

Abstract
Objective:
To assess and quantify the effect of perioperative music on medication requirement, length of stay and costs in adult surgical patients.
Summary Background Data:
There is an increasing interest in nonpharmacological interventions to decrease opioid analgesics use, as they have significant adverse effects and opioid prescription rates have reached epidemic proportions. Previous studies have reported beneficial outcomes of perioperative music.
Methods:
A systematic literature search of 8 databases was performed from inception date to January 7, 2019. Randomized controlled trials investigating the effect of perioperative music on medication requirement, length of stay or costs in adult surgical patients were eligible. Meta-analysis was performed using random effect models, pooled standardized mean differences (SMD) were calculated with 95% confidence intervals (CI). This study was registered with PROSPERO (CRD42018093140) and adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analysis guidelines.
Results:
The literature search yielded 2414 articles, 55 studies (N = 4968 patients) were included. Perioperative music significantly reduced postoperative opioid requirement (pooled SMD −0.31 [95% CI −0.45 to −0.16], P < 0.001, I 2 = 44.3, N = 1398). Perioperative music also significantly reduced intraoperative propofol (pooled SMD −0.72 [95% CI −1.01 to −0.43], P < 0.00001, I 2 = 61.1, N = 554) and midazolam requirement (pooled SMD −1.07 [95% CI −1.70 to −0.44], P < 0.001, I 2 = 73.1, N = 184), while achieving the same sedation level. No significant reduction in length of stay (pooled SMD −0.18 [95% CI −0.43 to 0.067], P = 0.15, I 2 = 56.0, N = 600) was observed.
Conclusions:
Perioperative music can reduce opioid and sedative medication requirement, potentially improving patient outcome and reducing medical costs as higher opioid dosage is associated with an increased risk of adverse events and chronic opioid abuse.
Keywords: analgesia, medication requirement, music, opioids, perioperative patient care, propofol, sedation, surgery
A majority of patients continues to experience moderate to severe postoperative pain,1 which is a risk factor for delayed hospital discharge2 and the occurrence of postoperative complications,3,4 persisting chronic pain and the predominant factor for the immediate postsurgical quality of life.5 Opioid analgesics are the primary treatment modality for acute postoperative pain, which is the second most common reason to prescribe opioids.6 However, opioid-related side effects are common.7,8 Opioid use is considered a risk factor for pruritus, nausea, vomiting, drowsiness, urinary retention and the development of delirium.9 Higher opioid doses also increase the incidence of postoperative ileus and respiratory depression.10,11 Moreover, persistent opioid use in surgical patients is quite prevalent. Earlier studies reported that 5.9% of patients still filled an opioid prescription 3 to 6 months after minor surgical procedures,12 whereas over half of the patients receiving 90 days of continuous opioid medication still use opioid analgetics 1 year later.13 Both opioid prescription dosage and duration of use are important predictors for chronic opioid use.6 The concomitant use of benzodiazepines can potentially increase the risk of adverse effects, delirium, and prolonged opioid misuse even more.11
Despite these common adverse events and an increase in opioid-related deaths, opioid prescription rates have currently reached epidemic proportions.6 Therefore, there is an increasing interest in nonpharmacological interventions to reduce both postoperative pain and opioid consumption. Recently, several studies have reported beneficial effects of perioperative music.14,15,16 The purpose of this systematic review and meta-analysis is to assess and quantify the effect of perioperative music as a nonpharmacological intervention on medication requirement before, during and after invasive, surgical procedures. Secondary outcomes are the effect of perioperative music on length of stay and cost reduction.
METHODS
This systematic review and meta-analysis adheres to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines and has been registered with PROSPERO (CRD42018093140).
Literature Search Strategy
A literature search using the exhaustive literature search method was performed with a biomedical information specialist.17 The databases Embase, Medline Ovid, Web-of-science, Scopus, Cochrane central, Cinahl, PsychINFO Ovid, and Google Scholar were searched from date of inception until January 7th, 2019. The full search terms and number of search results of each database are detailed in Appendix A. Also, manual cross-referencing of the included studies was performed.
Study Screening and Selection
Three reviewers (V.F., P.O., and V.E.) independently identified eligible studies using a 2-stage approach. First, title and abstract of all identified papers screened, followed by reading of the full text if eligibility criteria were matched. Inclusion criteria for this systematic review were all available, peer-reviewed, full-text articles of randomized controlled trials in the English language, containing adult patients ≥18 years old undergoing an inhospital or outpatient invasive, surgical procedure, investigating the use of recorded music before, during and/or after surgery with either medication requirement, hospital length of stay or direct medical costs as outcome measures. As these predefined outcome measures were often secondary outcomes and therefore not always mentioned in titles or abstracts, the 3 reviewers screened all studies full text for potential review inclusion if during the title and abstract screening process music as a perioperative intervention in adult patients was investigated. The music intervention was predefined as vocal sound, instrumental sound or both, containing the elements melody, harmony, and rhythm. Therefore, studies investigating solely nature sounds were excluded. Studies investigating live music with a music therapist were also excluded, because of the possibility that the effect is caused by the presence of the musical therapist and the irreproducibility of the study. Finally, studies investigating music with an additional, concomitant intervention were excluded, except if this additional intervention was used in both the intervention and control group (for example, the music intervention occurred during bed rest, and the control group received only bed rest). Disagreements between the investigators were resolved by referring to the supervisor (J.J.).
Data Extraction
Study data were independently extracted by the 3 reviewers (V.F., P.O., and V.E.) using a custom, predesigned Microsoft Excel 2010 document. Risk of bias was also independently assessed using the Cochrane Collaboration's tool for assessing risk of bias in randomized trials.18 Authors of included studies were contacted for additional information if necessary. All data was mutually discussed and disagreements between the investigators were resolved by referring to the supervisor (J.J.).
Statistical Analysis
Data were analyzed with the open-source, meta-analysis software OpenMeta-Analyst, which uses R as the underlying statistical engine.19 Random effect models were used, because heterogeneity between the included studies was assumed to be present. Standardized mean differences (SMD) and absolute mean differences were calculated with 95% confidence interval (CI). Studies were included for meta-analysis if mean values and standard deviations (SDs) of the outcome measures were reported. Opioid doses were converted to milligrams (mg) of morphine equianalgesic (ME), with 1 mg ME being equivalent to 1 mg parenteral morphine. If interquartile ranges or ranges were reported, an approximation of the SD was calculated by dividing the interquartile range by 1.35 and the range by 4. When the standard error of mean was reported, SDs were calculated by multiplying the standard error of mean with the square root of the number of patients.18 Publication bias was visually assessed using funnel plots, if more than ten studies were included in the meta-analysis. Heterogeneity was analyzed using the I 2-test. Statistical significance was inferred at P-value <0.05.
If studies included several music groups, the means and SDs of the music groups were pooled to an approximated mean and SD of the entire group.18 If this was not appropriate, the music group that offered patients the choice to select from a preselected music list was preferred for meta-analysis. Choosing music from a preselected playlist has been observed to have a more beneficial effect on postoperative pain, compared to the own favorite music of the patient or preselected music without offering any choice.16 If studies included several control groups, only the group which resembled standard perioperative patient care the most was included for meta-analysis.
RESULTS
The literature search yielded 2414 results. A total of 1524 titles and abstracts were screened after removal of duplicates and 154 articles were assessed full text. Fifty-five studies (4968 patients) were included in the qualitative synthesis and 33 studies (2390 patients)20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53 in the meta-analysis (Fig. 1). There was a high agreement rate of over 85% between the 3 reviewers on study inclusion, risk of bias assessment, and data extraction, and all disagreements could be resolved through mutual discussion.
FIGURE 1.
