

Abstract
Desmoid tumors are rare tumors which can cause intestinal obstructions. Surgical wide excision is currently the treatment of choice, with the goal of achieving free resection margins.
Keywords: desmoid, obstruction, small bowel, tumor
Desmoid tumor causing small bowel obstruction.

1. INTRODUCTION
Desmoid tumors are rare and benign but can be locally aggressive. In the majority of cases, they are asymptomatic and difficult to diagnose based on clinical and radiological criteria. Diagnosis is usually made on histopathology. Surgical wide excision is currently the treatment of choice.
2. CASE REPORT
A 52‐year‐old healthy patient presented with abdominal pain, nausea, and vomiting. Physical examination revealed abdominal distension and diffuse tenderness. Laboratory tests were unremarkable. An abdominal CT scan revealed a mesenteric mass measuring 9 × 6 cm in the pelvis and small bowel mechanical obstruction (Figure 1). This mass was not visible on a prior abdominal CT scan 2 years before. An exploratory laparoscopy was performed after failure of conservative treatment with a nasogastric tube for 48 hours. The mass was in contact with last ileal loop. A mini‐laparotomy was performed with small segmental resection and manual end‐to‐end anastomosis (Figure 2). The patient was discharged on postoperative day 4, and at follow‐up at 1 month, he had no complaints. Macroscopically, the lesion was a voluminous well‐defined nodular formation. Histopathological examination revealed richly vascularized fusocellular proliferation with elongated nuclei without atypia. This picture was compatible with a desmoid tumor, confirmed after molecular analysis (mutation CTNNB1 at 37.9%).
FIGURE 1.
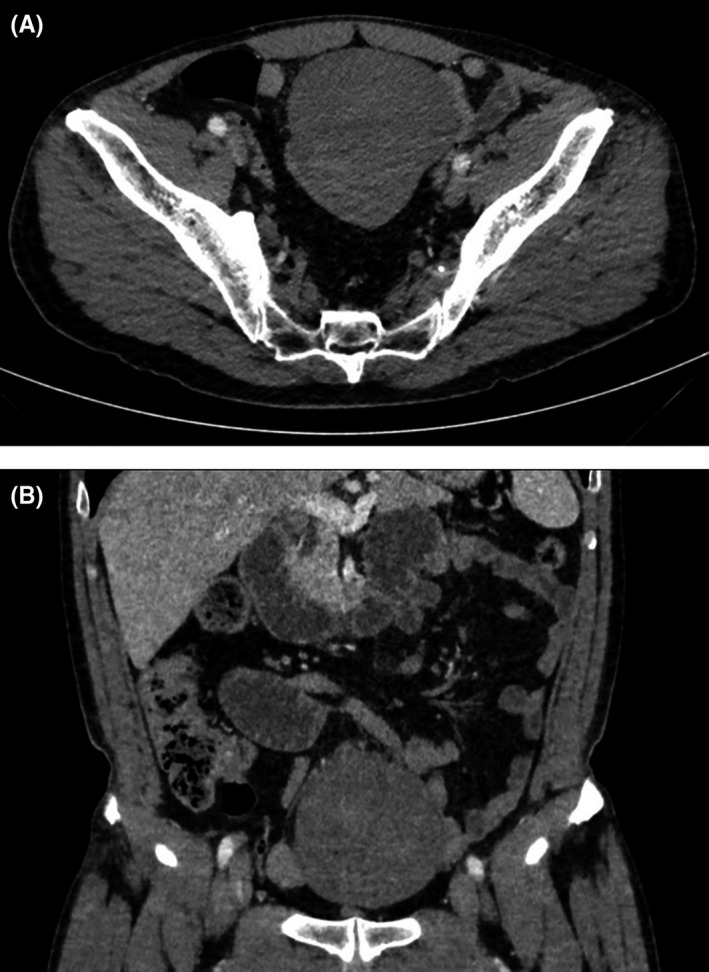
CT scan revealing a 9 × 6 cm mass in the pelvis in contact with small bowel (A: axial; B:coronal)
FIGURE 2.
