

Abstract
There is a need for inexpensive and reliable means to determine the modulation of cutaneous inflammation. The method outlined in this article draws together a number of scientific techniques and makes use of generally unwanted biological tissues as a means of determining skin inflammation ex vivo, and focuses on probing aspects of the arachidonic acid inflammation pathway. Freshly excised skin contains elevated levels of short-lived inducible cyclooxygenase-2 (COX-2) and, under viable conditions, COX-2 and its eicosanoid products will continue to be produced until tissue necrosis, providing a window of time in which relative levels can be probed to determine exacerbation due to an upregulating factor or downregulation due the presence of an agent exerting anti-inflammatory activity. Ex vivo porcine skin, mounted in Franz diffusion cells, is dosed topically with the xenobiotic challenge and then techniques such as Western blotting and immunohistochemistry can then be used to probe relative COX-2 levels on a semi-quantitative or qualitative level. Enzyme-linked immunosorbent assay or LCMS can be used to determine relative prostaglandin E-2 (PGE-2) levels. Thus far, the technique has been used to examine the effects of topically applied anti-inflammatories (betamethasone, ibuprofen, ketoprofen and methotrexate), natural products (fish oil, Devil’s claw extract and pomegranate rind extract) and drug delivery vehicle (polyNIPAM nanogels). Topically applied xenobiotics that modulate factors such as COX-2 and PGE-2 must penetrate the intact skin, and this provides direct evidence of overcoming the "barrier function" of the stratum corneum in order to target the viable epidermis in sufficient levels to be able to elicit such effects. This system has particular potential as a pre-clinical screening tool for those working on the development of topical delivery systems, and has the additional advantage of being in line with 3 Rs philosophy.
Keywords: skin, inflammation, COX-2, PGE2, ex vivo
INTRODUCTION
Skin and inflammation
Covering most of the body, the epidermis comprises a structured epithelium with five histologically distinct regions. With a turnaround time of approximately 4 weeks, keratinocytes of the epidermis basal layer undergo progressive transformations culminating in the formation of the outermost layer, the stratum corneum, before being shed from the surface via desquamation. The stratum corneum is a dense, non-viable tissue some 15 microns in thickness, in which the cells are fully differentiated and known as corneocytes. The purpose of this layer is to provide a “barrier function” by presenting a largely impenetrable, rate-limiting obstacle to the ingress of xenobiotics, ultraviolet (UV) radiation and microbes, whilst also limiting the egress of water and electrolytes [1]. The viable epidermis, in particular the basal layer, is highly metabolically active and expresses many phase I non-CYP and phase II enzymes [2] which respond to a range of stimuli such as trauma and xenobiotic or UV radiation ingress, and often results in activation of the arachidonic acid (AA) inflammation pathway, described later. The viable epidermis is also host to dendritic Langerhans cells that reside in the suprabasal layers of the epidermis in close contact with keratinocytes and help to prevent infections.
Inflammatory skin diseases are the most common problem encountered by dermatologists, ranging from superficial rashes to chronic conditions such as dermatitis (eczema), contact dermatitis, rosacea and psoriasis. Acute inflammation can result from exposure to UV irradiation, ionizing radiation, allergens, or to contact with chemical irritants, and is typically resolved within 1 to 2 weeks with little accompanying tissue destruction. Chronic inflammation results from prolonged immune cell mediated inflammatory response within the skin, and are long lasting with potential to cause serious tissue destruction, and are products of interplay between complex regulatory networks [3]. In the dermis, dendritic myeloid cells are involved in the pathogenesis of immune system related inflammatory disorders such as psoriasis by producing pro-inflammatory cytokines such as interleukins [4].
Mechanisms of skin inflammation
The process of skin inflammation is complex and is still not completely understood, and it can be triggered by a stimulus, a chemical irritant (e.g., xenobiotic) or allergens. Skin inflammation can also be associated with autoimmune conditions and can spread to skin from the main inflammation focus such as a joint affected by rheumatoid arthritis, or in the reverse direction as is the case with psoriatic arthritic. A further important stimulus in skin inflammation is UV radiation and cultured human keratinocytes irradiated with UVB showed a 6-fold increase in cyclooxygenase-2 (COX-2) that was evident at 6 h and peaked 24 h after irradiation [5]. Each of these causes the cells in the skin produce a variety of cytokines and chemokines that bind to specific receptors on target cells and stimulate the production of additional inflammatory signalling factors. Some of these cause vasodilation, resulting in familiar skin erythema and activation of nerve cells, causing pain. The two major inflammatory mediators involved in skin disorders are tumor necrosis factor (TNF)-α and prostaglandin E2 (PGE-2). While TNF-α plays a key role in immune system-based inflammation processes such as psoriasis, PGE-2 is a major factor in all types of skin inflammation, and many other tissues [6].
The cyclooxygenases (also known as prostaglandin-endoperoxide synthases) is a family of three known enzymes. COX-1 is expressed constitutively, i.e., it is produced by a cell under all types of physiological condition, predominating in the kidney, stomach and platelets. COX-3 is a relatively recent discovery and is not believed to be of interest in humans. The main analytical target in the current article is COX-2 which is an inducible enzyme that is the product of an “immediate-early” gene and is generally expressed only in cells where prostaglandins are upregulated, e.g., during trauma or inflammation—it is unexpressed under normal conditions, but elevated levels are found during episodes of trauma, irritancy and inflammation [7,8]. In the skin, COX-2 is expressed predominantly in suprabasal keratinocytes [5].
Regardless of subtype, the primary function of COX is to catalyze the production of eicosanoids from polyunsaturated fatty acid AA, which is stored in the phospholipids of bodily cells and is liberated from cell membranes upon demand, when COX converts it to prostaglandin G2 and prostaglandin H2. PGH2 is converted by prostaglandin E2 synthase into the potent inflammatory mediator PGE-2. COX-2 also converts AA to 15-hydroxyicosatetraenoic acids (15-HETE). Conversion of AA to is a two-step process [9]. Firstly, hydrogen is abstracted from C13 of AA, and two atoms of oxygen are added by the COX-2, giving PGG2. Secondly, PGG2 is reduced to PGH2 in the peroxidase active site. PGH2 is subsequently converted to prostaglandins (PGD2, PGE2, PGF2α), prostacyclin (PGI2), or thromboxane A2 by tissue-specific isomerases.
Crucially, in relation to the methodology that is the focus of this article, COX-2 has a short lifespan of 1–2 min at Vmax and becomes permanently inactivated after converting several hundred AA molecules [10]. As inflammatory mediators such as COX-2 have such short half-lives, constant stimulation is needed to maintain inflammation. In this way, any unnecessary inflammation is kept to a minimum. Conversely, once the injury is repaired, or other stimulus has been removed, the inflammatory cells begin to return to normal status. Similarly, levels of COX-2 production will diminish if an anti-inflammatory agent is present in sufficient quantity such that it can block the enzyme or interfere with another part of the AA inflammatory pathway upstream or downstream of COX, or the tissue loses viability. Over-expression of COX-2 and its product PGE-2 has been implicated in the aetiology of other disease states, such as restricted airflow in chronic obstructive pulmonary disease, COPD [11] and degenerative brain diseases [12]. The expression of COX-2 is known to be upregulated in many cancers, with high levels of PGE-2 implicated in breast [13] and skin cancer [5,14].
Drug therapy for skin inflammatory conditions
Therapeutic drugs to treat skin conditions can be administered either via the systemic circulation by injection or oral dose, or by local or topical delivery using a cream or gel formulation. The most commonly-used prescription drugs for treating skin inflammation arising from the cellular immune system include corticosteroids which are effective for eczema, including atopic dermatitis, allergic contact dermatitis, seborrheic dermatitis and psoriasis. However, first-line treatments tend to involve non-steroidal anti-inflammatory drugs (NSAIDs)—these possess analgesic, antipyretic and anti-inflammatory properties which inhibit prostaglandin production by blockade of cyclooxygenase active sites. Drugs aimed at treating skin inflammation (anti-inflammatories) are administered either systemically or topically—each with advantages and disadvantages. Oral systemic administration results in a very small amount of drug reaching the target inflamed skin, with the remainder interacting with other parts of the body unnecessarily—also, for profen-type NSAIDs, there are recognized risks of gastrointestinal upset and even heart failure [15]. The selective COX-2 inhibitors (Coxibs) have been associated with adverse effects [16]. Local administration, typically via cream or gel formulations, requires lower doses and involves minimal systemic absorption, but the drug must overcome the skin barrier function (except where the skin is already compromised, e.g., psoriasis).
A large variety of products is available for treating skin inflammation, both on prescription and over the counter, including hydrocortisone, betamethasone in addition to NSAID products such as Ibuleve (ibuprofen), Feldene (piroxicam) and Voltaren (diclofenac); the latter also indicated for relieving subcutaneous musculoskeletal pain. The delivery of anti-inflammatory drugs into and across remains a highly active research area, indicative of a continued clinical need for more efficacious products and methods by which to evaluate them. There are consequently many articles in the literature concerned with the dermal or transdermal delivery of anti-inflammatories [17], which are often used to test novel topical drug delivery systems, such as nanoparticles [18]. Typically these involve comparative drug transport by obtaining kinetic parameters, where data are often rationalized using Fickian laws or algorithms [19], or depth profiling whereby adhesive tape is used to sequentially strip skin layers which are then analyzed for drug content [20]. However, determining the mass transport across or mass localization within the skin alone does provide direct information relating to biological activity. Topically applied compounds that are observed to modulate COX-2 expression, either anti-inflammatory or pro-inflammatory, must ipso facto penetrate the skin in sufficient levels and penetrate viable cells allowing sufficient interaction with the inflammation factors, such as inhibiting COX-2.
Overall, new products aimed at relieving (skin) inflammation hence pain management are still needed. On the other hand, it is equally important to determine the toxicological potential or risk of topically applied compounds that are capable of inducing skin inflammation (pro-inflammatories). There is thus a need for robust, accurate methods for determining modulation of skin inflammation by xenobiotics that have successfully penetrated the barrier function of the stratum corneum. Furthermore, in the modern era new methods would be expected not involve the use live animals, broadly in line with 3 Rs goals [21].
