

Abstract
Sexual minority men (SMM) face substantial disparities in rates of binge eating compared to heterosexual individuals, underscoring the need to study risk factors for the development of binge eating amongst SMM. One potential explanation for this disparity in binge eating is minority stress theory, which posits that minority groups face stressors, such as discrimination, due to their stigmatized position in society. Additionally, specific domains of discrimination may confer different levels of risk for binge eating. Therefore, the current study examined the association of various forms of discrimination, including appearance-based discrimination, and binge eating in a sample of SMM. A sample of 200 SMM (analytic sample of N = 187) from the greater Boston area completed self-report questionnaires assessing frequency of different forms of perceived discrimination (appearance, sexual orientation, race, etc.) and binge eating. A hierarchical binary logistic regression model was used to examine the association of different forms of discrimination with binge eating. 9% of the sample reported binge eating. Appearance-based discrimination was the most common form of discrimination (47%), and was significantly associated with binge eating, over and above all other forms of discrimination and sociodemographic variables, OR = 1.71, 95% CI = [1.24, 2.35], Wald χ2 (1) = 10.65, p = .001. Findings suggest that appearance-based discrimination may be related to binge eating in SMM. Clinicians may consider assessing appearance-based discrimination among SMM patients.
Keywords: binge eating, discrimination, sexual minority men, appearance
1. Introduction
Discrimination is defined as negative actions/behaviors directed at an individual or group of people on the basis of some sort of domain, such as race, sexual orientation, etc. (McLeod, 2008). Discrimination may occur for a multitude of different domains and is often associated with negative outcomes for the target(s) of discrimination. For example, perceived racial discrimination was associated with depressive symptoms, hostility, and aggression among ethnic minorities (Borders & Liang, 2011). However, discrimination encompasses more than race, and a vast body of literature exists that supports the negative outcomes of various forms of discrimination. For instance, perceived interpersonal/systemic religious discrimination for Muslims living in Australia has been associated with lower self-esteem (Every & Perry, 2014). A strong positive association has been found between sexist events/discrimination and psychological distress (Hurst & Beesley, 2013). Similarly, experiences of ethnic discrimination were associated with increased levels of depressive symptoms and perceived stress for a sample of US Puerto Ricans (Todorova, Falcon, Lincoln, & Price, 2010). In a nationally representative sample of persons from the Midlife Development in the United States survey, perceived age discrimination was associated with higher psychological distress and lower positive well-being (Vogt Yuan, 2007). With regard to sexual minority men (SMM; men who identify as non-heterosexual and/or report same-gender attraction/sexual behavior), discrimination because of socio-economic status (SES) was the only significant predictor of higher depressive and anxious symptoms in US SMM (Gamarel, Reisner, Parsons, & Golub, 2012). Discrimination exists across a variety of domains and is associated with a host of negative health outcomes.
One group which experiences significant discrimination is sexual minority individuals. A prominent model that explains discrimination amongst sexual minority individuals is minority stress theory (Meyer, 2003). The minority stress model posits that being part of a minority group (sexual minorities) is accompanied with distal stressors (prejudice, victimization, and discrimination) and proximal stressors (internal processes following exposure to distal stressors; e.g., internalized homophobia, concealment) unique to that group, as well as generalized stressors that are not unique. These factors may converge and lead to negative mental health outcomes. Utilizing minority stress theory, various studies have examined the role that discrimination plays in eating pathology for sexual minorities. For example, Wang and Borders (2017) demonstrated that discrimination based on sexual orientation was associated with disordered eating in a sample of adult SMM. Furthermore, in a sample of adolescents, bullying victimization due to sexual minority status was associated with higher levels of coping-motivated eating among gay men (Katz-wise et al, 2015). In the 2017 LGBTQ National teen survey, Himmelstein, Puhl, and Watson (2019) found that weight-based victimization was associated with maladaptive eating (binge eating, use of diet pills, smoking to lose weight, etc.) among US LGBTQ adolescents. Lastly, a study of sexual minority adolescents found that those who reported weight-based discrimination were at greater risk of diet pill/laxative misuse, vomiting, and binge eating (Gordon et al, 2018). These findings suggest that eating pathology and discrimination often covary among SMM.
Given that sexual minority stressors/discrimination contribute to eating pathology, it is unsurprising that sexual minorities experience disproportionate rates of eating pathology compared to heterosexual individuals. For example, recent data from a nationally representative sample of U.S. adults (n = 35,995) indicated that sexual minority individuals have higher lifetime prevalence rates of eating disorders than heterosexual individuals. Specifically, sexual minorities had a higher lifetime prevalence rate of anorexia nervosa (AN; 1.71% vs 0.77%), bulimia nervosa (BN; 1.25% vs 0.24%), and binge eating disorder (BED; 2.17% vs 0.81%) than heterosexual individuals (Kamody, Grilo, & Udo, 2019). Subgroups of sexual minority individuals, such as SMM, share this vulnerability for eating pathology. Calzo, Blashill, Brown, and Argenal (2017) conducted a systematic review of disordered eating behaviors in sexual minority samples that illustrates this point. For example, men aged 14–24 who reported same-gender attractions had more disordered eating symptoms than those who reported other-gender attractions (Shearer et al., 2015). A further university sample of college students found that gay men reported significantly higher levels of disordered eating, such as restraint, eating concern, and shape/weight concern than heterosexual men (Smith, Hawkeswood, Bodell, & Joiner, 2011). In addition, SMM reported 3–4.5 times the odds of vomiting or taking laxatives to lose weight compared to heterosexual men (Matthews-Ewald, Zullig, & Ward, 2014). SMM are at increased risk for disordered eating behaviors, but it is imperative to examine which forms of disordered eating disproportionately affect SMM most frequently.
Of note, one particular form of eating pathology that disproportionately affects SMM is binge eating behavior. In a sample of 3,411 undergraduate men and women, 38.1% of SMM reported at least one episode of objective binge eating over the past 28 days, compared to 24.0% of heterosexual men (Von Schell, Ohrt, Bruening, & Perez, 2018). Additionally, utilizing data from the Growing Up Today Study (GUTS) from 1998–2005, gay (OR = 7.2) and bisexual (OR = 4.6) male youth reported significantly higher odds of at least monthly binge eating compared to heterosexual male youth (Austin et al., 2009). Lastly, sexual minority adolescent boys in the UK Avon Longitudinal Study of Parents and Children (ALSPAC; n = 5048) reported greater prevalence of binge eating than heterosexual adolescent boys at age 14 (7.5% vs 2.8%) and age 16 (21.2% vs 3.1%; Calzo, Austin, & Micali, 2018). Given the disproportionate rates of binge-eating found in SMM compared to heterosexual men, as well as the association between discrimination and eating pathology in SMM, it is imperative to identify specific forms of discrimination associated with binge eating in this population.
