

Abstract
Objective: Pulmonary hypertension (PAH) is a serious progressive and fatal pulmonary disease characterized by elevated pulmonary artery pressure. Mechanical sequential ventilation has been gradually applied in the treatment of patients with PAH complicated with RF, which can effectively reduce the incidence of VAP and better promote the recovery of respiratory function. This study is aimed to determine the efficacy of sequential ventilation and conventional invasive mechanical ventilation in the treatment of pulmonary hypertension (PAH) complicated with respiratory failure (RF). Methods: A total of 198 patients with both PAH and RF admitted to our hospital were enrolled. Among them, 102 patients were treated with sequential ventilation as a study group (stu group), and 96 patients were treated with conventional invasive mechanical ventilation as a control group (con group). Then the two groups were compared in efficacy and related indexes before and after treatment. Results: The stu group experienced significantly shorter invasive ventilation time, total mechanical ventilation time, and hospitalization time than the con group (all P<0.05), and showed a significantly lower complication rate than the con group (P<0.05). The reintubation rate, weaning failure rate, and ventilator-associated pneumonia (VAP) rate of the stu group were all significantly lower than those of the con group (all P<0.05), and the stu group showed significantly higher pondus hydrogenii (pH) and arterial partial pressure of oxygen (PaO2) and significantly lower arterial carbondioxide partial pressure (PaCO2) than the con group after treatment (all P<0.05). Additionally, after treatment, the level of brain natriuretic peptide (BNP) and pulmonary artery pressure in both groups declined significantly (P<0.05), and the decline of them in the stu group was more significant than that in the con group (P<0.05). Moreover, after treatment, endothelin (ET) and angiotensin II (Ang II) in both groups declined significantly, and the decline of them in the stu group was also more significant than that in the con group (P<0.05). Conclusion: Compared with conventional invasive mechanical ventilation, sequential ventilation can effectively minimize the treatment time of patients with PAH complicated with RF, reduce the incidences of adverse events and complications in them, and significantly improve the blood gas analysis indexes and BNP in them, so it is worthy of clinical promotion.
Keywords: Sequential ventilation, conventional invasive mechanical ventilation, pulmonary hypertension, respiratory failure, brain natriuretic peptide
Introduction
Pulmonary hypertension (PAH) is a serious progressive and fatal pulmonary disease characterized by elevated pulmonary artery pressure [1]. It is featured by poor remodeling of small pulmonary artery, which results in increased pulmonary vascular resistance [2]. PAH may be idiopathic (IPAH) or familial, induced by drugs and toxins, and may also be related to many diseases including connective tissue disease (CTD), congenital heart disease (CHD), portal hypertension or schistosomiasis [3,4]. The most common PAH includes IPAH (82.35%), and CTD-induced PAH (71.31%), and CHD-related PAH (60.26%) [5]. Patients with PAH usually suffer from respiratory failure (RF), fatigue, and syncope meantime. The increase of right ventricular after load will increase the high risk of right ventricular failure and premature death [6]. Patients with PAH have impaired lung ventilation function, which will lead to hypoxia, and then give rise to RF [7].
Currently, PAH complicated with RF is mainly treated by mechanical ventilation, which establish an artificial airway for patients to control their lung infection to the maximum extent and relieve respiratory muscle fatigue, thus effectively improving their respiratory and pulmonary functions [8]. Conventional invasive mechanical ventilation can quickly restore the smooth of respiratory duct in patients with PAH complicated with RF, reduce the retention of CO2 in the lungs, and thus effectively alleviate clinical symptoms [9]. However, it is traumatic to patients, and it is difficult to tolerate due to long ventilation time, which easily brings about complications such as ventilator-associated pneumonia (VAP) and airway injury, resulting in unsatisfactory clinical efficacy [10]. As science and technology advance, mechanical sequential ventilation has been gradually applied in the treatment of patients with PAH complicated with RF, which can effectively reduce the incidence of VAP and better promote the recovery of respiratory function [11].
This study mainly determined the changes of BNP and pulmonary artery pressure of patients in two groups treated with different mechanical ventilation therapies to determine the efficacy of sequential ventilation and conventional invasive mechanical ventilation in treating PAH complicated with RF, with the goal of providing a theoretical basis for clinical treatment of PAH complicated with RF.