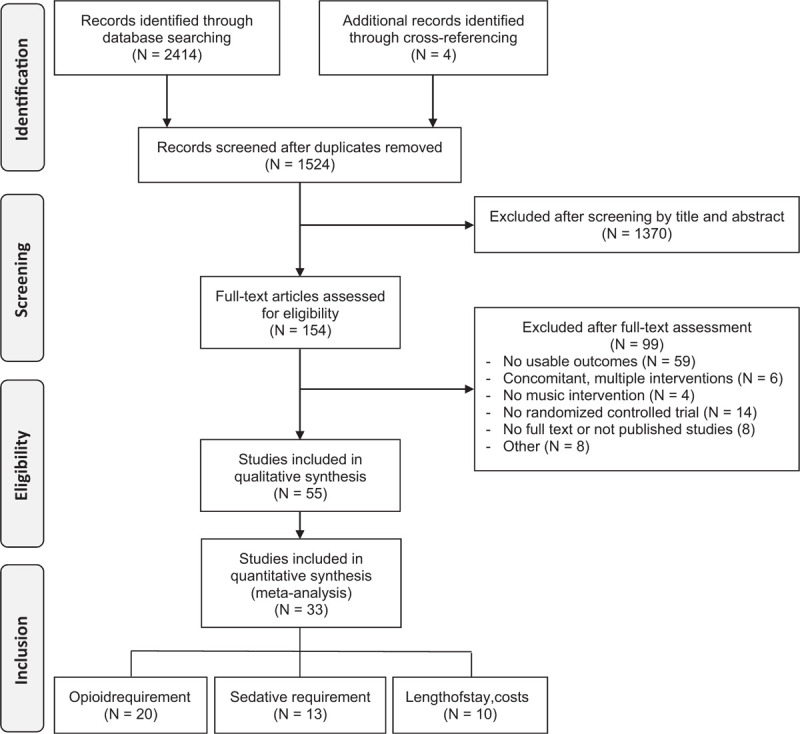
PRISMA Flow diagram. N indicates number of studies.
Study Characteristics
A detailed overview of the study characteristics is presented in Table 1. The music intervention was assessed in a wide range of different surgical procedures. General anesthesia was the most commonly used anesthesia method during surgery in 36 studies (65%), whereas locoregional anesthesia was used in 8 studies (15%). Eight studies (15%) did not report the anesthesia method used and 3 studies (5.5%) contained different surgical procedures with different anesthesia methods. The moment of music intervention varied. Music was played solely preoperatively in 3 (5.5%), intraoperatively in 10 (18%), postoperatively in 25 (45%), and on multiple moments in 15 studies (27%). Two studies by the same author contained both an intraoperative music intervention group and a second music intervention group in which the intervention was solely applied postoperatively.
TABLE 1.
Study Characteristics
| Study ID | Surgical Procedure | Anesthesia | Intervention | Moment | Duration | N | Control | N | Outcome Parameters |
| Allred, 2010 | Total knee arthroplasty | General or spinal with femoral block | Choice of easy listening, nonlyrical music | Postoperatively | POD 1, 20 min before and after first ambulation | 28 | Quiet rest period | 28 | Postoperative opioid requirement |
| Ames, 2017 | Surgical procedures requiring ICU stay | General | MusiCure | Postoperatively | POD 1-2, 50 min, 1-8 times | 20 | 50 min quiet rest | 21 | Postoperative opioid requirement |
| Ayoub, 2005∗ | Urological procedures | Regional | Own favorite music | Intraoperatively | Procedure duration | 31 | Headphones with operation noise recording | 28 | Intraoperative propofol requirement |
| PACU length of stay | |||||||||
| Bansal, 2010∗ | Abdominal, urological, or lower extremity surgery | Spinal | Choice of folk, classical, religious, soothing music | Intraoperatively | Not specified | 50 | Occlusive headphones | 50 | Intraoperative midazolam requirement |
| Binns-Turner, 2011 | Mastectomy | General | Choice of classical, easy-listening, new age, inspirational music | PreoperativelyIntraoperativelyPostoperatively | Not specified | 15 | Blank iPOD with occlusive headphones | 15 | Intraoperative opioid requirementPostoperative opioid requirementPACU length of stay |
| Blankfield, 1995∗ | Coronary artery bypass surgery | General | Dreamflight II by Herb Ernst | IntraoperativelyPostoperatively | Procedure duration and 2 × 30 min daily postoperatively | 32 | Blank tape intraoperatively and standard care postoperatively | 29 | Postoperative opioid requirementICU length of stayHospital length of stay |
| Chen, 2015∗ | Total knee replacement | Not specified | Chinese piano and violin music | PreoperativelyPostoperatively | Total 120 min | 15 | Standard care | 15 | Postoperative opioid requirement |
| Ciğerci and Özbayir, 2016∗ | Coronary artery bypass surgery | General | Choice of Turkish classical and folk music | PreoperativelyPostoperatively | 90 min before surgery, after surgery 30 min in ICU and 30 min each day | 34 | Standard care | 34 | Postoperative opioid requirement |
| Cutshall, 2011∗ | Coronary artery bypass graft and/or cardiac valve surgery | General | Choice of 4 CD's | Postoperatively | 2 × 20 min on POD 2–4, 120 min in total | 49 | Standard care with bed rest for 20 min | 51 | Postoperative opioid requirementHospital length of stay |
| Dabu-Bondoc, 2010∗ | Outpatient surgery | General | Own favorite music | Preoperatively Intraoperatively | Preoperative 30 min, procedure duration | 20 | Intraoperatively headphones with white noise | 20 | Intraoperative propofol requirementIntraoperative opioid requirementPostoperative opioid requirementPACU length of stay |
| Easter, 2010 | Elective outpatient surgery procedures | Not specified | Choice of easy-listening, country, gospel, rock | Postoperatively | During length of stay in PACU | 111 | No music | 102 | Postoperative opioid requirementPACU length of stay |
| Ebneshahidi and Mohseni, 2008∗ | Elective cesarean section surgery | General | Own favorite music | Postoperatively | 30 min in the recovery room | 38 | Headphones without music | 39 | Postoperative opioid requirement |
| Finlay, 2016 | Total knee arthroplasty | Spinal with nerve block | 32 tracks with range of genres | Postoperatively | 15 min | 72 | Headphones without music | 17 | Postoperative opioid requirement |
| Good, 1995∗ | Elective, open abdominal surgery | General | Choice of sedative nonlyrical piano, harp, synthesizer orchestral or slow jazz music | Postoperatively | 60 min during the first 2 d after surgery | 21 | Standard care | 21 | Postoperative opioid requirement |
| Good, 1999 | Elective, open, major abdominal surgery | General | Choice of taped soothing music | PreoperativelyPostoperatively | First 2 d after surgery | 151 | Standard care | 152 | Postoperative opioid requirement |
| Graversen and Sommer, 2013∗ | Laparoscopic cholecystectomy | General | Musicure using music pillow | PreoperativelyIntraoperativelyPostoperatively | Before surgery start until day care discharge | 40 | Standard care | 35 | Intraoperative propofol requirementIntraoperative opioid requirementPostoperative opioid requirementDay care unit length of stay |
| Heitz, 1992∗ | (Para)thyroidectomy or unilateral modified radical mastectomy | General | Choice of 3 instrumental classical tapes | Postoperatively | 15 min after PACU arrival until discharge | 20 | Headphones without music | 20 | Postoperative opioid requirement |
| Standard care | 20 | PACU length of stay | |||||||
| Hook, 2008∗ | Moderate or major elective surgery | General | Choice of Malay, Western, Chinese, soothing music | Preoperatively Postoperatively | 60 min before and 180 min after surgery | 51 | Standard care | 51 | Postoperative opioid requirement |
| Iblher, 2011 | Open heart surgery (coronary bypass, valvular transplant, or both combined) | General | Baroque organ, flute, string orchestra music with 60-80 bpm | Postoperatively | 60 min after ICU admission | 25 | Standard care | 25 | Postoperative opioid requirement |
| 60 min after sedation stop | 24 | Postoperative catecholamine requirement | |||||||
| Ignacio, 2012 | Elective spine, hip or knee surgery | General | Not specified | Postoperatively | 2 × 30 min | 12 | No music | 9 | Postoperative opioid requirement |
| Ikonomodou, 2004∗ | Laparoscopic sterilization or tubal dyeing | General | Peaceful pan flute music | PreoperativelyPostoperatively | 30 min before and after surgery | 29 | Blank compact disk | 26 | Postoperative opioid requirement |
| Johnson, 2012 | Gynaecological outpatient surgery | Not specified | Choice of soft country, classical/new age and inspirational music | PreoperativelyIntraoperativelyPostoperatively | On average 212 min | 43 | Headphones without music | 35 | Postoperative opioid requirement |
| Standard care | 41 | PACU length of stay | |||||||
| Kar, 2015∗ | Elective cardiac surgery under cardiopulmonary bypass | General | Raga therapy (Indian classical music) | Preoperatively Intraoperatively | 30 min before surgery and procedure duration | 17 | Headphones without music | 17 | Intraoperative sedative requirement Intraoperative opioid requirement |
