |
| Domestic violence Age 1 ↔ Age 3 | 0.43*** | 0.05 | |
| Verbal abuse Age 3 ↔ physical abuse Age 3 | 0.51*** | 0.02 | |
| Internalizing | |||
| CBCL anxious/depressed+ | 15 | 0.78*** | 0.02 |
| CBCL withdrawn/depressed | 15 | 0.73*** | 0.02 |
| Self-reported depression symptoms | 15 | 0.33*** | 0.03 |
| Self-reported anxiety symptoms | 15 | 0.29*** | 0.03 |
| Externalizing | |||
| CBCL aggressive behavior+ | 15 | 0.90*** | 0.02 |
| CBCL rule-breaking behavior | 15 | 0.81*** | 0.02 |
| Self-reported delinquent behaviors | 15 | 0.34*** | 0.03 |
| Covariances between indicators | |||
| Self-report anxiety ↔ depression | 0.62*** | 0.02 |
, represents the first indicator for each respective factor.
p < .001. CBCL, Child Behavior Checklist; SE, standard error.
Threat.
The latent construct of threat was modeled from seven manifest, categorical and continuous indicators comprised of both primary caregiver- and observational-report data from the Age 1 and Age 3 interviews (see Table 2 and Appendix S1). Consistent with DMAP (Sheridan & McLaughlin, 2014), and previous investigations of deprivation and threat (Machlin et al., 2019; Miller et al., 2018), these indicators were created to assess exposure or threat of exposure to interpersonal violence in the environment. Indicators included frequency of mother and father spanking of their infant (birth to Age 1), physical and emotional abuse as assessed by the Parent–Child Conflict Tactics Scale (Straus, 1979), and exposure to domestic and community violence. Higher scores reflect greater exposure to the threat.
Language ability.
At the Age 5 in-home interview, the child was administered the Woodcock–Johnson Letter–Word Identification Test (WJ; Woodcock et al., 2001) and Peabody Picture Vocabulary Test (PPVT-III; Dunn & Dunn, 1997). The WJ task assesses oral reading skills. The PPVT is an untimed test of receptive vocabulary. Here, we created a composite language ability score by taking the average of the standard score for both tests which reflects the performance of the child relative to same-aged peers1.. Twelve individuals only had one available score and were included in analyses.
Psychopathology. Age 15 internalizing symptoms:
Internalizing symptoms at Age 15 were assessed with a primary caregiver- and self-report instruments. The primary caregiver report included responses to the Child Behavior Checklist (CBCL; Achenbach, 1991). We used total sum scores on the Anxious/Depressed (six items) and Withdrawn/Depressed (two items) scales. Adolescents completed five items from the Centers for Epidemiological Studies Depression Scale (CES-D; Radloff, 1977) assessing depression symptoms and six items from the Brief Symptom Inventory-18 (BSI-18; Derogatis & Melisaratos, 1983) assessing anxiety symptoms. For both scales, the total sum score was used.
Age 15 externalizing symptoms:
Externalizing symptoms at Age 15 were assessed with a combination of primary caregiver- and self-report instruments. The primary caregiver report included total sum scores from the Aggressive (11 items) and Delinquent Behaviors (9 items) subscales of the CBCL. The adolescent completed 13 items drawn from the National Longitudinal Study of Adolescent Health assessing delinquent behaviors (e.g., drug use, vandalism, stealing). The total sum score was used.
Age 5 and Age 9 internalizing and externalizing symptoms:
At the Age 5 and Age 9 interviews, primary caregivers completed selected items from the CBCL (Achen-bach, 1991). We used the total sum score from available items measuring internalizing and externalizing symptoms. For Age 5, a separate mother survey was administered to the biological mother, that contained some other items for the CBCL, but here, we used only the primary caregiver survey consistent with other years. Thus, internalizing symptoms included 16 items from the Withdrawn/Depressed and Anxious/Depressed subscales, and externalizing symptoms included 24 items from the Aggressive and Delinquent Behaviors subscales. For Age 9, internalizing symptoms included 32 items from the Withdrawn/Depressed, Anxious/Depressed, and Somatic complaints subscales, and externalizing symptoms included 35 items from the Aggressive and Delinquent Behaviors sub-scales.
Covariates.
We considered additional covariates in sensitivity analyses (described below), income-to-needs ratio, maternal education level, and prenatal risk (index of prenatal exposure to alcohol, drugs, smoking, low birthweight, and postnatal doctor’s visits). Additional details are available in the Appendix S1. See Table S3 for correlations between latent deprivation and threat with covariates.