Materials and methods
General data
A total of 198 patients with both PAH and RF admitted to our hospital were enrolled. Among them, 102 patients were treated with sequential ventilation as a study group (stu group), and 96 patients were treated with conventional invasive mechanical ventilation as a control group (con group). The stu group consisted of 68 males and 34 females, with an average age of (52.89±6.43) years, while the con group consisted of 62 males and 34 females, with an average age of (53.02±6.57) years.
The inclusion criteria of the study: Patients accompanied by family members at admission, patients with detailed clinicopathologic data, patients meeting the diagnostic criteria for PAH issued on the World Symposium on Pulmonary Hypertension [12], patients diagnosed as RF according to related examination of blood gas analysis (arterial partial pressure of oxygen (PaO2≤60 mmHg) and arterial carbondioxide partial pressure (PaCO2≥50 mmHg). The exclusion criteria of the study: Patients with a history of mental disease or a family history of psychosis, patients with a history of autoimmune system deficiency or severe organ diseases, patients with pulmonary infection, patients with a history of drug dependence, and those who were unable to cooperate with examination due to aphasia, dysphoria, unconsciousness, or communication obstacle. This study was approved by the Ethics Committee of our hospital, and all patients and their families provided written informed consent after they we informed of the study.
Methods
Patients in the two groups were given routine treatment including anti-inflammation, phlegm dispelling, water-electrolyte balance adjustment, and acid-base balance adjustment, nutritional support, and infected patients among them were treated with routine antibiotics. Patients in the con group were given conventional invasive mechanical ventilation as follows: After tracheotomy, each patient was connected with a ventilator (Jmmedical Equipment Co., Ltd., Shanghai, China) to assist his/her breathing. The ventilator was adjusted to the synchronized intermittent mandatory ventilation (SIMV) mode, and its parameters were set as follows: Tidal volume of 6-12 mL/kg, oxygen concentration of 30%-100%, and respiratory rate of 12-20 beats/min. The SIMV respiratory rate was adjusted in time according to the patient’s specific condition. The ventilator was weaned, and the trachea cannula was withdrawn when the patient was able to breathe spontaneously and his/her symptoms were relieved, with oxygenation index (PaO2/inspired oxygen (FiO2)>150 mmHg. Patients in the stu group were given sequential ventilation as follows: Each patient was connected with a ventilator through orotracheal intubation under the guidance of laryngoscope. The ventilator was set as the volume control mode, and its parameters were set as follows: respiratory rate of 12-20 beats/min, and oxygen concentration of 30%-100%, and tidal volume of 6-12 mL/kg. The blood gas indexes of the patient were determined. The mode of the ventilator was adjusted to SIMV and pressure support mode according to the determination results, and the respiratory rate was adjusted according to the specific condition of the patient. In addition, the trachea cannula in the patient was withdrawn when his/her respiratory function improved, and then bi-level positive pressure ventilation with a mask was adopted to treat the patient. The parameters were gradually adjusted according to the patient’s specific condition. The ventilator was weaned when the patient was able to breathe spontaneously and his/her PaO2/FiO2 was within 200-300 mmHg.
Outcome measures
The treatment time, complications, and adverse events including weaning failure, reintubation and VAP of the two groups were recorded. At 1 day before treatment and 1 day after treatment, arterial and venous blood was sampled from each patient in the two groups, and the arterial blood gas analysis indexes (pondus hydrogenii (pH), PaO2 and PaCO2), brain natriuretic peptide (BNP), pulmonary artery pressure, endothelin (ET) and angiotensin II (Ang II) of patients in the two groups were determined and compared.
Statistical analyses
All statistical analysis of the experimental results was carried out using SPSS20.0 (IBM Corp, Armonk, NY, USA), and all graphical results were drawn by GraPAHPad Prism 7 (Graphpad Software Co., Ltd., San Diego, CA, USA). Enumeration data were expressed as [n (%)] and compared between groups by the chi-square test. Measurement data were expressed as the (x̅ ± sd), and compared between groups using the t test. P<0.05 suggests a significant difference.
Results
Comparison of general data
General data including age, body mass index, smoking history, and drinking history of the two groups were collected, and summarized in Table 1. No notable difference was seen in general data between the two groups (all P>0.05).
Table 1.
