

Key Points
Question
What is the association between the coronavirus disease 2019 (COVID-19) pandemic and out-of-hospital cardiac arrest (OHCA) outcomes in the US?
Findings
This registry study found that rates of return of spontaneous circulation were 18% lower overall than before the pandemic, including 11% to 15% lower in communities with low COVID-19 mortality. Rates of survival to discharge were 17% lower, primarily in communities with moderate to high COVID-19 mortality, and incidence of OHCA was higher, but largely in communities with high COVID-19 mortality.
Meaning
The outcomes of OHCA were worse during the first weeks of the COVID-19 pandemic in the US, and this was observed not only in areas with high case-fatality rates but also ones with lower rates.
This registry-based study compares out-of-hospital cardiac arrest outcomes in the first few weeks of the coronavirus disease 2019 pandemic in 2020 with outcomes in the same period in 2019.
Abstract
Importance
Recent reports from communities severely affected by the coronavirus disease 2019 (COVID-19) pandemic found lower rates of sustained return of spontaneous circulation (ROSC) for out-of-hospital cardiac arrest (OHCA). Whether the pandemic has affected OHCA outcomes more broadly is unknown.
Objective
To assess the association between the COVID-19 pandemic and OHCA outcomes, including in areas with low and moderate COVID-19 disease burden.
Design, Setting, and Participants
This study used a large US registry of OHCAs to compare outcomes during the pandemic period of March 16 through April 30, 2020, with those from March 16 through April 30, 2019. Cases were geocoded to US counties, and the COVID-19 mortality rate in each county was categorized as very low (0-25 per million residents), low (26-100 per million residents), moderate (101-250 per million residents), high (251-500 per million residents), or very high (>500 per million residents). As additional controls, the study compared OHCA outcomes during the prepandemic period (January through February) and peripandemic period (March 1 through 15).
Exposure
The COVID-19 pandemic.
Main Outcomes and Measures
Sustained ROSC (≥20 minutes), survival to discharge, and OHCA incidence.
Results
A total of 19 303 OHCAs occurred from March 16 through April 30 in both years, with 9863 cases in 2020 (mean [SD] age, 62.6 [19.3] years; 6040 men [61.3%]) and 9440 in 2019 (mean [SD] age, 62.2 [19.2] years; 5922 men [62.7%]). During the pandemic, rates of sustained ROSC were lower than in 2019 (23.0% vs 29.8%; adjusted rate ratio, 0.82 [95% CI, 0.78-0.87]; P < .001). Sustained ROSC rates were lower by between 21% (286 of 1429 [20.0%] in 2020 vs 305 of 1130 [27.0%] in 2019; adjusted RR, 0.79 [95% CI, 0.65-0.97]) and 33% (149 of 863 [17.3%] in 2020 vs 192 of 667 [28.8%] in 2019; adjusted RR, 0.67 [95% CI, 0.56-0.80]) in communities with high or very high COVID-19 mortality, respectively; however, rates of sustained ROSC were also lower by 11% (583 of 2317 [25.2%] in 2020 vs 740 of 2549 [29.0%] in 2019; adjusted RR, 0.89 [95% CI, 0.81-0.98]) to 15% (889 of 3495 [25.4%] in 2020 vs 1109 of 3532 [31.4%] in 2019; adjusted RR, 0.85 [95% CI, 0.78-0.93]) in communities with very low and low COVID-19 mortality. Among emergency medical services agencies with complete data on hospital survival (7085 total patients), survival to discharge was lower during the pandemic compared with 2019 (6.6% vs 9.8%; adjusted RR, 0.83 [95% CI, 0.69-1.00]; P = .048), primarily in communities with moderate to very high COVID-19 mortality (interaction P = .049). Incidence of OHCA was higher than in 2019, but the increase was largely observed in communities with high COVID-19 mortality (adjusted mean difference, 38.6 [95% CI, 37.1-40.1] per million residents) and very high COVID-19 mortality (adjusted mean difference, 28.7 [95% CI, 26.7-30.6] per million residents). In contrast, there was no difference in rates of sustained ROSC or survival to discharge during the prepandemic and peripandemic periods in 2020 vs 2019.
Conclusions and Relevance
Early during the pandemic, rates of sustained ROSC for OHCA were lower throughout the US, even in communities with low COVID-19 mortality rates. Overall survival was lower, primarily in communities with moderate or high COVID-19 mortality.
Introduction
Recent studies from communities severely affected by the novel coronavirus 2019 (COVID-19) pandemic have reported lower rates of successful resuscitation for out-of-hospital cardiac arrest (OHCA).1,2,3 Unadjusted rates of sustained return of spontaneous circulation (ROSC) decreased by an absolute 14.6% (from 25.2% in 2019 to 10.6% in 2020) in New York, New York,1 and by 8.5% (from 13.5% in 2019 to 5.0% in 2020) in northern Italy.2 Investigators have speculated that lower rates were because of higher patient illness severity and overwhelmed emergency medical service (EMS) agencies during the COVID-19 pandemic. However, it is unknown if lower rates of sustained ROSC for OHCA are generalizable to geographic regions less severely affected by the COVID-19 pandemic and/or accompanied by lower rates of survival to discharge.