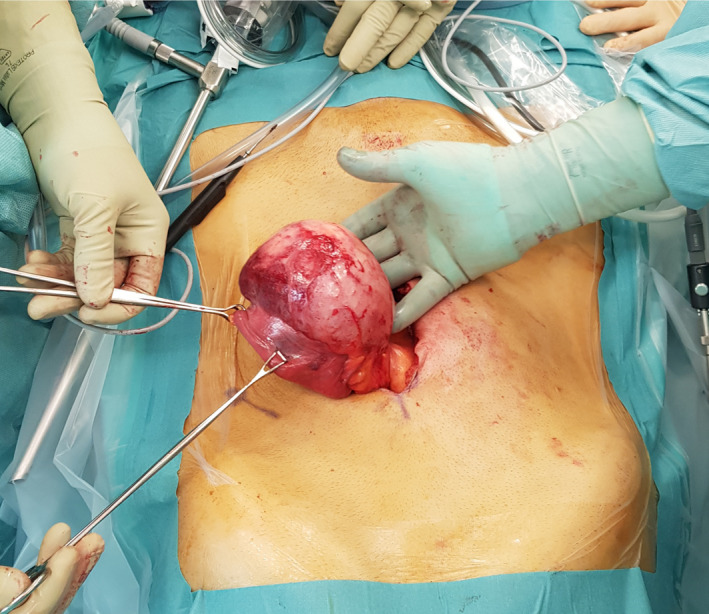
Mini‐laparotomy showing a tumor mass in contact with the ileal loop
3. DISCUSSION
Desmoid tumors are rare, benign, fibromatous lesions that are the result of abnormal proliferation of myofibroblasts. 1 Most intra‐abdominal desmoid tumors affect small bowel mesentery, usually measure between 5 and 10 cm, and occur in a wide age range of patients without gender or race predilection. 1 , 2 , 3 These tumors are common in familial adenomatous polyposis (FAP) and are characterized by their propensity for slow growth and invasion of adjacent organs, but do not show metastatic tendency. 4 , 5 Desmoid tumors causing bowel obstruction have been reported but remain a rare finding. 6 Surgical wide excision is currently the treatment of choice, with the goal of achieving free resection margins. 1 , 7
CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest.
AUTHOR CONTRIBUTIONS
All authors were involved in drafting the article or revising it, and approved the final version to be published.
ETHICAL APPROVAL
The Regional Committee for Medical and Health Research Ethics (CER‐VD) did not require ethical approval for reporting individual cases.
Martin D, Labgaa I, Petermann D, Di Mare L. Small bowel obstruction caused by a fast‐growing desmoid tumor. Clin Case Rep. 2020;8:2318–2319. 10.1002/ccr3.3162
REFERENCES
- 1. Sakorafas GH, Nissotakis C, Peros G. Abdominal desmoid tumors. Surg Oncol. 2007;16(2):131‐142. [DOI] [PubMed] [Google Scholar]
- 2. Faria SC, Iyer RB, Rashid A, Ellis L, Whitman GJ. Desmoid tumor of the small bowel and the mesentery. AJR Am J Roentgenol. 2004;183(1):118. [DOI] [PubMed] [Google Scholar]
- 3. Misiak P, Piskorz L, Wcislo S, Jablonski S, Brocki M. Giant mesentery fibromatosis presenting as acute abdomen ‐ case report. Contemp Oncol. 2013;17(5):468‐469. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4. Shields CJ, Winter DC, Kirwan WO, Redmond HP. Desmoid tumours. Eur J Surg Oncol. 2001;27(8):701‐706. [DOI] [PubMed] [Google Scholar]
- 5. Xuereb S, Xuereb R, Buhagiar C, Gauci J, Magri C. A case report of desmoid tumour‐a forgotten aspect of FAP? Int J Surg Case Rep. 2017;30:122‐125. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6. Jambhekar A, Robinson S, Zafarani P, Rucinski J, Gudavalli P. Intestinal obstruction caused by desmoid tumours: a review of the literature. JRSM Open. 2018;9(5):2054270418763340. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Disher AC, Biswas M, Miller TQ, Kuvhenguhwa A. Atypical desmoid tumor of the abdomen: a case report. J Natl Med Assoc. 1993;85(4):309‐311. [PMC free article] [PubMed] [Google Scholar]