One domain of discrimination potentially associated with binge eating in SMM that has been neglected in past research is discrimination based on physical appearance. Physical appearance-based discrimination might be particularly relevant for those who have appearance concerns distinct from weight, such as SMM, whose appearance concerns relate to muscularity and leanness in addition to body weight (Levesque & Vichesky, 2006; Smith, Hawkeswood, Bodell, & Joiner, 2011; Calzo et al, 2015). We propose that physical appearance-based discrimination, or discrimination based on some aspect of one’s appearance or physical shape, may be more appropriate for use with SMM than weight-based discrimination due to these concurrent drives for muscularity and leanness. Further, the use of physical appearance-based discrimination as a construct may encompass other aspects relevant to appearance satisfaction, such as concerns with height, penis size, or body hair that SMM endorse (Martins, Tiggemann, & Churchett, 2008). Therefore, the use of physical appearance discrimination may expand on past studies investigating weight-based discrimination in SMM, which has shown to be associated with binge eating for this population (Himmelstein et al., 2019; Gordon et al., 2018). Physical appearance-based discrimination has only been assessed in one prior study, to our knowledge. Various forms of discrimination were assessed in a national probability sample of US adults, and 5% reported appearance discrimination, whereas 7% reported weight discrimination, seeming to indicate that these are distinct concerns (Grollman, 2014). However, there are no known studies investigating physical appearance-based discrimination’s role in eating pathology, or its impact on SMM, leaving a notable gap for future research.
Therefore, the current study is the first study to examine the association between physical appearance-based discrimination and eating pathology in a sample of SMM. Furthermore, in addition to appearance discrimination, the current study accounts for various additional forms of discrimination including race, ethnicity, religion, age, income, gender, and sexual orientation to parse out the unique association of appearance discrimination and eating pathology. It was hypothesized that physical appearance discrimination would be associated with greater odds of binge eating over and above all other forms of discrimination. Physical appearance discrimination was hypothesized to have this effect above all other forms of discrimination, inclusive of sexual orientation discrimination, due to the association between weight-based discrimination (a construct that physical appearance discrimination expands upon) and binge eating found in SMM (Himmelstein et al., 2019; Gordon et al., 2018).
2. Methods
2.1. Participants and Procedure
Participants were 200 SMM from the greater Boston area who were enrolled in a study piloting an at-home rapid HIV detection test (Blashill et al, 2016; Safren et al, 2018). To be eligible, participants had to be over 18 years of age, test HIV-negative, and report at least one of the following sexual risk behaviors in the last 6 months: exchange of money, gifts, shelter, or drugs for sex with a male partner; four or more male anal sex partners; or condomless anal sex with a HIV-positive or unknown status male partner. Participants were excluded if they utilized pre-exposure prophylaxis (PrEP; a HIV preventative medication) at the time of enrollment, which spanned from 2012–2014. After enrollment, participants completed computerized self-report measures and structured clinician-based interviews at a Boston community health center that serves diverse populations, inclusive of SMM. Participants reported a mean age of 37 years (SD = 12) and were primarily White (70%). Most participants (n = 151, 76%) identified as gay, 37 (19%) identified as bisexual, 5 (3%) identified as heterosexual, 3 (3%) reported that they did not know their sexual orientation, and 1 (0%) participant indicated “other” as their sexual orientation. All participants provided informed consent and the study procedures were approved by the Institutional Review Board of Fenway Health (IRB00000858).
2.2. Measures
Perceived Discrimination.
The Everyday Discrimination Scale (Williams, Yu, Jackson, & Anderson, 1997) is a 9-item set of self-report statements that captures how often one experiences various forms of discrimination. Each statement describes a different experience of discrimination (e.g., “You are treated with less courtesy than other people are;” “You are threatened or harassed”). Participants also endorsed the type of discrimination they experienced for each statement. Types of discrimination included race, ethnicity, gender, sexual orientation, physical appearance, religion, age, and income. Each statement was binarily coded indicating whether or not a specific discrimination experience had ever occurred in one’s day to day life (0 = never, 1 = at least once), based on the frequency scale. Count scores were created to calculate the number of statements experienced for each type of discrimination. Thus, count scores for each type of discrimination ranged from 0 to 9, with higher scores indicating greater number of discriminatory experiences. This scale has been shown to have acceptable reliability and validity (Bastos, Celeste, Faerstein, & Barros, 2010). In the current sample, internal consistency for the set of various discriminations ranged from KR-20 = 0.89–0.96.
Binge Eating.
The Patient Health Questionnaire for Eating Disorders (PHQ-ED; Spitzer, Kroenke, & Williams, 1999) was utilized to denote the presence of binge eating in the current sample. To assess for binge eating, participants were asked two binary (yes/no) items designed to assess for loss of control and objective overeating. These two items were: ‘Do you often feel that you can’t control what or how much you eat?’ and ‘Do you often eat, within any 2-hour period, what most people would regard as an unusually large amount of food?’ If participants answered positively to both items they were classified as having experienced binge eating. Past research has similarly used this approach to operationally define binge eating amongst young adults (Striegel-Moore et al., 2009).
Socio-demographics.
Demographic information, including age, race, gender, sexual orientation, level of education, and income were collected.
2.3. Statistical Analyses
Frequencies of experience for all eight of the discrimination domains were calculated. Primary analyses examined the simultaneous association of each form of discrimination with odds of binge eating. Eight participants were excluded from analysis for missing PHQ-ED data, and five participants were excluded due to identification as transwomen, resulting in a final analytic sample of 187 cisgender participants. The aforementioned hypotheses were specified a priori, and the following analytic plan was pre-specified. A hierarchical logistic regression was conducted with the following three steps: 1.) count of physical appearance discrimination predicting binge eating as the binary criterion variable (0 = no binge eating, 1 = binge eating); 2.) adding the remaining discrimination count scores as predictors, and 3.) including additional socio-demographic covariates. Odds ratios (OR), 95% confidence intervals (CI), Wald’s chi-squared, and Nagelkerke’s R2 are reported. Analyses were conducted using SPSS version 26, with an alpha level of .05. Due to concerns about utilizing traditional maximum likelihood estimation when modeling the probability of rare events (King & Zeng, 2001), such as binge eating in this sample, sensitivity analyses employing logistic regression models using penalized likelihood estimation were also conducted to ensure that our results were robust (Firth, 1993). Penalized likelihood estimation reduces the small sample size bias inherent in maximum likelihood estimation and is the recommended method for modeling rare events (Leitgöb, 2013). Results were equivalent across both methods, thus, for parsimony, logistic regression with maximum likelihood is presented below.