For several reasons, it is possible that the impact of the COVID-19 pandemic on rates of sustained ROSC after OHCA has not been limited to just regions with high COVID-19 disease burden. Policy changes that were instituted among EMS agencies during the pandemic may have been implemented broadly, even in areas with low to moderate COVID-19 incidence. These changes may affect rates of sustained ROSC, including slower response because of a need to don personal protective equipment, shorter treatment duration on EMS arrival, or higher rates of termination of resuscitation in the field in patients without ROSC. It is also unclear if prior reports of lower rates of sustained ROSC during the pandemic actually resulted in lower rates of survival to discharge, because sustained ROSC is an intermediate outcome and can be influenced by multiple factors (eg, high-dose epinephrine) without improving overall survival.
Accordingly, we linked OHCA data from the Cardiac Arrest Registry to Enhance Survival (CARES) to COVID-19 disease mortality data in the US. Our primary goal was to examine whether rates of sustained ROSC for OHCA decreased and if such decreases were confined only to communities with high COVID-19 mortality rates. Additionally, we examined rates of termination of resuscitation in the field and overall survival to discharge and the extent to which the incidence of OHCA increased in US regions with low, moderate, and high COVID-19 disease burden.
Methods
Data Source and Study Design
The data that support the findings of this study are available from the corresponding author on request and approval by the CARES registry. The CARES registry is a prospective multicenter registry of patients with OHCA in the US with a catchment area of approximately 152 million residents. The design of the registry, which was established by the US Centers for Disease Control and Prevention and Emory University, has been previously described.4,5 Briefly, all patients with a confirmed OHCA for whom resuscitation was attempted are identified and followed up by EMS agencies. Data are collected from 3 sources: 911 dispatch (public safety answering point) centers, EMS agencies, and receiving hospitals. Standardized international Utstein definitions for defining clinical variables and outcomes are used to ensure uniformity.6 A CARES analyst (R.A.-A.) reviewed records for completeness and accuracy.5 The study was approved by Saint Luke’s Hospital’s institutional review board, which waived the requirement for informed consent because the study involved deidentified data.
Study Population
In this study, we were interested in comparing OHCAs occurring in 2020 vs 2019 during the months of January through April. Therefore, the cohort was restricted to EMS agencies that submitted data during these months in 2020 and 2019.
Data Collection and Processing
The CARES registry collects patient-level data on demographics (age, sex, and race/ethnicity [self-identified]), location of cardiac arrest, initial cardiac arrest rhythm, and whether the arrest was witnessed. Additionally, information on cardiac arrest causative mechanism (presumed cardiac, respiratory, drug overdose, and other mechanism) and as to whether bystander cardiopulmonary resuscitation (CPR) or defibrillation with an automated external defibrillator was administered prior to EMS arrival is collected, as well as the time interval to EMS arrival and the interval of EMS treatment.
The primary outcome was sustained ROSC, defined as restoration of a pulse for 20 minutes or longer. Secondary outcomes included termination of resuscitation in the field (ie, terminated CPR efforts and a patient declared dead without hospital transport) and incidence rate of OHCA. Additionally, within EMS agencies with complete (>99%) data on survival to discharge during 2020, we examined rates of survival to discharge. The independent variable was the year of arrest (2020 vs 2019), and we divided the months of January through April into 3 COVID-19 comparison periods: prepandemic (January 1 through February 28 or 29); peripandemic (March 1 through 15); and pandemic (March 16 through April 30), when the COVID-19 case surge led to lockdowns throughout much of the US. For the purposes of this study, we focused on OHCA outcomes in 2020 vs 2019 during the pandemic period (comparing March 16 through April 30 across both years) but used the prepandemic and peripandemic period comparisons as additional controls for the pandemic period results.
Besides an overall comparison of OHCA outcomes between 2020 and 2019 during the pandemic periods, we also examined whether differences in OHCA outcomes during the pandemic period in 2020 were confined to communities with high COVID-19 mortality rates. Daily county-level COVID-19 mortality data were obtained from publicly available sources.7 For each county, we calculated the mortality rate per million residents attributed to COVID-19 by dividing the total number of deaths attributed to COVID-19 occurring during the pandemic period by the number of residents in the county. Each patient in CARES was geocoded to a US county based on the zip code location of their OHCA through a crosswalk file from the US Department of Housing and Urban Development that links each zip code to a US county.8 This CARES file with county-level information was then merged with the COVID-19 mortality data file.
Statistical Analyses
Given the large sample size, baseline differences for patients with an OHCA during the pandemic period of March 16 through April 30, 2020, were compared with patients from the same period in 2019 using standardized differences, with a standardized difference of more than 10% denoting a clinically meaningful difference.9 To examine whether rates of sustained ROSC were different in 2020 vs 2019 during the pandemic period, we constructed multivariable hierarchical logistic regression models, with EMS agency as a random effect to account for clustering of patients within agencies. Modified Poisson regression with robust variance estimates was used to directly estimate rate ratios (RRs).10,11 The model adjusted for demographics (age, sex, and race/ethnicity), cardiac arrest characteristics (initial cardiac arrest rhythm, whether the cardiac arrest was witnessed, cardiac arrest location [home, commercial workplace, public location, recreational facility, nursing home or associated health care entity, or other], and causative mechanism of cardiac arrest [presumed cardiac mechanism, respiratory mechanism, drug overdose, and other]), whether bystander CPR or defibrillation was performed, and interactions between bystander CPR and defibrillation with OHCA location to account for differences in rates of bystander interventions performed at home vs the other locations.