Data analytic plan
Data were prepared using SPSS 26 for Mac (IBM Statistics, IBM Corp., Armonk, NY). Preliminary analyses and structural equation models (SEM), including measurement and structural models, were conducted with Mplus 8.4 for Mac (Muthén & Muthen, 2019). Preliminary analyses included descriptive statistics and bivariate correlations estimated in Mplus (See Appendix S1). Across all models described below, model fit was evaluated using a variety of indices consistent with Kline (2015). A nonsignificant chi-square suggests that the model fits the data; however, the chi-square statistic is sensitive to the sample size, resulting in a tendency to reject models with large sample sizes. Thus, alternative model fit statistics are recommended (Hooper et al., 2008). A root mean square error of approximation (RMSEA) around 0.05, a comparative fit index (CFI) over 0.90, and a standardized root mean square residual (SRMR) under 0.08 indicate close fitting models (Hu & Bentler, 1999). All regression coefficients and factor weights are presented as standardized simple effects. For each structural model described below, supplemental tables present results for all paths included (Tables S4–S6). To account for the mixture of continuous and categorical indicators for our latent constructs, the full model used a robust weighted least squares (WLSMV) estimator (Flora & Curran, 2004). WLSMV uses a process that incorporates all available data without deleting missing data or imputing values on other items. Like full information maximum likelihood (FIML) estimation, WLSMV outperforms listwise deletion which reduces power and can result in biased parameter estimates (Asparouhov & Muthén, 2010).
To test our first hypothesis, we constructed a measurement model of our predictors (deprivation and threat) using confirmatory factor analysis (CFA) following standard SEM procedures (Kline, 2015) (see Table 2). We additionally constructed a separate measurement model for Age 15 internalizing and externalizing symptoms (Table 2).2.
To test our second hypothesis, we fit the hypothesized structural model to the data (Figure 1). In this model, Age 15 internalizing and externalizing symptoms were the outcome. This model included direct paths from deprivation and threat to psychopathology. Additionally, Age 5 language ability was included as a mediator of the association between deprivation and psychopathology. Indirect effects were estimated using a nonparametric, bias-corrected bootstrapping approach with 1,000 bootstrap resamples; indirect paths are considered significant if the 95% confidence intervals do not contain zero (Preacher & Hayes, 2008). We present standardized coefficients and confidence intervals for indirect effects. Sex was included as a predictor of language ability and psychopathology. Age 5 psychopathology was included as a predictor of Age 15 psychopathology.3.
Figure 1.
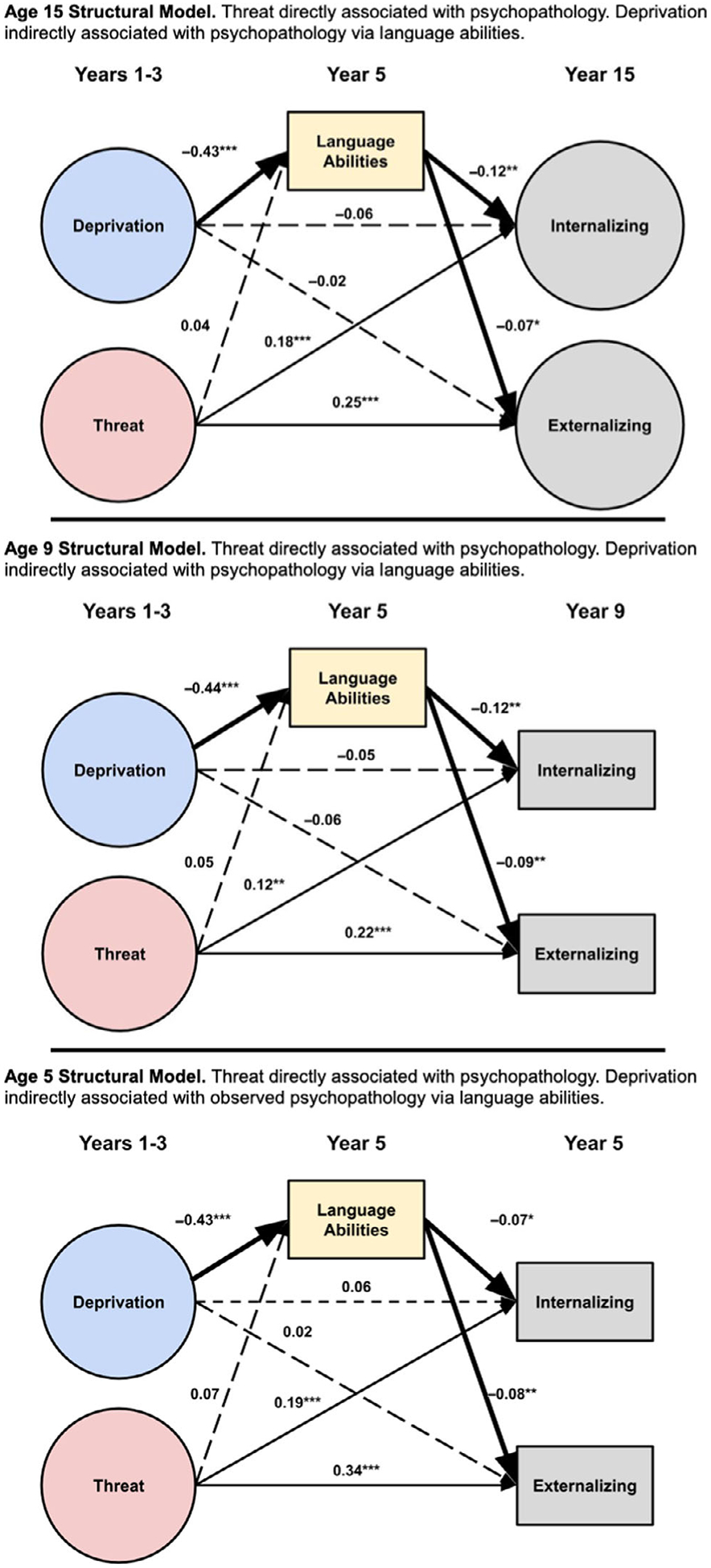
Structural models depicting paths among deprivation, threat, language abilities, and psychopathology. Solid lines depict significant paths, and the thicker lines represent the significant indirect effect from deprivation and psychopathology via language abilities. For clarity, covariates and covariances are not displayed. See Table S1 for all paths and covariances. Circles and rectangles represent latent and observed variables, respectively
