

ABSTRACT
We present a case of severe symptomatic hyponatremia (94 mEq/L) in a male patient who presented with nausea, vomiting, and multiple falls. The patient was found with symptomatic hypo-osmolar hypovolemic hyponatremia secondary to volume loss from vomiting, diuretic use, and consumption of solute-free water. To manage such a severely hyponatremic patient, concomitant 3% hypertonic saline and DDAVP were initiated with successful slow and sustained correction of sodium without complications of osmotic demyelination syndrome.
KEYWORDS: Hyponatremia, desmopressin, hypertonic saline, osmotic demyelination syndrome
1. Introduction
Severe hyponatremia, defined as serum sodium below 120 mEq/L, can be challenging to treat given untreated severe symptomatic hyponatremia can cause brain herniation [1] while its overcorrection can lead to osmotic demyelination syndrome (ODS) [2]. For patients at high risk for ODS, current expert panel guidelines recommend sodium correction by 4–6 mEq/L per day, even with severe symptoms [3]. Recent studies have advocated the combined use of 3% Hypertonic Saline and Desmopressin Acetate (DDAVP) for correcting severe hyponatremia [4,5]. We present a case of severe symptomatic hyponatremia (94 mEq/L) with a successful outcome with the infrequently used strategy of concomitant hypertonic saline and desmopressin.
2. Case presentation
An 83-year-old male with a history of Diabetes Mellitus Type 2, benign prostatic hyperplasia, and hypertension presented with nausea, vomiting, and multiple falls for several days. Patient reported drinking many glasses of water the day prior to admission and was also recently started on triamterene/hydrochlorothiazide for hypertension. Physical examination was benign. Laboratory data revealed serum sodium of 94 mg/dL; therefore, fluid restriction, concomitant 3% hypertonic saline and DDAVP were initiated in the intensive care unit as per Figure 1. Hypertonic saline was administered as 50 ccs/hr boluses with 2 mg of DDAVP every 6 hours for the first 96 hours until sodium was 113 mEq/L. Despite a hospital course complicated by retroperitoneal hemorrhage requiring transfusion and hypovolemic shock with a resultant acute tubular necrosis, the patient’s sodium slowly corrected to 136 mEq/L. The patient was eventually discharged without long-term neurologic or renal complications.
Figure 1.
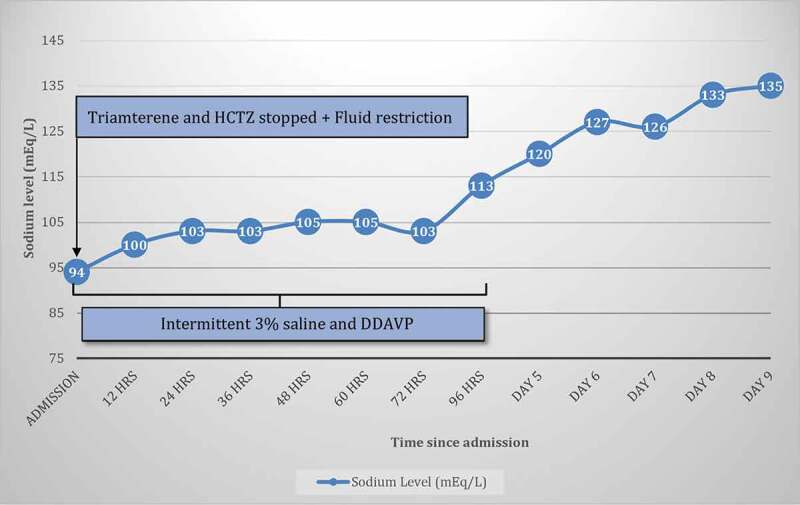
Serum sodium was 94 mEq/L on the day of admission. Triamterene/hydrochlorothiazide was stopped and fluid restriction was initiated on admission. 3% saline was administered intermittently and DDAVP was administered every 6 hours from day 1 until day 4.
3. Discussion
In order to prevent sodium overcorrection and complications of ODS, the commonly practiced reactive/rescue strategy relies on free water and DDAVP to slow sodium correction and prevent further free water diuresis, respectively [6]. Recent literature has suggested the proactive use of 3% hypertonic saline in combination with DDAVP as an efficacious method in correcting severe hyponatremia in a controlled manner [6].
Hyponatremia arises from different etiologies prompting treatments ranging from fluid restriction to hypertonic saline. The above patient presented with symptomatic hypo-osmolar hypovolemic hyponatremia secondary to volume loss from vomiting, diuretic use, and consumption of solute-free water. Hyponatremia secondary to diuretics/SSRIs and hypovolemia often experience a rapid decline in ADH levels and subsequent water diuresis once the offending agents have been removed. Subsequent rapid sodium overcorrection leads to ODS. Hypertonic 3% saline is used to ensure a slow and sustained rise in sodium levels while desmopressin is utilized to prevent free water diuresis [3,6].
For sodium <120 mEq/L, a proactive strategy of using desmopressin in combination with 3% saline [4,6] was found to be successful in correcting sodium in our severely hyponatremic patient. We agree that this proactive strategy is effective in certain hyponatremic patient populations, but future studies are warranted to determine optimal management.
Funding Statement
This work is not supported by any sponsors. No funding required in this study.
Disclosure statement
No potential conflict of interest was reported by the authors.
References
- [1].Arieff AI. Hyponatremia, convulsions, respiratory arrest, and permanent brain damage after elective surgery in healthy women. N Engl J Med. 1986;314(24):1529–1535. [DOI] [PubMed] [Google Scholar]
- [2].Odier C, Nguyen DK, Panisset M.. Central pontine and extrapontine myelinolysis: from epileptic and other manifestations to cognitive prognosis. J Neurol. 2010;257(7):1176–1180. [DOI] [PubMed] [Google Scholar]
- [3].Verbalis JG, Goldsmith SR, Greenberg A, et al. Diagnosis, evaluation, and treatment of hyponatremia: expert panel recommendations. Am J Med. 2013;126:10. [DOI] [PubMed] [Google Scholar]
- [4].Sood L, Sterns RH, Hix JK, et al. Hypertonic saline and desmopressin: a simple strategy for safe correction of severe hyponatremia. Am J Kidney Diseases. 2013;61(4):571–578. [DOI] [PubMed] [Google Scholar]
- [5].Macmillan TE, Tang T, Cavalcanti RB.. Desmopressin to prevent rapid sodium correction in severe hyponatremia: a systematic review. Am J Med. 2015;128:12. [DOI] [PubMed] [Google Scholar]
- [6].Tandukar S, Rondon‐Berrios H. Treatment of severe symptomatic hyponatremia. Physiol Rep. 2019;7:21. [DOI] [PMC free article] [PubMed] [Google Scholar]