We then included in the model above an interaction term between calendar year and the county-level COVID-19 mortality rate during the pandemic period to determine if sustained ROSC rates varied among communities with low, moderate, and high COVID-19 mortality. The COVID-19 mortality during the pandemic period was categorized as very low (0-25 COVID-19 deaths per million residents), low (26-100 COVID-19 deaths per million), moderate (101-250 COVID-19 deaths per million), high (251-500 COVID-19 deaths per million), and very high (>500 COVID-19 deaths per million).
We repeated these analyses for the secondary outcome of termination of resuscitation in the field, as well as survival to discharge in the EMS agencies with complete data on this outcome. Furthermore, we constructed hierarchical linear regression models with EMS agency as a random effect and compared OHCA incidence rates between 2020 vs 2019 overall and by COVID-19 mortality strata. Variables in the model had missing rates of less than 1% and were modeled as a separate category of missing data.
As additional controls for the primary outcome of sustained ROSC and the secondary outcome of survival to discharge, we examined whether there were differences in rates for each outcome in 2020 vs 2019 during the prepandemic period of January through February and the peripandemic period of March 1 through 15. In these analyses, we designated EMS agencies to be in the same COVID-19 mortality strata as they were during the pandemic period. For instance, EMS agencies in counties designated as being in the very high COVID-19 mortality stratum (>500 deaths per 1 000 000 residents) during the pandemic period were kept in this same category for analyses during the prepandemic and peripandemic periods, even though there would have been almost no COVID-19 deaths during these periods. Because we expected no difference in outcomes in 2020 vs 2019 in each of these strata during the prepandemic and peripandemic periods, these falsification analyses served as validating controls for any differences observed during the pandemic period.
For each analysis, the null hypothesis was evaluated at a 2-sided significance level of .05 and calculated 95% CIs, using robust standard errors. All statistical analyses were conducted using SAS version 9.1.3 (SAS Institute) and R version 2.6.0 (R Foundation for Statistical Computing).
Results
We initially identified 60 661 patients with an OHCA during the study period (Figure 1). We excluded 7686 cases witnessed by EMS personnel and 314 cases attributed to drowning or electrocution. We also excluded 53 patients with missing data on the primary outcome of sustained ROSC and 425 patients for whom we could not link to a US county or county-level COVID-19 mortality data. The final cohort included 52 183 patients with OHCAs in CARES-participating regions (and 783 EMS agencies), with 26 334 OHCAs occurring from January through February, 6546 from March 1 through 15, and 19 303 from March 16 through April 30 (Figure 1).
Figure 1. Definition of the Study Cohort.

The number of patients in the 3 study periods for 2020 and 2019 are depicted. COVID-19 indicates coronavirus disease 2019; EMS, emergency medical services; OHCA, out-of-hospital cardiac arrest.
Table 1 compares patients with an OHCA during the pandemic period in 2020 vs 2019, the focus of the analyses. Of the 19 303 OHCAs occurring during the pandemic period, 9863 cases were in 2020 (mean [SD] age of patients, 62.6 [19.3] years; 6040 men [61.3%]) and 9440 in 2019 (mean [SD] age of patients, 62.2 [19.2] years; 5922 men [62.7%]). There were no meaningful differences in age or sex, but patients in 2020, compared with 2019, were more likely to be of Black race/ethnicity (2019, 2137 individuals [22.6%]; 2020, 2751 individuals [28.0%]), present with an initial cardiac arrest rhythm of asystole (2019, 5071 [53.7%]; 2020, 5862 [59.6%]), experience arrest at a home location (2019, 6590 [69.8%]; 2020, 7385 [74.9%]), and have an arrest causative mechanism categorized as other (which included suspected COVID-19 infection; 2019, 132 [1.4%] vs 2020, 436 [4.4%]). Notably, the proportion of witnessed cardiac arrests were similar for both years, and there were no differences in the median time duration from 911 call to EMS arrival and duration of EMS treatment. Finally, rates of bystander CPR and defibrillation were also not different during the pandemic period in 2020 compared with the same period in 2019. Rates of bystander CPR, excluding patients in nursing homes, and bystander use of automated external defibrillators in public locations are reported in eTable 1 in the Supplement.