Current models of determining skin inflammation modulation
In vivo human trials are clearly the most reliable means of determining the effect of topically applied xenobiotics, however due to the enormous costs they are used only to evaluate final products. Live animal experimentation is consequently commonplace and numerous approaches have been used. In the TPA-induced mouse ear oedema technique the potent tumor promoter 12-O-tetradecanoylphorbol-13-acetate (TPA), derived from croton oil, which oedema and swelling when applied to the ears of mice. TPA applied topically on mouse ear skin induces vascular permeability, increases formation of leukotrienes and prostaglandins, increases the influx of neutrophil and macrophages, and induces proinflammatory cytokines, including TNF-α, interleukin (IL)-1β and IL-6 [22,23]. The blockade of upstream kinase IκBα kinase signaling by the natural phenolics tannic acid and protocatechuic acid, inhibited the enzyme level and the activity of COX-2 [24]. Ear punch biopsies are taken from the TPA treated mouse ears to measure weight changes [25,26]. Carrageenan-induced rat paw oedema model uses an irritant polysaccharide extracted from seaweed, which induces inflammation, vasodilatation and increases vascular permeability [27]. Anti-inflammatory activity of the topically applied xenobiotic is assessed by measuring their ability to reduce or prevent local inflammation caused by carrageenan injected into the paw of rats. Rat paw oedema can be quantified by a number of approaches [28].
As the major cytokine-releasing cells in the viable epidermis, the study of inflammation in keratinocytes has been detailed in numerous papers. In resting keratinocytes, immune mediators are at very low levels, however, under stimulatory conditions keratinocytes express cytokines, chemokines and accessory molecules, which transmit signals to cells of innate and adaptive immunity. Dysregulation and abnormal expression of inflammatory mediators in keratinocytes are implicated in the pathogenesis of chronic inflammatory skin diseases [29]. Cultured human keratinocytes were used to determine the effect UVB irradiation on COX-2 [5]. Keratinocytes have been widely used to model xenobiotic action in skin, for example the modulation of keratinocyte COX-2 expression was used in determining the anti-inflammatory effects of novel drugs, such as dithranol derivatives [30]. HaCaT cell line is a spontaneously immortalized, human keratinocyte which is widely used for skin biology studies, including inflammation such as cytokines IL-6, IL-8, IL-10 [31]. However, HaCaT cells were shown to produce 100-fold less PGE-2 than normal human epidermal keratinocytes, supporting the hypothesis that COX-2 activity was reduced as a result of immortalization [32]. Also, such a purely in vitro system is clearly incapable of responding in proportion to drug challenges arising from topically applied doses.
Much research has led to the development of tissue engineered reconstructed skin. Commercially available systems generally comprise a reconstituted organotypic culture of human keratinocytes forming a multilayer differentiated epidermis on a collagen matrix. The European Union Reference Laboratory for Alternatives to Animal Testing (ECVAM) introduced validated test tests for acute irritation potential from exposure to acutely irritant substances contained in various products using EpiSkin, EpiDerm SIT, Modified Epiderm and SkinEthic models (ECVAM). Studies on the activity of pro-inflammatory cytokines such as interleukins have been reported [33-36]. However, we were unable to locate literature reports on the use of these materials for determination of modulation of the AA inflammation pathway, the key target of topically delivered NSAIDs. A proteomic profile of the xenobiotic metabolizing enzymes in native human skin was compared with data obtained from a number of in vitro models of human skin, with considerable variability being shown [32]. Although such materials could be used to study skin inflammation, these tissues lack a recognizable fully differentiated stratum corneum, complete with appendages, as is found in vivo, and are therefore unlikely to accurately reflect inflammation modulation as a function of skin penetration. Furthermore, skin appendages (pilosebaceous units and sweat pores) are recognized as important “shunt routes” in the delivery of drugs into and across the skin [1], and can influence the timescale over which xenobiotics penetrate the skin and modulate inflammation [37].
Porcine ear skin as a model for human skin
Porcine (pig) skin has been used extensively in recent years as a model for human skin in topical penetration and permeation experiments. The driving force for this is largely due to the ethical and regulatory hurdles involved with using excised human skin. Other factors include its general availability and the sizeable areas of tissue available—workers sometimes use mouse or rat skin, where the available area of tissue is limited, for example the area of the dorsal surface of a pig ears versus the dorsal side of a mouse. Porcine organs are generally very similar to human skin and this has led to considerable research into xenotransplantation. The validity of the porcine skin model is supported in numerous published articles where it has been favorably compared to human skin in terms of: xenobiotic permeability [38-40], architecture [41-43], biology [44] and immunology [45,46]. Of the regions of porcine skin, the dorsal side of the ear is considered to be most similar to human skin and up to 15 Franz diffusion cells (FDCs) can be set up using skin from a single pig ear. However, variations in histology have been reported in porcine skin [47], a fact which must be borne in mind when interpreting data.
COX-2 and PGE-2 determination in ex vivo skin
Freshly excised porcine skin is metabolically active and contains elevated levels of the COX-2 due to the trauma of preparation and this is observed universally in our laboratory. If viable conditions are maintained COX-2 will continue to be produced until the inducing stimulus is removed or an anti-inflammatory agent is present. An ex vivo scenario can be described as one in which tissue is maintained in a state of viability once excised from the animal. The determination of relative COX-2 levels has been used in ex vivo tissue to determine anti-inflammatory, and in some cases pro-inflammatory, effects of a range of topically applied compounds. In a typical experiment, described shortly, a skin explant is mounted in a Franz diffusion cell and COX-2 modulation is then probed in the skin after an appropriate incubation period. The following is a typical experimental procedure.
MATERIALS
A convenient experimental set-up involves the FDC—a simple two-compartment device comprised of a donor compartment and receptor compartment that allow the determination of xenobiotic transport from the donor phase (in contact with the stratum corneum) into the skin or through it skin to the receptor phase [48]. FDCs are available in different forms—those used in the author’s laboratories have a nominal diffusional area of 1 cm diameter (0.88 cm2) and receptor phase volume of 3 ml (Fig. 1).
Figure 1.
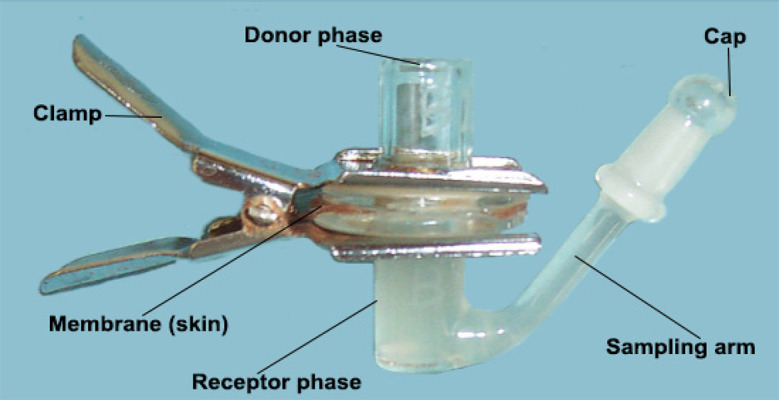
All-glass Franz diffusion cell, comprised of an upper donor phase and lower receptor phase. The skin membrane is positioned stratum corneum uppermost, between the 2 flanges and clamped together; the receptor phase filled with Hanks buffer and the skin dosed with the test substance.
Freshly excised porcine ears must be collected as soon as possible after slaughter. To facilitate the longevity of skin viability, the tissue is immersed in iced Hanks buffer, during transportation to the laboratory; in the author’s laboratory this is typically achieved within 1 h. As the animal has already undergone humane slaughtering, no ethical considerations apply regarding further procedures. However, the animals arriving at the abattoir have not been reared under laboratory conditions. Hence, there is a great deal of variation in the quality and cleanliness of the ear tissue, and one should only use unscarred, relatively clean material. Further gentle cleansing under running water is usually sufficient. In terms of breed, the “large white” are the most common and it is easier to spot defects and indeed to visualize stained COX-2 relative to other breeds that may have high melanin content and therefore obscure visualization. Also, it is of immense importance to stress here that the ears must be removed from the pig prior to undergoing sanitation, often by steam cleaning—a process which strips away the entire epidermis, clearly rendering the tissue unsuitable for experimentation.
Hanks buffer balanced salt or DMEM. Molecular biology reagents for example kits for analyzing COX-2 and prostaglandin; reagents necessary to perform immunohistochemical (IHC) and Western blot analysis, as detailed later. In typical transdermal delivery experiments, the choice of receptor phase is normally dictated by the need to provide “sink” conditions for the permeant drug, otherwise artificially high levels of drug can accumulate in the skin tissue. However, in an ex vivo scenario the receptor phase must also fulfill a further critical function—one of maintaining skin viability. Hanks balanced salt solution has been proven to maintain skin viability and is typically used in our laboratory and by other workers [49]. For polar permeants, Hanks buffer alone is sufficient. However, Hanks buffer must be altered in order to provide a sink for lipophilic permeants. An “organic modifier” such as alcohol such as methanol and ethanol should be avoided for compromising tissue viability; some success was obtained using DMSO. However, the most effective modifier we have found is the quaternary ammonium surfactant cetrimide, which is miscible with Hanks buffer and at levels of 30% does not compromise skin viability [50,51].
PROCEDURE
Ex vivo skin preparation
Once in the laboratory, the ears are cleansed under running water, hairs trimmed and the skin (typically the dorsal side only for consistency) liberated from the underlying cartilage by blunt dissection using a scalpel, whilst being continually bathed in Hanks buffer. Some papers use epidermal membranes liberated from full thickness skin by heat separation—however, the process deactivates skin metabolism, and so such tissue is not appropriate for use in this protocol. Skin sheets may then be further cut into 2 cm2 sections, carefully excluding areas containing scars and defects, and then used immediately.
Topical delivery
The ex vivo skin sample is mounted stratum corneum-uppermost, between the lightly pre-greased flanges and clamped into position—the purpose of the grease is to prevent leakage of liquid donor and receptor solutions, and should be used very sparingly. A micro-stirrer bar is added to the receptor compartment to assist mixing after placing on a stirrer plate, filled with degassed receptor phase, and the sampling arm capped. The complete cells are placed on a multiple stirrer plate in a thermostatically controlled water bath set at 37°C which generally provides a skin surface temperature of 32°C. After an equilibration period of typically 15 min, the donor phase is then dosed with the test xenobiotic—this can be in the form a solution or a formulation such as a cream, gel or even section of a transdermal patch. “Finite” doses are intended to simulate an in-use dosing regimen (e.g., a fixed, representative amount of formulation to be applied per area of skin, e.g., 20 mg/cm2) but, even after repeat-doses, this may not demonstrate that delivery to the viable epidermis has been achieved (i.e., < limit of detection of the assay). For maximal effect “infinite” doses, typically 1 ml, may be applied which is in sufficiently high concentration to show demonstration and achievement 0-order transport kinetics. To determine transdermal delivery parameters such as steady state flux and lag time, samples are taken from the receptor phase and analyzed for penetrant [48]. However, receptor phases may also be collected and used to re-apply apply to ex vivo skin to indicate that the levels of permeated compounds are able to exert an anti-inflammatory effect in deeper tissues [37,52]. At predetermined times, that should reflect an in-use situation, the FDC is dismantled and the skin membranes recovered. Excess formulation is carefully removed before the immediate commencement of biological analysis. At this stage, quantitative skin penetration data may be obtained using the tape stripping technique [20,37,48], whereby adhesive discs or tape is repeatedly applied to and removed from the area of drug application and the amount of drug then quantified; this is useful for determining the amount of drug localized at different stratigraphic/histological layers within the skin. Summating these amounts provides an estimation of drug reservoir (per unit area). Naturally, such work will involve different skin samples as tape stripping; for example, tape stripping is known to be a pro-inflammatory process, causing a transient increase in skin COX-2 mRNA [53]. Koppes et al. used in vivo tape stripping followed by the analysis of 38 inflammatory mediators to probe topical therapy of dermatitis [54].