| Kliempt, 1999 | Diverse range of surgical procedures | General | Classical music Adagio Karajan | Intraoperatively | Procedure duration | 25 | Headphones without music | 26 | Intraoperative opioid requirement |
| Koch, 1998∗ | Outpatient urological procedures | Spinal | Own favorite music | Intraoperatively | Procedure duration | 19 | Standard care | 15 | Intraoperative propofol requirementPACU length of stay |
| Koelsch, 2011∗ | Total hip arthroplasty | Spinal | Joyful instrumental music | Preoperatively Intraoperatively | 120 min beforesurgery and procedure duration | 20 | Headphones with breaking sea waves noise | 20 | Intraoperative propofol requirement |
| Kumar, 2014 | Hernia, breast, appendix and thyroid surgery | Not specified | Raga Ananda Bairavi (Indian classical music) | Preoperatively Postoperatively | At admission and POD 1–3 | 30 | Standard care | 30 | Postoperative opioid requirement |
| Laurion and Fetzer, 2003 | Gynecological, laparoscopic outpatient day surgery | General | Piano music | PreoperativelyIntraoperativelyPostoperatively | 2 times a day before surgery, procedure duration, PACU stay | 28 | Standard care | 28 | Postoperative opioid requirementPACU length of stay |
| Lepage, 2001∗ | Nononcologic, outpatient or short-stay surgery | Spinal | Choice of pop, jazz, classical, new age | PreoperativelyIntraoperativelyPostoperatively | Anesthesia induction until recovery | 25 | Standard care | 25 | Perioperative midazolam requirement |
| Liu and Petrini, 2015 | Thoracic surgery | General | Soft, melodious music 60-80 bpm | Postoperatively | 30 min daily on POD 1–3 | 56 | Standard care | 56 | Postoperative patient-controlled analgesia requirement |
| Macdonald, 2003 | Total abdominal hysterectomy | Not specified | Own favorite music | Postoperatively | 2–6 h on day of surgery | 30 | Standard care | 28 | Postoperative patient-controlled analgesia requirement |
| Masuda, 2005∗ | Orthopedic surgery | General and spinal | Choice of Noh, Gagaku, classical or Enka music | Postoperatively | 20 min | 22 | Standard care | 22 | Hospital length of stay |
| McCaffrey and Loscin, 2006 | Elective hip or knee surgery | Not specified | Choice of CD's | Postoperatively | 60 min 4 times a day | 62 | Standard care | 62 | Postoperative patient-controlled analgesia requirement |
| McRee, 2003 | ‘Low risk’ surgery | General, spinal, local and regional | Soft piano music | Preoperatively | 30 min | 13 | Standard care | 13 | Postoperative opioid requirement |
| Migneault, 2004∗ | Gynaecological surgery | General | Choice of jazz, classical, popular new-age or piano music | Intraoperatively | Procedure duration | 15 | Headphones without music | 15 | Intraoperative end-tidal isofluraneIntraoperative fentanyl requirementPostoperative opioid requirement |
| Miladinia, 2017∗ | Abdominal surgery | General | Relaxing nonlyrical music with a bpm of 60–80 | Postoperatively | 3 × 10 min sessions on day of surgery | 30 | Standard care | 30 | Postoperative opioid requirement |
| Nielsen, 2018∗ | Unspecified orthopedic, urological, gynaecological and general surgery | Epidural, spinal and local | Musicure | Intraoperatively | Procedure duration | 58 | Standard care | 44 | Intraoperative fentanyl requirementIntraoperative propofol requirement |
| Nilsson, 2001∗ | Elective abdominal hysterectomy | General | Relaxing, calming music with sea waves sound | Intraoperatively | Procedure duration | 30 | Headphones with operation noise recording | 28 | Postoperative opioid requirement Hospital length of stay |
| Nilsson, 2003a∗ | Daycare surgery: varicose veins, open inguinal hernia repair | General | Soft, relaxing and calming classical music | Postoperatively | PACU arrival until patient chose to stop | 62 | Headphones without music | 63 | Postoperative opioid requirement |
| Nilsson, 2003b∗ | Daycare surgery: varicose veins, open inguinal hernia repair | General | Soft instrumental new-age synthesizer music | Intraoperatively | Procedure duration | 51 | Headphones without music | 49 | Postoperative opioid requirement |
| Postoperatively | 1 h after PACU arrival | 51 | |||||||
| Nilsson, 2005∗ | Open hernia repair (Lichtenstein) | General | Soft, new-age synthesizer | Intraoperatively | Procedure duration | 25 | Headphones without music | 25 | Postoperative opioid requirement |
| Postoperatively | 1 h after PACU arrival | 25 | |||||||
| Nilsson, 2009a | Coronary artery bypass graft and/or aortic valve replacement | General | MusiCure using music pillow | Postoperatively | 30 min on POD1 | 20 | Standard care | 20 | Postoperative opioid requirement |
| Nilsson, 2009b∗ | Coronary artery bypass graft or aortic valve replacement | General | Soft, relaxing, new age style music using music pillow | Postoperatively | 30 min on POD1 | 28 | Standard care | 30 | Postoperative opioid requirement |
| Reza, 2007∗ | Elective caesean section | General | Soft, instrumental, Spanish style guitar music | Intraoperatively | Procedure duration | 50 | White music | 50 | Postoperative opioid requirement |
| Santhna, 2015 | Total knee replacement surgery | Not specified | Choice of soothing and relaxing nonlyrical piano or violin music | Postoperatively | 60 min, 4 times a day | 20 | Standard care | 20 | Postoperative opioid requirement |
| Schwartz, 2009∗ | Coronary artery bypass graft surgery | General | Light piano music | Postoperatively | Patient's choice in ICU | 35 | Standard care | 32 | ICU length of stayHospital costs |
| Sen, 2009a∗ | Local urological procedures | Propofol PCS with local infiltration | Own favorite music | Intraoperatively | Procedure duration | 30 | Earphones without music | 30 | Intraoperative propofol requirement |
| Sen, 2009b∗ | Elective caesarian section | General | Own favorite music | Preoperatively | 60 min | 50 | Headphones without music | 50 | Postoperative opioid requirement |
| Sen, 2010∗ | Elective caesarian section | General | Own favorite music | Postoperatively | 60 min | 35 | No music | 35 | Postoperative opioid requirement |
| Szmuk, 2008 | Laparoscopic hernia or cholecystectomy | General | Choice of pop-rock, classical or Israeli music | Intraoperatively | Procedure duration | 20 | Headphones without music | 20 | Intraoperative end-tidal sevoflurane Postoperative opioid requirement |
| Tse, 2005 | Endoscopic sinus surgery or tubinectomy | Not specified | Choice of Chinese, Western or own favorite music | Postoperatively | 2 × 30 min after surgery and on POD1 | 27 | Standard care | 30 | Postoperative analgesic medication requirement |
| Vaajoki, 2012 | Elective major abdominal midline incision surgery | General | Choice of 2000 popular music songs | Postoperatively | Total of 7 × 30 min | 83 | Standard care | 85 | Postoperative opioid requirementHospital length of stay |
| Zhang, 2005∗ | Total abdominal hysterectomy | General with spinal or epidural | Own favorite music | Intraoperatively | Procedure duration | 55 | Headphones without music | 55 | Intraoperative propofol requirement |
| Zhou, 2011∗ | Radical mastectomy | General | Choice of 202 songs | Postoperatively | 2 × 30 min daily | 60 | Standard care | 60 | Hospital length of stay |
| Zimmerman, 1996 | Coronary artery bypass graft surgery | General | Choice of 5 soothing music tapes | Postoperatively | 30 min daily during POD1-3 | 32 | Scheduled rest of 30 min | 32 | Postoperative opioid requirement |
| Hospital length of stay |
Denotes study included in meta-analysis.