Comparison of general clinical data between the two groups (x̅ ± s)/[n (%)]
| The study group (n=102) | The control group (n=96) | t/χ2 | P-value | |
|---|---|---|---|---|
| Age (Y) | 52.89±6.43 | 53.02±6.57 | 0.14 | 0.89 |
| Body mass index (kg/m2) | 22.14±1.34 | 22.35±1.42 | 1.07 | 0.29 |
| Sex | 0.10 | 0.76 | ||
| Male | 68 (66.67) | 62 (64.58) | ||
| Female | 34 (33.33) | 34 (35.42) | ||
| Smoking history | 0.35 | 0.55 | ||
| Yes | 72 (70.59) | 64 (66.67) | ||
| No | 30 (29.41) | 32 (33.33) | ||
| Drinking history | 0.11 | 0.74 | ||
| Yes | 64 (62.75) | 58 (60.42) | ||
| No | 38 (37.25) | 38 (39.58) | ||
| APACHE II score | 21.47±2.48 | 20.89±3.04 | 1.48 | 0.14 |
Note: APACHE II: Acute Physiology and Chronic Health Evaluation II.
Comparison of treatment time between the two groups
Comparison of treatment time between the stu group and the con group showed that the former group experienced significantly shorter invasive ventilation time, total mechanical ventilation time, and hospitalization time than the latter group (all P<0.05) Figure 1.
Figure 1.
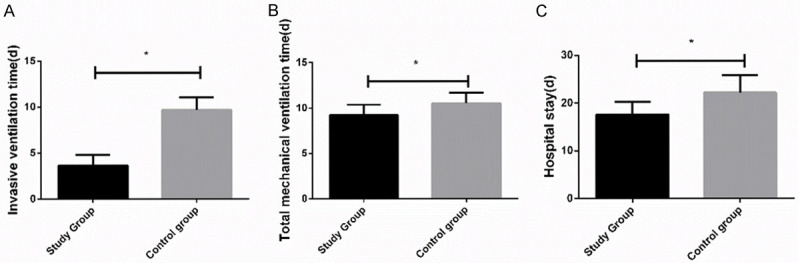
Comparison of treatment time between the two groups. A. The invasive ventilation time consumed by the study group was significantly shorter than that consumed by the control group. B. The total mechanical ventilation time consumed by the study group was significantly shorter than that consumed by the control group. C. The hospitalization time consumed by the study group was significantly shorter than that consumed by the control group. * indicates that in comparison between the two groups, P<0.05.
Comparison of complication rate between the two groups
Comparison of complication rate between the stu group and the con group showed that the complication rate of the former group was significantly lower than that of the latter group (17.65% vs. 30.21%, P<0.05), and complications in the stu group were more self-relieving symptoms such as dry nose and mouth and facial pain Table 2.
Table 2.
Comparison of complication rate between the two groups [n (%)]
| Dry nose and mouth | Facial pain | Respiratory tract infection | Pneumothorax | Patient-ventilator asynchrony | Incidence of complications (%) | |
|---|---|---|---|---|---|---|
| The study group (n=102) | 6 (5.88) | 8 (7.84) | 2 (1.96) | 0 (0.00) | 2 (1.96) | 18 (17.65) |
| The control group (n=96) | 0 (0.00) | 0 (0.00) | 14 (14.58) | 5 (5.21) | 10 (10.42) | 29 (30.21) |
| χ2 | - | - | - | - | - | 4.31 |
| P | - | - | - | - | - | 0.04 |
Incidence of adverse events in the two groups
Comparison of the two groups in the incidence of adverse events showed that the weaning failure rate, reintubation rate, and VAP rate of the stu group were all significantly lower than those of the con group (all P<0.05) Figure 2.
Figure 2.
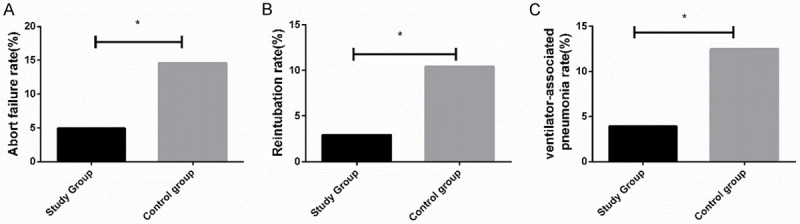
Comparison of the incidence of adverse events between the two groups. A. The weaning failure rate of the study group was significantly lower than that of the control group. B. The reintubation rate of the study group was significantly lower than that of the control group. C. The VAP rate of the study group was significantly lower than that of the control group. * indicates that in comparison of the two groups, P<0.05.