To examine our third hypothesis, we constructed two additional structural models with Age 5 and Age 9 psychopathology as the outcome. Each of these models was identical to our main model with one exception. We did not have access to sufficient indicators to model latent psychopathology factors at Age 5 and Age 9. Sex was included as a predictor of language ability and psychopathology in both models. Age 5 psychopathology was included as a predictor of Age 9 psychopathology.4.
For each age, we ran three sensitivity models (N = 9 models) including income-to-needs, maternal education, and prenatal risk as predicators of language ability and psychopathology.
As is common in large population-based studies, missing data are expected across years. Rates of missing data are available in Table 1 and Tables S3, S7, and S8. Comparison of those with valid outcome data (i.e., psychopathology indicators) across years 5, 9, and 15 (N = 2,301) to those without valid outcome data (N = 2,597) across all years revealed no demographic differences by sex, χ2(1) = 0.02, p = .89, race, χ2(1) = 1.26, p = .26, or income-to-needs, t = 0.54, p = .59. Additionally, to ensure our main results were not being driven by sample selection, we ran our measurement and main models for those with valid outcome data at Year 5 (N = 2,960), Year 9 (N = 3,257), and Year 15 (N = 3,595). The pattern of results from both the measurement and main structural model from these sampling conventions was substantively unchanged from the main study sample5. (see Appendix S2, Tables S6, S9, and S10).
Table 1.
Means, standard deviations, range, and model estimated correlations of observed and latent (L) variables
| % Miss. | M | SD | Min/max | Skewness/kurtosis | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Deprivation Age 1–3(L) | - | 0+ | 0.50+ | −1.5/1.5+ | - | - | ||||||||
| 2. Threat Age 1–3(L) | - | 0+ | 0.52+ | −1.57/1.57+ | - | .37*** | - | |||||||
| 3. Language ability Age 5 | 17% | 96.71 | 13.37 | 40/147 | 0.40/0.99 | −.40*** | −.11** | - | ||||||
| 4. Internalizing Age 5 | 1.8% | 4.32 | 3.51 | 0/22 | 1.18/1.56 | .15*** | .22*** | −.11*** | - | |||||
| 5. Externalizing Age 5 | 2.8% | 9.47 | 5.99 | 0/35 | 0.91/0.83 | .18*** | .36*** | −.13*** | .44*** | - | ||||
| 6. Internalizing Age 9 | 6.3% | 5.08 | 5.88 | 0/64 | 3.72/26.22 | .09* | .17*** | −.13*** | .33*** | .20*** | - | |||
| 7. Externalizing Age 9 | 4.3% | 6.44 | 7.20 | 0/70 | 2.76/14.11 | .12** | .35*** | −.13*** | .21*** | .43*** | .68*** | - | ||
| 8. Internalizing Age 15(L) | - | −0.66+ | 1.43+ | −4.95/3.63+ | - | .10* | .17*** | −.12*** | .24*** | .25*** | .36*** | .33*** | - | |
| 9. Externalizing Age 15(L) | - | −0.44+ | 3.10+ | −9.74/8.86+ | - | .16*** | .35*** | −.12*** | .14*** | .40*** | .20*** | .49*** | .62*** | - |
| 10. Sex | 0% | - | - | −.04 | −.11** | .19*** | −.01 | −.10*** | .01 | −.12*** | .14*** | −.10*** |
N = 2,301,
p<.05,
p<.01,
p<.001;
M, mean; SD, standard deviation, L = latent variable.
