

Abstract
Female athletes are at a greater risk for anterior cruciate ligament (ACL) injuries than males. Current training programs for ACL injury reduction focus on muscle strengthening, appropriate movement patterns, and balance training. However, there is limited research on effective strategies to teach youth female soccer athletes how to properly perform desired movements associated with a decreased risk of ACL injuries. Behavioral skills training (BST) programs have been shown to be effective in teaching a wide variety of skills, but research on applications to sports is limited. This study evaluated a BST package for teaching a stepwise agility program to 3 youth female soccer athletes that consisted of verbal instructions, modeling, rehearsal, and feedback, which included video replay. Results showed a significant improvement in the number of steps the participants performed correctly relative to baseline, as well as maintenance of skills at follow-up. Implications for coaches and athletes, as well as limitations and directions for future research, are discussed.
Keywords: BST, Soccer athletes, Sports performance, Video feedback
Soccer is currently the most played sport in the world and has grown in popularity in the United States (Dai, Mao, Garrett, & Yu, 2014; Malliou, Gioftsidou, Pafis, Beneka, & Godolias, 2004; Wong & Hong, 2005). Although it is generally perceived as a male-dominated sport (Jeanes, 2011; Rutkowska & Bergier, 2015; Soroka & Bergier, 2011), current trends suggest that the continued rise in participation can be primarily attributed to the increasing interest in the sport from females (Kiani, Hellquist, Ahlqvist, Gedeborg, Michaëlson, & Byberg, 2010; Le Gall, Carling, & Reilly, 2008; Soroka & Bergier, 2011).
Given this increased participation of female athletes, researchers and pediatricians have reported concerns regarding the high frequency of soccer-related injuries in females (Smith, Chounthirath, & Xiang, 2016). Studies show that female soccer athletes experience the majority of their injuries in the knee, ankle, and thigh areas (Le Gall et al., 2008) and that females are treated for ankle and knee injuries at a higher rate than males (Smith et al., 2016). Of these lower extremity injuries, injury to the anterior cruciate ligament (ACL) is one of the most common and also the most serious (Kiani et al., 2010; Lohmander, Englund, Dahl, & Roos, 2007). The ACL is dense connective tissue that serves as one of the four major ligaments within the knee joint. With an injured or torn ACL, athletes whose sport requires quick, rapid side movements such as cutting, shuffling, and sidestepping are unable to continue to fully participate in their sport (Gammons & Schwartz, 2016).
Injury to the ACL is a specific concern in female soccer athletes because (a) female soccer athletes are about two to three times more likely to experience ACL injuries in comparison to their male counterparts (Dai et al., 2014; Prodromos, Han, Rogowski, Joyce, & Shi, 2008; Walden, Haggland, Werner, & Ekstrand, 2011), (b) female soccer athletes’ risk of noncontact injury is four to six times greater than males (Arendt, Agel, & Dick, 1999; Morgan, Johnson, Bovbjerg, & Norcross, 2018), and (c) the short-term and long-term consequences associated with ACL injuries can potentially be very costly. Gianotti, Marshall, Hume, and Bunt (2009) suggested that female athletes in late adolescence are at greatest risk for ACL injuries, as the incidences of ACL injury in youth female soccer athletes increase between the ages of 10 and 12 (Thompson et al., 2017). In addition, about 70% of ACL injuries in female soccer players occur as noncontact incidences, with no external contact made to the knee joint (e.g., ball to knee, player to player, knee to goalpost or ground; Gianotti et al., 2009; Granan, Bahr, Steindal, Furnes, & Engerbresten, 2008), making this a risk that is potentially modifiable (Morgan et al., 2018; Sigward, Cesar, & Havens, 2015). As more extensive research is conducted regarding noncontact ACL injuries in females, researchers are realizing that there is not one major contributing factor to injuries to the ACL (Hewett, Myer, & Ford, 2006; Thompson et al., 2017).
The injury risk that is associated with the ACL is considered multifactorial, consisting of anatomical, hormonal, neuromuscular, and biomechanical factors (Hewett et al., 2006; Thompson et al., 2017). Although anatomical and hormonal factors are basically impossible to change behaviorally, neuromuscular and biomechanical factors are modifiable and can have the greatest potential for injury reduction strategies that provide a significant decrease in ACL injuries to be implemented. The most common injury scenarios that occur prior to a noncontact ACL injury involve changing direction or cutting maneuvers in combination with deceleration (Boden, Sheehan, Torg, & Hewett, 2010; Faude, Junge, Kindermann, & Dvorak, 2005), landing from a jump in or near full leg extension, and pivoting with the knee near full extension and a planted foot (Boden et al., 2010; Fauno & Wulff, 2006). Increasing the likelihood of the proper execution of change-of-direction movements can be developed by focusing on technical and tactical skill development among youth female soccer athletes (Bailey & Collins, 2013; Lagestad, Aether, & Ulvik, 2017).