Comparison of blood gas analysis indexes between the two groups before and after treatment
Comparison of the two groups in terms of blood gas analysis indexes before and after treatment showed that before treatment, there was no significant difference between them in blood gas analysis indexes (all P>0.05), while after treatment, the stu group showed significantly higher pH and PaO2 and significantly lower PaCO2 than the con group (all P<0.05) Figure 3.
Figure 3.
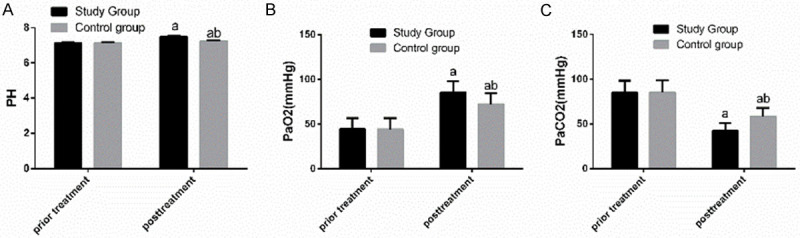
Comparison of blood gas analysis indexes between the two groups before and after treatment. A. Before treatment, there was no notable difference between the two groups in pH, while after treatment, pH of the study group was significantly higher than that of the control group. B. Before treatment, there was no notable difference between the two groups in PaO2, while after treatment, PaO2 of the study group was significantly higher than that of the control group. C. Before treatment, there was no notable difference between the two groups in PaCO2, while after treatment, PaCO2 of the study group was significantly lower than that of the control group. a indicates that in comparison of the same group before and after treatment, aP<0.05. b indicates that in comparison with the study group after treatment, bP<0.05.
Comparison of BNP between the two groups before and after treatment
Comparison of BNP between the two groups before and after treatment showed that before treatment, there was no significant difference between the two groups in BNP (P>0.05), while after therapy, BNP in both groups decreased significantly (both P<0.05), and the decrease in the stu group was more significant than that in the con group (P<0.05) Figure 4.
Figure 4.
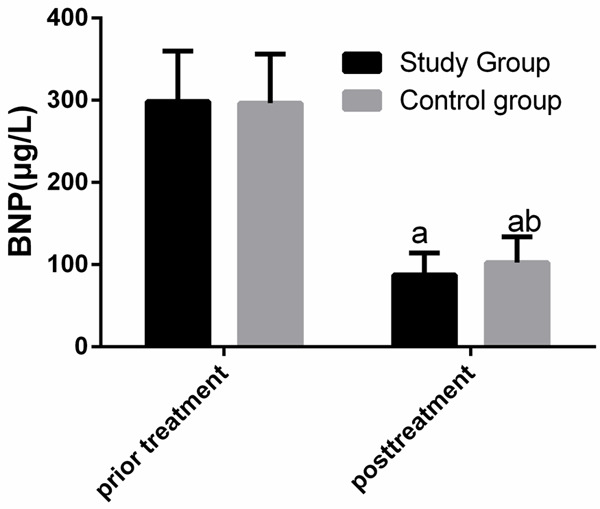
Comparison of BNP between the two groups before and after treatment. Before treatment, there was no significant difference between the two groups in BNP, while after treatment, BNP in both groups decreased significantly, and BNP in the study group was significantly lower than that in the control group. a indicates that in comparison of the same group before and after treatment, aP<0.05. b indicates that in comparison with the study group after treatment, bP<0.05.
Comparison of pulmonary artery pressure between the two groups before and after treatment
Comparison of the two groups in pulmonary artery pressure before and after treatment showed that before treatment, there was no significant difference between the two groups in pulmonary artery pressure (P>0.05), while after treatment, pulmonary artery pressure in both groups decreased significantly (both P<0.05), and the decrease in the stu group was more significant than that in the con group (P<0.05) Figure 5.
Figure 5.