Table 1. Baseline Characteristics of Patients During the Pandemic Period of March 16 Through April 30, 2020, vs the Same Period in 2019.
| Variable | Patients, No. (%) | Standardized difference, %a | |
|---|---|---|---|
| 2019 (n = 9440) | 2020 (n = 9863) | ||
| Patient factors | |||
| Age, y | |||
| Mean (SD) | 62.2 (19.2) | 62.6 (19.3) | 2.1 |
| Median (IQR) | 65.0 (52.0-76.0) | 65.0 (52.0-77.0) | |
| Sex | |||
| Female | 3517 (37.3) | 3819 (38.7) | 3.0 |
| Male | 5922 (62.7) | 6040 (61.3) | |
| Missing, No. | 1 | 4 | |
| Race/ethnicity | |||
| White | 4844 (51.3) | 4716 (48.1) | 17.6 |
| Black | 2137 (22.6) | 2751 (28.0) | |
| Other | 915 (9.7) | 1160 (11.8) | |
| Unknown | 1544 (16.4) | 1186 (12.1) | |
| Missing, No. | NA | 50 | |
| Cardiac arrest factors | |||
| First documented cardiac arrest rhythm | |||
| Nonshockable | |||
| Asystole | 5071 (53.7) | 5862 (59.6) | 14.2 |
| Pulseless electrical activity | 1766 (18.7) | 1801 (18.3) | |
| Unknown nonshockable rhythm | 829 (8.8) | 750 (7.6) | |
| Shockable | |||
| Ventricular fibrillation | 1277 (13.5) | 1034 (10.5) | |
| Ventricular tachycardia | 75 (0.8) | 80 (0.8) | |
| Unknown shockable rhythm | 422 (4.5) | 309 (3.1) | |
| Missing, No. | NA | 27 | |
| Location of cardiac arrest | |||
| Home | 6590 (69.8) | 7385 (74.9) | 21.3 |
| Industrial or commercial building | 771 (8.2) | 377 (3.8) | |
| Nursing home and other health care residence | 1479 (15.7) | 1609 (16.3) | |
| Street and other public areas | 455 (4.8) | 393 (4.0) | |
| Recreational facility | 104 (1.1) | 35 (0.4) | |
| Other | 41 (0.4) | 60 (0.6) | |
| Missing, No. | NA | 4 | |
| Witnessed status of cardiac arrest | |||
| Bystander witnessed | 4127 (43.7) | 4049 (41.1) | 5.4 |
| Unwitnessed | 5313 (56.3) | 5812 (58.9) | |
| Missing, No. | NA | 2 | |
| Cardiac arrest causative mechanism | |||
| Presumed cardiac | 7957 (84.3) | 7935 (80.5) | 18.5 |
| Respiratory | 769 (8.1) | 878 (8.9) | |
| Drug overdose | 582 (6.2) | 614 (6.2) | |
| Other | 132 (1.4) | 436 (4.4) | |
| Bystander cardiopulmonary resuscitation | |||
| Yes | 4418 (46.8) | 4690 (47.7) | 1.7 |
| Missing, No. | 1 | 24 | |
| Bystander defibrillation with automated external defibrillator | |||
| Yes | 766 (8.1) | 565 (5.7) | 9.4 |
| Missing, No. | NA | 1 | |
| EMS treatment time intervals, median (IQR)b | |||
| Time from 911 call to EMS arrival | 8.5 (6.5-11.3) | 9.0 (6.9-12.0) | 0.5 |
| Duration of EMS treatment | 22.2 (15.0-32.0) | 24.8 (16.7-37.0) | 3.4 |
Abbreviations: EMS, emergency medical services; IQR, interquartile range; NA, not applicable.
Given the large sample size, P values are not reported. Instead, standardized differences of more than 10% are used to denote a meaningful difference between 2020 vs 2019.
Data were missing in 23% of patients for the interval from 911 call to EMS arrival and 50% of patients for duration of EMS treatment.
The overall rate of sustained ROSC for OHCA during the pandemic period in 2020 was 23.0% vs 29.8% during the same period in 2019 and remained lower after model adjustment (adjusted rate ratio [RR], 0.82 [95% CI, 0.78-0.87]; P < .001). A significant interaction was found between year and the county-level COVID-19 mortality rate (Figure 2). Among counties with high and very high COVID-19 mortality, rates of sustained ROSC were 21% lower (286 of 1429 [20.0%] in 2020 vs 305 of 1130 [27.0%] in 2019; adjusted RR, 0.79 [95% CI, 0.65-0.97]) and 33% lower (149 of 863 [17.3%] in 2020 vs 192 of 667 [28.8%] in 2019; adjusted RR, 0.67 [95% CI, 0.56-0.80]), respectively; however, rates of sustained ROSC were also 11% lower (583 of 2317 [25.2%] in 2020 vs 740 of 2549 [29.0%] in 2019; adjusted RR, 0.89 [95% CI, 0.81-0.98]) to 15% lower (889 of 3495 [25.4%] in 2020 vs 1109 of 3532 [31.4%] in 2019; adjusted RR, 0.85 [95% CI, 0.78-0.93]) in communities with very low and low COVID-19 mortality (interaction P = .03; eTable 2 in the Supplement). In contrast, overall rates of termination of resuscitation in the field were higher in 2020 compared with 2019 during the pandemic period (5314 of 9863 [53.9%] vs 3768 of 9440 [39.9%]) and remained 27% (95% CI, 23%-33%) higher in 2020 after model adjustment (Figure 2; eTable 3 in the Supplement). Termination rates increased the most in communities with high and very high COVID-19 mortality rates (adjusted RR, 1.40 [95% CI, 1.26-1.55] and 1.83 [95% CI, 1.62-2.05], respectively) but were also 12% to 24% higher in communities with the lowest COVID-19 mortality (interaction P < .001).