3. Results
Table 1 displays characteristics of the current sample. Sixteen participants reported binge eating (9% of the sample). Physical appearance-based discrimination was the most common form of discrimination, with 47% of participants reporting at least one instance, followed closely by income (45%) and sexual orientation (44%; see figure 1). Furthermore, Table 2 displays a correlation matrix of all study variables.
Table 1.
Demographics of the Current Sample
| Characteristic | |
|---|---|
| M (SD) | |
| Age | 37 (12) |
| Weight | 191 (45) |
| Reported Gender of Sexual Partners | N (%) |
| Men | 186 (95) |
| Women | 39 (20) |
| Missing | 2 (1) |
| Sexual Orientation | N (%) |
| Gay | 150 (78) |
| Bisexual | 37 (19) |
| Heterosexual | 3 (2) |
| Don’t know | 1 (0) |
| Other | 2 (1) |
| Missing | 2 (1) |
| Race | N (%) |
| White | 130 (70) |
| Black | 39 (21) |
| Asian | 4 (2) |
| Multi-racial/other | 14 (8) |
| Missing | 8 (4) |
| Ethnicity | N (%) |
| Hispanic/Latino | 31 (16) |
| Not Hispanic/Latino | 164 (84) |
| Education | N (%) |
| Did not complete high school | 9 (5) |
| High school diploma/GED | 34 (17) |
| Some college | 49 (25) |
| Associate’s/technical degree | 23 (12) |
| Bachelor’s degree | 35 (18) |
| Some graduate school | 11 (6) |
| Master’s degree | 24 (12) |
| Doctorate degree | 10 (5) |
| Income | N (%) |
| Less than $10,000 | 51 (26) |
| $10,000–$19,999 | 39 (20) |
| $20,000–$29,999 | 18 (9) |
| $30,000–$39,999 | 20 (10) |
| $40,000–$49,999 | 15 (8) |
| $50,000–$59,999 | 16 (8) |
| $60,000–$69,999 | 11 (6) |
| Greater than $70,000 | 23 (12) |
| Missing | 2 (1) |
Figure 1.
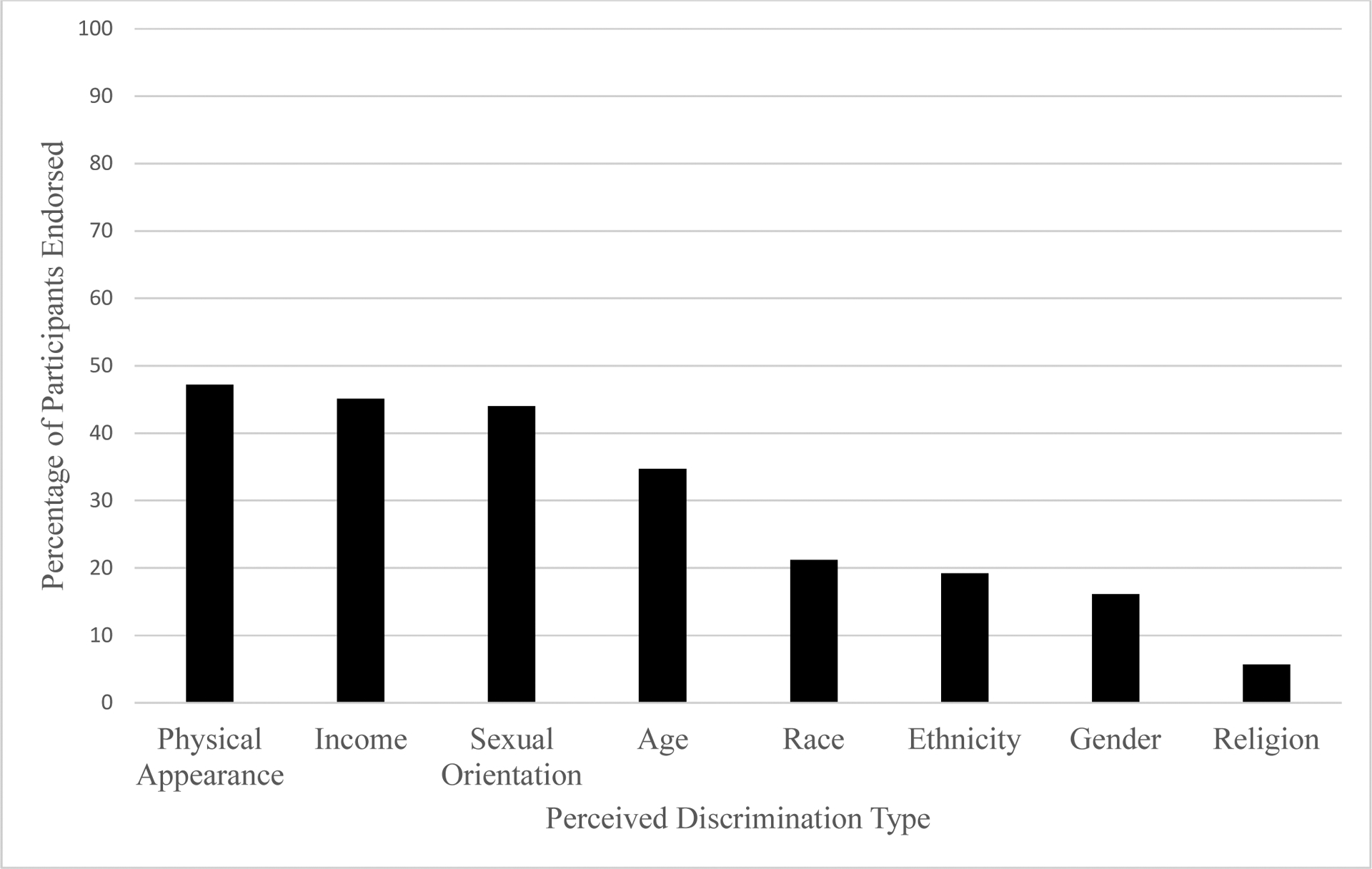
Frequency of perceived discrimination by domain of discrimination.
Table 2.