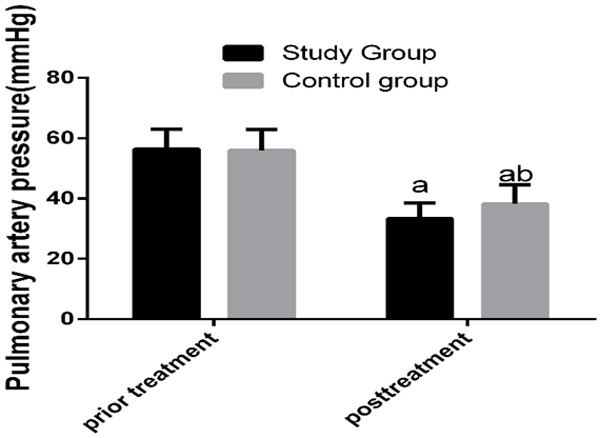
Comparison of pulmonary artery pressure between the two groups before and after treatment. Before treatment, there was no significant difference between the two groups in pulmonary artery pressure, while after treatment, pulmonary artery pressure in both groups decreased significantly, and pulmonary artery pressure in the study group was significantly lower than that in the control group. a indicates that in comparison of the same group before and after treatment, aP<0.05. b indicates that in comparison with the study group after treatment, bP<0.05.
Comparison of ET and Ang II between the two groups before and after treatment
Comparison of ET and Ang II between the two groups before and after treatment showed that before treatment, there was no significant difference between the two groups in ET and Ang II (P>0.05), while after treatment, ET and Ang II in both groups decreased significantly (both P<0.05), and the decrease in the stu group was more significant than that in the con group (P<0.05) See Figure 6.
Figure 6.
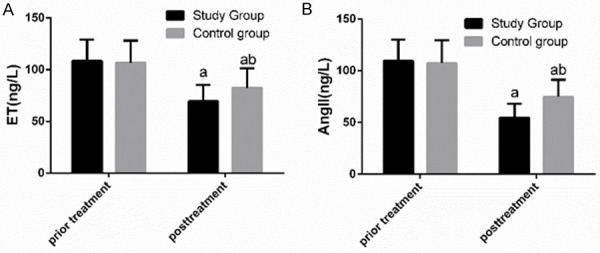
Comparison of ET and Ang II between the two groups before and after treatment. A. Before treatment, there was no notable difference between the two groups in ET, while after treatment, ET of both groups decreased significantly, and ET of the study group was significantly lower than that of the control group. B. Before treatment, there was no notable difference between the two groups in Ang II, while after treatment, Ang II of both groups decreased significantly, and Ang II of the study group was significantly lower than that of the control group. a indicates that in comparison of the same group before and after treatment, aP<0.05. b indicates that in comparison with the study group after treatment, bP<0.05.
Discussion
PAH is a disease syndrome featured by elevated pulmonary artery pressure and pulmonary vascular remodeling. It is not a single disease, but a syndrome involving various acute and chronic diseases due to different origins and causes, which have the common feature of average pulmonary artery pressure above 20-25 mmHg [13]. The 3-year survival rate of patients with PAH is less than 60% [14], and women are more likely to suffer from the disease, but the survival rate of women is higher than that of men [15]. According to one study, there were 384 patients hospitalized for PAH in France in 2013, and there were 1271 patients suffering from PAH-related diseases, which implies that although PAH is rare, it accounts for a high economic burden [16]. Clinically, patients with PAH usually suffer from RF [17]. Currently, PAH complicated with RF is usually treated by mechanical ventilation, so this study was designed to determine the efficacy of sequential ventilation and conventional invasive mechanical ventilation in treating PAH complicated with RF.