Figure 2. Rates of Sustained Return of Spontaneous Circulation (ROSC), Termination of Resuscitation, and Survival to Discharge During the 2020 Pandemic Period vs 2019.

Comparisons of rates are shown for the overall cohort and stratified by the county-level coronavirus disease 2019 (COVID-19) mortality rate. The analysis for the outcome of survival to discharge was restricted to emergency medical services agencies with complete data on this outcome. RR indicates rate ratio.
Data on survival to discharge were complete in 468 of 783 EMS agencies (59.8%). There was a total of 7025 OHCAs (3393 in 2019 and 3632 in 2020) during the pandemic period from these 468 agencies. Overall, rates of survival to discharge were 6.6% (239 of 3632 individuals) in 2020 compared with 9.8% (332 of 3393 individuals) in 2019 and were 17% lower after model adjustment (adjusted RR, 0.83 [95% CI, 0.69-1.00]; P = .048). Rates of survival to discharge during the pandemic period were lower only in counties with a COVID-19 mortality rate of more than 100 deaths per million residents (101-250 deaths per million: RR, 0.54 [95% CI, 0.36-0.79]; 251-500 deaths per million: RR, 0.71 [95% CI, 0.43-1.20]; >500 deaths per million: RR, 0.67 [95% CI, 0.42-1.05]) and were unchanged in counties with very low or low COVID-19 mortality (interaction P = .049) (Figure 2; eTable 4 in the Supplement).
Notably, the incidence rate of OHCA was higher overall during the pandemic period compared with 2019 (mean [SD], 88.5 [64.1] vs 69.7 [49.8] cardiac arrests per million residents; P < .001). After adjustment, communities with high or very high COVID-19 mortality rates had a 52% increase in OHCA incidence (incidence rate ratio, 1.52) during the pandemic period compared with the same period in 2019 (Table 2). In communities with low or very low COVID-19 mortality, however, OHCA incidence was only marginally higher in 2020 (incidence rate ratio range, 1.05-1.26).
Table 2. Incidence Rate of Out-of-Hospital Cardiac Arrest (OHCA) During the 2020 Pandemic Period vs 2019, Overall and Stratified by County-Level Coronavirus Disease 2019 (COVID-19) Mortality Ratea.
| Variable | Unadjusted OHCA incidence, mean (SD), per 1 000 000 residents | Adjusted mean difference in incidence (95% CI) | P value | Incidence rate ratio | |
|---|---|---|---|---|---|
| 2020 | 2019 | ||||
| Overall | 88.5 (64.1) | 69.7 (49.8) | 14.8 (14.2-15.3) | <.001 | 1.21 |
| County-level COVID-19 mortality rate per million residents | |||||
| 0-25 | 86.7 (47.8) | 79.7 (43.8) | 4.3 (3.2-5.4) | <.001 | 1.05 |
| 26-100 | 64.1 (43.2) | 57.7 (41.5) | 6.9 (6.0-7.9) | <.001 | 1.12 |
| 101-250 | 111.6 (81.9) | 83.8 (63.3) | 22.0 (20.7-23.3) | <.001 | 1.26 |
| 251-500 | 121.0 (65.2) | 73.9 (49.8) | 38.6 (37.1-40.1) | <.001 | 1.52 |
| >500 | 90.9 (85.1) | 55.5 (57.2) | 28.7 (26.7-30.6) | <.001 | 1.52 |
The adjusted mean difference in OHCA incidence was derived from hierarchical linear regression models and therefore is not simply the difference in unadjusted OHCA incidence between 2020 and 2019.
As additional controls for the pandemic period findings, we compared 2020 vs 2019 rates of sustained ROSC and survival to discharge during the prepandemic period of January through February and the peripandemic period of March 1 through 15. Rates of both outcomes were similar in 2020 compared with 2019 during both of these nonpandemic periods, overall and when counties were analyzed by their COVID-19 mortality rate during the pandemic period (Figure 3; eTable 5 in the Supplement).
Figure 3. Comparison of 2020 vs 2019 Rates of Sustained Return of Spontaneous Circulation (ROSC) and Survival to Discharge During the Prepandemic, Peripandemic, and Pandemic Periods.