CD indicates compact disk; ICU, intensive care unit; Min, minutes; N, number of patients; PACU, post-anesthesia care unit; PCS, patient-controlled sedation; POD, postoperative day; d, days; h, hours.
The music intervention was commonly described as soothing, relaxing, nonlyrical, instrumental music and was preselected by the research team in most studies (45 studies, 82%): patients could select music from a preselected list in 21 studies (38%), whereas no choice was offered in 24 studies (44%). The preferred music of the patient was used in 9 studies (16%), whereas 1 study (1.8%) did not elaborate on the exact music intervention. In a majority of studies, music delivery was achieved using a music player and headphones (41 studies, 75%). Other reported music delivery methods were a music pillow (3 studies, 5.5%), CD-player (3 studies, 5.5%), personal stereo (1 study, 1.8%), an integrated music system in the patient room (1 study, 1.8%), or not specified (6 studies, 11%). The control group consisted of standard care (26 studies, 47%), headphones without music (16 studies, 29%), headphones with white noise or recorded OR noise intraoperatively (5 studies, 9.1%), no music without further specification (3 studies, 5.5%), or an unspecified rest period (3 studies, 5.5%). Two studies (3.6%) had both a standard care and headphones without music group acting as control.
Risk of Bias Assessment
An overview of the risk of bias assessment is presented in Fig. 2 and a more detailed description in Appendix B. A potentially high risk of selection bias was present in several studies (8 studies, 15%),24,29,47,54,55,56,57,58 as sequence generation was done using odd and even numbers, days of the week or hospital record number. Several studies provided insufficient details to assess selection bias (14 studies, 25%).20,22,26,27,28,30,32,36,38,40,59,60,61,62 A moderate to high risk of performance bias was present, as blinding of patients for the music intervention is only possible when the intervention is performed solely intraoperatively during general anesthesia. Blinding of personnel can theoretically be achieved by using headphones for all patients, but is more difficult in practice when patients are free to change music tracks or adjust the volume. Five studies (9.3%) employed a study design in which patients, surgical personnel and outcome assessors were all blinded adequately.38,41,46,63,64 The “other risk of bias” category was reported as unclear in more than half of the studies (36 studies, 65%), because one of the baseline characteristics age, sex, weight, or the duration of surgery, which can influence intraoperative and postoperative medication requirement, was not reported. There was a high risk of other bias because of significant difference in either surgery duration or age between the music and control group in 3 studies.25,36,45 A funnel plot to investigate publication bias of studies assessing the effect of perioperative music on postoperative opioid requirement showed a near funnel-shaped plot, lacking a small number of studies in the lower-left corner which could be indicative of studies with relatively small samples sizes and small effect sizes being potentially absent (Appendix C).
FIGURE 2.
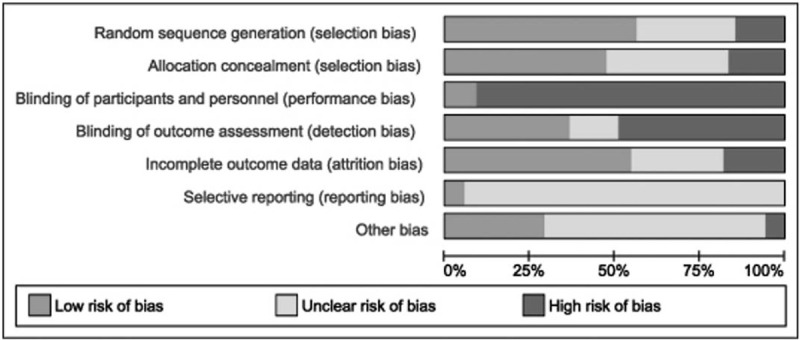
Risk of bias summary. Risk of bias summary graph.
Opioid Requirement
The effect of perioperative music on postoperative opioid requirement was assessed in 42 studies, of which 2022,23,24,26,27,28,29,30,31,32,38,39,41,42,43,45,46,49,50 could be included in the meta-analysis. Thirteen studies presented the postoperative opioid dose requirement as morphine equivalents (ME) or parenteral morphine. In 3 studies, postoperative ketobemidone requirement was evaluated, which are equipotent to parenteral morphine (1 mg parenteral ketobemidone = 1 mg ME65). Postoperative parenteral tramadol requirement (10 mg parenteral tramadol = 1 mg ME66) was assessed in 3 studies and pethidine requirement in 1 study (10 mg pethidine = 1 mg ME67). Length of follow-up differed, as 5 studies assessed opioid requirement during the stay in the post-anesthesia care unit,26,29,30,32,43 3 within the first 2 postoperative hours27,42,44 and 2 within the first 12 postoperative hours.39,46 Ten studies (50%) assessed opioid requirement for minimally 24 hours after surgery or longer.22,23,24,28,31,38,41,45,49,50 General anesthesia was used during surgery in all of these 20 studies.
Perioperative music significantly reduced postoperative opioid requirement (pooled SMD −0.31 [95% CI −0.45 to −0.16], P < 0.001, I 2 = 44.3, N = 1398 patients) (Fig. 3). The mean overall absolute reduction in postoperative opioid requirement of the 8 studies which measured postoperative opioid requirement during post-anesthesia care unit stay or within the first 2 postoperative hours was −1.0 mg ME (95% CI −1.6 to −0.49, P < 0.001, I 2 = 10.5, N = 698 patients). The mean absolute reduction in postoperative opioid requirement of the 10 studies which measured postoperative opioid requirement for at least 24 hours or more after surgery was −4.4 mg ME (95% CI −8.2 to −0.65, P = 0.022, I 2 = 69.6, N = 598 patients). The mean absolute reduction in 5 of these studies which measured opioid requirement for at least 3 postoperative days and involved major surgical procedures was −9.82 mg ME (95% CI −17.9 to −1.70, P = 0.018, I 2 = 48.8, N = 298 patients).22,23,24,31,41 Intraoperative music during general anesthesia in 3 of the 20 studies in which the patients, surgical staff, and outcome assessors were all blinded did not significantly reduce postoperative opioid requirement (pooled SMD −0.16 [95% CI −0.63 to 0.31], P = 0.49, I 2 = 57.1, N = 188 patients).38,41,46
FIGURE 3.
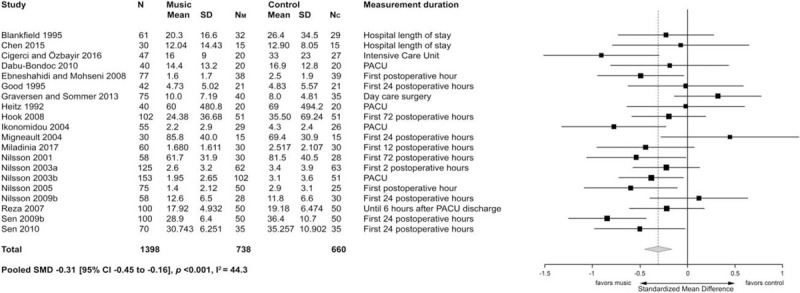
Effect of perioperative music on postoperative opioid requirement. Forest plot presenting the effect of perioperative music on postoperative opioid requirement (milligrams of morphine equianalgesics). CI indicates confidence interval; Mean, mean milligrams of morphine equianalgesics; N, total number of patients in study; NC, number of patients in the control group; NM, number of patients in the music group; PACU, post-anesthesia care unit; SD, standard deviation in milligrams of morphine equianalgesics; SMD, standardized mean difference.
The effect of preoperative and/or intraoperative music on intraoperative opioid requirement was assessed in 7 studies.23,26,29,33,38,40,63 Meta-analysis was not performed because of insufficient data presented, the broad variation in the types of surgery performed and difference in surgery duration.