For almost four decades, the application of behavioral principles has been researched in the sports arena. The effectiveness of behavioral procedures such as public postings, goal setting, self-recording, video modeling, and behavioral coaching has been empirically demonstrated in several studies (e.g., Stokes, Luiselli, Reed, & Flemming, 2010; see Luiselli, Woods, & Reed, 2011, for a review). Of particular relevance to sports performance are behavioral training procedures. Behavioral skills training (BST) has emerged as an effective method for teaching a variety of skills, including child safety skills, graphing skills to graduate students, job interviewing skills, assessment techniques, and tackling skills (e.g., Barker, Moore, Olmi, & Rowsey, 2019; Himle & Wright, 2014; Miltenberger, 2008; Shayne & Miltenberger, 2013; Stocco, Thompson, Hart, & Soriano, 2017; Tai & Miltenberger, 2017).
BST can be described as an empirically supported training protocol consisting of instruction, modeling, rehearsal, and feedback. The instruction component of BST involves providing a description of the desired target skill that the individual is expected to perform. The modeling component entails demonstrating to the individual how to perform the target skill. Lastly, the rehearsal and feedback components give the individual the opportunity to practice the skill to criterion while receiving feedback on performance (Miltenberger, 2003).
Due to the well-documented effectiveness and generality of BST, a growing body of research has explored the effects of using BST to increase sports performance. For example, Tai and Miltenberger (2017) examined the effects of BST on the acquisition of safe tackling skills in football players. The researchers created a task analysis specifying the appropriate steps involved in their definition of a safe tackle. Following the implementation of BST, participants increased the number of correct steps performed for each tackle. The results of this study provide support for BST as an effective method for teaching safe tackling skills and are consistent with previous research on BST as a teaching method for skill acquisition.
More recently, Quintero et al. (2019) used BST to teach a heading technique to youth soccer players to minimize the risk of head injuries. In this study, three participants were provided instructions on a 14-step task analysis of the technique and had the opportunity to observe the modeled steps, rehearse with a foam soccer ball, and receive feedback on their performance. Their results showed improved performance relative to baseline levels, as well as maintenance of the acquired skills over time. To our knowledge, this is the only published study examining the effects of BST on the improvement of technique by soccer players to reduce the risk of sports-related injuries.
To extend the findings on evidence-based strategies designed to teach soccer skills accurately and safely, we examined the effects of BST on three female soccer athletes’ performance of movement patterns in an agility soccer drill. This study aimed to determine whether a BST package increased the accuracy of youth female soccer athletes performing a specific zigzag movement pattern. Because female athletes have a greater tendency than males to engage in risky movement patterns during exercises in cutting and changing direction (Thompson et al., 2017), identifying procedures that will teach female athletes to better execute these skills safely is critical to reduce the risk of ACL injuries.
Method
Participants and Setting
Three youth female soccer athletes from an organized, competitive soccer league in the mid-southern United States participated in the study. Participants were selected based on meeting age and gender requirements and being able to participate in the study during the summer. Shelby, 12 years old, was in her seventh season of playing competitive soccer as a defensive midfielder. Allison was 13 years old and in her sixth season of playing competitive soccer with a primary position as an attacking center midfielder. Miranda was 12 years old and in her fourth season of playing competitive soccer with a primary position as an outside back. Miranda and Shelby both reported that they had participated in specialized speed training but had not focused on movement training. Allison reported that she had no current or previous experience with any type of specialized training. None of the participants reported having previous experience with performing the zigzag agility drill. All sessions were conducted on a soccer field.
Target Behavior and Data Collection
The dependent variable for this study was the number of steps that the participants performed correctly during a zigzag drill. An eight-step task analysis was used to score the participants’ performance. During the drill, field cones were placed in a zigzag pattern and equidistant from each other. The participant moved from one cone to the next, practicing a series of movements throughout the entire drill. This particular zigzag pattern was chosen to mimic movement patterns utilized by soccer athletes. The zigzag drill is a training tool used to improve body positioning when engaging in change-of-direction movements (Hewett, Stroupe, Nance, & Noyes, 1996).