Correlation Matrix for all Variables Involved in Analysis
| Binge eating | Physical Appearance Dis. | Income Dis. | Religious Dis. | Age Dis. | Racial Dis. | Ethnicity Dis. | Gender Dis. | Sexual Orientation Dis. | Age | Income | Ethnicity | Sexual Orientation | Race | Education | Weight | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Binge eating | — | |||||||||||||||
| Physical Appearance Dis. | .20** | — | ||||||||||||||
| Income Dis. | .03 | .39** | — | |||||||||||||
| Religious Dis. | .00 | .25** | .32** | — | ||||||||||||
| Age Dis. | .00 | .35** | .31** | .43** | — | |||||||||||
| Racial Dis. | .14* | .15* | .10 | .16* | .19** | — | ||||||||||
| Ethnicity Dis. | .13 | .19** | .10 | .25** | .24** | .49** | — | |||||||||
| Gender Dis. | .03 | .42** | .28** | .47** | .38** | .31** | .24** | — | ||||||||
| Sexual Orientation Dis. | .00 | .32** | .16* | .30** | .24** | .26** | .17* | .47** | — | |||||||
| Age | .08 | −.08 | −.08 | −.10 | −.15 | .05 | −.07 | −.11 | −.04 | — | ||||||
| Income | −.05 | .01 | .01 | −.12 | −.03 | −.11 | −.06 | −.16* | −.15* | .15* | — | |||||
| Ethnicity | .02 | −.14* | −.08 | .00 | −.08 | .12 | .26** | −.05 | .02 | −.09 | .10 | — | ||||
| Sexual Orientation | .15* | −.15* | −.02 | .04 | −.05 | .09 | .02 | .03 | .02 | .15* | −.31** | .23** | — | |||
| Race | −.09 | .17* | .20** | .00 | .13 | −.42** | −.21** | −.06 | −.06 | −.08 | .32** | −.07 | −.16* | — | ||
| Education | −.02 | −.05 | −.05 | −.01 | −.04 | −.03 | −.03 | −.03 | −.05 | −.04 | −.04 | −.03 | −.01 | .05 | — | |
| Weight | .04 | .17* | −.03 | −.04 | −.06 | .01 | −.04 | −.03 | .03 | .31* | −.04 | −.09 | −.01 | .05 | .04 | — |
Note.
p < .05,
p < .01,
Discrimination count scores ranged from 0–9; Ethnicity was coded as 0 for “Not Hispanic/Latino” and 1 for “Hispanic/Latino”; Sexual orientation was coded as 0 for “Gay” and 1 for “Other”; Race was coded as 0 for “White” and 1 for “Other”; Income was treated as an ordinal variable; Education was coded as 0 for “High school diploma or less” and 1 for “Other.”
A hierarchical binary logistic regression model with three steps was employed to test the contributions of discrimination and sociodemographic variables in predicting the odds of binge eating; Table 3 shows the results of these analyses. In Step 1 (Nagelkerke’s R2 = .08, model χ2 (1) = 6.27, p = .012), physical appearance discrimination was positively associated with binge eating, OR = 1.31, 95% CI = [1.07, 1.60], Wald χ2 (1) = 6.87, p = .009. In Step 2, after adding all other forms of discrimination (Nagelkerke’s R2 = .15, Step 2 χ2 (7) = 6.67 p = .464; model χ2 (8) = 12.94, p = .114), physical appearance discrimination remained significantly positively associated with binge eating, OR = 1.50, 95% CI = [1.14, 1.97], Wald χ2 (1) = 8.51, p = .004. No other forms of discrimination were statistically significant in this Step. In Step 3, with the inclusion of additional sociodemographic covariates such as education level, income, sexual orientation, race, ethnicity, and weight (Nagelkerke’s R2 = .28, Step 3 χ2 (7) = 11.91, p = .103; model χ2 (15) = 24.85, p = .052), physical appearance discrimination was still significantly positively associated with binge eating, OR = 1.71, 95% CI = [1.24, 2.35], Wald χ2 (1) = 10.65, p = .001. Here too, no other forms of discrimination were statistically significant in this final step.
Table 3.
Summary of Hierarchical Logistic Regression Analysis for Variables Predicting Binge Eating
| Variable | OR | 95% CI | Wald χ2 | R2 a | ΔR2 a |
|---|---|---|---|---|---|
| Step 1: Physical Appearance Discrimination | 1.31 | [1.07, 1.60] | 6.78** | .08 | |
| Step 2: Discrimination variables | .15 | .07 | |||
| Physical Appearance | 1.50 | [1.14, 1.97] | 8.51** | ||
| Income | 0.95 | [0.66, 1.36] | 0.81 | ||
| Religious | 1.26 | [0.48, 3.31] | 0.21 | ||
| Age | 0.90 | [0.59, 1.39] | 0.22 | ||
| Racial | 1.31 | [0.97, 1.78] | 3.05 | ||
| Ethnicity | 1.13 | [0.81, 1.57] | 0.48 | ||
| Gender | 0.68 | [0.35, 1.33] | 1.33 | ||
| Sexual Orientation | 0.84 | [0.59, 1.18] | 1.01 | ||
| Step 3: Discrimination and demographic variables | .28 | .13 | |||
| Discrimination | |||||
| Physical Appearance | 1.71 | [1.24, 2.35] | 10.65** | ||
| Income | 0.98 | [0.67, 1.43] | 0.15 | ||
| Religious | 1.12 | [0.34, 3.67] | 0.03 | ||
| Age | 0.84 | [0.53, 1.32] | 0.61 | ||
| Racial | 1.23 | [0.85, 1.78] | 1.16 | ||
| Ethnicity | 1.28 | [0.87, 1.88] | 1.59 | ||
| Gender | 0.70 | [0.36, 1.36] | 1.10 | ||
| Sexual Orientation | 0.85 | [0.60, 1.20] | 0.87 | ||
| Demographics | |||||
| Age | 1.02 | [0.96, 1.09] | 0.57 | ||
| Income | 1.09 | [0.80, 1.48] | 0.28 | ||
| Ethnicity | 1.67 | [0.27, 10.21] | 3.37 | ||
| Sexual Orientation | 2.42 | [0.55, 10.66] | 0.88 | ||
| Race | 1.69 | [0.32, 9.02] | 0.85 | ||
| Education | 0.13 | [0.24, 0.64] | 6.26* | ||
| Weight | 1.00 | [0.99, 1.02] | 0.21 | ||
Note. OR = odds ratio; CI = confidence interval;
p < .05,
p < .01,
p < .001;
Discrimination count scores ranged from 0–9; Ethnicity was coded as 0 for “Not Hispanic/Latino” and 1 for “Hispanic/Latino”; Sexual orientation was coded as 0 for “Gay” and 1 for “Other”; Race was coded as 0 for “White” and 1 for “Other”; Income was treated as an ordinal variable; Education was coded as 0 for “High school diploma or less” and 1 for “Other.”
Nagelkerke R2 is reported.