In this study, the invasive ventilation time, total mechanical ventilation time, and hospitalization time of the stu group were significantly shorter than those of the con group. There is also one study indicating that for ICU patients, rapid examination and relatively short mechanical ventilation time and ventilation time in hospital are all related to the improvement of prognosis [18]. These results imply that compared with conventional invasive mechanical ven-tilation, sequential ventilation can shorten treatment time, relieve the patient’s disease more effectively and quickly, and improve their prognosis. In this study, complications of the two groups were detected. It came out that the complication rate of the stu group was significantly lower than that of the con group (17.65% vs. 30.21%), and complications in the stu group were more self-relieving symptoms such as dry nose and mouth and facial pain. One study has concluded that VAP is a main complication of mechanical ventilation [19]. In this study, the incidence of VAP in the stu group was significantly lower than that in the con group, and the weaning failure and reintubation rates of the stu group were also significantly lower than those of the con group. Therefore, it can be inferred that compared with conventional invasive mechanical ventilation, sequential ventilation is more effective in reducing the incidences of complications and adverse events in the treatment of PAH complicated with RF, indicating that sequential ventilation causes less stimulation to patients with PAH complicated with RF and contributes to faster recovery of them. We compared the blood gas analysis indexes between the two groups, and found that after treatment, pH and PaO2 of the stu group were significantly higher than those of the con group, and PaCO2 of the stu group was significantly lower than that of the con group. One study has pointed out that arterial blood gas analysis is an crucial examination method for emergency patients and a means to evaluate human respiratory function and acid-base balance, which can directly reflect lung ventilation function and acid-base balance [20,21]. Thus, it can be inferred that sequential ventilation is more effective in improving patients’ respiratory function and homoiostasis in the treatment of PAH complicated with RF. As a crucial part in cardiovascular endocrinology, BNP plays a pivotal role in regulating human blood pressure, body fluid balance, and cardiovascular function [22]. It is mainly synthesized and secreted by right ventricular myocyte, and ventricular wall tension and pressure load can stimulate the synthesis and secretion of it [23]. In addition, BNP can be synthesized and secreted instantaneously [24]. Therefore, we adopted pulmonary artery pressure and BNP to judge the efficacy of different mechanical ventilation therapies in treating PAH complicated with RF. In the study, before treatment, there was no notable difference in BNP and pulmonary artery pressure between the two groups, while after treatment, the two indexes of both groups decreased significantly, indicating that both mechanical ventilation therapies can effectively treat patients with PAH complicated with RF. In addition, the decrease of BNP and pulmonary artery pressure in the stu group was more notable than that in the con group after treatment, implying that sequential ventilation can effectively treat patients with the diseases. Moreover, in our study, there was no notable difference between the two groups in ET and Ang II before treatment, while the two indexes in both groups decreased significantly after treatment. Some studies have pointed out that the increase of ET and Ang II can give rise to pulmonary artery vasoconstriction, and thereby lead to continuous increase of pulmonary artery pressure [25,26]. It can be concluded that both mechanical ventilation therapies can effectively improve ET and Ang II in patients with PAH complicated with RF. The decrease of ET and Ang II in the stu group was more significant than that in the con group, suggesting that sequential ventilation can effectively patients with PAH complicated with RF.
This study mainly determined the changes of blood gas analysis indexes, BNP, and pulmonary artery pressure of patients treated with sequential ventilation and those treated with conventional invasive mechanical ventilation to explore the efficacy of the two ventilation therapies in the treatment of PAH complicated with RF, so as to provide a theoretical basis for clinical treatment of PAH complicated with RF. However, this study has some limitations, because it has not continued to follow up patients. In the future study, the research content will be continuously improved to provide a more scientific reference for clinical treatment, so as to further improve the prognosis of patients.
To sum up, compared with conventional invasive mechanical ventilation, sequential ventilation can effectively shorten the treatment time of patients with PAH complicated with RF, reduce the incidences of adverse events and complications in them, and significantly improve their blood gas analysis indexes and BNP, so it is worthy of clinical promotion.
Disclosure of conflict of interest
None.