We have used “reverse-tape stripping” to provide more direct quantitation of xenobiotics successfully reaching and localizing within the viable epidermis—the technique is as above, but uses isolated epidermis and application of the first tape strip to the basal layer rather than stratum corneum.
Preparation of skin lysates
The first step in the process is the preparation of skin lysates in order to release the protein content including COX-2 [53]—this must be carried out very promptly to minimize further metabolic change. To prepare the skin lysates, the diffusional area of application from the FDC is excised by blunt dissection using a scalpel, cut into small pieces and added to 1 ml radioimmunoprecipitation lysis buffer. Additional protease inhibitors are added immediately prior to maceration using a probe homogeniser 1 min. Crude lysates are incubated for 15 min on ice then pelleted by centrifugation at 1400 g for 2 × 15 min at 4°C, and the supernatant stored at –20°C. Inflammatory mediators can then be probed, and two main techniques have been used—these are well known techniques and so only a brief synopsis is given.
Western blotting analysis of COX-2
Western blotting (WB) is a well-established analytical tool for protein identification and quantitation, with methods that are well described in the literature [5,55,56]. The protocol used, including the major steps of protein estimation and denaturation, polyacrylamide gel electrophoresis, transfer, blocking, detection/probing using primary antibody and secondary antibody/reporter conjugate can be found in Abdelouahab Ouitas and Heard [52] and Abu Samah and Heard [57]. Finally, results are visualized and relative COX-2 levels determined following densitometric scanning, which can be used on a purely qualitative basis. For semi quantitative data (i.e., COX-2 levels relative to a control), the Western blot band intensities are normalized against a ubiquitous protein, typically β-actin [58], which is run simultaneously and arbitrarily set to 100%. Each experiment should be performed in ≥ triplicate for each sample and the result expressed as the mean ± SD.
Analysis of inflammatory prostaglandin E2 levels
Skin extracts such as the lysates prepared in Section 8.3 may also be analyzed for COX-2 product prostaglandin, although analyzable samples may also be obtained more simply using a probe homogenizer. Enzyme immunosorbent assay (EIA) kits are commercially available, e.g., Cayman Chemical which involves and incubation: 18 h, development in 60–90 min and colorimetric determination at 405–420 nm; and has a range of 7.8–1000 pg/ml and sensitivity of 15 pg/ml. GCMS and LCMSMS are also used for such analyses.
Immunohistochemical analysis of COX-2 in ex vivo skin
To supplement the WB data the relative levels of COX-2 expression in skin may be visualized prior to lysing, allowing visual qualitative comparison of anti-inflammatory effects relative to an untreated control. IHC is already embedded as a major diagnostic tool in pathology for many markers [59], including COX-2 [60]. Unlike WB, the analysis of COX-2 is performed in situ rather than following liberation from the tissue, e.g., in punch biopsies [61]. The general methodology is explained in detail in the literature. However, it is worth stressing that effective preparation of the skin sample is critical to maintain cell morphology, tissue architecture, antigenicity and the level and location of target epitopes. Consequently, exacting tissue collection, fixation and sectioning protocols are essential.
PUBLISHED DATA USING THIS APPROACH
Background levels
Viable, but otherwise untreated ex vivo skin universally displays elevated levels of COX-2 and PGE-2, as evidenced in later sections by WB and intense IHC staining and is a response to combination of shutting down, ear excision and the preparation processes prior to use. The control tissue thus provides background levels of conveniently upregulated COX-2 and PGE-2 against which to compare test substances and formulations, via either pro-inflammatory action (where the levels increase post treatment) or, usually, anti-inflammatory (where the levels decrease post treatment). Background levels are determined in each experiment for internal consistency, and modulations due to treatment determined statistically, generally using one-way analysis of variance (ANOVA) followed by appropriate post-tests, using InStat for Macintosh, version 3.0 (GraphPad Software Inc, San Diego, CA).
Positive controls
Although the topical delivery and activity of anti-inflammatory activity is important in its own right, their inclusion in our work to date has largely been as validators, i.e., to serve as positive controls, as successful delivery to the viable epidermis should be reflected in lower levels of epidermal COX-2 relative to untreated skin. In the following examples, the level of activity was variable and this is due to numerous factors including: dosage form, concentration of drug, amount dosed and excipient effects - indeed optimization of such factors is pivotal in the development of new topical formulations.
Ibuprofen is a commonly used non-steroidal anti-inflammatory drug (NSAID) of the profen-type and is available as topically applied hydrogels (e.g., 5% Ibuprofen pain relief gel, 10% Ibugel Forte, Dermal Laboratories). More recently a cutaneous lotion has become available to treat minor sunburn (Soleve sunburn relief, Diomed Developments Limited), which contains 1% ibuprofen and claims to be clinically proven for relieving the pain and soreness of mild to moderate sunburn. Using the current model, solutions of ibuprofen have been used as positive control to determine the relative anti- and pro-inflammatory effects of H. procumbens (Devil’s claw) where WB analysis revealed that, following the dosing of 500 μM ibuprofen in PBS onto the skin for 6 h, COX-2 was reduced by ~50% [52,62].
Ketoprofen is another non-steroidal anti-inflammatory of the profen-type and is available as hydrogel (e.g., 2.5% Oruvail, Sanofi; ketoprofen 2.5% w/w gel, Pinewood Healthcare). Using the current model, 2.5% aqueous ketoprofen solution was used as a control for the anti-inflammatory effects of a formulation containing both ketoprofen and Ω-3 fatty acids in a two-pronged anti-inflammatory system. IHC analysis revealed that whereas ketoprofen exerted no effect upon LOX expression, a significant decrease on COX-2 expression was observed [63]. Naproxen, also a non-steroidal anti-inflammatory drug of the profen-type, was the focus of a novel topical drug delivery system involving activated nanogels, where is also served as a control when dosed as a simple solution. Compared to untreated ex vivo skin, Western blot analysis showed the naproxen solution elicited anti-inflammatory activity by the reduction of COX-2 to 88.6% after 6 h and 84% after 10 h post-application [64].
Betamethasone and betamethasone dipropionate, like most glucocorticoids, possess potent anti-inflammatory activities. However, the mechanism of action differs to profen-type NSAIDs and involves the synthesis of lipocortin-1 (annexin-1) which suppresses phospholipase A2, thereby blocking eicosanoid production. In the work of Zulfakar et al., another 2-pronged anti-inflammatory system was investigated based upon a combination of betamethasone dipropionate and omega-3 fatty acids [50]. A dose of 0.5 g of an ointment containing 0.1% w/w betamethasone dipropionate (plus 3% salicylic acid intended to model Diprosalic ointment) was applied to ex vivo porcine skin. IHC analysis revealed a reduction in the intensity of COX-2 staining after 6 h and analysis by enzyme-linked immunosorbent assay (ELISA) analysis further revealed the level of PGE-2 had decreased by 50%.
Fish oil and Ω-3 polyunsaturated fatty acids
Fish oil has been extensively researched due to the purported health benefits conferred by its constituent major Ω-3 fatty acids: eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). These are associated with anti-inflammatory activity, resulting from the formation of less potent eicosanoids compared to those derived from Ω-6 fatty acids, mainly AA [65,66]. Typical levels in fish oil are EPA (33%) and DHA (22%) and with sufficient bioavailability they can be incorporated into cell membranes from where it subsequently competes with AA in the inflammation cascade [67]. In addition to its anti-inflammatory activity, Ω-3 fatty acids can act as a skin permeation enhancer in formulations containing fish oil and NSAIDs, where the amount of NSAID and EPA from the fish oil delivered to the skin was increased compared to fish oil or NSAIDs alone [68,69].
In our laboratory, fish oil has generally been co-administered with an anti-inflammatory drug such as ketoprofen or betamethasone dipropionate with the aim of developing a two-pronged therapeutic to treat acute inflammation. Ketoprofen blocks synthesis of prostaglandins by COX-2, whilst high bioavailability of fish oil directs the remaining prostaglandin to more benign forms incorporating EPA and DHA. Similarly, betamethasone dipropionate reduces eicosanoid production by blocking phospholipase A2 production, and co-administered with fish oil again directs the remaining prostaglandin to more benign forms incorporating EPA and DHA.
Using the general approach outlined above the effect of topically applied fish oil and ketoprofen on cyclooxygenase (COX-2) and lipoxygenase (LOX) were determined within freshly excised porcine ear skin [63]. IHC data revealed that the fish oil formulation qualitatively inhibited the expression of both COX-2 and LOX enzymes. A formulation containing both fish oil and ketoprofen proved to be the most effective at inhibiting the expression of both COX-2 and LOX, further demonstrating that permeation of the fish oil enhanced the permeation of ketoprofen; enhancement behavior was attributed at least in part to π-π interactions [70].
