

This study examines the impact that social distancing measures introduced to combat coronavirus disease 2019 (COVID‐19) have had on the orthopaedic trauma load at a level 1 trauma hospital in Sydney.
Keywords: COVID‐19, hospital presentations, orthopaedic surgery, social distancing, trauma
Abstract
Background
The coronavirus disease 2019 (COVID‐19) pandemic has affected communities worldwide. This study examines the impact that public health measures to control viral spread have had on orthopaedic trauma presenting to an Australian level 1 trauma centre. We hypothesized that the volume of orthopaedic trauma in the period of social distancing would decrease, and the mechanisms of injury differ, compared to pre‐pandemic times.
Methods
We performed a retrospective analysis of patients requiring emergency orthopaedic surgery between 16 March and 21 April 2020 (the period after social distancing and lockdown commenced), and compared it to the group of patients from the same period in 2019. We collected demographic data, as well as injury type, anatomical location, mechanism of injury and surgical logistics.
Results
During the COVID‐19 period, total emergency operations performed decreased by 15.6% compared to the same period in 2019. Orthopaedic admissions decreased by 30.8%. Demographics of the groups were unchanged. Anaesthetic time decreased, but total time spent in the operating theatre was unchanged. Road trauma comprised a similar proportion of cases overall; however, cycling‐related accidents increased significantly, making up 11% of presentations during COVID‐19. Sporting injuries, work‐related injuries and multi‐traumas reduced during the pandemic.
Conclusion
The impact of COVID‐19‐related lockdown measures and social distancing on orthopaedic trauma in Australia has been an overall decrease in volume of cases, combined with significant changes in the mechanisms of injury necessitating surgery.
Introduction
Coronavirus disease 2019 (COVID‐19) has had profound impacts worldwide. Shortly after the World Health Organization declared a pandemic on 11 March 2020, 1 Australia implemented public health infection control measures by restricting travel, public gatherings, sport and workplace attendance. 2 , 3 , 4 , 5 In turn, the Australian healthcare system responded by postponing elective surgery, expanding telehealth services, establishing dedicated testing facilities to limit exposure to healthcare workers and preserving hospital resources including personal protective equipment (PPE). 6 However, besides decreasing the rate of viral transmission, social distancing has had other consequences.
During the initial wave, New South Wales had the highest number of diagnosed cases in Australia, with the majority of those within metropolitan Sydney. Within Sydney, Northern Sydney Local Health District has faced the second greatest burden (522 confirmed cases). 7 Royal North Shore Hospital (RNSH) is the largest hospital in this network, and is a tertiary referral trauma centre covering both metropolitan and rural areas. Emergency surgery has continued throughout the pandemic, with new perioperative protocols in place, including negative pressure operating theatres (with anterooms), additional PPE, anaesthetic protocols for aerosolizing procedures and recovery within the theatre itself.
The aim of this study is to examine the impact of social distancing measures and local COVID‐19 protocols on orthopaedic trauma surgery at RNSH, by comparing patient cohorts from the affected period and the same period 1 year prior. We postulated that the incidence and mechanism of orthopaedic trauma would be altered due to social distancing measures, with similar changes to surgical and anaesthetic durations secondary to amended local protocols.
Methods
This study was conducted retrospectively. Following ethics approval, an analysis of all patients requiring emergency orthopaedic surgery over a 5‐week period after commencement of social restrictions (16 March to 21 April 2020) was conducted via the PowerChart electronic medical record system (Cerner, North Kansas City, MO, USA). All patients with general orthopaedic injuries necessitating surgery were included. Patients who underwent operative management of isolated spinal or hand injuries were excluded, as these are considered separate sub‐specialties at RNSH. Patients who had orthopaedic injuries combined with spinal or hand trauma were included.
Outcomes assessed included basic demographic and injury information, as well as surgical data (time between injury and intervention, total anaesthetic and surgical times, and personnel involved in the procedure). These were compared to the cohort of patients requiring emergency orthopaedic surgery for the same time period in 2019. Standard protocols regarding the ethical use of patient data were applied. Datapoints were summarized as means with standard deviations where appropriate, or as a percentage of proportions in the case of dichotomous variables. Comparisons were made using the Student's two‐tailed, unpaired t‐test for continuous variables and using chi‐squared tests for dichotomous variables (with Fisher's exact test where the incidence of a particular event was less than 5). Alpha was set at 0.05 for all data points.
Results
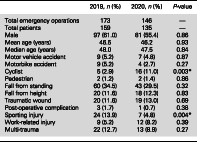
During the 5‐week period in 2020, 146 emergency orthopaedic operations were performed on 135 patients. This was a 15.6% decrease from the 2019 cohort, where 173 procedures were performed on 159 patients. Total orthopaedic admissions (elective and emergency) in this period were 173, diminished by 30.8% from 250 in 2019. There was no significant difference in age or gender between the two groups (Table 1).