The field cones were used as markers to indicate where the participant was supposed to run toward and initiate the cutting movement to change direction before sprinting to the next cone. Figure 1 illustrates the position of the cones in the zigzag drill. A GoPro HERO6 camera was used to record the sessions, and video was imported into Coach’s Eye (TechSmith Corporation, 2019), a video analysis app. This app allowed the researcher to provide feedback to the participant through video playback that could be slowed down, spotlighted to highlight important details, and drawn on using lines to emphasize technique. Each session consisted of the participant performing the zigzag drill from start to finish. The researcher used the task analysis to score whether the participant performed the series of movements within the drill accurately.
Fig. 1.
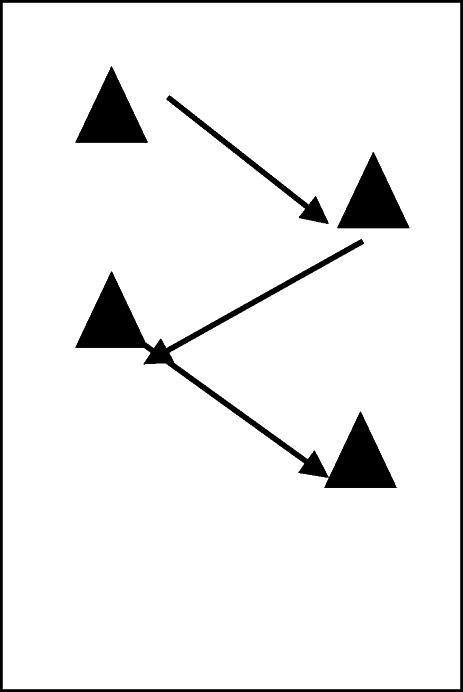
A pictorial representation of the zigzag pattern utilized in the research study
Interobserver Agreement
Interobserver agreement (IOA) was scored for 35% of sessions across all phases (baseline, intervention, and generalization) by two independent observers. The first observer was a doctoral student with previous soccer experience, and the second observer was a current collegiate soccer athlete. IOA was calculated by dividing the number of agreements for each step in the task analysis by the total number of steps in the task analysis and multiplying by 100%. If both observers scored a step as either correct or incorrect, the researchers counted it as an agreement. The mean IOA for all participants was 81.3% (range 75%–100%) in baseline, 88% (range 75%–100%) during the intervention phase, and 88% (range 75%–100%) in generalization.
Materials
The materials used in this research study included a GoPro HERO6 video camera, four orange field cones, a measuring tape, Coach’s Eye (a video analysis app), an iPad mini, and a video tripod. All participants performed the drill in athletic apparel and soccer cleats during all sessions of the study.
Research Design and Procedures
A multiple-baseline design across participants was used to evaluate the effectiveness of BST with video feedback. At the beginning of each phase of the study, the soccer field was set up using four orange field cones in a zigzag pattern. Each field cone was 6 m away from the next cone, totaling 18 m from start to finish of the zigzag. All the procedures were implemented by the first author.
Baseline
During baseline, the participants performed the zigzag drill, moving from one field cone to the next in sequential order. The researcher verbally instructed each participant to run from one cone to the next as coaches typically do during a prepractice warm-up. No specific details about how participants were expected to complete the drill were provided. Each participant performed the drill without other participants present. If participants arrived early, they were instructed to stand in a designated area where they were unable to view the participant performing the drill. All baseline sessions were conducted in 1 day.
BST
The BST components that were used to teach each step of the zigzag drill included (a) instruction, (b) modeling by the researcher, (c) rehearsal by the participant, and (d) feedback via video analysis. The intervention was implemented in a staggered manner across the participants. During the instruction phase, the researcher provided participants with verbal instructions as to how to perform each of the eight steps in the zigzag drill task analysis. The steps included in the task analysis are shown in Table 1. The task analysis describes the appropriate technique to move from the first cone through the third. The fourth cone was utilized to ensure that the participants continued with fluid movement and did not engage in a stopping motion prematurely at the third cone. After the researcher modeled each of the steps, the participant was given the opportunity to rehearse the drill. Feedback included the researcher viewing the video with the participant, providing verbal praise for the steps that were performed correctly, and providing corrective feedback for the steps that the participant performed incorrectly. After completing each BST session, participants were asked to perform the drill. Training continued after a 2-min break if the participant performed two or more steps incorrectly. Three training and probe sessions were conducted daily with each participant.
Table 1.