4. Discussion
The current study examined binge eating in a sample of SMM. Furthermore, to our knowledge, this was the first study to examine the association between physical appearance discrimination and binge eating, controlling for other salient forms of discrimination. Results indicated that binge eating was present in 9% of the current sample. The frequency of binge eating in the current sample was lower than found in past studies, which reported frequencies of 21.2% among 16-year old SMM in the UK, and 38.1% among US undergraduate SMM (Calzo et al., 2018; Von Schell et al., 2018). This lower frequency of binge eating may be due to the higher average age of participants in the current sample (M = 37), as binge eating frequency has shown to decline with age in men (Abebe, Lien, Torgersen, von Soest, 2012). Notably, a sample of 21,743 US adult men of unspecified sexual orientation with an average age similar to that of the current study (M = 44) displayed a comparable frequency of binge eating (7.5%), demonstrating the impact that age has on the frequency of binge eating behavior (Striegel, Bedrosian, Wang, & Schwartz, 2011). Furthermore, items that assessed binge eating in the current study determined if participants ‘often’ endorsed aspects of binge eating. Perhaps, participants did not have sufficient information as to what frequency constitutes binge eating ‘often’ and therefore indicated that they did not participate in binge eating, potentially explaining its lower frequency in the current study compared to past research. Future studies that examine the association between binge eating and physical appearance discrimination via the PHQ may want to specifically define what is considered binge eating ‘often,’ in order to more accurately compare frequencies of binge eating across studies with samples of SMM. Additionally, the frequency of reported discrimination in the current sample was strikingly high. Forty-seven percent of participants reported at least one instance of physical appearance discrimination, 45% reported at least one instance of discrimination based on income, and 44% reported sexual orientation discrimination. The elevated frequency of physical appearance discrimination in the current sample, along with its unique associated with binge eating, provides evidence that physical appearance discrimination is a salient construct for SMM, and therefore should be included in future comparative studies of discrimination among SMM.
The current study included and compared different forms of discrimination in a multiple regression model, parsing out the unique association of physical appearance discrimination with binge eating, while controlling for other forms of discrimination. Endorsing appearance-based discrimination was associated with greater odds of binge eating both alone and while controlling for other forms of discrimination/sociodemographic variables. It is important to note that appearance-based discrimination was the only significant form of discrimination associated with binge eating, and the inclusion of weight as a covariate did not change these results. Past research has found that individuals who binge eat at subclinical/clinical levels tend to have higher BMIs and levels of obesity than non-binge eaters (e.g., Striegel-Moore et al., 2000), and thus individuals with higher body weights may experience greater appearance-based discrimination due to this higher weight status, a pattern that has been reported with regard to weight-based stigma (Puhl & Brownwell, 2006; Watt & Carels, 2010). Indeed, the cyclic obesity/weight-based stigma model (COBWEBS; Tomiyama, 2014) posits that individuals with higher body weights experience more instances of discrimination, leading to increased caloric consumption for affect regulation and/or in response to cortisol increases, which may cause additional weight gain. However, weight was not a significant contributor to binge eating in the current study, supporting findings that levels of binge/purge eating pathology did not significantly differ among obese/non-obese individuals who binge eat (Didie & Fitzgibbon, 2005; Barry, Grilo, Masheb, 2003). However, it is unclear if this phenomenon generalizes outside of the current sample of SMM. Regardless, results of the current study suggest that weight may not be a salient predictor of binge eating among SMM, and that physical appearance discrimination may contribute to binge eating above weight in this sample. However, the current study did not assess height, thus, BMI was not able to be calculated. Future research should investigate the association between physical appearance discrimination and binge eating in a SMM sample, controlling for BMI, to confirm the current pattern of results.
One theoretical explanation as to why physical appearance discrimination was associated with binge eating in the current study is emotion dysregulation theory. This theory suggests that negative affect from various stressors causes such serious pain and emotional distress that individuals look for ways to escape from their current situation (e.g., Linehan, 1993). Physical appearance discrimination may lead to negative affect, potentially motivating targets of discrimination to seek momentary relief from this negative affect through coping behavior(s) such as binge eating. Difficulties in regulating negative emotions have been associated with loss of control eating in a sample of US youths, and an association has been found between emotion dysregulation items and BN symptoms (such as binge eating) in adults with clinical/subclinical BN (Czaja, Rief, & Hilbert, 2009; Lavender et al., 2014). Notably, emotion dysregulation has been associated with binge eating in SM samples, who are more likely to experience discrimination than heterosexual individuals (Mason & Lewis, 2015; Conner, Johnson, & Grogan, 2004). Therefore, the association between physical appearance discrimination and binge eating in the current study may have been the product of emotion dysregulation. However, given the cross-sectional design and lack of emotion dysregulation items in the current study, this association is speculative. Future research should test these associations longitudinally with a mediation model, in order to determine if emotion dysregulation is driving the association between physical appearance discrimination and binge eating in SMM.
Of note, this was only the second known study to utilize a measure of physical appearance discrimination (Grollman, 2014). In contrast to prior studies that employed weight-based discrimination, using physical appearance broadened this construct to include additional appearance-based attributes such as shape or physique. This is particularly relevant when studying men, who tend to internalize and pursue the mesomorphic body ideal (Karazsia, Dulmen, Wong, & Crowther, 2013). The mesomorphic ideal emphasizes high muscle volume with low levels of body fat (Pope, Phillips, & Olivardia, 2000). Men who embody the mesomorphic ideal may possess high BMIs, which is largely a function of muscle mass in lieu of adiposity. Therefore, ‘weight’ itself may not be as salient as ‘appearance’ in achieving the ideal male physique (Ridgeway & Tylka, 2005). Additionally, gay men have previously reported a greater desire to be both lean and muscular than heterosexual men (Tiggemann, Martins, & Kirkbride, 2007), as well as reporting specific appearance concerns such as height, penis size, or body hair (Martins et al., 2008). Thus, using the construct of physical appearance discrimination in lieu of weight-based discrimination may be more relevant for the concerns routinely endorsed in SMM.