Intraoperative Sedative Requirement
The effect of perioperative music on intraoperative sedative medication requirement was assessed in 13 studies (846 patients). Propofol requirement was assessed in 9,20,26,29,33,34,35,40,48,51 midazolam requirement in 3,21,33,36 and end-tidal inhalation anesthetics concentration in 2 studies.38,64 In one of these aforementioned studies, both propofol and midazolam were administered intraoperatively for sedation.33 Incremental intraoperative sedative medication doses were administered based on sedation depth, which was either assessed using a bispectral index monitor or a validated sedation scale. The infusion rate was patient-controlled in 4 studies.20,34,36,48 The manner of sedation depth assessment and whether or not infusion rate was patient-controlled is specified in Fig. 4.
FIGURE 4.
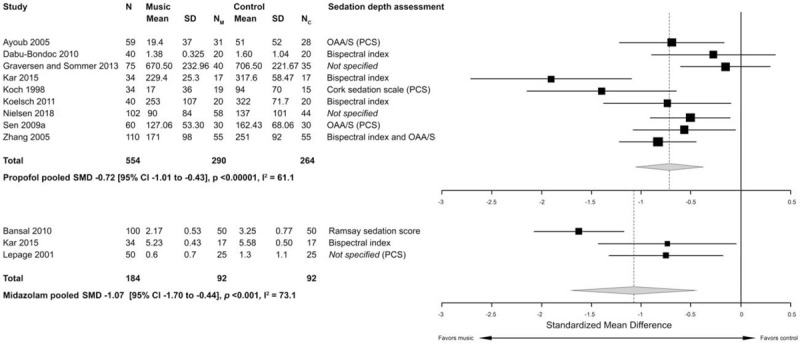
Effect of perioperative music on intraoperative sedative medication requirement. Forest plot presenting the effect of perioperative music on intraoperative propofol (above) and midazolam (below) medication requirement. CI indicates confidence interval; Mean, mean milligrams of propofol or midazolam; N, total number of patients in study; NC, number of patients in the control group; NM, number of patients in the music group; OAA/S, observer assessment of alertness/sedation scale; PACU, post-anesthesia care unit; PCS, patient-controlled sedation; SD, standard deviation in milligrams of propofol or midazolam; SMD, standardized mean difference.
Perioperative music significantly reduced intraoperative propofol requirement (pooled SMD −0.72 [95% CI −1.01 to −0.43], P < 0.00001, I 2 = 61.1, N = 554 patients, 9 studies) (Fig. 4). All included studies evaluating the effect of music on propofol requirement, except 229,40 that did not specify the manner of sedation depth assessment, reported that the level of sedation did not differ between the music and control group. This reduction in intraoperative propofol requirement remained present when these 2 studies29,40 were excluded from the analysis (pooled SMD −0.86, [95% CI −1.18 to −0.53], P < 0.00001, I 2 = 54.9, N = 377 patients, 7 studies), and when the 3 studies with patient-controlled propofol infusion rate were analyzed as a separate subgroup (pooled SMD −0.82 [95% CI −1.25 to −0.38], P = 0.00025, I 2 = 40.1, N = 153 patients). Perioperative music also significantly reduced intraoperative midazolam requirement (pooled SMD −1.07 [95% CI −1.70 to −0.44], P < 0.001, I 2 = 73.1, N = 184 patients) (Fig. 4), while achieving the same sedation depth.
Length of Stay and Medical Costs
The effect of perioperative music on length of stay was assessed in 17 studies, of which 9 studies could be included in the meta-analysis. Total length of hospital stay of surgical inpatients was assessed in 4 studies,22,25,37,52 length of stay in the post-anesthesia or day care unit of patients undergoing outpatient surgery in 4 other studies20,26,29,34 and intensive care unit length of stay in 1 study.47 Perioperative music did not significantly reduce length of stay (pooled SMD −0.18 [95% CI −0.43 to 0.067], P = 0.15, I 2 = 56.0, N = 600 patients) (Fig. 5). When analyzing the studies with outpatient surgical patients (pooled SMD −0.053 [95% CI −0.35 to 0.24], P = 0.73, I 2 = 13.1, N = 208 patients) and inpatient operations (pooled SMD −0.21 [95% CI −0.66 to 0.25], P = 0.37, I 2 = 75.2, N = 325 patients) separately, length of stay was also not reduced.
FIGURE 5.
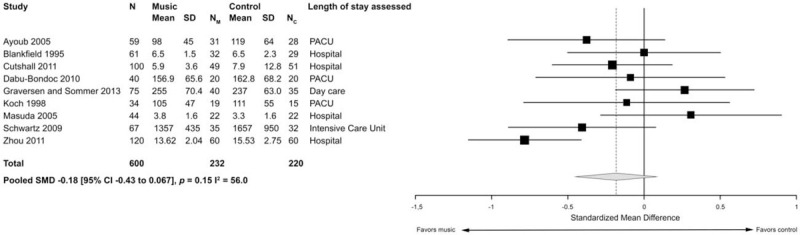
Effect of perioperative music on length of stay. Forest plot presenting the effect of perioperative music on length of stay. CI indicates confidence interval; Mean, mean length of stay; N, total number of patients in study; NC, number of patients in the control group; NM, number of patients in the music group; PACU, post-anesthesia care unit; SD, standard deviation; SMD, standardized mean difference.
Intensive care unit costs tended to be lower in 1 pilot study [3911 (SD 1566) versus 4365 dollars (SD 2632), P = 0.09], as time spent in the intensive care unit was significantly reduced in the music group compared to the control group.47 However, this did not reach statistical significance and overall direct medical costs during hospital length of stay did not differ significantly.
DISCUSSION
This systematic review and meta-analysis of 55 randomized controlled trials evaluates the effect of perioperative music on intraoperative and postoperative medication requirement and length of stay. Because of the current opioid epidemic, which has increased opioid-related deaths and led to a substantial financial burden,6,68 there is an increased interest in nonpharmacological interventions that can reduce both postoperative pain and opioid consumption. Perioperative music reduced opioid consumption by 4.4 mg ME in studies measuring opioid requirement for at least 24 hours or more after surgery. In studies measuring at least 72 hours or more after major surgical procedures, a reduction of 9.82 mg ME was observed. Opioid-related adverse effects have been observed to be dose-dependent and an increased requirement of 3 to 4 mg ME after surgery has been related to the occurrence of 1 additional, clinically meaningful, adverse event.69 A maximum daily dose exceeding 2 mg of parenteral hydromorphone, equivalent to 10 to 14 mg ME,70 were significantly associated with the development of postoperative ileus after colorectal surgery, increasing morbidity, length of hospital stay, and direct medical costs.71 Both a higher daily opioid dose and a prolonged use in opioid-naive patients also increase the risk of chronic opioid use.6 As more elderly patients are nowadays undergoing surgery, this group would be of particular interest to the use of perioperative music, as they have an increased risk of opioid-related adverse effects and chronic abuse because of polypharmacy and comorbidity.72,73
Perioperative music also significantly reduced both intraoperative propofol and midazolam requirement, whilst achieving the same sedation level. Midazolam is often used during locoregional anesthesia or as a preoperative anxiolytic, but is a risk factor for the occurrence of postoperative delirium.74 A higher level of preoperative anxiety has been associated with a higher amount of intravenous sedation requirement to induce and maintain adequate sedation level during surgery.75 Previous studies have reported a beneficial effect of perioperative music on anxiety levels,14,15,16 which could theoretically explain the reduced sedation dosage needed. Although a dose-dependent relation of sedative medication and intraoperative hemodynamic changes has been observed,76 the predictive outcome capabilities of intraoperative hemodynamics have only been investigated sparingly.77
No effect of perioperative music on length of stay was demonstrated. However, only 4 studies assessed total length of stay and organizational rather than patient factors are the most important predictors of delayed discharge.78 Moreover, almost half of the studies (44%) that assessed length of stay did so in patients undergoing minor surgery in the outpatient setting, making it unlikely to find a clinically relevant difference. Even though opioids are relatively cheap, opioids accounted for 1% of total hospital costs in an observational study of patients undergoing joint replacement surgery.79 As one of the most commonly performed procedures in the developed world, yearly costs in the United States alone amount to more than $20 billion.80 It is therefore likely that the beneficial effects of perioperative music on mediation requirement will also be observed financially, especially when taking into account the costs that come with opioid-related adverse effects.10