Task Analysis of the Zigzag Drill
| Steps in Sequential Order | |
|
1. Sprint from the first cone to the second cone. 2. Shuffle feet to decelerate (slow down). 3. Plant outside foot at the cone. (The foot is flat when planting, and the athlete’s heel and ball of the foot should remain in contact with the ground.) 4. Keep nose aligned to belly button. (The athlete’s body position should not be leaning to either side when the foot is planted.) 5. Keep knees stable. (Knee position should be straight, and neither knee should be positioned inward when planted.) 6. Point lead (inside) foot in direction of the next cone. (The left foot should be pointed toward the next cone in front of the participant.) 7. Stay low to the ground. (The athlete is bent at the knees when planting.) 8. Sprint to the next cone. |
Assessment of generalization
Prior to the study, all participants mentioned that noise and movement from other teams were frequent interferences during practice sessions. Practice sessions typically involved having to share the field with up to four teams (approximately 44 players and 5–8 adult coaches), each team practicing within 5 ft (1.52 m) from the others on both sides of the practice space. The generalization settings represented some of these distractions and challenges.
Two generalization phases probed participants’ performance on the drill when BST was withdrawn and while being presented with distractors. The participants were not provided with any specific instructions, modeling of the desired skill, rehearsal of skill, or verbal and video feedback. In the first generalization phase, participants performed the agility drill in the presence of visible distractors (absence of BST plus indirect distractors). A group of younger children was playing a small-side game near the participant. In the second generalization phase, participants were required to interact with a soccer ball thrown toward their practice space (absence of BST plus direct distractor). Each of these generalization phases is described next.
Absence of BST plus indirect distractors
In this phase, the researcher set up a smaller soccer game consisting of four boys playing two versus two about 8 to 10 ft (2.43 to 3 m) from where the participants were performing the drill. This scenario was designed to gauge the success of the participant while adding in a distractor that frequently occurred during regular practice sessions.
Absence of BST plus direct distractor
In this phase, a soccer ball was kicked with precision between the first and the second cones of the zigzag drill. This required participants to perform a change of direction at the first cone and, while en route to the second cone, pick their heads up to receive the ball at their feet. The participants anticipated having to change direction at the first cone but did not know at what point between the first and the next cone they would have to trap the ball.
Maintenance
In maintenance, the participants performed the zigzag drill 3 weeks after the intervention had been completed. During the 3-week break, there were no instructions provided to continue working on the drill or to complete a certain number of repetitions. The participants performed the drill in the absence of BST and video feedback and were only given the directions provided in baseline. The maintenance phase served as a return to baseline to gauge whether the skill set maintained with the same level of accuracy or reverted back to preintervention levels.
Results
The results of this study showed that BST was effective in increasing the number of steps correctly performed in the zigzag drill. All three participants showed improved accuracy in performing the steps when the BST package was implemented. Figure 2 shows the percentage of steps correctly performed by Miranda, Allison, and Shelby across all conditions of the study. During baseline, the mean percentage of steps performed correctly was 42% (range 37.5%–50%) for Shelby, 54% (range 50%–62.5%) for Allison, and 28% (range 0%–37.5%) for Miranda. After the implementation of BST, Shelby increased her mean average of 42% in baseline to 72.5% (range 50%–100%). Allison’s mean average of 54% in baseline increased to 86% (range 87.5%–100%), and Miranda increased her mean average of 28% in baseline to 74% (range 62.5%–87.5%).
Fig. 2.

Percentage of steps performed correctly by each participant during baseline, intervention, generalization, and maintenance
After BST, generalization was evaluated in two phases. First, participants were instructed to perform the drill while other individuals not in the study were playing soccer on the field immediately to the right of the drill. In the second generalization phase, the participants were instructed to change direction at whatever step they were performing in the drill to chase a ball that was kicked toward a space within the field cones. During the first phase, Shelby performed the steps of the drill with 100% accuracy, Allison performed the steps of the drill with 75% accuracy, and Miranda performed the steps of the drill with 87.5% accuracy. In the second phase, Shelby performed the steps of the drill with 100% accuracy, Allison performed the steps of the drill with 87.5% accuracy, and Miranda performed the steps of the drill with 100% accuracy.
Maintenance probes were conducted 3 weeks after baseline and intervention. During maintenance, Shelby performed the drill with a mean average of 75% (range 62.5%–87.5%), Allison performed the drill with a mean average of 100%, and Miranda performed the drill with a mean average of 87.5% (range 75%–100%).
A six-item survey, using a 5-point Likert scale (1 = strongly disagree, 5 = strongly agree; Tai & Miltenberger, 2017) was e-mailed to the participants and their parents at the end of the study to assess the social validity of the study (see Table 2). All three participants reported that BST improved their cutting movements. Participants also reported that watching their performance on video helped them improve their performance on the drills. In addition, all parents agreed on the importance of BST as a tool that coaches could use as a part of their soccer programs, and they would recommend it to other parents.