Means and standard deviations for latent variables are model estimates from the Year 15 structural model. Ranges for latent variables are approximated at 3 standard deviations above and below the mean. Correlations among all variables are model estimated. See Tables S7 and S8 for rates of missingness for latent construct indicators and consideration of alternative estimators robust to nonnormality for the Age 9 models.
Results
Descriptive statistics
Basic descriptive information, including means, standard deviations, frequencies for categorical variables, and correlations for each item-level study variable, can be found in Tables S1, S7, and S8. Descriptive statistics and model estimated correlations among latent constructs and observed variables are shown in Table 1. Briefly, deprivation was positively correlated with threat and internalizing and externalizing symptoms and negatively correlated with language ability. Threat was positively correlated with internalizing and externalizing symptoms and negatively correlated with language ability. Language ability was negatively correlated with internalizing and externalizing symptoms.
Measurement models
Consistent with our first hypothesis, the measurement model for deprivation and threat latent constructs demonstrated acceptable fit, N = 2,283, χ2(71) = 262.49, p < .001, RMSEA = .03[.03,.04], CFI = 0.93, SRMR = 0.06. All indicators loaded positively and significantly onto the two hypothesized latent constructs (Table 2). The measurement model for Age 15 internalizing and externalizing symptoms demonstrated acceptable fit, N = 2,301, χ2(12) = 127.11, p < .001, RMSEA = .07[.06,.08], CFI = 0.97, SRMR = 0.04. All indicators loaded positively and significantly onto the hypothesized latent constructs (Table 2). Covariances were allowed between some indicators and are presented in Table 2.
Age 15 structural model
The Age 15 model demonstrated good fit to the data, χ2(253) = 863.82, p < .001, RMSEA = .03[.03,.04], CFI = 0.93, SRMR = 0.05. Higher language ability was associated with lower internalizing symptoms, β = −0.12, p = .001, and externalizing symptoms, β = −0.07, p < .05. Greater deprivation was associated with lower language ability, β = −0.43, p < .001. Threat was not associated with language ability, β = 0.04, p = .38. As expected, higher threat was directly associated with higher internalizing, β = 0.18, p < .001, and externalizing, β = 0.25, p < .001, symptoms. The direct relationship between deprivation and internalizing, β = −0.06, p = .32, and externalizing, β = −0.02, p = .64, symptoms was not significant. However, consistent with our second hypothesis, the indirect effect from deprivation to internalizing and externalizing symptoms via language ability was significant, β = 0.05, 95%CI[0.02,0.09], β = 0.03, 95%CI[0.01,0.07], respectively. The indirect effect from threat to internalizing and externalizing symptoms via language ability was not significant β = −0.004, 95%CI[−0.02,0.005], β = −0.003, 95% CI[−0.02,0.003], respectively. Overall, the structural model accounted for 13% and 20% of the variance in latent internalizing and externalizing symptoms, respectively (p’s < .001).
Age 9 structural model
The Age 9 model demonstrated good fit, χ2(151) = 505.44, p < .001, RMSEA = .03[.03,.04], CFI = 0.96, SRMR = 0.05. As in the main model, higher language ability was associated with lower internalizing, β = −0.12, p < .001, and externalizing, β = −0.09, p < .01, symptoms. Greater deprivation was associated with lower language ability, β = −0.44, p < .001. Threat was not associated with language ability, β = 0.05, p = .24. As expected, higher threat was directly associated with higher internalizing, β = 0.12, p = .001, and externalizing, β = 0.22, p < .001, symptoms. The direct relationship between deprivation and internalizing, β = −0.05, p = .30, and externalizing, β = −0.06, p = .21, symptoms was not significant. However, as hypothesized, the indirect effect from deprivation to internalizing and externalizing symptoms via language ability was significant, β = 0.05, 95%CI [0.02,0.09], β = 0.04, 95%CI[0.01,0.08], respectively. Consistent with hypotheses, the indirect effect from threat to internalizing and externalizing symptoms via language ability was not significant, β = −0.005, 95%CI[−0.02,0.003], β = −0.004, 95% CI[−0.02,0.002], respectively. This model accounted for 13% and 23% of the variance in internalizing and externalizing symptoms, respectively (p’s < .001).