This meta-analysis has several strong points. A comprehensive literature search was performed with a dedicated biomedical information specialist. A predefined definition of music was used and studies with live music, a music therapist and concomitant interventions were excluded. In comparison to earlier performed meta-analyses investigating the effects of perioperative music, our focus was solely on medication requirement and length of stay in adult surgical patients. Vetter et al did observe a significant reduction in pain medication requirement by perioperative music in fourteen studies, but this was not significant for the subgroup of patients who received general anesthesia in 9 studies.15 The meta-analysis by Hole et al contained studies with both surgical and nonsurgical, diagnostic procedures leading to clinical heterogeneity, and did not differentiate between opioid, benzodiazepines, and sedative medication requirement.14 Nevertheless, this meta-analysis has limitations as well. The included studies contained different surgical patients, surgical procedures, and follow-up duration of the outcome assessment. This was reflected in the moderate to high level of heterogeneity observed. Medication requirement can be influenced by factors such as age, body weight, and the duration of surgery. Some of these baseline characteristics were not reported in the included studies, potentially increasing the risk of bias in interpreting results. Therefore, it is not entirely clear whether perioperative music can have the same beneficial effect size on medication requirement for all surgical procedures. Measurement duration of postoperative opioid requirement in 15 of the 20 studies was 24 hours after surgery or less. Consequently, the mean absolute reduction in mg ME in the music group was relatively low and perhaps does not reflect the full beneficial effect of perioperative music on medication requirement. Although a meta-regression analysis could be performed with covariates such as music intervention duration, music exposure moment relative to the surgical procedure (ie, preoperatively, intraoperatively, postoperatively, or multiple moments), operative severity (ie, minor, moderate, or major surgery), and measurement duration, this was not deemed appropriate as at least ten studies for each co-variate are recommended.18 Only postoperative opioids were assessed, as other analgesic medications were often not reported. Some included studies did report that perioperative music also reduced nonopioid analgesic requirement postoperatively.24,49
Our literature search did not include patient-reported outcome measures. However, it should be noted that patients in the included studies were extremely positive towards the use of perioperative music. Almost all patients (88% or higher) found perioperative music to be an enjoyable experience.23,35,55,56,81,82,83 Likewise, a majority would opt for music again in the future,21,25,28 even pro-actively asking for music in subsequent surgical procedures.21 Patient satisfaction was also markedly increased in the music group,48,49,50,51,56 with the only negative comments observed being from those who did not get music or related to the type of available music.25,84 Although side-effects of perioperative music could theoretically occur, none of the included studies reported any adverse effects. Specifically, no cardiorespiratory depressions were observed,34,51 while McCaffrey et al reported that perioperative music had a significant beneficial effect on delirium and confusion.56,85 In some studies, care was taken to restrict music volume and adhere to the noise and hearing loss guidelines to prevent hearing damage,86 whereas others allowed patients the option to adjust the music volume to their liking. The most well-known implemented nonpharmacological, multimodal interventions in surgical patient care are part of the guidelines collectively known as the Enhanced Recovery After Surgery protocols, which focus on reducing the physiological stress response to surgery by optimizing nutritional state, reducing opioid use and early mobilization.87 Originally introduced in colorectal surgical patient care, it has subsequently been implemented in a wide range of different surgical specialties with surgery-specific variations. Likewise, the use of perioperative music should be adapted to fit into the operative procedure, individual clinical setting, and wishes and requirements of the medical team. Although it is difficult to draw a firm clinical recommendation based on the data in our meta-analysis, 75% of studies assessing opioid requirement exposed patients to a total of 120 minutes perioperative music on average or less, delivered either before, during and/or on the first 2 days after surgery. Therefore, it seems that a relatively short exposure to music can already be beneficial, with a majority of the studies using a music player and headphones to avoid disrupting communication of the medical staff. Further research could focus on the effect of perioperative music on postoperative complications, clinical recovery, costs, and implementation.
CONCLUSIONS
Perioperative music can reduce postoperative opioid and intraoperative sedative medication requirement. Therefore, perioperative music may potentially improve patient outcome and reduce medical costs, as a higher opioid dosage is associated with an increased risk of adverse events and chronic opioid use. The use of perioperative music seems to be safe and patient-friendly, given the high patients satisfaction reported whilst no adverse effects were observed.
Acknowledgments
The authors thank W. Bramer, biomedical information specialist of the Medical Library, Erasmus MC University Medical Centre, Rotterdam, for his assistance with the literature search. The authors thank V.P.B. Elbers, BsC, Medical Student, for assistance in the literature screening. The authors thank A. Tomer, MsC, Statistician, for assistance in the statistical analysis.
Supplementary Material
Footnotes
No external funding was received for this study.
The authors declare no conflict of interest.
REFERENCES
- 1.Gan TJ, Habib AS, Miller TE, et al. Incidence, patient satisfaction, and perceptions of post-surgical pain: results from a US national survey. Curr Med Res Opin 2014; 30:149–160. [DOI] [PubMed] [Google Scholar]
- 2.Pavlin DJ, Rapp SE, Polissar NL, et al. Factors affecting discharge time in adult outpatients. Anesth Analg 1998; 87:816–826. [DOI] [PubMed] [Google Scholar]
- 3.Ballantyne JC, Carr DB, deFerranti S, et al. The comparative effects of postoperative analgesic therapies on pulmonary outcome: cumulative meta-analyses of randomized, controlled trials. Anesth Analg 1998; 86:598–612. [DOI] [PubMed] [Google Scholar]
- 4.Vadivelu N, Mitra S, Narayan D. Recent advances in postoperative pain management. Yale J Biol Med 2010; 83:11–25. [PMC free article] [PubMed] [Google Scholar]
- 5.Taylor RS, Ullrich K, Regan S, et al. The impact of early postoperative pain on health-related quality of life. Pain Pract 2013; 13:515–523. [DOI] [PubMed] [Google Scholar]
- 6.Shah A, Hayes CJ, Martin BC. Factors influencing long-term opioid use among opioid naive patients: an examination of initial prescription characteristics and pain etiologies. J Pain 2017; 18:1374–1383. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Dolin SJ, Cashman JN. Tolerability of acute postoperative pain management: nausea, vomiting, sedation, pruritus, and urinary retention. Evidence from published data. Br J Anaesth 2005; 95:584–591. [DOI] [PubMed] [Google Scholar]
- 8.Roberts GW, Bekker TB, Carlsen HH, et al. Postoperative nausea and vomiting are strongly influenced by postoperative opioid use in a dose-related manner. Anesth Analg 2005; 101:1343–1348. [DOI] [PubMed] [Google Scholar]