Table 1.
Patient and injury demographics
| 2019, n (%) | 2020, n (%) | P‐value | |
|---|---|---|---|
| Total emergency operations | 173 | 146 | — |
| Total patients | 159 | 135 | — |
| Male | 97 (61.0) | 81 (55.4) | 0.86 |
| Mean age (years) | 46.5 | 46.2 | 0.93 |
| Median age (years) | 48.0 | 47.5 | 0.84 |
| Motor vehicle accident | 9 (5.2) | 7 (4.8) | 0.87 |
| Motorbike accident | 9 (5.2) | 4 (2.7) | 0.27 |
| Cyclist | 5 (2.9) | 16 (11.0) | 0.003 |
| Pedestrian | 2 (1.2) | 2 (1.4) | 0.86 |
| Fall from standing | 60 (34.5) | 43 (29.5) | 0.32 |
| Fall from height | 20 (11.6) | 18 (12.3) | 0.83 |
| Traumatic wound | 20 (11.6) | 19 (13.0) | 0.69 |
| Post‐operative complication | 3 (1.7) | 1 (0.7) | 0.38 |
| Sporting injury | 24 (13.9) | 7 (4.8) | 0.004 |
| Work‐related injury | 9 (5.2) | 12 (8.2) | 0.39 |
| Multi‐trauma | 22 (12.7) | 13 (8.9) | 0.27 |
There was no significant difference in the proportion of patients whose injuries were sustained by road trauma (which included car, motorbike, cycling and pedestrian accidents), nor was there a difference in the number of patients presenting with a work‐related injury. Road trauma was responsible for 25 presentations (14.5%) in 2019, and 29 patients (16.8%) in 2020 (P = 0.2). However, the proportion of the road trauma patients who were cyclists significantly increased. Cyclists comprised 16 patients (11.0%) in 2020, compared to just five patients (2.9%) in 2019 (P = 0.003). There was a significant decrease in the proportion of patients who injured themselves playing sports (organized or social sports, excluding cycling), down to seven cases in 2020, compared to 24 cases in 2019 (P = 0.004) (Table 1). There was a decrease in multi‐trauma patients (defined as patients presenting with more than one discrete anatomical location of injury) to 13 in 2020, compared to 22 previously; however, this was not significant (P = 0.27). There was no difference in the proportion of patients who presented with geriatric hip fractures during the studied period; similarly, proportions of patients with upper limb or lower limb injuries were unchanged.
There was no significant difference in the types of operations performed (Table 2), nor was there a change in the proportion of cases done out of hours (between 17.00 and 08.00 hours). The mean number of surgical team members involved in the operations was 2.26 and 2.28 in 2019 and 2020, respectively, demonstrating no difference in surgical staffing. However, the percentage of cases that were consultant‐led (consultant listed as primary surgeon) significantly increased from 110 of 173 cases (63.6%) in 2019 to 112 of 146 cases (76.7%) in 2020 (P = 0.01). There was a decrease in the mean anaesthetic time (time from commencement of anaesthesia to commencement of surgery) from 44.5 min in 2019 to 39.0 min during COVID (P = 0.02), but there was no significant difference in the total time the patient spent in the operating room (Table 3).
Table 2.
Operations performed
| Operation performed (%) | 2019, n (%) | 2020, n (%) | P‐value |
|---|---|---|---|
| Closed reduction | 26 (15.0) | 28 (19.1) | 0.33 |
| Internal fixation | 55 (31.2) | 40 (27.4) | 0.39 |
| Intramedullary nail | 17 (9.8) | 16 (11.0) | 0.74 |
| External fixation | 0 | 3 (2.1) | 0.08 |
| Arthroplasty | 13 (7.5) | 11 (7.5) | 0.99 |
| Debride infection | 20 (11.6) | 20 (13.7) | 0.57 |
| Debride traumatic wound | 24 (13.9) | 22 (15.1) | 0.76 |
Table 3.
Surgical logistics
| 2019 | 2020 | P‐value | |
|---|---|---|---|
| Consultant primary surgeon, n (%) | 110 (63.6%) | 112 (76.7%) | 0.01 |
| Cases done out of hours † , n (%) | 55 (31.8) | 54 (37.0) | 0.33 |
| Average number of surgical team scrubbed | 2.26 | 2.28 | 0.79 |
| Average anaesthetic time (min) | 44.5 | 39.0 | 0.02 |
| Average surgical time (min) | 66.6 | 56.1 | 0.06 |
| Average total time in room (min) | 98.7 | 87.2 | 0.07 |
| Average time from triage to theatre (min) | 2383.3 | 2525.0 | 0.83 |
Saturday, Sunday or case commencing after 17.00 hours weekdays.