The findings of the current study should be interpreted with the following limitations in mind. First, the design was cross-sectional, precluding any causal or temporal inferences. Second, the current study utilized a sample of SMM that were enrolled in a larger program piloting an at-home HIV test, who also had to report at least one instance of sexual risk behaviors within the past 6-months. Therefore, the current results may not be generalizable to SMM more broadly and may be limited to SMM who report some level of sexual risk and are aware of their HIV status. Third, discrimination was assessed via self-report, which may weaken the accuracy of the reported frequencies of discrimination. Collecting data on discrimination via self-report may result in difficulties in memory regarding discriminatory events as well as difficulties in domain attribution during instances of interpersonal discrimination (i.e., higher weight African American women may report that discrimination is due to race more so than weight, even if the act of discrimination was truly regarding weight status; Lewis, Cogburn, & Williams, 2015). Additionally, physical appearance discrimination may be acting as a proxy for body dissatisfaction and/or weight bias internalization, as body dissatisfaction has been identified as a longitudinal predictor of binge eating (e. g., Wertheim, Koerner, & Paxton, 2001), and weight-bias internalization has repeatedly been associated with binge eating (Puhl, Moss-Racusin, & Schwartz, 2007; Schvey & White, 2015). However, upon testing a cross-sectional mediation model, perceived discrimination was found to have an indirect effect on a latent eating disturbance variable (inclusive of binge eating and body dissatisfaction) via its association with weight bias internalization, with the caveat that this indirect association was present among overweight/obese individuals only (Durso, Latner, & Hayashi, 2012). This may suggest that physical appearance discrimination, an expansion upon weight discrimination, is at least partially disentangled from these established predictors of binge eating in non-obese samples, and may not simply be acting as a proxy for these variables; however, additional prospective research is needed to clarify these associations. Lastly, binge eating behavior was assessed through the PHQ-ED, a self-report measure. Given that prior studies comparing self-report to clinician-administered measures have noted significant discrepancies in binge eating frequency (e.g., Berg, Peterson, Frazier, & Crow, 2011), future research should investigate the association between physical appearance discrimination and binge eating utilizing clinician-administered measures of eating pathology.
Additional research should be conducted in order to replicate the novel findings of the current study. If the current results are confirmed by additional prospective research, this may indicate that appearance-based discrimination is a risk factor for binge eating amongst SMM. Furthermore, future longitudinal research may wish to explore mediators of the reported association between physical appearance discrimination and binge eating. Some potential mediators of this association include body dissatisfaction, weight bias internalization, and mesomorphic ideal internalization. Due to the association that physical appearance discrimination displayed with binge eating in the current study, future research should analyze its association with other forms of eating pathology, particularly purging, fasting, or other extreme weight control behaviors. In addition, future research should examine the association of physical appearance discrimination with binge eating in samples of varying demographics, including women and heterosexual men, in order to ascertain whether this effect generalizes beyond SMM.
The results from the current study may impart certain implications regarding the assessment and development of binge eating. The most salient finding is that appearance-based discrimination was relevant for binge eating in SMM, over and above the effect of sexual orientation discrimination. Therefore, clinicians may benefit from assessing physical appearance discrimination among their SMM patients so as not to assume that sexual orientation discrimination is the most prevalent or predictive form of discrimination for binge eating. Additionally, clinicians may consider providing strategies for coping with appearance discrimination as indicated. If clinicians can effectively provide tools for coping with appearance discrimination, this may reduce binge eating among vulnerable populations such as SMM. However, mechanisms through which physical appearance discrimination may lead to binge eating need to be identified in future research, in order to guide these coping strategies presented by clinicians.
In conclusion, the current study was the first study to examine the association of physical appearance discrimination with binge eating among SMM. At least one instance of physical appearance discrimination was reported by 47% of the current sample of SMM, and this form of discrimination was positively associated with increased odds of binge eating, above all other forms of discrimination and sociodemographic covariates. The presence of physical appearance discrimination may be related to binge eating; therefore, future research should examine this association longitudinally to elucidate the temporal ordering of these variables.
Acknowledgment
Author time was supported by Grant 9K24DA040489 (Safren). This work was supported by NIH grant P01 AI074415, an unrestricted research grant from the Harvard University Center for AIDS Research. We thank Julia Tomassilli for her assistance in managing this cohort. All authors are responsible for reported research and have participated in the concept and design, analysis and interpretation of data, drafting or revising, and have approved this manuscript as submitted.
Footnotes
Publisher's Disclaimer: This is a PDF file of an article that has undergone enhancements after acceptance, such as the addition of a cover page and metadata, and formatting for readability, but it is not yet the definitive version of record. This version will undergo additional copyediting, typesetting and review before it is published in its final form, but we are providing this version to give early visibility of the article. Please note that, during the production process, errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
Declaration of interests
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Previous Peer Review: This manuscript has previously been under peer review, and has been rejected once before. One of the chief concerns was our explanation of physical appearance discrimination versus weight-based discrimination. We have defined each and how they are distinct from one another, making sure to not conflate these terms. Further, we have provided examples of each different type of discrimination (race, ethnicity, sexual orientation, etc.) and how they are associated with distress or eating pathology. Another concern was the presentation of our results in the tables, which we have addressed by clearly defining all variables in a legend for ease of interpretation. We also have presented the discussion in a clear way in order to not appear redundant in the interpretation of our findings. We believe these changes and our current manuscript can potentially add to Appetite and we look forward to it’s review.
References
[dataset] Due to the sensitive nature of the questions asked in this study, survey respondents were assured raw data would remain confidential and would not be shared.