Age 5 structural model
The Age 5 model demonstrated acceptable fit, χ2(121) = 445.05, p<.001, RMSEA = .03[.03,.04], CFI = 0.91, SRMR = 0.05. Higher language ability was associated with lower internalizing, β = −0.07, p < .05, and externalizing, β = −0.08, p = .01, symptoms. Greater deprivation was associated with lower language ability, β = −0.43, p < .001. Threat was not associated with language ability, β = 0.07, p = .12. Higher threat was directly associated with higher internalizing, β = 0.19, p < .001, and externalizing, β = 0.34, p < .001, symptoms. Greater deprivation was not directly associated with greater Age 5 internalizing, β = .06, p = .18, or externalizing, β = 0.02, p = .62, symptoms. Contrary to hypotheses, the indirect effect from deprivation to internalizing and externalizing symptoms via language ability was significant, β = 0.03, 95%CI[0.001,0.06], β = 0.03, 95%CI[0.01,0.07], respectively. The indirect effect from threat to internalizing and externalizing symptoms via language ability was not significant β = − 0.004, 95%CI[−0.02,0.001], β = −0.005, 95%CI[−0.02,0.001], respectively. This model accounted for 6% and 14% of the variance in internalizing and externalizing symptoms, respectively (p’s < .001).
Sensitivity analyses
Model fit across all alternative models with income-to-needs, maternal education, and prenatal risk as covariates was not acceptable (CFI’s ≤ 0.89 and/or SRMR’s > .07; See Appendix S2, Table S5). Therefore, these models should be interpreted with extreme caution. However, across these models, the pattern of findings from the main structural model was largely unchanged. In particular, the indirect effect of deprivation to internalizing and externalizing symptoms via language ability remained significant for Age 9 and Age 15. At Age 5, the indirect effect of deprivation to externalizing symptoms via language ability remained significant for all covariates, and the indirect effect of deprivation to internalizing problems via language ability remained significant when income-to-needs or maternal education were included. These models resulted in a significant negative relationship between language and threat, and in some cases, a significant, inconsistent mediation, likely the result of statistical suppression (see Appendix S2 for greater discussion).
Discussion
In the present study, we examined pathways of risk from early childhood adversity to psychopathology in a large national sample. Consistent with core predictions of the DMAP (Sheridan & McLaughlin, 2016), we hypothesized that deprivation, but not threat, would be associated with internalizing and externalizing symptoms in adolescence indirectly through language ability. Deprivation from birth to three years old showed an indirect effect on internalizing and externalizing symptoms in adolescence through language ability measured at Age 5 over and above previous internalizing and externalizing symptoms. Threat measured from birth to Age 3 was directly associated with internalizing and externalizing symptoms in adolescence. These findings are comparable to a previous test of this model with a smaller sample and slightly different age ranges (Miller et al., 2018) where we found that deprivation experiences in early childhood were associated with externalizing symptoms in late adolescence via early adolescent verbal ability. As with the present findings, threat was directly associated with internalizing and externalizing symptoms (Miller et al., 2018). However, unlike in the previous study, here we find that language ability additionally mediated the association between deprivation and internalizing problems.
Consistent with our first hypothesis, we found support for two underlying factors of deprivation and threat based on indicators from a child’s early life from birth to Age 3. There is ongoing debate with regard to how to best capture an individual’s exposure to early adversity. Indeed, we have previously used composite index scores (e.g., Machlin et al., 2019) to categorize exposures along dimensions of deprivation and threat. Within this sample, the measurement model supports that the latent structure of deprivation and threat is separable and distinct.
Deprivation was associated with lower language ability. This finding is consistent with prior work that has found significant associations between deprivation and language ability in institutionalized samples (e.g., Fox, Almas, Degnan, Nelson, & Zeanah, 2011) and in children from low socioeconomic status families (Bradley & Corwyn, 2002; McLoyd, 1998). Thus, the current study contributes to the body of literature suggesting that deprivation is associated with decreases in language ability. While deprivation was correlated with psychopathology, deprivation was not directly associated with psychopathology symptoms in the structural models. Given that a substantial portion of the variance in psychopathology remained unexplained in the present study, there may be other mediators in the link between deprivation and psychopathology. Future research in this area is warranted. Additionally, greater threat was correlated at the bivariate level with lower language abilities. This is likely due to the overlap between deprivation and threat exposures as evidenced by the lack of an association in the fully controlled model.
Higher language ability at Age 5 significantly predicted lower internalizing and externalizing symptoms at Age 15. This finding is consistent with prior work linking reduced language ability with higher risk for psychopathology (Bornstein et al., 2013; Petersen et al., 2013). Salmon and colleagues note that language skills are necessary for self-regulation, problem solving, and emotional understanding, all factors that contribute to psychopathology risk (Salmon et al., 2016). Further, language ability is strongly linked with academic performance (Deary et al., 2007), and lower academic achievement has been linked with increased psychopathology risk (Verboom et al., 2014).