Discussion
COVID‐19, the disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS‐CoV‐2), has challenged healthcare systems globally. 1 With no proven therapeutic agent, many governments have focused instead on limiting the spread of the virus via broad public health measures, with varying degrees of social ‘lockdown’. 2 Australia's response to COVID‐19 commenced on 23 January 2020, with the first case in Australia recorded on 25 January, 8 and the first death on 1 March. 9 Following the declaration of a global pandemic by the World Health Organization on 11 March, 1 a progressive shutdown of social and economic activity throughout the country over the subsequent 2 weeks was commenced. 10 International travel was banned, and overseas travellers returning to Australia were required to quarantine. 3 Australians were urged to stay home, leaving home only for exercise, food, essential work and study, or to act as a carer.
The response of the Australian healthcare system had several goals: to prepare hospitals for high numbers of COVID‐19 patients; manage the workforce, assuming large groups of staff may be required to quarantine; and maintain safe delivery of essential care, including conservation of PPE. 10 Non‐essential elective surgery in both public and private hospitals was postponed indefinitely on 25 March. 6 Telehealth clinics were established, and patients were encouraged to defer non‐essential appointments. During the first wave of COVID‐19 in Australia, the number of new daily cases reported peaked at 469 on 28 March before slowly decreasing. 11 Although the aforementioned disease‐control measures have had significant societal and economic costs, their implementation has circumvented the overwhelming of the healthcare system.
At our tertiary referral institution, local protocols regarding PPE allocation and staffing were developed to safely continue emergency and essential elective surgery. ‘Pandemic medicine’ treatment protocols for orthopaedic patients were not utilized. All fractures were treated on their merit, with the ability to do so due to maintained capacity in both the hospital and healthcare district (despite treating the second highest number of COVID‐19 patients in New South Wales). 7 This is in contrast to the National Health Service (UK), which was in a very different position regarding the available healthcare resources and the burden of COVID‐19 patients. In April, the National Health Service clinical guide for trauma and orthopaedic patients advocated for non‐operative management to be explored as the primary option, performing surgery as day‐only cases wherever possible, and limiting outpatient attendance. 12 A tertiary centre in London that did not alter its threshold for surgery based on this recommendation noted a decrease in surgical cases of one‐third compared to pre‐pandemic, suggesting that the primary driver of decreased procedures was decreased referral volume, rather than local protocol. 13 Similar decreases in trauma referrals have been recognized in centres in the USA, 14 Spain 15 and India. 16
Physical distancing requirements and mandatory shutdown of businesses, workplaces and gatherings have transformed daily activities. The Citimapper Mobility Index estimates the movement of people within Sydney decreased by up to 84% in March, as fewer people utilized public transport or drove to their places of work. 17 On the basis of these changes, it was hypothesized there would be a decrease in the total number of orthopaedic trauma patients presenting to emergency, and indeed, this was the case in our study. Similarly, we anticipated a drop in patients with work‐related injuries (given a large proportion of workers are now working from home, or unemployed) and sporting‐related injuries (given the cancellation of organized sport and group activities), but a rise in trauma related to home ‘do‐it‐yourself’ projects. Our findings were as expected for sporting and ‘do‐it‐yourself’ injuries; however, work‐related injuries remained largely unchanged. This is possibly because the majority of these injuries occurred on construction sites, with most construction continuing throughout the studied period. The number of geriatric hip fracture presentations was also predicted to decrease, given that this population is at higher risk of COVID‐19, and would be more likely to adhere to social distancing recommendations by remaining indoors, potentially reducing the risk of falls. However, the proportion of geriatric hip fractures remained unchanged when comparing the two time periods, consistent with prior evidence that the majority of hip fractures occur after a fall at home or indoors, 18 and is similar to international reports during this pandemic. A tertiary centre in Barcelona, Spain, found that the volume of hip fractures remained stable despite a decrease in overall trauma presentations. All patients were tested for COVID‐19 on presentation given high levels of community spread – the prevalence in this population was 19.4%, leading to surgical delays and higher in‐hospital mortality. 15 By contrast, our 30‐day hip fracture mortality rate was not affected during this period (4%, compared with the 2019 national average of 5%). 19 Because of the low prevalence of COVID‐19 in our population, patients were only tested if symptomatic, and there were few delays to surgery.