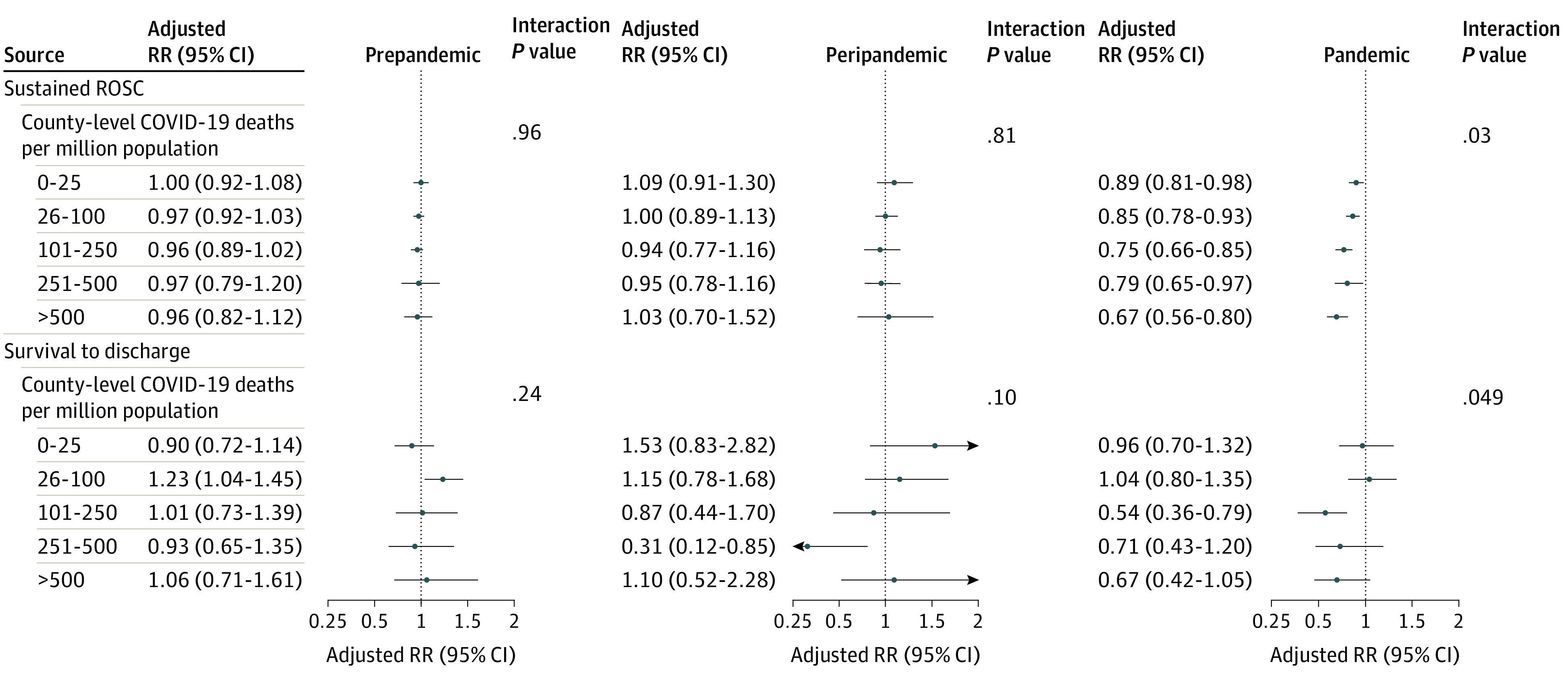
The analysis for the outcome of survival to discharge was restricted to emergency medical services agencies with complete data on this outcome. The prepandemic period was January through February; the peripandemic period, March 1 through 15; and the pandemic period, March 16 through April. COVID-19 indicates coronavirus disease 2019; RR, rate ratio.
Discussion
During the first weeks of the COVID-19 pandemic in the US, the likelihood of sustained ROSC after an OHCA decreased by 18% and the likelihood of termination of resuscitation in the field increased by 27% when compared with the same period in 2019. Although these patterns were more prominent in counties most affected by the COVID-19 pandemic, lower rates of sustained ROSC and higher rates of termination of resuscitation were also observed in counties with low COVID-19 mortality rates, despite only small increases in the incidence of OHCA in these less-affected communities. Rates of survival to discharge were also lower during the pandemic period compared with 2019, especially in communities with more than 100 COVID-19 deaths per million residents during the study period. Collectively, our findings provide more granular information on the association between the COVID-19 pandemic and OHCA outcomes in the US, even among communities not severely affected by COVID-19.
To date, there have been limited reports on the association between the COVID-19 pandemic and OHCA outcomes from regions such as northern Italy and New York, New York.1,2 Although these studies found marked increases in cardiac arrest incidence and lower rates of sustained ROSC compared with 2019, these regions were severely affected early during the pandemic and had exceptionally high COVID-19 incidence. Based on county-level data, there were 2135 deaths per million residents in New York, New York, during the study’s pandemic period. Thus, it is not unexpected that this surge would affect EMS treatment outcomes for emergency conditions such as OHCA in these locations. Yet, little is known about the association of the COVID-19 pandemic on OHCA outcomes in less-affected communities. Moreover, these initial reports did not contain information on survival to discharge, and lower rates of sustained ROSC and higher termination rates in the field may simply represent more appropriate decision-making of OHCA patients during the pandemic.
Our findings extend our understanding of the COVID-19 pandemic and OHCA outcomes in 2 main ways. First, we found that rates of sustained ROSC were lower in all communities, even in those with low COVID-19 mortality rates, where OHCA incidence was only marginally higher. Second, in the 60% of EMS agencies with complete data on survival to discharge, we found that rates of survival to discharge were lower, primarily in communities that were moderately to severely affected by COVID-19.