Finally, we investigated whether the main structural model from deprivation and threat to psychopathology was present prior to adolescence in early or late childhood. Given that the models included different indicators by necessity given measurement differences across years, absolute, direct comparisons between models cannot be made. Thus, we recommend caution in comparing these results. Contrary to hypotheses, overall results for the early childhood (Age 5) and late childhood (Age 9) model were nearly identical to the main adolescent model. These findings suggest that deprivation may increase risk for psychopathology through reduced language ability across development. One possibility is that language ability may be protective against increased psychopathology symptoms across the lifespan (Salmon et al., 2016). Critically, these results suggest that targeted intervention when deprivation-associated language deficits emerge may help decrease risk of psychopathology in children exposed to deprivation. Encouragingly, early interventions for language ability have already been successfully developed (Domitrovich et al., 2009; Mendelsohn et al., 2001).
The current study makes a novel contribution by measuring deprivation and threat through latent constructs and lending support for a specific structural model across development based on DMAP hypotheses. However, several limitations should be noted. First, the DMAP hypothesizes specific neurobiological pathways for how deprivation and threat become biologically embedded to impact psychopathology risk. Future work focusing on neurobiological pathways would delineate how dimensions of experience are associated with increased psychopathology risk. Second, while this is a large, national sample, it is not representative of the United States as a whole (Reichman et al., 2001). The FFCWS sample was recruited to specifically address nonmarital childbearing and is representative of nonmarital births in US cities with a population over 200,000. Thus, our findings may be specific to this sample. Third, we used child language ability at Age 5 as a marker of language ability. The DMAP model hypothesizes broader effects on cognitive functioning. Thus, future work with more robust measurement of cognitive ability is warranted. Additionally, while we tested three potential confounders, others, such as stress exposure, are important variables to consider in future tests of this model. Here, model fit was not acceptable when including covariates, limiting our interpretation of those models. Finally, while our study benefited from a combination of self-, parent, and observer report across years, items measuring psychopathology were not consistent across years which precluded us from examining growth curves. Relatedly, an ideal test of mediation would demonstrate temporal change across the predictor, mediator, and outcome. We were unable to examine change in each component of our model given the limitations of the data.
In the present study, we extended prior work by measuring deprivation and threat as latent constructs and demonstrating distinct pathways through which deprivation is associated with externalizing and internalizing symptoms in adolescence. Together, our findings support language ability as one potential mediating variable linking deprivation, but not threat, to psychopathology. Clinically, the model provides explicit targets to prevent or mitigate the psychopathology risk across development.
Supplementary Material
sKey points.
The Dimensional Model of Adversity and Psychopathology (DMAP) hypothesizes that deprivation and threat impact psychopathology through distinct paths.
Here, we evaluate a model linking early deprivation with psychopathology prospectively through language ability.
Findings suggest that the impact of deprivation, but not threat, on psychopathology in early childhood, late childhood, and adolescence is in part explained by early childhood language ability.
This suggests an opportunity for intervention on children’s language ability to mitigate psychopathology associated with deprivation.
Acknowledgements
Research reported in this publication was supported by the Eunice Kennedy Shriver National Institute of Child Health and Human Development (NICHD) of the National Institutes of Health under award numbers R01HD36916, R01HD39135, and R01HD40421, as well as a consortium of private foundations. The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health. Preparation of this manuscript was supported by grants from the National Institute of Mental Health (K01MH116325 to A.B.M.; 5T32HD07376 to L.S.M.; R01MH103291, R01MH106482 to K.A.M.; R01MH115004 to M.A.S.). The authors have declared that they have no competing or potential conflicts of interest.
Footnotes
Supporting information
Additional supporting information may be found online in the Supporting Information section at the end of the article:
Conflict of interest statement: No conflicts declared.
Notes
See Appendix S2 and Table S2 for results from the main model separately for WJ and PPVT.
For the internalizing/externalizing measurement model, the MLR estimator, robust to nonnormality, was used given that indicators were mildly skewed.
We ran an additional age 15 model that just included CBCL caregiver report of internalizing and externalizing indices. The pattern of results was identical. See Appendix S2.
We ran additional main structural models without including the language covariate. See Appendix S2 and Figure S1 for results.
In the model with all individuals with valid Year 9 data only, the path between deprivation and externalizing was negative, β=−.08, p = .044. In the model with all individuals with Valid Year 15 data only, greater threat was marginally associated with higher language, β= .08, p = .05. All other paths remained similar to the main study models, including the indirect effects from deprivation to internalizing and externalizing problems via language ability. See Appendix S2.