Table 2.
Social Validity Survey Responses From Parents and Participants
| Respondents | Statement | Mean Rating |
|---|---|---|
| Participants | Overall, I feel BST improved my cutting skills. | 4.6 |
| I feel it is important to learn to improve cutting movements when playing soccer. | 4.3 | |
| I feel I am able to perform cutting movements more safely. | 4.3 | |
| I am confident in my ability to complete cutting movements correctly. | 4.6 | |
| I feel like watching myself on video and being provided feedback helped me the next time I performed the movements. | 4.6 | |
| I enjoyed the BST I received. | 4.3 | |
| Parents | Overall, I feel BST improved my child’s cutting movements. | 4.3 |
| I feel it is important that my child learns proper cutting movements. | 5.0 | |
| I feel my child will be able to utilize what she learned in the study on the field. | 4.3 | |
| I think coaches should implement BST as part of their soccer programs. | 4.6 | |
| I believe the use of video recording as a tool for feedback was helpful. | 4.6 | |
| I would recommend BST to other parents. | 4.6 |
Discussion
The high prevalence of soccer-related injuries in the United States (Quintero et al., 2019; Smith et al., 2016) and the high incidences of young female soccer players sustaining an ACL injury (Dai et al., 2014; Gianotti et al., 2009; Thompson et al., 2017; Walden et al., 2011) reveal a need for the development and implementation of injury prevention strategies in these players’ training routines. Some of the movements that are associated with a high risk of ACL injury are changing direction rapidly while running and other cutting and deceleration maneuvers (Boden et al., 2010), all of which are frequently practiced by all players on the field.
The present study explored the use of video feedback during BST to improve athletes’ technique while performing a zigzag soccer drill. As in the study by Quintero et al. (2019), the present study shows that when BST was implemented, a significant increase in the number of correctly performed steps of the zigzag drill was observed across all three participants. This increment remained above baseline levels throughout the intervention phase and during generalization and maintenance probes.
During the intervention, Allison and Miranda performed the drill at 87.5% accuracy, which corresponds to performing seven of the eight steps of the agility drill correctly. Both participants failed to perform Step 5 correctly (keep knees stable) due to recurrences of knee valgus. Because knee valgus often requires the strengthening of muscles and whole-body technique modification, it is particularly difficult to correct (Dempsey, Lloyd, Elliott, Steele, & Munro, 2009). It is likely that due to continued practice, Allison mastered the skill in maintenance, and Miranda in generalization. Focusing on practicing only Step 5 to accuracy before resuming practice of the whole drill may have facilitated mastery during the intervention.
Although the use of video feedback to improve athletes’ performance has been demonstrated in sports such as gymnastics (Boyer, Miltenberger, Batsche, & Fogel, 2009) capoeira (BenitezSantiago & Miltenberger, 2016), and yoga (Downs, Miltenberger, Biedronski, & Witherspoon, 2015), to our knowledge this is the first study to evaluate BST in soccer with female athletes, using video as an added feature to the feedback component of BST. This study extends the recent findings of Quintero et al. (2019) by demonstrating the effectiveness and practicality of using video feedback in the feedback component of BST and by assessing generalization of skills to practice-like situations. Two generalization probes were designed to mimic some of the distractors encountered during a typical practice. During these probes, Shelby performed the steps with 100% accuracy when other athletes were playing nearby, and Shelby and Miranda performed the steps with 100% accuracy when the drill also involved having to receive a ball thrown in their direction.
In sum, this study suggests that BST with video feedback is an effective method of teaching soccer athletes to correctly perform the movements involved in a zigzag drill. The findings of this study add to the recent research on the use of BST to reduce sports-related injuries in soccer players (Quintero et al., 2019), suggest the effectiveness of using video feedback as part of BST, and demonstrate generalization of the acquired skills to practice-like situations. Additionally, participants and parents rated the intervention highly (between 4.3 and 5 on a 5-point Likert scale) in terms of their satisfaction with procedures and outcomes. They considered video to be a helpful resource and suggested that BST should be implemented by coaches in soccer programs. Although an average of 88% IOA for all three participants was obtained during intervention and generalization, higher scores could have been obtained if data collectors had used the video recordings to collect IOA data. Observers’ drift could be prevented by evaluating the accuracy of the descriptions provided for each of the steps of the task analysis.
The results obtained in this study should be considered in light of some limitations. One limitation of this study was that, although generalization probes mimicked practice situations, they did not assess performance of the skills during a soccer game. Arguably, however, practice and game situations may share similar challenges and require a similar set of skills. For example, the first generalization phase may be similar to a soccer game in which the player is required to cut and maneuver in an attempt to get open or provide support on the weak side of the field. The second phase may resemble a game situation in which a player is required to make quick movements in anticipation of receiving a ball either to the feet or played into open space.