The ex vivo porcine ear model was used to probe the influence of co-formulated fish oil on the topical delivery and anti-inflammatory properties of betamethasone dipropionate from ointment formulations [50]. The skin was probed by IHC for COX-2 and the tissue was also assayed for PGE-2 using a commercially available ELISA kit (Cayman Chemical, Ann Arbor, MI). Expression of COX-2 is known to decrease in response to the presence of glucocorticoids [7]. The data showed that whereas betamethasone and salicylic acid reduced COX-2 expression within the epidermis, greater reduction was observed when fish oil was included in the ointment, as indicated by reduced COX-2 expression. Modulation of PGE-2 production also supported the anti-inflammatory properties of fish oil, reducing PGE-2 levels that reflected the reduction by betamethasone dipropionate. However, combining fish oil with betamethasone dipropionate did not provide the anticipated synergistic effect i.e., no further COX-2 reduction was observed. Addition of fish oil also enhanced the anti-inflammatory activity of betamethasone dipropionate, attributed to increased amounts of the drug present in the skin and/or the intrinsic anti-inflammatory activity of fish oil (Fig. 2). Fish oil is a complex mixture of fatty acids as triacylglycerols and ethyl esters, in addition to other components, such as antioxidants. Some compounds have pro-inflammatory activity, such as AA [66]. Therefore, rather than propose that fish oil has anti-inflammatory activity, it is more accurate to say the anti-inflammatory compounds such as EPA and DHA counteract the presence of pro-inflammatory factors leading the downregulation of COX-2 as observed in the current model.
Figure 2.

The effects of topically applied betamethasone diproprionate and fish oil on porcine skin ex vivo. A. Immunohistochemical staining for the presence of COX-2 in ex vivo skin following 4 treatments at different time points at 40× magnification. Key: a1. control, a2. betamethasone dipropionate, a3. fish oil, a4. betamethasone dipropionate + fish oil, after 0 h; b1. untreated, b2. betamethasone dipropionate, b3. fish oil, b4. betamethasone dipropionate + fish oil after 6 h (n = 3 ± SEM). Note the very low staining when fish oil was combined with BD in a single formulation. B. Levels of PGE-2 in ex vivo skin. Key: 1. untreated control, 2. betamethasone dipropionate, 3. fish oil, and 4. betamethasone dipropionate + fish oil for 6 h (n = 3 ± SEM). Treatments 2–4 all significantly reduced PGE-2 in ex vivo skin relative to untreated skin P < 0.05 (one way ANOVA followed by Dunnett’s post hoc tests). Note: topically applied fish oil gave a similar result to topically applied steroid betamethasone dipropionate, although a combination provided no further reduction.
Devil’s claw (Harpagophytum procumbens) extract
Devil’s claw is the common name for the prepared tuber of the southern African plant, H. procumbens (L.) and for centuries it has been used as a folklore treatment for a variety of inflammatory disorders [71]. As a natural product, its extracts contain a wide array of chemical compounds, although its major phytochemical components, harpagoside, harpagide, 8-coumaroylharpagide and verbascoside were believed to be responsible for its anti-inflammatory effects.
Using the methods described above, an ethanol-soluble extract of H. procumbens tubers and two of the pure compounds tested showed reductions in COX-2 in WB and IHC analysis, with harpagoside and 8-coumaroylharpagide exhibiting greater reductions in COX-2 expression than verbascoside [62]. Dosing with ibuprofen led to a 40% decrease in COX-2 (Fig. 3).
Figure 3.

Effects of the components of Devils claw (H. procumbens) ethanolic extract on the expression of COX-2 in ex vivo porcine skin (n = 3 ± SD) where β-actin was used as the housekeeping protein. Key: 1. untreated control, 2. H. procumbens ethanolic extract, 3. admixture (harpagoside, 8-coumaroylharpagide, verbascoside), 4. admixture (harpagoside, harpagide, 8-coumaroylharpagide, verbascoside), 5. harpagoside (P < 0.05), 6. harpagide (P < 0.05), 7. 8-coumaroylharpagide (P < 0.05), 8. verbascoside (P < 0.05) and 9. ibuprofen (P < 0.05) (one way ANOVA followed by Dunnett’s post hoc comparisons). Note: anti-inflammatory activity of harpagoside, 8-coumaroylharpagide and verbascoside, but pro-inflammatory activity of harpagide.
It was surprising to discover that the compound harpagide in fact caused a significant increase in the levels of COX-2 expression above control levels after 6 h of topical application. The data therefore suggest that the efficacy of H. procumbens is dependent upon the ratios of the phytochemicals present, which is inconsistent with some current official monograph specifications based solely on harpagoside content. With this in mind, the relative efficacies of six commercial formulations of H. procumbens were evaluated [72]. Based upon the recommended dosages on the product label, the total daily amounts were determined and used to establish anti-/pro-inflammatory (A/P) factors; again the formulations were compared using ex vivo porcine skin for their activities towards COX-2 by WB. The results showed great variability in the phytochemical composition of the six formulations examined and this inconsistency correlated with relative COX-2 expression (Fig. 4). The conclusion was that although the data supported the beneficial anti-inflammatory effects from the use of some of the brands tested, others would appear potentially to exacerbate inflammation.
Figure 4.

Effects of the topical application of commercial Devil’s claw formulations 3–8 and positive control 2 on the expression of COX-2 in ex vivo porcine skin, where 1 is untreated control; β-actin was used as the housekeeping protein. A. Bar chart (n = 3 ± SD), where β-actin was used as the housekeeping protein. B. Western blots for COX-2 expression. One way ANOVA followed by Dunnett’s post hoc comparisons revealed only product 4 to be anti-inflammatory (P < 0.05), whereas products 6 and 8 were pro-inflammatory (P < 0.05). The identity of 3–8 can be found in Abdelouahab and Heard [72]. Note: the wide variations in pro- and anti-inflammatory activities of the six commercial Devil’s Claw (H. procumbens) products.
Pomegranate rind extract and punicalagin
Pomegranates are obtained from the fruit of the Punica granatum (L.) tree, and pomegranate rind extract (PRE) contains a high level of polyphenolics, in particular, tannins such as punicalagin. When co-administered with Zn (II) ions, pomegranate rind extract (PRE) has been found to be a potent microbicidal system [73], with potential as a new topical treatment for Herpes simplex virus (HSV) infections and inflamed perioral lesions. The anti-inflammatory activity of PRE total pomegranate tannins (TPT) and zinc (II) were studied from pH 4.5 phthalate buffer solutions using the ex vivo porcine skin model by assessing their effect on the expression of endogenous COX-2 by WB and IHC [19]. Results revealed that the application of PRE and PRE + ZnSO4 both led to the statistically significant (P > 0.01) reduction of COX-2 expression by 66.5 ± 3.6% and 64.5 ± 5.1%, respectively (Fig. 5A).
Figure 5.

The effects of topically applied pomegranate rind extract and zinc sulfate on porcine skin, ex vivo. A. Bar chart showing COX-2 expression by Western blotting after full thickness porcine skin was treated with topical ZnSO4 (1 M), pomegranate rind extract (PRE) (1 mg/ml), PRE (1 mg/ml) + ZnSO4 (1 M) and phthalate buffer as a control for 6 h, protein was extracted and 30 μg was loaded and separated via SDS-PAGE. The histogram represents COX-2 (72 kDa) levels normalized against β-actin (42 kDa). Note: significant anti-inflammatory activities of PRE, PRE + ZnSO4 and TPT (one way ANOVA followed by Dunnett’s post hoc analysis), indifferent effect of ZnSO4 and TFF. B. Western blots for COX-2 expression. C. Reverse tape stripping of porcine epidermis: punicalagin recovered after 24 h by reverse tape stripping three times epidermal membranes (where 1 is the basal layer) dosed with two formulations, F1 (left) and F2 (right) (mean ± SD, n = 4). Note: significantly higher levels of anti-inflammatory punicalagin in basal layer (one way ANOVA followed by Mann-Whitney U test).
The reduction of COX-2 by PRE was similar to that previously reported where COX-2 reduction of 79% was observed in colon cancer cells [74]. Using one-way ANOVA analysis, the application of ZnSO4 demonstrated no statistically significant effect on the level of COX-2 expression (P > 0.05), in line with data previously shown [75]. COX-2 was also downregulated following the application of an equal concentration of TPT but this level (40.5%) was significantly higher (reduced by only 26%) than the result obtained from PRE in the presence or absence of ZnSO4. A tannin-free PRE (i.e., PRE after tannins removed) failed to show any modulation of COX-2. The WB data were supplemented by IHC that followed the same trend. Therefore, reduction in COX-2 expression was determined to be greatest when PRE remained as a whole extract, with TPT (even with its high punicalagin content) exhibiting anti-inflammatory activity to a lesser extent. Olajide et al. reported the pre-treatment of rat primary microglia with punicalagin (5–40 μM) prior to LPS (10 ng/ml) stimulation which produced a significant (P < 0.05) inhibition of TNF-α, IL-6 and PGE-2 production; protein and mRNA expressions of COX-2 and microsomal prostaglandin E synthase 1 were also reduced by punicalagin pretreatment [76]. PRE and Zn (II) was subsequently formulated as hydrogels and then used to determine permeation across epithelial membranes prone to HSV infection [77]. When PRE/Zn (II) gels at two concentrations were applied to porcine epidermis, the gel with the higher loading showed higher permeation than the one with the lower loading. However, when the amount of punicalagin in the basal layer was determined by reverse tape stripping (whereby the basal layer is stripped first), the same amounts were found to have been delivered from each gel. COX-2 reduction was found to be 33% relative to the untreated control. This shows firstly, that the tissue was saturated with punicalagin using both formulations (Fig. 5B) and secondly, that the level of punicalagin delivered to the lower layers was sufficient to elicit an anti-inflammatory response A further novel approach was taken in that study whereby the receptor phase was collected at the end of the experiment and then used to dose ex vivo porcine skin in further diffusion cells. COX-2 expression was reduced by 64% relative to control after 6 h, confirming the delivery of anti-inflammatory levels across skin.
It is notable that the above data were achieved with intact stratum corneum, confirming skin penetration of punicalagin and Zn(II); however, the molecular weights of punicalagin and the Zn(II) ion are 1084 and 65 respectively, and are both differ markedly from the generally accepted optimum of ~400 [48,19]. Given the clear anti-inflammatory effects observed, appendageal delivery via shunt routes [78] may have been of significance here.
Nanoparticles
Nanotechnology remains a major growth area of research for new therapeutic systems including topical delivery. Stimulus-responsive nanogels, i.e., those that release drug depending on such parameters as temperature and pH, have potential as carriers for drugs targeting the skin. The current ex vivo porcine skin model has been used to examine potential anti- and pro-inflammatory effects associated with the topical application of these materials.