References
- Achenbach TM (1991). Manual for the Child Behavior Checklist/4–18 and 1991 profile. Burlington, VT: Department of Psychiatry, University of Vermont. [Google Scholar]
- Anda RF, Felitti VJ, Bremner JD, Walker JD, Whitfield C, Perry BD, Dube SR, & Giles WH (2005). The enduring effects of abuse and related adverse experiences in childhood. European Archives of Psychiatry and Clinical Neuroscience, 256, 174–186. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ashford J, Van Lier PA, Timmermans M, Cuijpers P, & Koot HM (2008). Prenatal smoking and internalizing and externalizing problems in children studied from childhood to late adolescence. Journal of the American Academy of Child & Adolescent Psychiatry, 47, 779–787. [DOI] [PubMed] [Google Scholar]
- Asparouhov T, & Muthén B (2010). Weighted least squares estimation with missing data. Mplus Technical Appendix. Available from: http://www.statmodel.com/download/GstrucMissingRevision.pdf [last accessed 20 January 2019]. [Google Scholar]
- Bøe T, Sivertsen B, Heiervang E, Goodman R, Lundervold AJ, & Hysing M (2014). Socioeconomic status and child mental health: The role of parental emotional well-being and parenting practices. Journal of Abnormal Child Psychology, 42, 705–715. [DOI] [PubMed] [Google Scholar]
- Bornstein MH, Hahn C-S, & Suwalsky JTD (2013). Language and internalizing and externalizing behavioral adjustment: Developmental pathways from childhood to adolescence. Development and Psychopathology, 25, 857–878. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bradley RH, & Corwyn RF (2002). Socioeconomic status and child development. Annual Review of Psychology, 53, 371–399. [DOI] [PubMed] [Google Scholar]
- Busso DS, McLaughlin KA, & Sheridan MA (2017). Dimensions of adversity, physiological reactivity, and externalizing psychopathology in adolescence: Deprivation and Threat. Psychosomatic Medicine, 79, 162. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carpenter JL, & Drabick DAG (2011). Co-occurrence of linguistic and behavioural difficulties in early childhood: A developmental psychopathology perspective. Early Child Development and Care, 181, 1021–1045. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cohen NJ, Farnia F, & Im-Bolter N (2013). Higher order language competence and adolescent mental health. Journal of Child Psychology and Psychiatry, 54, 733–744. [DOI] [PubMed] [Google Scholar]
- Deary IJ, Strand S, Smith P, & Fernandes C (2007). Intelligence and educational achievement. Intelligence, 35, 13–21. [Google Scholar]
- Derogatis LR, & Melisaratos N (1983). The brief symptom inventory: An introductory report. Psychological Medicine, 13, 595–605. [PubMed] [Google Scholar]
- Domitrovich CE, Gest SD, Gill S, Bierman KL, Welsh JA, & Jones D (2009). Fostering high-quality teaching with an enriched curriculum and professional development support: The head start REDI program. American Educational Research Journal, 46, 567–597. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dunn LM, & Dunn LM (1997). Examiner’s manual for the PPVT-III peabody picture vocabulary test: Form IIIA and Form IIIB. Circle Pines, MN: AGS. [Google Scholar]
- Flora DB, & Curran PJ (2004). An empirical evaluation of alternative methods of estimation for confirmatory factor analysis with ordinal data. Psychological Methods, 9, 466–491. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Forbes MK, Rapee RM, & Krueger RF (2019). Opportunities for the prevention of mental disorders by reducing general psychopathology in early childhood. Behaviour Research and Therapy, 119, 103411. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Fox NA, Almas AN, Degnan KA, Nelson CA, & Zeanah CH (2011). The effects of severe psychosocial deprivation and foster care intervention on cognitive development at 8 years of age: Findings from the Bucharest Early Intervention Project. Journal of Child Psychology and Psychiatry, 52, 919–928. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Green JG, McLaughlin KA, Berglund PA, Gruber MJ, Sampson NA, Zaslavsky AM, & Kessler RC (2010). Childhood adversities and adult psychiatric disorders in the national comorbidity survey replication I: Associations with first onset of DSM-IV disorders. Archives of General Psychiatry, 67, 113–123. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Helland WA, Lundervold AJ, Heimann M, & Posserud MB (2014). Stable associations between behavioral problems and language impairments across childhood – The importance of pragmatic language problems. Research in Developmental Disabilities, 35, 943–951. [DOI] [PubMed] [Google Scholar]
- Hooper D, Coughlan J, & Mullen M (2008). Structural equation modelling: Guidelines for determining model fit. Electronic Journal of Business Research Methods, 6, 53–60. [Google Scholar]
- Hu L, & Bentler PM (1999). Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. Structural Equation Modeling: A Multidisciplinary Journal, 6, 1–55. [Google Scholar]