However, several differences between practice and game situations should be noted. For example, during practice sessions, athletes performed drills in a much smaller area. During the first generalization phase, participants performed the drill in an area of 18 m2 and focused on the zigzag drill only. By contrast, soccer games are played on fields from 90 to 120 m long and 45 to 90 m wide, and players are often required to focus on several situations at one time. In addition, during a game, athletes do not necessarily know when they will have to change direction, how quickly they will have to complete the movement, and what other movements they will have to perform once they have changed direction. Future research could evaluate generalization of the skill to game situations.
Another limitation of the study is that although the results suggest that the use of video feedback was a helpful resource to integrate into a BST program, the contribution of the video feedback component to the overall effectiveness of BST cannot be determined. It would be interesting to investigate if higher accuracy or less time to reach mastery criteria is observed when BST is implemented with and without video feedback. In addition, because research has documented the effectiveness of video feedback alone in sports performance, researchers could also consider comparing increments in athletes’ performances after using video feedback alone, BST, and BST with video feedback.
Future research could also investigate the effectiveness of this intervention when implemented entirely by previously trained coaches. In the current study, the intervention was implemented by one of the authors, who is an athlete with expertise in health promotion, physiology, and kinesiology. To date, the coaching licensure system for youth soccer coaches focuses mainly on technical aspects of striking the ball (e.g., passing, shooting) and on psychological components such as motivation, winning versus losing, decreasing burnout, and managing parental expectations. In addition, because the majority of youth soccer coaches are volunteers with varying levels of training and experience, most of them lack expertise in the biomechanics of proper running technique. Recognizing the importance of injury prevention during running drills and using BST with video feedback to teach proper technique may significantly lower the risk of injury. Research studies demonstrating a reduction in the number of ACL injuries in female athletes after BST plus video feedback training are required to further support the findings of this study. Coaching communities and athletes could benefit significantly from the use of these procedures in their regular practice.
As one of the few applications of BST to soccer training, this study supports the effectiveness of a model that could be used by coaches and parents to assist athletes in skill acquisition of movement technique that may minimize the risk of ACL injuries. More generally, it contributes to the growing literature and research on applications of behavior-analytic principles and interventions to sports performance, health, and fitness.
Compliance with Ethical Standards
Conflict of interest
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or nonfinancial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this article.
Footnotes
Research Highlights
• This study shows an effective implementation of behavioral skills training (BST) with video feedback to teach a soccer agility technique.
• The study extends recent findings on an effective implementation of BST in soccer training by adding video feedback and evaluating generalization.
• This study provides a training strategy that could be easily incorporated into soccer training programs to reduce the risk of knee injuries such as those to the anterior cruciate ligament.
• The study shows the effective application of behavior-analytic principles to the field of sports performance and fitness.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Arendt, A., Agel, J., & Dick, R. (1999). Anterior cruciate ligament injury patterns among collegiate men and women. Journal of Athletic Training, 34, 86–92. [PMC free article] [PubMed]
- Bailey, R., & Collins, D. (2013). The standard model of talent development and its discontent. Human Kinetics, 2, 248–259. 10.1123/KRJ.2.4.248.
- Barker, L. K., Moore, J. W., Olmi, D. J., & Rowsey, K. (2019). A comparison of immediate and post-session feedback with behavioral skills training to improve interview skills in college students. Journal of Organizational Behavior Management, 39, 145–163. 10.1080/01608061.2019.1632240.
- BenitezSantiago, A., & Miltenberger, R. G. (2016). Using video feedback to improve martial arts performance. Behavioral Interventions, 31, 12–27. 10.1002/bin.1424.
- Boden, B., Sheehan, F., Torg, J., & Hewett, T. (2010). Non-contact ACL injuries: Mechanisms and risk factors. Journal of American Academy of Orthopedic Surgeon, 18(9), 520–527. [DOI] [PMC free article] [PubMed]
- Boyer, E., Miltenberger, R. G., Batsche, C., & Fogel, V. (2009). Video modeling by experts with video feedback to enhance gymnastics skills. Journal of Applied Behavior Analysis, 42, 855–860. 10.1901/jaba.2009.42-855. [DOI] [PMC free article] [PubMed]
- Dai, B., Mao, B., Garrett, W., & Yu, B. (2014). Anterior cruciate ligament injuries in soccer loading mechanisms, risk factors, and prevention programs. Journal of Sport and Health Science, 3(4), 299–306. 10.1016/j.jshs.2014.06.002.