As such products are directly in contact with skin, and evidence has been published to show they can permeate across skin [79], it was important to determine the potential to induce irritation or inflammation. The ex vivo porcine ear model has been used to estimate the biocompatibility of polyN-isopropylacrylamide (polyNIPAM), poly(NIPAM copolymerized butyl acrylate) [poly(NIPAM-co-BA)], and poly(NIPAM copolymerized with 5% w/v acrylic acid) [poly(NIPAM-co-AAc)(5%)] nanogels [57]. WB of skin lysates for COX-2 expression demonstrated that the materials had penetrated the skin and interacted with keratinocytes of the viable epidermis. The poly(NIPAM-co-BA) nanogel was found to elicit a pro-inflammatory response when applied topically, as reflected by 67% higher COX-2 expression relative to the control treatment (Fig. 6A). The data obtained for the poly(NIPAM-co-AAc)(5%) nanogel, on the other hand, indicated no significant modulation in the expression of COX-2, suggesting the particles are compatible with skin (Fig. 6B). This was even the case in the presence of co-administered aqueous citric acid solution. Overall the data support the use of the multi-responsive poly(NIPAM-co-AAc)(5%) nanogel for triggered topical drug delivery applications. However, nanoparticles are often intended to be the vector for delivering a loaded drug to the target site. If the loaded drug is an anti-inflammatory it can compensate for any pro-inflammatory effects of the nanogel itself, such that the net effect in one of anti-inflammatory activity.
Figure 6.

The effects of topically applied nanogels on COX-2 expression in porcine skin, ex vivo. A. Western blotting analysis of COX-2 expression in full-thickness ex vivo porcine skin following topical treatment for 9 h (n = 3 ± SD). β-actin was used as the housekeeping protein. Key: 1. control (de-ionized water), 2. NIPAM monomer (1% w/v), 3. polyNIPAM, 4. poly(NIPAM-co-BA), 5. MTX (positive control). Note: pro-inflammatory response from topically applied poly(NIPAM-co-BA) nanogel (4), as reflected by 67% higher COX-2 expression relative to the control treatment (P < 0.05, one-way ANOVA with Tukey’s post hoc test). B. Western blots for COX-2 for (A). C. Western blotting analysis of COX-2 expression in full-thickness ex vivo porcine skin following topical treatment for 9 h (n = 3 ± SD). β-actin was used as the housekeeping protein. Key: a. control (de-ionized water), b. NIPAM monomer (1% w/v), c. AAc monomer (0.05% v/v), d. aqueous solution of CA (5% w/v), e. polyNIPAM, f. poly(NIPAM-co-AAc)(5%), g. poly(NIPAM-co-AAc)(5%) followed by CA solution, h. positive control (methotrexate). Note: generally better skin compatibility of blank nanoparticles based on poly(NIPAM-co-AAc)(5%) (P < 0.05, one-way ANOVA with Tukey’s post hoc test). D. Western blots for COX-2 for (C).
Methotrexate is a potent folate analogue that reduces the activity of the body’s immune system, which may be overactive in some conditions such as rheumatoid arthritis, psoriatic arthritis and vasculitis. Methotrexate is approved by the FDA to treat psoriasis, and it continues to be a first-line treatment for psoriatic arthritis where is it exerts indirect inhibition of COX-2 synthesis [80]. The ex vivo porcine skin model was used to demonstrate the improved dermal delivery of methotrexate utilizing activated nanogels based on co-polymerized polyNIPAM and butylacrylate [81]. In so doing, a novel mechanism was established whereby the change in temperature experienced by the nanogel as it penetrated skin induced de-swelling and expulsion of methotrexate in situ. Finite doses were applied to full-thickness porcine ear skin ex vivo, which was then treated with radioimmunoprecipitation buffer and probed for levels of PGE-2 using a commercial enzyme immunoassay kit. The added sodium carbonate led to further solubilization and MTX release, hence increasing the concentration gradient, flux and reducing PGE-2 production. The methotrexate-loaded nanogel, which demonstrated de-swelling by 7% over the range 25–37°C, provided a methotrexate flux of 1.4 ± 0.3 ng/cm2/h; this increased to 3.1 ± 0.22 ng/cm2/h upon the addition of saturated aqueous. PGE-2 levels for water (control) and sodium carbonate) were similar, but reduced by 33% when the methotrexate-loaded nanogel was applied, and by 57% when this was followed by the application of sodium carbonate (P < 0.01, ANOVA).
A similar responsive system was used to determine the modulation of skin COX-2 levels with polyNIPAM nanogels loaded with naproxen [64]. Nanogels were prepared under standard and acidic conditions using citric acid whereby the nanoparticles were in an expanded state allowing maximal expansion, prior to collapse and drug expulsion by addition of base. Following massaging into skin, the skin was probed (with and without base activation by sodium carbonate (or triethylamine) for depth penetration and transdermal delivery of drug, and anti-inflammatory activity in the relative levels of COX-2 expression (Fig. 7A). When activated by sodium carbonate, there was a particle size reduction of 19%. Tape stripping revealed significantly greater delivery of naproxen into the epidermis for the activated nanogel and the steady state flux was enhanced by a factor of 2.8. WB showed reduced COX-2 with base-activated nanogel was 50% lower than unactivated nanogel, and this trend was confirmed semi-quantitatively by immunostaining (Fig. 7B). Importantly, this work included an in vivo evaluation using the rat paw oedema test which further confirmed the increased activity of the activated nanogel in the reduction of rat paw swelling, providing ex vivo–in vivo correlation (Fig. 8).
Figure 7.

Effects of topically applied naproxen-loaded thermorespnsive nanogels on porcine skin, ex vivo. A. Representative Western blots for COX-2 expression following the dosing of porcine skin with naproxen-loaded PNIPAM nanogels after 6 and 10 h, relative to water control. β-actin was used as the housekeeping protein. The upper blots show COX-2 for each treatment where the intensity of the bands and is directly proportional to protein level. The lower blots show the β-actin control (n = 3 ± SD). Key: 1. control (untreated), 2. NNCA + TEA (naproxen nanogel + citric acid + triethylamine) at 6 h, 3. NNCA + TEA (naproxen nanogel + citric acid + triethylamine) at 10 h, 4. Naproxen solution at 10 h, 5. NNCA (naproxen nanogel + citric acid + sodium carbonate) at 6 h, 6. NNCA (naproxen nanogel + citric acid + sodium carbonate) at 10 h, 7. NNCA + SC (naproxen nanogel + sodium carbonate) at 6 h, 8. NNCA + SC (naproxen nanogel + sodium carbonate) at 10 h, 9. naproxen solution at 6 h. Note: significant anti-inflammatory active of naproxen-loaded nanogels, in particular from those involving the addition of sodium carbonate (one way ANOVA followed by Dunnett’s post hoc analysis). B. Western blots for COX-2 in ex vivo porcine skin. C. Representative immunostaining images for COX-2 in ex vivo porcine skin dosed with PNIPAM nanogels. Ex vivo porcine skin treated with: BN (blank nanogel) after 6 h (top left), BN (blank nanogel) after 10 h (bottom left), NNCA (naproxen nanogel + citric acid) after 6 h (top center), NNCA (naproxen nanogel with citric acid) after 10 h (bottom center), NNCA + SC (naproxen nanogel with citric acid, then sodium carbonate) after 6 h (top right), NNCA + SC (naproxen nanogel with citric acid, then sodium carbonate) after 10 h (bottom right). Note: high staining (high COX-2) in the blanks, lower staining (lower COX-2) when naproxen nanogel applied, much lower staining (much lower COX-2) following the application of sodium carbonate causing the greater release of naproxen in situ.
Figure 8.

Time course of carrageenan-induced oedema in the in vivo rat paw test following administration of PNIPAM nanogels. Results, expressed as % swelling determined at different times after injection of carrageenan in the left hind foot pad. Key: Green: naproxen solution control, Blue: blank nanogel control, Red: NNCA (naproxen nanogel with citric acid), Black: NNCA + SC (mean ± SD, n = 3). Note: lowest swelling when dosed with NNCA + SC (naproxen nanogel + citric acid, activated by sodium carbonate).
DISCUSSION
Generally, live animals are the mainstay of anti-inflammatory activity determinations, prior to testing in humans. Although relatively straightforward, such techniques incur significant costs due to husbandry and licensing. Furthermore, TPA and rat paw oedema tests undeniably cause pain and discomfort to the subject animals, which by convention would be sacrificed at the end of the procedures and are therefore are not aligned with the current drive for “3 Rs”—reduction, refinement and replacement [21]. The principle of the 3 Rs has become embedded in national and international legislation regulating the use of animals in scientific procedures. It may appear counter-intuitive that the use of excised porcine skin also does not fit with 3 Rs philosophy. However, porcine ears are generally unwanted byproducts of the food industry, in the UK at least, and involve animals that have already been slaughtered. Wider adoption of the general approach outlined in this article has potential significance in the Replacement and Reduction of in vivo experiments using live animals, for example in the development of further products intended for topical application.
Importantly for this protocol, the death of the pig in addition to the crude processing of the ear tissue renders the skin in a state of inflammation prior to experimentation. This is something observed in all our studies, and it provides a convenient platform against which to determine anti-inflammatory activity, bearing in mind that COX-2 and eicosanoids are constitutive and have very short half-lives. No prior treatment is required to induce inflammation, e.g., with TNF-α, to stimulate eicosanoid production, which in itself could subsequently modulate the delivery and efficacy of the test substance. The anti-inflammatory effects observed in the cases described above arise from modulation key events in the AA pathway [82]. Conversely, the application of pro-inflammatory compounds induces such events, for example as observed with harpagide [62]. As a constitutive enzyme, COX-2 is absent or in very low concentration in most normal tissues; however, it is induced at sites of inflammation by cytokines, growth factors and tumor promoters. Downregulation of eicosanoid production can be taken to mean that the permeant has docked within the active site of COX-2 and therefore inhibited the biosynthesis of further PGE-2, and therefore via negative feedback has resulted in less COX-2 being expressed, as COX-2 is strongly induced by pro-inflammatory challenges. However, the active site of COX-2 is well documented and blockade of the COX-2 active site is the MOA for NSAIDs such as the profens which have been designed to fit into this pocket. However, the literature contains reports of compounds that have a modulating effect on COX-2 inhibitors, although their chemistries cannot be rationalized in terms of active site pocket fitting. These include flavonoids [83,84] and pomegranate rind extract and the polyphenolic punicalagin [73]. These have potent antioxidant properties and can deactivate the free radicals generated in first stage of AA conversion by COX-2. As the function of COX-2 is to catalyze the production of eicosanoids, it is intuitive that a reduction in COX-2 should go hand in hand with reduction in PGE-2. However, in reality the situation is not so clear. Additionally, the bioavailability of Ω3 fatty acids (EPA, DHA) should be manifested in a reduction in the level of PGE-2. This was observed by Zulfakar et al., where the reduction of PGE-2 was rationalized in that the topical application of fish oil resulted in competition between the Ω-3 fatty acids and AA, producing a different series of prostaglandins which are less potent inflammatory mediators than its AA-derived counterparts [50]. The presence of more benign prostaglandins would feedback and cause downregulation of COX-2, which could further explain the reduction in PGE-2 levels.