- 9.Clegg A, Young JB. Which medications to avoid in people at risk of delirium: a systematic review. Age Ageing 2011; 40:23–29. [DOI] [PubMed] [Google Scholar]
- 10.Gan TJ, Robinson SB, Oderda GM, et al. Impact of postsurgical opioid use and ileus on economic outcomes in gastrointestinal surgeries. Curr Med Res Opin 2015; 31:677–686. [DOI] [PubMed] [Google Scholar]
- 11.Nagappa M, Weingarten TN, Montandon G, et al. Opioids, respiratory depression, and sleep-disordered breathing. Best Pract Res Clin Anaesthesiol 2017; 31:469–485. [DOI] [PubMed] [Google Scholar]
- 12.Brummett CM, Waljee JF, Goesling J, et al. New persistent opioid use after minor and major surgical procedures in US adults. JAMA Surg 2017; 152:e170504. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Martin BC, Fan MY, Edlund MJ, et al. Long-term chronic opioid therapy discontinuation rates from the TROUP study. J Gen Intern Med 2011; 26:1450–1457. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hole J, Hirsch M, Ball E, et al. Music as an aid for postoperative recovery in adults: a systematic review and meta-analysis. Lancet 2015; 386:1659–1671. [DOI] [PubMed] [Google Scholar]
- 15.Vetter D, Barth J, Uyulmaz S, et al. Effects of art on surgical patients: a systematic review and meta-analysis. Ann Surg 2015; 262:704–713. [DOI] [PubMed] [Google Scholar]
- 16.Kuhlmann AYR, de Rooij A, Kroese LF, et al. Meta-analysis evaluating music interventions for anxiety and pain in surgery. Br J Surg 2018; 105:773–783. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Bramer WM, Rethlefsen ML, Mast F, et al. Evaluation of a new method for librarian-mediated literature searches for systematic reviews. Res Synth Methods 2018; 9:510–520. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011. Available at: www.handbook.cochrane.org. Accessed April 29, 2019. [Google Scholar]
- 19.Wallace BC, Dahabreh IJ, Trikalinos TA, et al. Closing the gap between methodologists and end-users: R as a computational back-end. J Stat Softw 2012; 49:1–15. [Google Scholar]
- 20.Ayoub CM, Rizk LB, Yaacoub CI, et al. Music and ambient operating room noise in patients undergoing spinal anesthesia. Anesth Analg 2005; 100:1316–1319. [DOI] [PubMed] [Google Scholar]
- 21.Bansal P, Kharod U, Patel P, et al. The effect of music therapy on sedative requirements and haemodynamic parameters in patients under spinal anaesthesia; a prospective study. J Clin Diagn Res 2010; 4:2782–2789. [Google Scholar]
- 22.Blankfield RP, Zyzanski SJ, Flocke SA, et al. Taped therapeutic suggestions and taped music as adjuncts in the care of coronary-artery-bypass patients. Am J Clin Hypn 1995; 37:32–42. [DOI] [PubMed] [Google Scholar]
- 23.Chen HJ, Chen TY, Huang CY, et al. Effects of music on psychophysiological responses and opioid dosage in patients undergoing total knee replacement surgery. Jpn J Nurs Sci 2015; 12:309–319. [DOI] [PubMed] [Google Scholar]
- 24.Ciğerci Y, Özbayir T. The effects of music therapy on anxiety, pain and the amount of analgesics following coronary artery surgery. Turk J Thorac Cardiovasc Surg 2016; 24:44–50. [Google Scholar]
- 25.Cutshall SM, Anderson PG, Prinsen SK. Effect of the combination of music and nature sounds on pain and anxiety in cardiac surgical patients: a randomized study. Altern Therap Health Med 2011; 17:16–23. [PubMed] [Google Scholar]
- 26.Dabu-Bondoc S, Vadivelu N, Benson J, et al. Hemispheric synchronized sounds and perioperative analgesic requirements. Anesth Analg 2010; 110:208–210. [DOI] [PubMed] [Google Scholar]
- 27.Ebneshahidi A, Mohseni M. The effect of patient-selected music on early postoperative pain, anxiety, and hemodynamic profile in cesarean section surgery. J Altern Complement Med 2008; 14:827–831. [DOI] [PubMed] [Google Scholar]
- 28.Good M. A comparison of the effects of jaw relaxation and music on postoperative pain. Nurs Res 1995; 44:52–57. [PubMed] [Google Scholar]
- 29.Graversen M, Sommer T. Perioperative music may reduce pain and fatigue in patients undergoing laparoscopic cholecystectomy. Acta Anaesthesiol 2013; 57:1010–1016. [DOI] [PubMed] [Google Scholar]
- 30.Heitz L, Symreng T, Scamman FL. Effect of music therapy in the postanesthesia care unit: a nursing intervention. J Post Anesth Nurs 1992; 7:22–31. [PubMed] [Google Scholar]
- 31.Hook L, Sonwathana P, Petpichetchian W. Music therapy with female surgical patients: effect on anxiety and pain. Thai J Nurs Res 2008; 12:259–271. [Google Scholar]
- 32.Ikonomidou E, Rehnstrom A, Naesh O. Effect of music on vital signs and postoperative pain. AORN J 2004; 80:269–274. [DOI] [PubMed] [Google Scholar]
- 33.Kar SK, Ganguly T, Roy SS, et al. Effect of indian classical music (Raga therapy) on fentanyl, vecuronium, propofol requirements and cortisol levels in cardiopulmonary bypass. J Anesth Crit Care 2015; 2:1–5. [Google Scholar]
- 34.Koch ME, Kain ZN, Ayoub C, et al. The sedative and analgesic sparing effect of music. Anesthesiology 1998; 89:300–306. [DOI] [PubMed] [Google Scholar]
- 35.Koelsch S, Fuermetz J, Sack U, et al. Effects of music listening on cortisol levels and propofol consumption during spinal anesthesia. Front Psychol 2011; 2:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Lepage C, Drolet P, Girard M, et al. Music decreases sedative requirements during spinal anesthesia. Anesth Analg 2001; 93:912–916. [DOI] [PubMed] [Google Scholar]
- 37.Masuda T, Miyamoto K, Shimizu K. Effects of music listening on elderly orthopaedic patients during postoperative bed rest. Nordic J Music Ther 2005; 14:4–14. [Google Scholar]
- 38.Migneault B, Girard F, Albert C, et al. The effect of music on the neurohormonal stress response to surgery under general anesthesia. Anesth Analg 2004; 98:527–532. [DOI] [PubMed] [Google Scholar]
- 39.Miladinia M, Pishgooie AH, Aliyari S, et al. The comparison of the effect of two complementary medicine methods (music therapy and massage therapy) on postoperative acute pain after abdominal surgery: a randomized clinical trial study. Iran Red Crescent Med J 2017; 19:1–7. [Google Scholar]
- 40.Nielsen E, Wahlin I, Frisman GH. Evaluating pictures of nature and soft music on anxiety and well-being during elective surgery. Open Nurs J 2018; 12:58–66. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.Nilsson U, Rawal N, Uneståhl LE, et al. Improved recovery after music and therapeutic suggestions during general anaesthesia: a double-blind randomised controlled trial. Acta Anaesthesiol Scand 2001; 45:812–817. [DOI] [PubMed] [Google Scholar]
- 42.Nilsson U, Rawal N, Enqvist B, et al. Analgesia following music and therapeutic suggestions in the PACU in ambulatory surgery; a randomized controlled trial. Acta Anaesthesiol Scand 2003; 47:278–283. [DOI] [PubMed] [Google Scholar]
- 43.Nilsson U, Rawal N, Unosson M. A comparison of intra-operative or postoperative exposure to music – a controlled trial of the effects on postoperative pain. Anaesthesia 2003; 58:699–703. [DOI] [PubMed] [Google Scholar]
- 44.Nilsson U, Unosson M, Rawal N. Stress reduction and analgesia in patients exposed to calming music postoperatively: a randomized controlled trial. Eur J Anaesthesiol 2005; 22:96–102. [DOI] [PubMed] [Google Scholar]
- 45.Nilsson U. Soothing music can increase oxytocin levels during bed rest after open-heart surgery: a randomised control trial. J Clin Nurs 2009; 18:2153–2161. [DOI] [PubMed] [Google Scholar]
- 46.Reza N, Ali SM, Saeed K, et al. The impact of music on postoperative pain and anxiety following cesarean section. Middle East J Anesthiol 2007; 19:573–586. [PubMed] [Google Scholar]
- 47.Schwartz FJ. A pilot study of patients in postoperative cardiac surgery. Music Med 2009; 1:70–74. [Google Scholar]
- 48.Şen H, Ateş F, Sizlan A, et al. Effect of music on sedation during local urological surgeries. Anatolian J Clin Invest 2009; 3:131–135. [Google Scholar]