- Dempsey, A. R., Lloyd, D. G., Elliott, B. C., Steele, J. R., & Munro, B. J. (2009). Changing side-step cutting technique reduces knee valgus loading. American Journal of Sports Medicine, 37(11), 2194–2200. 10.1177/0363546509334373. [DOI] [PubMed]
- Downs, H. E., Miltenberger, R., Biedronski, J., & Witherspoon, L. (2015). The effects of video-self-evaluation on skill acquisition with yoga postures. Journal of Applied Behavior Analysis, 48, 930–935. 10.1002/jaba.248. [DOI] [PubMed]
- Faude, O., Junge, A., Kindermann, W., & Dvorak, J. (2005). Injuries in female soccer players: A prospective study in the German national league. American Journal of Sports Medicine, 33, 1694–1700. 10.1177/0363546505275011. [DOI] [PubMed]
- Faunø, P., & Wulff, J. B. (2006). Mechanism of anterior cruciate ligament injuries in soccer. International Journal of Sports Medicine, 27(1), 75–79. 10.1055/s-2005-837485. [DOI] [PubMed]
- Gammons, M., & Schwartz, E. (2016). Anterior cruciate ligament injury. Retrieved on September 30, 2018, from www.medscape.com.
- Gianotti, S., Marshall, S., Hume, P., & Bunt, L. (2009). Incidence of anterior cruciate ligament injury and other knee ligament injuries: A national population-based study. Journal of Science and Medicine in Sport, 12(6), 622–627. 10.1016/j.jsams.2008.07.005. [DOI] [PubMed]
- Granan, L., Bahr, R., Steindal, K., Furnes, O., & Engebresten, L. (2008). Development of a national cruciate ligament surgery registry: The Norwegian National Knee Ligament Registry. American Journal of Sports Medicine, 36(2), 308–315. 10.1177/0363546507308939. [DOI] [PubMed]
- Hewett, T. E., Myer, G. D., & Ford, K. R. (2006). Anterior cruciate ligament injuries in female athletes, Part 1: Mechanisms and risk factors. American Journal of Sports Medicine, 34(2), 299–311. 10.1177/0363546505284183. [DOI] [PubMed]
- Hewett, T. E., Stroupe, A. L., Nance, T. A., & Noyes, F. R. (1996). Plyometric training in female athletes decreased impact forces and increased hamstring torques. The American Journal of Sports Medicine, 24 765–773. 10.1177/036354659602400611. [DOI] [PubMed]
- Himle, M., & Wright, K. (2014). Behavioral skills training to improve installation and use of child passenger safety restraints. Journal of Applied Behavior Analysis, 47, 549–599. 10.1002/jaba.143. [DOI] [PubMed]
- Jeanes, R. (2011). “I’m into high heels and make up but I still love football”: Exploring gender identity and football participation with preadolescent girls. Soccer & Society, 12, 402–420. 10.1080/14660970.2011.568107.
- Kiani, A., Hellquist, E., Ahlqvist, K., Gedeborg, R., Michaëlson, K., & Byberg, L. (2010). Prevention of soccer-related knee injuries in teenage girls. Archives of Internal Medicine, 170(1), 43–49. 10.1001/archinternmed.2009.289. [DOI] [PubMed]
- Lagestad, P., Aether, S., & Ulvik, A. (2017). Differences in coaching feedback between coaches of junior elite soccer players and junior amateur soccer players. Journal of Physical Education and Sport, 3, 2049–2058. 10.7752/jpes.2017.03207.
- Le Gall, F., Carling, C., & Reilly, T. (2008). Injuries in young elite female soccer players: An 8-season prospective study. American Journal of Sports Medicine, 36(2), 276–284. 10.1177/0363546507307866. [DOI] [PubMed]
- Lohmander, L., Englund, P., Dahl, L., & Roos, E. (2007). The long-term consequence of anterior cruciate ligament and meniscus injuries: Osteoarthritis. American Journal of Sports Medicine, 35(10), 1756–1759. 10.1177/0363546507307396. [DOI] [PubMed]
- Luiselli, J. K., Woods, K. E., & Reed, D. D. (2011). Review of sports performance research with youth, collegiate and elite athletes. Journal of Applied Behavior Analysis, 44, 999–1002. 10.1901/jaba.2011.44-999. [DOI] [PMC free article] [PubMed]
- Malliou, P., Gioftsidou, A., Pafis, G., Beneka, A., & Godolias, G. (2004). Proprioceptive training reduces lower extremity injuries in young soccer players. Journal of Back and Musculo-skeletal Rehabilitation, 17(3), 101–104. 10.3233/BMR-2004-173-403.