Furthermore, although it had been generally accepted that the pharmacological action of NSAIDs is mediated by inhibiting the activity of COX [85], some drugs can have the effect, at least in part, of suppressing COX-2 gene transcription. First reported by Xu et al., the pharmacological action of salicylate could not be explained by its inhibition of cyclooxygenase activity, rather that salicylate exerts its anti-inflammatory action in part by suppressing COX-2 induction, thereby reducing the synthesis of pro-inflammatory prostaglandins [86]. Modulation of any of these processes will result in lower PGE-2 production and result in the downregulation of COX-2 via negative feedback. However, as noted in some of the above cases, application of some compounds to skin can exacerbate inflammation, as shown by the eliciting of the upregulation of COX-2 expression. This is evidenced by increased levels of COX-2 compared to control e.g., harpagide [62].
A further key attribute of the current protocol is that the very fact the penetrant molecules have achieved this modulation is direct evidence that it has successfully penetrated the skin, in particular the barrier function of the fully differentiated stratum corneum, in sufficient amounts to elicit such a response. In comparison with reconstructed epidermis models, in which the stratum corneum typically lacks normal structure, e.g., in terms of lipoidal domains and presence of appendages, the current model is superior in better mimicking an in vivo scenario. Furthermore, such models lack appendages, and sweat pores are found over the entire body with a density of 400 glands per cm2 and have the purpose of exuding sweat, an aqueous electrolyte solution. Given the clear anti-inflammatory effects with PRE such channels appear to provide a short-cut by allowing the permeants to bypass the barrier function of the stratum corneum which is primarily lipoidal in nature. This is sometimes referred to as a “shunt route” [78] and its effect can only be truly accounted for using natural skin.
Limitations of this protocol primarily relate to the fact that despite the use of buffers that support viability, the tissue tends to undergo necrosis between 24 and 48 h. The limited lifespan in ex vivo systems is a recognized limitation, and the model is not appropriate for studying modulation of cutaneous inflammation over prolonged timescales [87]. The lack of connectivity with other tissues is a potential issue with all ex vivo systems, for example the effect of changes in COX-2 and PGE-2 levels on regional blood flow (erythema) and pain cannot be determined. Also, the tissue is not available through a supplier, and has to be obtained directly from a cooperative abattoir, although laboratory-bred animals could be used equally effectively. A summary of the advantages and disadvantages of this and competing techniques is shown in Table 1.
Table 1.
Summary of the advantages and disadvantages of non-clinical techniques available to study cutaneus inflammation.
| Technique | Advantages | Disadvantages |
|---|---|---|
| Animal paw, in vivo |
|
|
| Cell culture |
|
|
| Human reconstructed tissue |
|
|
| Ex vivo porcine |
|
|
This protocol has focused upon the modulation of the AA/COX-2 inflammation pathway as a consequence of the topical application of xenobiotic compounds. The use of the technique to study phototoxicity and sunscreen efficacy in terms of modulation of the AA pathway is currently in progress. However, there are numerous other signaling pathways within the skin that could potentially be probed based up the general methodology described herein, although whereas COX-2 was universally modulated in the examples given, attempts to determined modulation of 5-LOX in this model were less predictable; the reason for this remains unclear. The current model is by its very nature a composite of xenobiotic transport and biological activity. Indeed, biological activity can only be observed if sufficient compound has penetrated the skin and diffused across the stratum corneum to the dividing keratinocytes of the viable epidermis.
Finally, it is recognized that this review relates almost entirely to the work carried out in the author’s laboratory. It is hoped the approaches described can be adopted more widely in the area of topical drug delivery system development.
CONCLUSION
In this article, a reproducible protocol has been described for determining the modulatory effects of topically applied xenobiotics on the arachidonic acid inflammation pathway within ex vivo skin. The major advantages include:
Freshly excised porcine ears are generally accessible, inexpensive and free of ethical restrictions.
Modulation of short-lived COX-2 is a useful marker for skin inflammation, as it is directly linked to PGE-2 levels.
Determination readily achieved by regular molecular biology techniques: semi quantitative WB and/or qualitative IHC.
Able to provide direct evidence of xenobiotic (pro- or anti-inflammatory) penetration across the stratum corneum to the viable epidermis, including shunt routes, unlike cell culture and reconstructed epidermis models.
Based on ex abattoir material, the method is conducive to broad 3 Rs philosophy, and has potential for the significant “replacement” of live animal experimentation.
Acknowledgments
The author is grateful to those individuals whose work contributed to developing this method, in particular Dr. Hanif Zulfakar, Dr. Nassima Ouitas Abdelouahab, Dr. Nor Hayati Abu Samah, Dr. Zoe Davison, Dr. Christopher Thomas, Dr. David Houston, Dr. Aysu Yurdasiper and Charlene Mei Yian Ong.
References
- 1.Schaefer H, Redelmeier TE. (1996) Skin Barrier, Principles of Percutaneous Absorption. Basel: S. Karger; 310 p. [Google Scholar]
- 2.Oesch F, Fabian E, Oesch-Bartlomowicz B, Werner C, Landsiedel R. (2007) Drug-metabolizing enzymes in the skin of man, rat, and pig. Drug Metab Rev 39: 659-698. doi: 10.1080/03602530701690366. [DOI] [PubMed] [Google Scholar]
- 3.Pasparakis M, Haase I, Nestle FO. (2014) Mechanisms regulating skin immunity and inflammation. Nat Rev Immunol 14: 289-301. doi: 10.1038/nri3646. [DOI] [PubMed] [Google Scholar]
- 4.Monteleone G, Pallone F, MacDonald TT, Chimenti S, Costanzo A. (2011) Psoriasis: from pathogenesis to novel therapeutic approaches. Clin Sci 120: 1-11. doi: 10.1042/CS20100163. [DOI] [PubMed] [Google Scholar]
- 5.Buckman SY, Gresham A, Hale P, Hruza G, Anast J, Masferrer J, Pentland AP. (1998) COX-2 expression is induced by UVB exposure in human skin: implications for the development of skin cancer. Carcinogenesis 19: 723-729. doi: 10.1093/carcin/19.5.723. [DOI] [PubMed] [Google Scholar]
- 6.Ahuja M, Dhake AS, Sharma SK, Majumdar DK. (2008) Topical ocular delivery of NSAIDs. AAPS J 10: 229-241. doi: 10.1208/s12248-008-9024-9. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Crofford LJ. (1997) COX-1 and COX-2 tissue expression: implications and predictions. J Rheumatol Suppl 49: 15-19. PMID: [PubMed] [Google Scholar]
- 8.Marks F, Fürstenberger G, Müller-Decker K. (1998) Arachidonic acid metabolism as a reporter of skin irritancy and target of cancer chemoprevention. Toxicol Lett 96-97: 111-118. doi: 10.1016/s0378-4274(98)00057-5. PMID: [DOI] [PubMed] [Google Scholar]
- 9.Marnett LJ, Rowlinson SW, Goodwin DC, Kalgutkar AS, Lanzo CA. (1999) Arachidonic Acid Oxygenation by COX-1 and COX-2. J Biol Chem 274: 22903-22906. doi: 10.1074/jbc.274.33.22903. [DOI] [PubMed] [Google Scholar]
- 10.Chandrasekharan NV, Simmons DL. (2004) The cyclooxygenases. Genome Biol 5: 241. doi: 10.1186/gb-2004-5-9-241. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Chen Y, Chen P, Hanaoka M, Droma Y, Kubo K. (2008) Enhanced levels of prostaglandin E2 and matrix metalloproteinase-2 correlate with the severity of airflow limitation in stable COPD. Respirology 13: 1014-1021. doi: 10.1111/j.1440-1843.2008.01365.x. PMID: [DOI] [PubMed] [Google Scholar]
- 12.Minghetti L. (2004) Cyclooxygenase-2 (COX-2) in inflammatory and degenerative brain diseases. J Neuropathol Exp Neurol 63: 901-910. doi: 10.1093/jnen/63.9.901. PMID: [DOI] [PubMed] [Google Scholar]
- 13.Nassar A, Radhakrishnan A, Cabrero IA, Cotsonis G, Cohen C. (2007) COX-2 expression in invasive breast cancer. Appl Immunohistochem Mol Morphol 15: 255-259. doi: 10.1097/01.pai.0000213130.63417.b3. [DOI] [PubMed] [Google Scholar]
- 14.Menter DG, Schilsky RL, DuBois RN. (2010) Cyclooxygenase-2 and cancer treatment: understanding the risk should be worth the reward. Clin Cancer Res 16: 1384-1390. doi: 10.1158/1078-0432.CCR-09-0788. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Lawrence J. (2016) Anti-inflammatory drugs linked with higher risk of heart failure. Pharm J 8 doi: 10.1211/PJ.2016.20201783. [DOI] [Google Scholar]
- 16.Cannon CP, Cannon PJ. (2012) Physiology. COX-2 inhibitors and cardiovascular risk. Science 336: 1386-1387. doi: 10.1126/science.1224398. PMID: [DOI] [PubMed] [Google Scholar]