- 49.Şen H, Sizlan A, Yanarates O, et al. The effect of musical therapy on postoperative pain after caesarean section. TAF Prevent Med Bull 2009; 8:107–112. [Google Scholar]
- 50.Şen H, Yanarateş Ö, Sizlan A, et al. The efficiency and duration of the analgesic effects of musical therapy on postoperative pain. Agri 2010; 22:145–150. [PubMed] [Google Scholar]
- 51.Zhang XW, Fan Y, Manyande A, et al. Effects of music on target-controlled infusion of propofol requirements during combined spinal-epidural anaesthesia. Anaesthesia 2005; 60:990–994. [DOI] [PubMed] [Google Scholar]
- 52.Zhou KN, Li XM, Yan H, et al. Effects of music therapy on depression and duration of hospital stay of breast cancer patients after radical mastectomy. Chin Med J (Engl) 2011; 124:2321–2327. [PubMed] [Google Scholar]
- 53.Zimmerman L, Nieveen J, Barnason S, et al. The effects of music interventions on postoperative pain and sleep in coronary artery bypass graft (CABG) patients... including commentary by Miaskowski C. Scholar Inq Nurs Pract 1996; 10:153–174. [PubMed] [Google Scholar]
- 54.Easter B, DeBoer L, Settlemyre G, et al. The impact of music on the PACU patient's perception of discomfort. J Perianesth Nurs 2010; 25:79–87. [DOI] [PubMed] [Google Scholar]
- 55.Liu Y, Petrini MA. Effects of music therapy on pain, anxiety, and vital signs in patients after thoracic surgery. Complement Ther Med 2015; 23:714–718. [DOI] [PubMed] [Google Scholar]
- 56.McCaffrey R, Locsin R. The effect of music on pain and acute confusion in older adults undergoing hip and knee surgery. Holist Nurs Pract 2006; 20:218–224. [DOI] [PubMed] [Google Scholar]
- 57.Tse MMY, Chan MF, Benzie IFF. The effect of music therapy on postoperative pain, heart rate, systolic blood pressure and analgesic use following nasal surgery. J Pain Palliative Care Pharmacother 2005; 19:21–29. [PubMed] [Google Scholar]
- 58.Vaajoki A, Pietila AM, Kankkunen P, et al. Effects of listening to music on pain intensity and pain distress after surgery: an intervention. J Clin Nurs 2012; 21:708–717. [DOI] [PubMed] [Google Scholar]
- 59.Johnson SP, Chung KC, Zhong L, et al. Risk of prolonged opioid use among opioid-naive patients following common hand surgery procedures. J Hand Surg Am 2016; 41:947–957. [DOI] [PubMed] [Google Scholar]
- 60.Kumar TS, Muthuraman M, Krishnakumar R. Effect of the raga ananda bhairavi in post operative pain relief management. Indian J Surg 2014; 76:363–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61.Laurion S, Fetzer SJ. The effect of two nursing interventions on the postoperative outcomes of gynecologic laparoscopic patients. J Perianesth Nurs 2003; 18:254–261. [DOI] [PubMed] [Google Scholar]
- 62.Macdonald RAR, Mitchell LA, Dillon T, et al. An empirical investigation of the anxiolytic and pain reducing effects of music. Psychol Music 2003; 31:187–203. [Google Scholar]
- 63.Kliempt P, Ruta D, Ogston S, et al. Hemispheric-synchronisation during anaesthesia: a double blind randomised trial using audiotapes for intra-operative nociception control. Anaesthesia 1999; 54:769–773. [DOI] [PubMed] [Google Scholar]
- 64.Szmuk P, Aroyo N, Ezri T, et al. Listening to music during anesthesia does not reduce the sevoflurane concentration needed to maintain a constant bispectral index. Anesth Analg 2008; 107:77–80. [DOI] [PubMed] [Google Scholar]
- 65.Ohqvist G, Hallin R, Gelinder S, et al. A comparison between morphine, meperidine and ketobemidone in continuous intravenous infusion for postoperative relief. Acta Anaesthesiol Scand 1991; 35:44–48. [DOI] [PubMed] [Google Scholar]
- 66.Grond S, Sablotzki A. Clinical pharmacology of tramadol. Clin Pharmacokinet 2004; 43:879–923. [DOI] [PubMed] [Google Scholar]
- 67.Stanley G, Appadu B, Mead M, et al. Dose requirements, efficacy and side effects of morphine and pethidine delivered by patient-controlled analgesia after gynaecological surgery. Br J Anaesth 1996; 76:484–486. [DOI] [PubMed] [Google Scholar]
- 68.Mohamadi A, Chan JJ, Lian J, et al. Risk factors and pooled rate of prolonged opioid use following trauma or surgery: a systematic review and meta-(regression) analysis. J Bone Joint Surg Am 2018; 100:1332–1340. [DOI] [PubMed] [Google Scholar]
- 69.Zhao SZ, Chung F, Hanna DB, et al. Dose-response relationship between opioid use and adverse effects after ambulatory surgery. J Pain Sympt Manage 2004; 28:35–46. [DOI] [PubMed] [Google Scholar]
- 70.Lowe A, Hamilton M, Greenall BMJ, et al. Fatal overdoses involving hydromorphone and morphine among inpatients: a case series. CMAJ Open 2017; 5:E184–E189. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 71.Barletta JF, Asgeirsson T, Senagore AJ. Influence of intravenous opioid dose on postoperative ileus. Ann Pharmacother 2011; 45:916–923. [DOI] [PubMed] [Google Scholar]
- 72.Sun EC, Darnall BD, Baker LC, et al. Incidence of and risk factors for chronic opioid use among opioid-naive patients in the postoperative period. JAMA Intern Med 2016; 176:1286–1293. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73.Chau DL, Walker V, Pai L, et al. Opiates and elderly: use and side effects. Clin Interv Aging 2008; 3:273–278. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 74.Inouye SK, Robinson T, Blaum C, et al. Postoperative delirium in older adults: best practice statement from the American Geriatrics Society. J Am Coll Surg 2015; 220:136–148. [DOI] [PubMed] [Google Scholar]
- 75.Kil HK, Kim WO, Chung WY, et al. Preoperative anxiety and pain sensitivity are independent predictors of propofol and sevoflurane requirements in general anaesthesia. Br J Anaesth 2012; 108:119–125. [DOI] [PubMed] [Google Scholar]
- 76.de Wit F, van Vliet AL, de Wilde RB, et al. The effect of propofol on haemodynamics: cardiac output, venous return, mean systemic filling pressure, and vascular resistances. Br J Anaesth 2016; 116:784–789. [DOI] [PubMed] [Google Scholar]
- 77.Prasad V, Guerrisi M, Dauri M, et al. Prediction of postoperative outcomes using intraoperative hemodynamic monitoring data. Sci Rep 2017; 7:1–11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 78.Challis D, Hughes J, Xie C, et al. An examination of factors influencing delayed discharge of older people from hospital. Int J Geriatr Psychiatry 2014; 29:160–168. [DOI] [PubMed] [Google Scholar]
- 79.Macario A, McCoy M. The pharmacy cost of delivering postoperative analgesia to patients undergoing joint replacement surgery. J Pain 2003; 4:22–28. [DOI] [PubMed] [Google Scholar]
- 80.Lam V, Teutsch S, Fielding J. Hip and knee replacements: a neglected potential savings opportunity. JAMA 2018; 319:977–978. [DOI] [PubMed] [Google Scholar]
- 81.Allred KD, Byers JF, Sole ML. The effect of music on postoperative pain and anxiety. Pain Manage Nurs 2010; 11:15–25. [DOI] [PubMed] [Google Scholar]
- 82.Ignacio JJ, Fai CM, Hui TEOS, et al. Research in brief – the effect of music on pain, anxiety, and analgesic use on adults undergoing an orthopaedic surgery: a pilot study. Singapore Nurs J 2012; 39:49–51. [Google Scholar]
- 83.Nilsson U. The effect of music intervention in stress response to cardiac surgery in a randomized clinical trial. Heart Lung 2009; 38:201–207. [DOI] [PubMed] [Google Scholar]
- 84.Johnson B, Raymond S, Goss J. Perioperative music or headsets to decrease anxiety. J Perianesth Nurs 2012; 27:146–154. [DOI] [PubMed] [Google Scholar]
- 85.McCaffrey R. The effect of music on acute confusion in older adults after hip or knee surgery. Appl Nurs Res 2009; 22:107–112. [DOI] [PubMed] [Google Scholar]
- 86.Centers for Disease Control and Prevention (CDC). Noise and Hearing Loss Prevention, 2018. Available at: https://www.cdc.gov/niosh/topics/noise/reducenoiseexposure/regsguidance.html. Accessed April 7, 2019. [Google Scholar]
- 87.Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg 2017; 152:292–298. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.