- Abebe DS, Lien L, Torgersen L, & von Soest T (2012). Binge eating, purging and non-purging compensatory behaviours decrease from adolescence to adulthood: A population-based, longitudinal study. BMC Public Health, 12(32), 1–10. doi: 10.1186/1471-2458-12-32 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Austin SB, Ziyadeh NJ, Corliss HL, Rosario M, Wypij D, Haines J,… Field AE (2009). Sexual orientation disparities in purging and binge eating from early to late adolescence. The Journal of Adolescent Health: Official Publication of the Society for Adolescent Medicine, 45(3), 238–245. doi: 10.1016/j.jadohealth.2009.02.001 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bastos JL, Celeste RK, Faerstein E, & Barros AJD (2010). Racial discrimination and health: A systematic review of scales with a focus on their psychometric properties. Social Science and Medicine, 70, 1091–1099. doi: 10.1016/j.socscimed.2009.12.020 [DOI] [PubMed] [Google Scholar]
- Barry DT, Grilo CM, & Mashed RM (2003). Comparison of patients with bulimia nervosa, obese patients with binge eating disorder, and nonobese patients with binge eating disorder. Journal of Nervous and Mental Disease, 191(9), 589–594. doi: 10.1097/01.nmd.0000087185.95446.65 [DOI] [PubMed] [Google Scholar]
- Berg KC, Peterson CB, Frazier P, & Crow SJ (2011). Convergence of scores on the interview and questionnaire versions of the Eating Disorder Examination: A meta-analytic review. Psychological Assessment, 23, 714–724. doi: 10.1037/a0023246 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Blashill AJ, Tomassilli J, Biello K, O’Cleirigh C, Safren SA, & Mayer KH (2016). Body dissatisfaction among sexual minority men: Psychological and sexual health outcomes. Archives of Sexual Behavior, 45, 1241–1247. doi: 10.1007/s10508-015-0683-1 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borders A, & Liang CTH (2011). Rumination partially mediates the associations between perceived ethnic discrimination, emotional distress, and aggression. Cultural Diversity and Ethnic Minority Psychology, 17, 125–133. doi: 10.1037/a0023357 [DOI] [PubMed] [Google Scholar]
- Calzo JP, Austin SB & Micali N (2018). Sexual orientation disparities in eating disorder symptoms among adolescent boys and girls in the UK. European Child Adolescent Psychiatry, 27, 1483–1490. doi: 10.1007/s00787-018-1145-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calzo JP, Blashill AJ, Brown TA, & Argenal RL (2017). Eating disorders and disordered weight and shape control behaviors in sexual minority populations. Current Psychiatry Reports, 19(49), 1–10. doi: 10.1007/s11920-017-0801-y [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calzo JP, Masyn KE, Corliss HL, Scherer EA, Field AE, & Austin SB (2015). Patterns of body image concerns and disordered weight- and shape-related behaviors in heterosexual and sexual minority adolescent males. Developmental Psychology, 51, 1216–1225. doi: 10.1037/dev0000027 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Conner M, Johnson C, & Grogan S (2004). Gender, sexuality, body image and eating behaviours. Journal of Health Psychology, 9(4), 505–515. doi: 10.1177/1359105304044034 [DOI] [PubMed] [Google Scholar]
- Czaja J, Rief W, & Hilbert A (2009). Emotion regulation and binge eating in children. International Journal of Eating Disorders, 42, 356–362. doi: 10.1002/eat.20630 [DOI] [PubMed] [Google Scholar]
- Didie ER, & Fitzgibbon M (2005). Binge eating and psychological distress: Is the degree of obesity a factor? Eating Behaviors, 6(1) 35–41. doi: 10.1016/j.eatbeh.2004.08.007 [DOI] [PubMed] [Google Scholar]
- Durso LE, Latner JD, & Hayashi K (2012). Perceived discrimination is associated with binge eating in a community sample of non-overweight, overweight, and obese adults. Obesity Facts, 5, 869–880. doi: 10.1159/000345931 [DOI] [PubMed] [Google Scholar]
- Eichen DM, Chen E, Boutelle KN, & McCloskey MS (2017). Behavioral evidence of emotion dysregulation in binge eaters. Appetite, 111, 1–6. doi: 10.1016/j.appet.2016.12.021 [DOI] [PubMed] [Google Scholar]
- Every D & Perry R (2014), Discrimination, self-esteem, and Muslim Australians. Australian Journal of Psychology, 66, 241–248. doi: 10.1111/ajpy.12067 [DOI] [Google Scholar]
- Firth D (1993). Bias reduction of maximum likelihood estimates. Biometrika, 80, 27–38. doi: 10.1093/biomet/80.1.27 [DOI] [Google Scholar]
- Gamarel KE, Reisner SL, Parsons JT, & Golub SA (2012). Association between socioeconomic position discrimination and psychological distress: Findings from a community-based sample of gay and bisexual men in New York City. American journal of Public Health, 102(11), 2094–2101. doi: 10.2105/AJPH.2012.300668 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gordon AR, Kenney EL, Haines J, Ziyadeh N, Calzo JP, Rosario M, & Austin B (2018). Weight-based discrimination and disordered eating behaviors among U.S. sexual minority adolescents and young adults. Journal of Adolescent Health, 62, S1. doi: 10.1016/j.jadohealth.2017.11.005 [DOI] [Google Scholar]
- Grollman EA (2014). Multiple disadvantaged statuses and health: The role of multiple forms of discrimination. Journal of Health and Social Behavior, 55, 3–19. doi: 10.1177/0022146514521215 [DOI] [PubMed] [Google Scholar]
- Himmelstein MS, Puhl RM, & Watson RJ (2019). Weight-based victimization, eating behaviors, and weight-related health in sexual and gender minority adolescents. Appetite, doi: 10.1016/j.appet.2019.104321 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hurst RJ, & Beesley D Perceived sexism, self-silencing, and psychological distress in college women. Sex Roles 68, 311–320. doi: 10.1007/s11199-012-0253-0 [DOI] [Google Scholar]
- Kamody RC, Grilo CM, & Udo T (2019). Disparities in DSM-5 defined eating disorders by sexual orientation among U.S. adults. International Journal of Eating Disorders, 1–10. doi: 10.1002/eat.23193 [DOI] [PubMed] [Google Scholar]
- Karazsia BT, van Dulmen MHM, Wong K, & Crowther JH (2013). Thinking meta-theoretically about the role of internalization in the development of body dissatisfaction and body change behaviors. Body Image, 10, 433–441. doi: 10.1016/j.bodyim.2013.06.005 [DOI] [PubMed] [Google Scholar]
- Katz-Wise SL, Scherer EA, Calzo JP, Sarda V, Jackson B, Haines J, & Austin SB (2015). Sexual minority stressors, internalizing symptoms, and unhealthy eating behaviors in sexual minority youth. Annals of Behavioral Medicine, 49, 839–852. doi: 10.1007/s12160-015-9718-z [DOI] [PMC free article] [PubMed] [Google Scholar]
- King G, & Zeng L (2001). Logistic regression in rare events data. Political Analysis, 9, 137–163. doi: 10.1093/oxfordjournals.pan.a004868 [DOI] [Google Scholar]
- Lavender JM, Wonderlich SA, Peterson CB, Crosby RD, Engel SG, Mitchell JE,…Berg KC (2014). Dimensions of emotion dysregulation in Bulimia Nervosa. European Eating Disorders Review, 22, 212–216. doi: 10.1002/erv.2288 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Leitgöb H (2013, July). The problem of modeling rare events in ML-based logistic regression - assessing potential remedies via MC simulations Poster presented at the European Survey Research Association Conference, Ljubljana, Slovenia. [Google Scholar]