- Keyes KM, Eaton NR, Krueger RF, McLaughlin KA, Wall MM, Grant BF, & Hasin DS (2012). Childhood maltreatment and the structure of common psychiatric disorders. The British Journal of Psychiatry, 200, 107–115. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kline RB (2015). Principles and practice of structural equation modeling. New York, NY: Guilford publications. [Google Scholar]
- Lambert HK, King KM, Monahan KC, & McLaughlin KA (2017). Differential associations of threat and deprivation with emotion regulation and cognitive control in adolescence. Development and Psychopathology, 29, 929–940. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Machlin L, Miller AB, Snyder J, McLaughlin KA, & Sheridan MA (2019). Differential associations of deprivation and threat with cognitive control and fear conditioning in early childhood. Frontiers in Behavioral Neuroscience, 13, 80. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLaughlin KA, Green JG, Gruber MJ, Sampson NA, Zaslavsky AM, & Kessler RC (2012). Childhood adversities and first onset of psychiatric disorders in a national sample of adolescents. Archives of General Psychiatry, 69, 1151–1160. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McLoyd VC (1998). Socioeconomic disadvantage and child development. The American Psychologist, 53, 185–204. [DOI] [PubMed] [Google Scholar]
- Mendelsohn AL, Mogilner LN, Dreyer BP, Forman JA, Weinstein SC, Broderick M, … & Napier C (2001). The impact of a clinic-based literacy intervention on language development in inner-city preschool children. Pediatrics, 107, 130–134. [DOI] [PubMed] [Google Scholar]
- Miller AB, Sheridan MA, Hanson JL, McLaughlin KA, Bates JE, Lansford JE, … & Dodge KA (2018). Dimensions of deprivation and threat, psychopathology, and potential mediators: A multi-year longitudinal analysis. Journal of Abnormal Psychology, 127, 160–170. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Muthén L, & Muthén B (2019). Mplus user’s guide (1998– 2019) (7th edn). Los Angeles, CA: Muthén & Muthén. [Google Scholar]
- Petersen IT, Bates JE, D’Onofrio BM, Coyne CA, Lansford JE, Dodge KA, … & Van Hulle CA (2013). Language ability predicts the development of behavior problems in children. Journal of Abnormal Psychology, 122, 542–557. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Preacher KJ, & Hayes AF (2008). Asymptotic and resampling strategies for assessing and comparing indirect effects in multiple mediator models. Behavior Research Methods, 40, 879–891. [DOI] [PubMed] [Google Scholar]
- Radloff LS (1977). The CES-D scale: A self-report depression scale for research in the general population. Applied Psychological Measurement, 1, 385–401. [Google Scholar]
- Reichman NE, Teitler JO, Garfinkel I, & McLanahan SS (2001). Fragile Families: Sample and design. Children and Youth Services Review, 23, 303–326. [Google Scholar]
- Salmon K, O’Kearney R, Reese E, & Fortune C-A (2016). The role of language skill in child psychopathology: Implications for intervention in the early years. Clinical Child and Family Psychology Review, 19, 352–367. [DOI] [PubMed] [Google Scholar]
- Schroeder A, Slopen N, & Mittal M (2020). Accumulation, timing, and duration of early childhood adversity and behavior problems at age 9. Journal of Clinical Child & Adolescent Psychology, 49, 36–49. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheridan MA, & McLaughlin KA (2014). Dimensions of early experience and neural development: Deprivation and threat. Trends in Cognitive Sciences, 18, 580–585. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Sheridan MA, & McLaughlin KA (2016). Neurobiological models of the impact of adversity on education. Current Opinion in Behavioral Sciences, 10, 108–113. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Straus MA (1979). Measuring intrafamily conflict and violence: The conflict tactics (CT) scales. Journal of Marriage and Family, 41, 75–88. [Google Scholar]
- Verboom CE, Sijtsema JJ, Verhulst FC, Penninx BW, & Ormel J (2014). Longitudinal associations between depressive problems, academic performance, and social functioning in adolescent boys and girls. Developmental Psychology, 50, 247. [DOI] [PubMed] [Google Scholar]
- Wolf S, & Suntheimer NM (2019). A dimensional risk approach to assessing early adversity in a national sample. Journal of Applied Developmental Psychology, 62, 270–281. [Google Scholar]
- Woodcock R, Mcgrew K, & Murray N (2001). Woodcock-Johnson® III assessment battery. Rolling Meadows, IL: Riverside Publishing Company. [Google Scholar]
- Yew SGK, & O’Kearney R (2013). Emotional and behavioural outcomes later in childhood and adolescence for children with specific language impairments: Meta-analyses of controlled prospective studies. Journal of Child Psychology and Psychiatry, and Allied Disciplines, 54, 516–524. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.