Several possible factors may explain our findings. With marked decreases in hospitalization for myocardial infarction, heart failure, and noncardiac conditions during the pandemic period,12,13,14,15,16 some have suggested that delayed medical care during the national lockdown in the US could have contributed to higher cardiac arrest and death rates at home and, if resuscitation was attempted, lower rates of sustained ROSC. To support this, we found large increases in OHCA incidence in areas most severely affected by COVID-19. However, delays in seeking medical care during the lockdown may not entirely explain the 11% to 15% lower rates of sustained ROSC that we observed in communities with low COVID-19 mortality rates, because the incidence of OHCA did not increase substantially in these communities. It is also possible that lower rates of bystander CPR and defibrillation, longer response intervals for EMS arrival, and shorter duration of EMS treatment during the pandemic could explain our findings, but we found that each of these parameters were similar to those during the same period in 2019. And although there were higher rates of OHCAs occurring at home and with an initial nonshockable rhythm during the pandemic period, rates of sustained ROSC and survival to discharge remained lower after adjustment for these differences.
This raises the possibility of whether protocols that were rapidly put into place following the beginning of the pandemic could have influenced patients’ likelihood of achieving sustained ROSC. For instance, the US Centers for Disease Control and Prevention17 and the American Heart Association18 each established interim guidelines for EMS and its professionals during the pandemic, which included screening 911 calls for likelihood of COVID-19 infection, limiting the number of EMS personnel during initial response, pausing critical chest compressions during aerosolizing procedures such as intubation, limiting bag-mask ventilation when done without specialized filtration, and not transporting patients to hospitals without ROSC. Many of these recommendations are believed to be essential for protecting frontline health care workers from unnecessary exposure in communities severely affected by the COVID-19 pandemic but may also decrease the likelihood of a successful resuscitation. Whether these recommendations may have been implemented more broadly than communities severely affected by COVID-19 and whether such practices affected rates of successful resuscitation deserve further study.
Limitations
Our study should be interpreted in the context of the following limitations. First, data on our outcome of survival to discharge were restricted to 60% of the EMS agencies with complete data on hospital outcomes (because 2020 CARES data on overall survival can be submitted until March 2021); therefore, this outcome should be interpreted with some caution. Second, granular information on quality of CPR (eg, chest compression quality) and reason for termination of resuscitation (eg, futility, COVID-19 policy, patient preference) were not available and may have explained study results if EMS resuscitation practices differed by county-level COVID-19 disease severity. Third, our study was limited to EMS agencies participating in CARES, and our findings may not be generalizable to nonparticipating agencies. Finally, we assessed the association between the COVID-19 pandemic and OHCA outcomes during the initial period of March 16 through April 30. Whether rates of sustained ROSC and survival to discharge continued to be lower in counties with contemporaneously low to moderate COVID-19 disease burden after this period remains critical to understand, especially because the COVID-19 pandemic in the US has shifted across regions over time.
Conclusions
In conclusion, we found that rates of sustained ROSC were lower throughout the US during the initial weeks of the COVID-19 pandemic, even in communities with low COVID-19 mortality rates. However, rates of survival to discharge were lower only in communities with moderate or high COVID-19 mortality.
eTable 1. Rate of Bystander CPR in Non-Healthcare Facilities and Bystander AED Use in Public Locations.
eTable 2. Rates of Sustained ROSC During the 2020 Pandemic Period vs. 2019, Stratified by the County-Level COVID-19 Incidence Rate.
eTable 3. Rates of Termination of Resuscitation During the 2020 Pandemic Period vs. 2019, Stratified by the County-Level COVID-19 Mortality Rate.
eTable 4. Rates of Survival to Discharge During the 2020 Pandemic Period vs. 2019, Stratified by the County-Level COVID-19 Mortality Rate.
eTable 5. Comparison of 2020 vs. 2019 Outcomes During the Pre-Pandemic, Peri-Pandemic, and Pandemic Periods.