- Levesque MJ, & Vichesky DR (2006). Raising the bar on the body beautiful: An analysis of the body image concerns of homosexual men. Body Image, 3(1), 45–55. doi: 10.1016/j.bodyim.2005.10.007 [DOI] [PubMed] [Google Scholar]
- Lewis TT, Cogburn CD, & Williams DR (2015). Self-reported experiences of discrimination and health: Scientific advances, ongoing controversies, and emerging issues. Annual Review of Clinical Psychology, 11, 407–440. doi: 10.1146/annurev-clinpsy-032814-112728 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Linehan MM (1993). Diagnosis and treatment of mental disorders Skills training manual for treating borderline personality disorder. New York, NY, US: Guilford [Google Scholar]
- Martins Y, Tiggemann M, & Churchett L (2008). The shape of things to come: Gay men’s satisfaction with specific body parts. Psychology of Men & Masculinity, 9(4), 248–256. doi: 10.1037/a0012473 [DOI] [Google Scholar]
- Mason TB, & Lewis RJ (2015) Minority stress and binge eating among Lesbian and Bisexual women. Journal of Homosexuality, 62(7), 971–992. doi: 10.1080/00918369.2015.1008285 [DOI] [PubMed] [Google Scholar]
- Matthews-Ewald MR, Zullig KJ, & Ward RM (2014). Sexual orientation and disordered eating behaviors among self-identified male and female college students. Eating Behaviors, 15, 441–444. doi: 10.1016/j.eatbeh.2014.05.002 [DOI] [PubMed] [Google Scholar]
- McLeod SA (2008). Prejudice and discrimination. Simply Psychology. https://www.simplypsychology.org/prejudice.html [Google Scholar]
- Meyer IH (2003). Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin, 129, 674–697. doi: 10.1037/0033-2909.129.5.674 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pope HG, Phillips KA, & Olivardia R (2000). The Adonis Complex: The Secret Crisis of Male Body Obsession. New York, New York: The Free Press. [Google Scholar]
- Puhl RM, & Brownwell KD (2006). Confronting and coping with weight stigma: An investigation of overweight and obese results. Obesity, 14(10), 1802–1815. doi: 10.1038/oby.2006.208 [DOI] [PubMed] [Google Scholar]
- Puhl RM, Moss-Racusin CA, & Schwartz MB (2007). Internalization of weight bias: Implications for binge eating and emotional well-being. Obesity, 15(1), 19–23. doi: 10.1038/oby.2007.521 [DOI] [PubMed] [Google Scholar]
- Ridgeway RT, & Tylka TL (2005). College men’s perceptions of ideal body composition and shape. Psychology of Men and Masculinity, 6, 209–220. doi: 10.1037/1524-9220.6.3.209 [DOI] [Google Scholar]
- Safren SA, Blashill AJ, Lee JS, O’Cleirigh C, Tomassili J, Biello KBJ, … Mayer KH (2018). Condom-use self-efficacy as a mediator between syndemics and condomless sex in men who have sex with men (MSM). Health Psychology, 37, 820–827. doi: 10.1037/hea0000617 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schvey NA, & White MA (2015). The internalization of weight bias is associated with severe eating pathology among lean individuals. Eating Behaviors, 17, 1–5. doi: 10.1016/j.eatbeh.2014.11.001Get [DOI] [PubMed] [Google Scholar]
- Shearer A, Russon J, Herres J, Atte T, Kodish T, & Diamond G (2015). The relationship between disordered eating and sexuality amongst adolescents and young adults. Eating Behaviors, 19, 115–119. doi: 10.1016/j.eatbeh.2015.08.001 [DOI] [PubMed] [Google Scholar]
- Smith AR, Hawkeswood SE, Bodell LP, & Joiner TE (2011). Muscularity versus leanness: An examination of body ideals and predictors of disordered eating in heterosexual and gay college students. Body Image, 8, 232–236. doi: 10.1016/j.bodyim.2011.03.005 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Spitzer RL, Kroenke K, & Williams JB (1999). Validation and utility of a self-report version of PRIME-MD. Journal of the American Medical Association, 282, 1737–1744. doi: 10.1001/jama.282.18.1737 [DOI] [PubMed] [Google Scholar]
- Striegel RH, Bedrosian R, Wang C, & Schwartz S (2011). Why men should be included in research on binge eating: Results from a comparison of psychosocial impairment in men and women. International Journal of Eating Disorders, 45(2), 233–240. doi: 10.1002/eat.20962 [DOI] [PubMed] [Google Scholar]
- Striegel-Moore RH, Dohm FA, Solomon EE, Fairburn CG, Pike KM,…Wilfley DE (2000). Subthreshold binge eating disorder. International Journal of Eating Disorders, 27, 270–278. doi: 10.1002/(SICI)1098-108X [DOI] [PubMed] [Google Scholar]
- Striegel-Moore RH, Rosselli F, Perrin N, DeBar L, Wilson TG, May A,…Kraemer HC (2009). Gender difference in the prevalence of eating disorder symptoms. The International Journal of Eating Disorders, 42, 471–474. doi: 10.1002/eat.20625 [DOI] [PMC free article] [PubMed] [Google Scholar]
- Todorova IL, Falcón LM, Lincoln AK & Price LL (2010), Perceived discrimination, psychological distress and health. Sociology of Health & Illness, 32, 843–861. doi: 10.1111/j.1467-9566.2010.01257.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- Tomiyama AJ (2014). Weight stigma is stressful. A review of evidence for the cyclic obesity/weight-based stigma model. Journal of Appetite, 82, 8–15. doi: 10.1016/j.appet.2014.06.108 [DOI] [PubMed] [Google Scholar]
- Tiggemann M, Martins Y, & Kirkbride A (2007). Oh to be lean and muscular: Body image ideals in gay and heterosexual men. Psychology of Men & Masculinity, 8, 15–24. doi: 10.1037/1524-9220.8.1.15 [DOI] [Google Scholar]
- Vogt Yuan AS (2007). Perceived age discrimination and mental health. Social Forces, 86(1), 291–311. doi: 10.1353/sof.2007.0113 [DOI] [Google Scholar]
- Von Schell A, Ohrt TK, Bruening AB, & Perez M (2018). Rates of disordered eating behaviors across sexual minority undergraduate men and women. Psychology of Sexual Orientation and Gender Diversity, 5(3), 352–359. doi: 10.1037/sgd0000278 [DOI] [Google Scholar]
- Wang SB & Borders A (2017). Rumination mediates the associations between sexual minority stressors and disordered eating, particularly for men. Eating and Weight Disorders - Studies on Anorexia, Bulimia and Obesity, 22, 699–706. doi: 10.1007/s40519-016-0350-0 [DOI] [PubMed] [Google Scholar]
- Wertheim EH, Koerner J, & Paxton SJ (2001). Longitudinal predictors of restrictive eating and bulimic tendencies in three different age groups of adolescent girls. Journal of Youth and Adolescence, 30, 69–81. doi: 10.1023/A:1005224921891 [DOI] [Google Scholar]
- Williams DR, Yu Y, Jackson JS, & Anderson NB (1997). Racial differences in physical and mental health: Socioeconomic status, stress, and discrimination. Journal of Health Psychology, 2, 335–351. doi: 10.1177/135910539700200305 [DOI] [PubMed] [Google Scholar]
- Wott CB, & Carels RA (2010). Overweight stigma, psychological distress and weight loss treatment outcomes. Journal of Health Psychology, 15(4), 203–209. doi: 10.1177/1359105309355339 [DOI] [PubMed] [Google Scholar]