- 17.Barkin RL. (2015) Topical nonsteroidal anti-inflammatory drugs: The importance of drug, delivery, and therapeutic outcome. Am J Ther 22: 388-407. doi: 10.1097/MJT.0b013e3182459abd. PMID: [DOI] [PubMed] [Google Scholar]
- 18.Potts RO, Guy RH. (1992) Predicting skin permeability. Pharm Res 9: 663-669. doi: 10.1023/a:1015810312465. PMID: [DOI] [PubMed] [Google Scholar]
- 19.Sütő B, Berkó S, Kozma G, Kukovecz Á, Budai-Szűcs M, et al. (2016) Development of ibuprofen-loaded nanostructured lipid carrier-based gels: characterization and investigation of in vitro and in vivo penetration through the skin. Int J Nanomedicine 11: 1201-1212. doi: 10.2147/IJN.S99198. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Lademann J, Jacobi U, Surber C, Weigmann H, Fluhr JW. (2008) The tape stripping procedure--evaluation of some critical parameters. Eur J Pharm Biopharm 72: 317-323. doi: 10.1016/j.ejpb.2008.08.008. PMID: [DOI] [PubMed] [Google Scholar]
- 21.Flecknell P. (2002) Replacement, reduction and refinement. ALTEX 19: 73-78. PMID: [PubMed] [Google Scholar]
- 22.Bralley EE, Greenspan P, Hargrove JL, Wicker L, Hartle DK. (2008) Topical anti-inflammatory activity of Polygonum cuspidatum extract in the TPA model of mouse ear inflammation. J Inflamm (Lond) 5: 1. doi: 10.1186/1476-9255-5-1. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Kim EJ, Park H, Kim J, Park JHY. (2010) 3,3'-diindolylmethane suppresses 12-O-tetradecanoylphorbol-13-acetate-induced inflammation and tumor promotion in mouse skin via the downregulation of inflammatory mediators. Mol Carcinog 49: 672-683. doi: 10.1002/mc.20640. PMID: [DOI] [PubMed] [Google Scholar]
- 24.Cichocki M, Blumczyńska J, Baer-Dubowska W. (2009) Naturally occurring phenolic acids inhibit 12-O-tetradecanoylphorbol-13-acetate induced NF-kappaB, iNOS and COX-2 activation in mouse epidermis. Toxicology 268: 118-124. doi: 10.1016/j.tox.2009.12.013. PMID: [DOI] [PubMed] [Google Scholar]
- 25.Burke JR, Davern LB, Stanley PL, Gregor KR, Banville J, et al. (2001) BMS-229724 is a tight-binding inhibitor of cytosolic phospholipase A2 that acts at the lipid/water interface and possesses anti-inflammatory activity in skin inflammation models. J Pharmacol Exp Ther 298: 376-385. PMID: [PubMed] [Google Scholar]
- 26.De Vry CG, Valdez M, Lazarov M, Muhr E, Buelow R, et al. (2005) Topical application of a novel immunomodulatory peptide, RDP58, reduces skin inflammation in the phorbol ester-induced dermatitis model. J Invest Dermatol 125: 473-481. doi: 10.1111/j.0022-202X.2005.23831.x. PMID: [DOI] [PubMed] [Google Scholar]
- 27.Morris CJ. (2003) Carrageenan-induced paw edema in the rat and mouse. Methods Mol Biol 225: 115-121. doi: 10.1385/1-59259-374-7:115. PMID: [DOI] [PubMed] [Google Scholar]
- 28.Sharma JN, Samud AM, Asmawi MZ. (2004) Comparison between plethysmometer and micrometer methods to measure acute paw oedema for screening anti-inflammatory activity in mice. Inflammopharmacology 12: 89-94. doi: 10.1163/156856004773121400. PMID: [DOI] [PubMed] [Google Scholar]
- 29.Albanesi C, Scarponi C, Giustizieri ML, Girolomoni G. (2005) Keratinocytes in inflammatory skin diseases. Curr Drug Targets Inflamm Allergy 4: 329-334. doi: 10.2174/1568010054022033. PMID: [DOI] [PubMed] [Google Scholar]
- 30.Lau WM, Ng KW, White AW, Heard CM. (2011) Therapeutic and cytotoxic effects of the novel antipsoriasis codrug, naproxyl-dithranol, on HaCaT cells. Mol Pharm 8: 2398-2407. doi: 10.1021/mp200327k. PMID: [DOI] [PubMed] [Google Scholar]
- 31.Zampetti A, Mastrofrancesco A, Flori E, Maresca V, Picardo M, et al. (2009) Proinflammatory cytokine production in HaCaT cells treated by eosin: implications for the topical treatment of psoriasis. Int J Immunopathol Pharmacol 22: 1067-1075. doi: 10.1177/039463200902200423. PMID: [DOI] [PubMed] [Google Scholar]
- 32.Hewitt NJ, Edwards RJ, Fritsche E, Goebel C, Aeby P, et al. (2013) Use of human in vitro skin models for accurate and ethical risk assessment: metabolic considerations. Toxicol Sci 133: 209-217. doi: 10.1093/toxsci/kft080. PMID: [DOI] [PubMed] [Google Scholar]
- 33.Roguet R, Cohen C, Dossou KG, Rougier A. (1994) Episkin, a reconstituted human epidermis for assessing in vitro the irritancy of topically applied compounds. Toxicol In Vitro 8: 283-291. doi: 10.1016/0887-2333(94)90195-3. PMID: [DOI] [PubMed] [Google Scholar]
- 34.Spielmann H, Hoffmann S, Liebsch M, Botham P, Fentem JH, et al. (2007) The ECVAM international validation study on in vitro tests for acute skin irritation: report on the validity of the EPISKIN and EpiDerm assays and on the Skin Integrity Function Test. Altern Lab Anim 35: 559-601. doi: 10.1177/026119290703500614. PMID: [DOI] [PubMed] [Google Scholar]
- 35.de Yzaguirre MM, Bacchini G, Luna EG, Vila-Martínez E. (2014) Anti-inflammatory efficacy of product containing “skin calm complex” in vitro reconstructed epidermis. JCDSA 4: 309-315. doi: 10.4236/jcdsa.2014.45040. [DOI] [Google Scholar]
- 36.Weindl G, Castello F, Schäfer-Korting M. (2011) Evaluation of anti-inflammatory and atrophogenic effects of glucocorticoids on reconstructed human skin. Altern Lab Anim 39: 173-187. doi: 10.1177/026119291103900212. PMID: [DOI] [PubMed] [Google Scholar]
- 37.Houston DMJ, Bugert J, Denyer SP, Heard CM. (2016) Anti-inflammatory activity of Punica granatum L. (Pomegranate) rind extracts applied topically to ex vivo skin. Eur J Pharm Biopharm 112: 30-37. doi: 10.1016/j.ejpb.2016.11.014. PMID: [DOI] [PubMed] [Google Scholar]
- 38.Dick IP, Scott RC. (1992) Pig ear skin as an in-vitro model for human skin permeability. J Pharm Pharmacol 44: 640-645. doi: 10.1111/j.2042-7158.1992.tb05485.x. PMID: [DOI] [PubMed] [Google Scholar]
- 39.Godin B, Touitou E. (2007) Transdermal skin delivery: predictions for humans from in vivo, ex vivo and animal models. Adv Drug Deliv Rev 59: 1152-1161. doi: 10.1016/j.addr.2007.07.004. PMID: [DOI] [PubMed] [Google Scholar]
- 40.Barbero AM, Frasch HF. (2008) Pig and guinea pig skin as surrogates for human in vitro penetration studies: a quantitative review. Toxicol In Vitro 23: 1-13. doi: 10.1016/j.tiv.2008.10.008. PMID: [DOI] [PubMed] [Google Scholar]
- 41.Gray GM, Yardley HJ. (1975) Lipid compositions of cells isolated from pig, human, and rat epidermis. J Lipid Res 16: 434-440. PMID: [PubMed] [Google Scholar]
- 42.Schmook FP, Meingassner JG, Billich A. (2001) Comparison of human skin or epidermis models with human and animal skin in in-vitro percutaneous absorption. Int J Pharm 215: 51-56. doi: 10.1016/s0378-5173(00)00665-7. PMID: [DOI] [PubMed] [Google Scholar]
- 43.Kong R, Bhargava R. (2011) Characterization of porcine skin as a model for human skin studies using infrared spectroscopic imaging. Analyst 136: 2359-2366. doi: 10.1039/c1an15111h. PMID: [DOI] [PubMed] [Google Scholar]
- 44.Meyer W. (1996) Comments on the suitability of swine skin as a biological model for human skin. Hautarzt 47: 178-182. doi: 10.1007/s001050050399. PMID: [DOI] [PubMed] [Google Scholar]
- 45.Meurens F, Summerfield A, Nauwynck H, Saif L, Gerdts V. (2011) The pig: a model for human infectious diseases. Trends Microbiol 20: 50-57. doi: 10.1016/j.tim.2011.11.002. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 46.Summerfield A, Meurens F, Ricklin ME. (2014) The immunology of the porcine skin and its value as a model for human skin. Mol Immunol 66: 14-21. doi: 10.1016/j.molimm.2014.10.023. PMID: [DOI] [PubMed] [Google Scholar]
- 47.Turner NJ, Pezzone D, Badylak SF. (2014) Regional variations in the histology of porcine skin. Tissue Eng Part C Methods 21: 373-384. doi: 10.1089/ten.TEC.2014.0246. PMID: [DOI] [PubMed] [Google Scholar]
- 48.Williams AC. (2003) Transdermal and Topical Drug Delivery from Theory to Clinical Practice. London: Pharmaceutical Press; 224 p. [Google Scholar]
- 49.Bronaugh RL. (2013) Methods for in vitro skin metabolism studies. Wilhelm KP, Zhai H, Maibach HI. (Eds.). Dermatotoxicology (8th ed.). Boca Raton: CRC Press; Chapter 43. [Google Scholar]
- 50.Zulfakar MH, Abdelouahab N, Heard CM. (2009) Enhanced topical delivery and ex vivo anti-inflammatory activity from a betamethasone dipropionate formulation containing fish oil. Inflamm Res 59: 23-30. doi: 10.1007/s00011-009-0065-z. PMID: [DOI] [PubMed] [Google Scholar]
- 51.Thomas CP, Heard CM. (2006) Probing the skin permeation of eicosapentaenoic acid and ketoprofen 2. Comparative depth profiling and metabolism of eicosapentaenoic acid. Eur J Pharm Biopharm 67: 156-165. doi: 10.1016/j.ejpb.2006.11.024. PMID: [DOI] [PubMed] [Google Scholar]
- 52.Ouitas NA, Heard CM. (2009) A novel ex vivo skin model for the assessment of the potential transcutaneous anti-inflammatory effect of topically applied Harpagophytum procumbens extract. Int J Pharm 376: 63-68. doi: 10.1016/j.ijpharm.2009.04.017. PMID: [DOI] [PubMed] [Google Scholar]
- 53.Laouini D, Elkhal A, Yalcindag A, Kawamoto S, Oettgen H, et al. (2005) COX-2 inhibition enhances the TH2 immune response to epicutaneous sensitization. J Allergy Clin Immunol 116: 390-396. doi: 10.1016/j.jaci.2005.03.042. PMID: [DOI] [PubMed] [Google Scholar]