- Miltenberger, R. G. (2003). Behavior modification: Principles and procedures. Belmont, CA: Wadsworth.
- Miltenberger, R. G. (2008). Behavior modification: Principles and procedures (4th ed.). Pacific Grove, CA: Thomson/Wadsworth.
- Morgan, E., Johnson, S., Bovbjerg, V., & Norcross, M. (2018). Associations between player age club soccer coaches’ perceptions of injury risk and lower extremity injury prevention program use. International Journal of Sports Science & Coaching, 13, 122–128. 10.1177/1747954117707480.
- Prodromos, C. C., Han, Y., Rogowski, J., Joyce, B., & Shi, K. (2008). A meta-analysis of the incidence of anterior cruciate ligament tears as a function of gender, sport, and a knee injury–reduction regimen. Arthroscopy: The Journal of Arthroscopic & Related Surgery, 23(12), 1320–1325. 10.1016/j.arthro.2007.07.003. [DOI] [PubMed]
- Quintero, L. M., Moore, J. W., Garrett Yeager, M., Rowsey, K., Joe Olmi, D., Britton Slater, J., et al. (2019). Reducing risk of head injury in youth soccer: An extension of behavioral skills training for heading. Journal of Applied Behavior Analysis, 53(1), 237–248. 10.1002/jaba.557. [DOI] [PubMed]
- Rutkowska, K., & Bergier, J. (2015). Psychological gender and emotional intelligence in youth female soccer players. Journal of Human Kinetics, 47, 285–291. 10.1515/hukin-2015-0084. [DOI] [PMC free article] [PubMed]
- Shayne, R., & Miltenberger, R. (2013). Evaluation of behavioral skills training for teaching assessment and treatment selection skills to parents. Behavioral Interventions, 28(1), 4–21. 10.1002/bin.1350.
- Sigward, S. M., Cesar, G. M., & Havens, K. L. (2015). Predictors of frontal plane knee moments during side-step cutting to 45o and 110o in men and women: Implications for ACL injury. Clinical Journal of Sport Medicine, 25(6), 529–534. 10.1097/JSM.0000000000000155. [DOI] [PMC free article] [PubMed]
- Smith, N., Chounthirath, T., & Xiang, H. (2016). Soccer-related injuries treated in emergency departments: 1990–2014. Pediatrics, 138(4), 1–9. 10.1542/peds.2016-0346. [DOI] [PubMed]
- Soroka, A., & Bergier, J. (2011). Sense of gender identity in women practicing football with consideration of the formation. Polish Journal of Sport and Tourism, 18, 45–58. 10.2478/v10197-011-0004-8.
- Stocco, C., Thompson, R., Hart, J., & Soriano, H. (2017). Improving the interview skills of college students using behavioral skills training. Journal of Applied Behavior Analysis, 50, 495–510. 10.1002/jaba.385. [DOI] [PubMed]
- Stokes, J. V., Luiselli, J. K., Reed, D. D., & Flemming, R. K. (2010). Behavioral coaching to improve offensive line pass-blocking skills of high school football athletes. Journal of Applied Behavior Analysis, 43, 463–472. 10.1901/jaba.2010.43-463. [DOI] [PMC free article] [PubMed]
- Tai, A., & Miltenberger, R. (2017). Evaluating behavioral skills training to teach safe tackling skills to youth football players. Journal of Applied Behavior Analysis, 50, 849–855. 10.1002/jaba.412. [DOI] [PubMed]
- TechSmith Corporation (2019). Coach’s Eye. Retrieved from https://www.coachseye.com/.
- Thompson, J., Tran, A., Gatewood, C., Schultz, R., Slider, A., Delp, S., & Dragoo, J. (2017). Biomechanical effects of an injury prevention program in preadolescent female soccer athletes. American Journal of Sports Medicine, 45, 294–301. 10.1177/0363546516669326. [DOI] [PMC free article] [PubMed]
- Walden, M., Haggland, M., Werner, J., & Ekstrand, J. (2011). The epidemiology of anterior cruciate ligament injury in football (soccer): A review of the literature from a gender-related perspective. Knee Surgery, Sports Traumatology, and Arthroscopy, 19(1), 3–10. 10.1007/s00167-010-1172-7. [DOI] [PubMed]
- Wong, P., & Hong, Y. (2005). Soccer injury in the lower extremities. British Journal of Sports Medicine, 39(8), 473–482. 10.1136/bjsm.2004.015511. [DOI] [PMC free article] [PubMed]