References
- 1.Liyan C, Min P, Nan L, Hua W, Chunli L, Nuofu Z, Wang J. Pulmonary arterial hypertension as the initial pulmonary manifestation in a patient with primary antiphospholipid antibody syndrome: a case report. Int J Clin Exp Med. 2019;12:1122–1126. [Google Scholar]
- 2.Palazzini M, Dardi F, Manes A, Bacchi Reggiani ML, Gotti E, Rinaldi A, Albini A, Monti E, Galie N. Pulmonary hypertension due to left heart disease: analysis of survival according to the haemodynamic classification of the 2015 ESC/ERS guidelines and insights for future changes. Eur J Heart Fail. 2018;20:248–255. doi: 10.1002/ejhf.860. [DOI] [PubMed] [Google Scholar]
- 3.Lin KY, Chen H, Yu L. Pulmonary arterial hypertension caused by congenital extrahepatic portocaval shunt: a case report. BMC Cardiovasc Disord. 2019;19:141. doi: 10.1186/s12872-019-1124-1. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Liu HD, Xiong W, Liu F, Lin F, He JB, Liu C, Lin YW, Dong SH. Significant role and mechanism of microRNA-143-3p/KLLN axis in the development of coronary heart disease. Am J Transl Res. 2019;11:3610–3619. [PMC free article] [PubMed] [Google Scholar]
- 5.Arvanitaki A, Boutsikou M, Anthi A, Apostolopoulou S, Avgeropoulou A, Demerouti E, Farmakis D, Feloukidis C, Giannakoulas G, Karvounis H, Karyofyllis P, Mitrouska I, Mouratoglou S, Naka KK, Orfanos SE, Panagiotidou E, Pitsiou G, Rammos S, Stagaki E, Stanopoulos I, Thomaidi A, Triantafyllidi H, Tsangaris I, Tsiapras D, Voudris V, Manginas A Hellenic Society for the Study of Pulmonary Hypertension (HSSPH) Epidemiology and initial management of pulmonary arterial hypertension: real-world data from the Hellenic pulmOnary hyPertension rEgistry (HOPE) Pulm Circ. 2019;9:2045894019877157. doi: 10.1177/2045894019877157. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Antigny F, Mercier O, Humbert M, Sabourin J. Excitation-contraction coupling and relaxation alteration in right ventricular remodelling caused by pulmonary arterial hypertension. Arch Cardiovasc Dis. 2020;113:70–84. doi: 10.1016/j.acvd.2019.10.009. [DOI] [PubMed] [Google Scholar]
- 7.Liu M, Yuan Q, Zhao H, Wang Y. Williams-campbell syndrome complicated with pulmonary hypertension and Type 2 respiratory failure: an adult case report. Clin Respir J. 2019;13:795–799. doi: 10.1111/crj.13090. [DOI] [PubMed] [Google Scholar]
- 8.Stewart DL, Vogel PA, Jarrett B, Potenziano J. Effect of inhaled nitric oxide on oxygen therapy, mechanical ventilation, and hypoxic respiratory failure. Minerva Pediatr. 2018;70:51–58. doi: 10.23736/S0026-4946.17.04944-1. [DOI] [PubMed] [Google Scholar]
- 9.Yao SS, Yang F, Zheng ZG, Cao YF, Zhong M, Zeng QX, Dong H, Liu N, Hu JY, Chen RC. The effect of a breathing trainer on relieving airway pressure caused by active cough in patients with mechanical ventilation. Zhonghua Jie He He Hu Xi Za Zhi. 2020;43:136–139. doi: 10.3760/cma.j.issn.1001-0939.2020.02.012. [DOI] [PubMed] [Google Scholar]
- 10.Windisch W, Dreher M, Geiseler J, Siemon K, Brambring J, Dellweg D, Grolle B, Hirschfeld S, Köhnlein T, Mellies U, Rosseau S, Schönhofer B, Schucher B, Schütz A, Sitter H, Stieglitz S, Storre J, Winterholler M, Young P, Walterspacher S für die Leitliniengruppe, Nichtinvasive und invasive Beatmung als Therapie der chronischen respiratorischen Insuffizienz. Guidelines for non-invasive and invasive home mechanical ventilation for treatment of chronic respiratory failure - update 2017. Pneumologie. 2017;71:722–795. doi: 10.1055/s-0043-118040. [DOI] [PubMed] [Google Scholar]
- 11.Lv Y, Lv Q, Lv Q, Lai T. Pulmonary infection control window as a switching point for sequential ventilation in the treatment of COPD patients: a meta-analysis. Int J Chron Obstruct Pulmon Dis. 2017;12:1255–1267. doi: 10.2147/COPD.S126736. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Simonneau G, Montani D, Celermajer DS, Denton CP, Gatzoulis MA, Krowka M, Williams PG, Souza R. Haemodynamic definitions and updated clinical classification of pulmonary hypertension. Eur Respir J. 2019;53:1801913. doi: 10.1183/13993003.01913-2018. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13.Bonnet S, Provencher S, Guignabert C, Perros F, Boucherat O, Schermuly RT, Hassoun PM, Rabinovitch M, Nicolls MR, Humbert M. Translating research into improved patient care in pulmonary arterial hypertension. Am J Respir Crit Care Med. 2017;195:583–595. doi: 10.1164/rccm.201607-1515PP. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Hester J, Ventetuolo C, Lahm T. Sex, gender, and sex hormones in pulmonary hypertension and right ventricular failure. Compr Physiol. 2019;10:125–170. doi: 10.1002/cphy.c190011. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Alencar AKN, Montes GC, Costa DG, Mendes LVP, Silva AMS, Martinez ST, Trachez MM, Cunha VDMN, Montagnoli TL, Fraga AGM, Wang H, Groban L, Fraga CAM, Sudo RT, Zapata-Sudo G. Cardioprotection Induced by activation of GPER in ovariectomized rats with pulmonary hypertension. J Gerontol A Biol Sci Med Sci. 2018;73:1158–1166. doi: 10.1093/gerona/gly068. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Bergot E, De Leotoing L, Bendjenana H, Tournier C, Vainchtock A, Nachbaur G, Humbert M. Hospital burden of pulmonary arterial hypertension in France. PLoS One. 2019;14:e0221211. doi: 10.1371/journal.pone.0221211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Piroddi IM, Barlascini C, Nicolini A. Severe respiratory failure due to interferon beta-related pulmonary hypertension. Am J Ther. 2016;23:e1275–1276. doi: 10.1097/MJT.0000000000000348. [DOI] [PubMed] [Google Scholar]
- 18.Durie ML, Darvall JN, Hadley DA, Tacey MA. A “Code ICU” expedited review of critically ill patients is associated with reduced emergency department length of stay and duration of mechanical ventilation. J Crit Care. 2017;42:123–128. doi: 10.1016/j.jcrc.2017.07.011. [DOI] [PubMed] [Google Scholar]
- 19.Vijay G, Mandal A, Sankar J, Kapil A, Lodha R, Kabra SK. Ventilator associated pneumonia in pediatric intensive care unit: incidence, risk factors and etiological agents. Indian J Pediatr. 2018;85:861–866. doi: 10.1007/s12098-018-2662-8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Wong EKC, Lee PCS, Ansary S, Asha S, Wong KKH, Yee BJ, Ng AT. Role of venous blood gases in hypercapnic respiratory failure chronic obstructive pulmonary disease patients presenting to the emergency department. Intern Med J. 2019;49:834–837. doi: 10.1111/imj.14186. [DOI] [PubMed] [Google Scholar]
- 21.Wu J, Pan M, Ouyang H, Yang Z, Zhang Q, Cai Y. Establishing and evaluating autoverification rules with intelligent guidelines for arterial blood gas analysis in a clinical laboratory. SLAS Technol. 2018;23:631–640. doi: 10.1177/2472630318775311. [DOI] [PubMed] [Google Scholar]
- 22.Meng P, Nguyen LS, Jabbour F, Ogna A, Clair B, Orlikowski D, Annane D, Lofaso F, Fayssoil A. Accuracy of B-natriuretic peptide for the diagnosis of decompensated heart failure in muscular dystrophies patients with chronic respiratory failure. Neurol Int. 2018;10:7917. doi: 10.4081/ni.2018.7917. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23.Young DJ, McCall PJ, Kirk A, Macfie A, Kinsella J, Shelley BG. B-type natriuretic peptide predicts deterioration in functional capacity following lung resection. Interact Cardiovasc Thorac Surg. 2019;28:945–952. doi: 10.1093/icvts/ivz016. [DOI] [PubMed] [Google Scholar]
- 24.Adrish M, Nannaka VB, Cano EJ, Bajantri B, Diaz-Fuentes G. Significance of NT-pro-BNP in acute exacerbation of COPD patients without underlying left ventricular dysfunction. Int J Chron Obstruct Pulmon Dis. 2017;12:1183–1189. doi: 10.2147/COPD.S134953. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 25.Becirovic-Agic M, Jonsson S, Tveitaras MK, Skogstrand T, Karlsen TV, Liden A, Leh S, Ericsson M, Nilsson SK, Reed RK, Hultstrom M. Time course of decompensation after angiotensin II and high-salt diet in Balb/CJ mice suggests pulmonary hypertension-induced cardiorenal syndrome. Am J Physiol Regul Integr Comp Physiol. 2019;316:R563–R570. doi: 10.1152/ajpregu.00373.2018. [DOI] [PubMed] [Google Scholar]
- 26.Li X, Qiu J, Pan M, Zheng D, Su Y, Wei M, Kong X, Sun W, Zhu J. Correlation between congenital heart disease complicated with pulmonary artery hypertension and circulating endothelial cells as well as endothelin-1. Int J Clin Exp Pathol. 2015;8:10743–10751. [PMC free article] [PubMed] [Google Scholar]