- 54.Koppes SA, Brans R, Ljubojevic Hadzavdic S, Frings-Dresen MHW, Rustemeyer T, et al. (2016) Stratum corneum tape stripping: monitoring of inflammatory mediators in atopic dermatitis patients using topical therapy. Int Arch Allergy Immunol 170: 187-193. doi: 10.1159/000448400. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 55.Kurien BT, Scofield RH. (2006) Western blotting. Methods 38: 283-293. doi: 10.1016/j.ymeth.2005.11.007. PMID: [DOI] [PubMed] [Google Scholar]
- 56.Alegria-Schaffer A. (2014) Western blotting using chemiluminescent substrates. Methods Enzymol 541: 251-259. doi: 10.1016/B978-0-12-420119-4.00019-7. PMID: [DOI] [PubMed] [Google Scholar]
- 57.Abu Samah NH, Heard CM. (2013) The effects of topically applied polyNIPAM-based nanogels and their monomers on skin cyclooxygenase expression, ex vivo. Nanotoxicology 8: 100-106. doi: 10.3109/17435390.2012.754511. PMID: [DOI] [PubMed] [Google Scholar]
- 58.Gilda JE, Gomes AV. (2013) Stain-Free total protein staining is a superior loading control to β-actin for Western blots. Anal Biochem 440: 186-188. doi: 10.1016/j.ab.2013.05.027. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 59.Dewar R, Andea AA, Guitart J, Arber DA, Weiss LM. (2015) Best practices in diagnostic immunohistochemistry: workup of cutaneous lymphoid lesions in the diagnosis of primary cutaneous lymphoma. Arch Pathol Lab Med 139: 338-350. doi: 10.5858/arpa.2014-0018-CP. PMID: [DOI] [PubMed] [Google Scholar]
- 60.Hassan HE, Mohamed AAB, Bakhiet AO, Ahmed HG. (2013) Immunohistochemical expression of COX2 and iNOS in bladder cancer and its association with urinary schistosomiasis among Sudanese patients. Infect Agent Cancer 8: 9. doi: 10.1186/1750-9378-8-9. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Hamamoto T, Yabuki A, Yamato O, Fujiki M, Misumi K, et al. (2009) Immunohistochemical analysis of cyclooxygenase-2 induction during wound healing in dog skin. Res Vet Sci 87: 349-354. doi: 10.1016/j.rvsc.2009.05.004. [DOI] [PubMed] [Google Scholar]
- 62.Abdelouahab N, Heard C. (2008) Effect of the major glycosides of Harpagophytum procumbens (Devil's Claw) on epidermal cyclooxygenase-2 (COX-2) in vitro. J Nat Prod 71: 746-749. doi: 10.1021/np070204u. PMID: [DOI] [PubMed] [Google Scholar]
- 63.Thomas CP, Davison Z, Heard CM. (2007) Probing the skin permeation of fish oil/EPA and ketoprofen-3. Effects on epidermal COX-2 and LOX. Prostaglandins Leukot Essent Fatty Acids 76: 357-362. doi: 10.1016/j.plefa.2007.05.002. PMID: [DOI] [PubMed] [Google Scholar]
- 64.Yurdasiper A, Ertan G, Heard CM. (2018) Enhanced delivery of naproxen to the viable epidermis from an activated poly N-isopropylacrylamide (PNIPAM) Nanogel: Skin penetration, modulation of COX-2 expression and rat paw oedema. Nanomedicine 14: 2051-2059. doi: 10.1016/j.nano.2018.05.017. PMID: [DOI] [PubMed] [Google Scholar]
- 65.Gil A. (2002) Polyunsaturated fatty acids and inflammatory diseases. Biomed Pharmacother 56: 388-396. doi: 10.12691/jfnr-3-9-10. [DOI] [PubMed] [Google Scholar]
- 66.Bagga D, Wang L, Farias-Eisner R, Glaspy JA, Reddy ST. (2003) Differential effects of prostaglandin derived from omega-6 and omega-3 polyunsaturated fatty acids on COX-2 expression and IL-6 secretion. Proc Natl Acad Sci U S A 100: 1751-1756. doi: 10.1073/pnas.0334211100. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 67.Nugteren DH, Christ-Hazelhof E, van der Beek A, Houtsmuller UM. (1985) Metabolism of linoleic acid and other essential fatty acids in the epidermis of the rat. Biochim Biophys Acta 834: 429-436. doi: 10.1016/0005-2760(85)90017-7. PMID: [DOI] [PubMed] [Google Scholar]
- 68.Puglia C, Tropea S, Rizza L, Santagati NA, Bonina F. (2005) In vitro percutaneous absorption studies and in vivo evaluation of anti-inflammatory activity of essential fatty acids (EFA) from fish oil extracts. Int J Pharm 299: 41-48. doi: 10.1016/j.ijpharm.2005.04.031. PMID: [DOI] [PubMed] [Google Scholar]
- 69.Thomas CP, Heard CM. (2005) In vitro transcutaneous delivery of ketoprofen and essential polyunsaturated fatty acids from a fish oil vehicle incorporating 1,8-cineole. Drug Deliv 12: 7-14. doi: 10.1080/10717540590889565. PMID: [DOI] [PubMed] [Google Scholar]
- 70.Thomas CP, Heard CM. (2007) Probing the skin permeation of eicosapentaenoic acid and ketoprofen2. Comparative depth profiling and metabolism of eicosapentaenoic acid. Eur J Pharm Biopharm 67: 156-165. doi: 10.1016/j.ejpb.2006.11.024. [DOI] [PubMed] [Google Scholar]
- 71.Mncwangi N, Chen W, Vermaak I, Viljoen AM, Gericke N. (2012) Devil's Claw-a review of the ethnobotany, phytochemistry and biological activity of Harpagophytum procumbens. J Ethnopharmacol 143: 755-771. doi: 10.1016/j.jep.2012.08.013. PMID: [DOI] [PubMed] [Google Scholar]
- 72.Ouitas NA, Heard C. (2010) Estimation of the relative antiinflammatory efficacies of six commercial preparations of Harpagophytum procumbens (Devil's Claw). Phytother Res 24: 333-338. doi: 10.1002/ptr.2930. PMID: [DOI] [PubMed] [Google Scholar]
- 73.Houston DMJ, Bugert JJ, Denyer SP, Heard CM. (2017) Potentiated virucidal activity of pomegranate rind extract (PRE) and punicalagin against Herpes simplex virus (HSV) when co-administered with zinc (II) ions, and antiviral activity of PRE against HSV and aciclovir-resistant HSV. PLoS One 12: doi: 10.1371/journal.pone.0179291. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Adams LS, Seeram NP, Aggarwal BB, Takada Y, Sand D, et al. (2006) Pomegranate juice, total pomegranate ellagitannins, and punicalagin suppress inflammatory cell signaling in colon cancer cells. J Agric Food Chem 54: 980-985. doi: 10.1021/jf052005r. PMID: [DOI] [PubMed] [Google Scholar]
- 75.Roselli M, Finamore A, Garaguso I, Britti MS, Mengheri E. (2003) Zinc oxide protects cultured enterocytes from the damage induced by Escherichia coli. J Nutr 133: 4077-4082. doi: 10.1093/jn/133.12.4077. PMID: [DOI] [PubMed] [Google Scholar]
- 76.Olajide OA, Kumar A, Velagapudi R, Okorji UP, Fiebich BL. (2014) Punicalagin inhibits neuroinflammation in LPS-activated rat primary microglia. Mol Nutr Food Res 58: 1843-1851. doi: 10.1002/mnfr.201400163. PMID: [DOI] [PubMed] [Google Scholar]
- 77.Houston DMJ, Robins B, Bugert JJ, Denyer SP, Heard CM. (2016) In vitro permeation and biological activity of punicalagin and zinc (II) across skin and mucous membranes prone to Herpes simplex virus infection. Eur J Pharm Sci 96: 99-106. doi: 10.1016/j.ejps.2016.08.013. PMID: [DOI] [PubMed] [Google Scholar]
- 78.Flynn GL, Stewart B. (1988) Percutaneous drug penetration: Choosing candidates for transdermal development. Drug Dev Res 13: 169-185. doi: 10.1002/ddr.430130209. [DOI] [Google Scholar]
- 79.Samah NA, Williams N, Heard CM. (2010) Nanogel particulates located within diffusion cell receptor phases following topical application demonstrates uptake into and migration across skin. Int J Pharm 401: 72-78. doi: 10.1016/j.ijpharm.2010.08.011. PMID: [DOI] [PubMed] [Google Scholar]
- 80.Cutolo M, Sulli A, Pizzorni C, Seriolo B, Straub RH. (2001) Anti-inflammatory mechanisms of methotrexate in rheumatoid arthritis. Ann Rheum Dis 60: 729-735. doi: 10.1136/ard.60.8.729. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Singka GSL, Samah NA, Zulfakar MH, Yurdasiper A, Heard CM. (2010) Enhanced topical delivery and anti-inflammatory activity of methotrexate from an activated nanogel. Eur J Pharm Biopharm 76: 275-281. doi: 10.1016/j.ejpb.2010.06.014. PMID: [DOI] [PubMed] [Google Scholar]
- 82.Ricciotti E, FitzGerald GA. (2011) Prostaglandins and inflammation. Arterioscler Thromb Vasc Biol 31: 986-1000. doi: 10.1161/ATVBAHA.110.207449. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 83.Kiraly AJ, Soliman E, Jenkins A, Van Dross RT. (2015) Apigenin inhibits COX-2, PGE2, and EP1 and also initiates terminal differentiation in the epidermis of tumor bearing mice. Prostaglandins Leukot Essent Fatty Acids 104: 44-53. doi: 10.1016/j.plefa.2015.11.006. PMID: [DOI] [PubMed] [Google Scholar]
- 84.Rathee P, Chaudhary H, Rathee S, Rathee D, Kumar V, et al. (2009) Mechanism of action of flavonoids as anti-inflammatory agents: a review. Inflamm Allergy Drug Targets 8: 229-235. doi: 10.2174/187152809788681029. PMID: [DOI] [PubMed] [Google Scholar]
- 85.Vane JR. (1971) Inhibition of prostaglandin synthesis as a mechanism of action for aspirin-like drugs. Nat New Biol 231: 232-235. doi: 10.1038/newbio231232a0. PMID: [DOI] [PubMed] [Google Scholar]
- 86.Xu XM, Sansores-Garcia L, Chen XM, Matijevic-Aleksic N, Du M, et al. (1999) Suppression of inducible cyclooxygenase 2 gene transcription by aspirin and sodium salicylate. Proc Natl Acad Sci U S A 96: 5292-5297. doi: 10.1073/pnas.96.9.5292. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]
- 87.Ong SL, Gravante G, Metcalfe MS, Dennison AR. (2013) History, ethics, advantages and limitations of experimental models for hepatic ablation. World J Gastroenterol 19: 147-154. doi: 10.3748/wjg.v19.i2.147. PMID: [DOI] [PMC free article] [PubMed] [Google Scholar]