References
- 1.Lai PH, Lancet EA, Weiden MD, et al. Characteristics associated with out-of-hospital cardiac arrests and resuscitations during the novel coronavirus disease 2019 pandemic in New York City. JAMA Cardiol. 2020;(Jun):19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Baldi E, Sechi GM, Mare C, et al. ; Lombardia CARe Researchers . Out-of-hospital cardiac arrest during the COVID-19 outbreak in Italy. N Engl J Med. 2020;383(5):496-498. doi: 10.1056/NEJMc2010418 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Marijon E, Karam N, Jost D, et al. Out-of-hospital cardiac arrest during the COVID-19 pandemic in Paris, France: a population-based, observational study. Lancet Public Health. 2020;5(8):e437-e443. doi: 10.1016/S2468-2667(20)30117-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.McNally B, Stokes A, Crouch A, Kellermann AL; CARES Surveillance Group . CARES: Cardiac Arrest Registry to Enhance Survival. Ann Emerg Med. 2009;54(5):674-683.e2. doi: 10.1016/j.annemergmed.2009.03.018 [DOI] [PubMed] [Google Scholar]
- 5.McNally B, Robb R, Mehta M, et al. Out-of-hospital cardiac arrest surveillance—Cardiac Arrest Registry to Enhance Survival (CARES), United States, October 1, 2005–December 31, 2010. MMWR Surveill Summ. 2011;60:1-19. [PubMed] [Google Scholar]
- 6.Jacobs I, Nadkarni V, Bahr J, et al. ; International Liaison Committee on Resuscitation; American Heart Association; European Resuscitation Council; Australian Resuscitation Council; New Zealand Resuscitation Council; Heart and Stroke Foundation of Canada; InterAmerican Heart Foundation; Resuscitation Councils of Southern Africa; ILCOR Task Force on Cardiac Arrest and Cardiopulmonary Resuscitation Outcomes . Cardiac arrest and cardiopulmonary resuscitation outcome reports: update and simplification of the Utstein templates for resuscitation registries: a statement for healthcare professionals from a task force of the International Liaison Committee on Resuscitation (American Heart Association, European Resuscitation Council, Australian Resuscitation Council, New Zealand Resuscitation Council, Heart and Stroke Foundation of Canada, InterAmerican Heart Foundation, Resuscitation Councils of Southern Africa). Circulation. 2004;110(21):3385-3397. doi: 10.1161/01.CIR.0000147236.85306.15 [DOI] [PubMed] [Google Scholar]
- 7.New York Times . COVID-19 data. Published 2020. Accessed May, 15, 2020.https://github.com/nytimes/covid-19-data/blob/master/us-counties.csv
- 8.Department of Housing and Urban Development Office of Policy Development and Research (PD&R) . USPS crosswalk API. Accessed June 11, 2020. https://www.huduser.gov/portal/dataset/uspszip-api.html
- 9.Austin PC. Using the standardized difference to compare the prevalence of a binary variable between two groups in observational research. Communications in Statistics—Simulation and Computation. 2009;38:1228-1234. doi: 10.1080/03610910902859574 [DOI] [Google Scholar]
- 10.Greenland S. Model-based estimation of relative risks and other epidemiologic measures in studies of common outcomes and in case-control studies. Am J Epidemiol. 2004;160(4):301-305. doi: 10.1093/aje/kwh221 [DOI] [PubMed] [Google Scholar]
- 11.Zou G. A modified Poisson regression approach to prospective studies with binary data. Am J Epidemiol. 2004;159(7):702-706. doi: 10.1093/aje/kwh090 [DOI] [PubMed] [Google Scholar]
- 12.De Filippo O, D’Ascenzo F, Angelini F, et al. Reduced rate of hospital admissions for ACS during COVID-19 outbreak in northern Italy. N Engl J Med. 2020;383(1):88-89. doi: 10.1056/NEJMc2009166 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Hall ME, Vaduganathan M, Khan MS, et al. Reductions in heart failure hospitalizations during the COVID-19 pandemic. J Card Fail. 2020;26(6):462-463. doi: 10.1016/j.cardfail.2020.05.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Gluckman TJ, Wilson MA, Chiu ST, et al. Case rates, treatment approaches, and outcomes in acute myocardial infarction during the coronavirus disease 2019 pandemic. JAMA Cardiol. Published August 7, 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Anderson TS, Stevens JP, Pinheiro A, Li S, Herzig SJ. Hospitalizations for emergent medical, surgical, and obstetric conditions in Boston during the COVID-19 pandemic. J Gen Intern Med. 2020;35(10):3129-3132. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Jasne AS, Chojecka P, Maran I, et al. Stroke code presentations, interventions, and outcomes before and during the COVID-19 pandemic. Stroke. 2020;51(9):2664-2673. doi: 10.1161/STR.0000000000000347 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.US Centers for Disease Control and Promotion . Interim recommendations for emergency medical services (EMS) systems and 911 public safety answering points/emergency communication centers (PSAP/ECCs) in the United States during the coronavirus disease (COVID-19) pandemic. Published 2020. Accessed August 21, 2020. https://www.cdc.gov/coronavirus/2019-ncov/hcp/guidance-for-ems.html
- 18.Edelson DP, Sasson C, Chan PS, et al. ; American Heart Association ECC Interim COVID Guidance Authors . Interim guidance for basic and advanced life support in adults, children, and neonates with suspected or confirmed COVID-19: from the Emergency Cardiovascular Care Committee and Get With The Guidelines–Resuscitation Adult and Pediatric Task Forces of the American Heart Association. Circulation. 2020;141(25):e933-e943. doi: 10.1161/CIRCULATIONAHA.120.047463 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
eTable 1. Rate of Bystander CPR in Non-Healthcare Facilities and Bystander AED Use in Public Locations.
eTable 2. Rates of Sustained ROSC During the 2020 Pandemic Period vs. 2019, Stratified by the County-Level COVID-19 Incidence Rate.
eTable 3. Rates of Termination of Resuscitation During the 2020 Pandemic Period vs. 2019, Stratified by the County-Level COVID-19 Mortality Rate.
eTable 4. Rates of Survival to Discharge During the 2020 Pandemic Period vs. 2019, Stratified by the County-Level COVID-19 Mortality Rate.
eTable 5. Comparison of 2020 vs. 2019 Outcomes During the Pre-Pandemic, Peri-Pandemic, and Pandemic Periods.