Although the volume of road trauma patients was unchanged, the distribution altered significantly, with a small decrease in car‐related injuries, a substantial decrease in motorbike accidents and a large increase in trauma from cycling. The proportion of pedestrians was roughly the same between years. This is consistent with data from the Bureau of Infrastructure, Transport and Regional Economics, which, although analysing deaths rather than injury, reflects a similar change in how roads are being utilized during COVID‐19. In Australia, road deaths during April 2020 totalled 75, down 25.3% compared with the monthly average in the previous 5 years (100.5 deaths). Motorcyclist deaths were down 8.8%. There was, however, an increase in cycling‐related deaths of 21.6% (to 45 cyclists) compared to April 2019 (37 cyclists), despite fewer vehicles being on the road. 20
The decrease in trauma patients from road accidents is easily explained given the restrictions placed on travel. The increased proportion of cycling‐related trauma in this group is multifactorial. During April 2020, Sydney City Council reported increased cycle traffic of 25–50%, despite the drop in people movement. 21 Bicycle sales also increased by up to 28% as people took up cycling during the pandemic as a hobby following the closure of gyms, 22 and rising demand for home food delivery led to more cyclists working for food delivery companies. 23 These cyclists may have been inexperienced and therefore more likely to be involved in an accident. 24 As restrictions ease and people eventually return to work, it is expected there will be an increase in commuting and transit via bicycle as people practice social distancing and avoid public transport. For the same reason, more cars will return to the roads, and it is likely cyclists will continue to be vulnerable to trauma in the post‐lockdown period.
Whilst the number of surgical team members scrubbed during trauma operations was unchanged during the studied period, the proportion of cases that were consultant‐led significantly increased. This was not driven by hospital or department policy. At RNSH, there is a high level of consultant involvement at baseline, and there was no observable changes in definitive management or unplanned return to theatres during the studied period. Contrary to our hypothesis, anaesthetic time actually decreased by an average of 5 min per patient. There was a change in the anaesthetic department's protocols for routine anaesthesia, given that aerosolizing procedures carry a high risk of COVID‐19 transmission. As such, there was an increase in consultant‐driven anaesthesia, and a change in practice to allow early extubation in theatre, rather than in recovery. Despite the change in protocols, the total length of time patients spent inside the theatre was unaffected.
Australian states and territories slowly eased social restrictions from 1 May 2020, which included the recommencement of elective surgery in a restricted capacity and a gradual return to full surgical capacity planned over several weeks to months. 25 RACS estimates that the backlog of elective operations in Australia due to COVID‐19 is nearly 400 000 cases, 26 a burden that will take many months to clear, potentially decreasing many patients' quality of life during this time. This is just one of the many challenges that the healthcare systems are facing globally during the recovery period.
While there are several studies examining the impact of COVID‐19 on elective surgery, few studies analyse its effect on orthopaedic trauma, particularly in Australia. Despite social distancing and travel restrictions, there has been a persistent (although decreased) demand for emergency orthopaedic care throughout the pandemic. This study aids in understanding how human movement and social activities contribute to orthopaedic trauma, both for future resource allocation and for trauma prevention. Future research should further appraise changes in trauma demographics, both domestic and international, as well as whether the trends observed will reverse as the pandemic eases.
Author Contributions
Annabel Probert: Conceptualization; data curation; investigation; project administration; writing‐original draft; writing‐review and editing. Brahman Sivakumar: Conceptualization; formal analysis; methodology; project administration; supervision; writing‐review and editing. Vincent An: Data curation; formal analysis. Sarah Nicholls: Data curation; investigation. Jobe Shatrov: Conceptualization; methodology; project administration; resources; supervision. Michael Symes: Conceptualization; data curation; methodology; project administration; supervision; validation; writing‐review and editing. Andrew Ellis: Conceptualization; project administration; supervision; writing‐review and editing.
Conflicts of interest
None declared.
A. C. Probert MBBS; B. S. Sivakumar MBBS, FRACS; V. An MD, MPhil; S. L. Nicholls MBBS; J. G. Shatrov MBBS, FRACS; M. J. Symes MBBS, FRACS; A. M. Ellis MBBS, FRACS.
References
- 1. World Health Organization . Virtual press conference on COVID‐19 11 March 2020. 2020. [Cited 29 July 2020]. Available from URL: https://www.who.int/docs/default‐source/coronaviruse/transcripts/who‐audio‐emergencies‐coronavirus‐press‐conference‐full‐and‐final‐11mar2020.pdf?sfvrsn=cb432bb3_2
- 2. Anderson RM, Heesterbeek H, Klinkenberg D, Hollingsworth TD. How will country‐based mitigation measures influence the course of the COVID‐19 epidemic? Lancet 2020; 395: 931–4. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3. Burke K. Australia closes borders to stop coronavirus. 7 News. 2020. [Cited 29 July 2020.] Available from URL: https://7news.com.au/lifestyle/health‐wellbeing/australia‐closes‐borders‐to‐stop‐coronavirus‐c‐752927
- 4. Knaus C. PM announces pubs, clubs and cinemas to close, schools stay open in stage one measures – as it happened. The Guardian Australia. 2020. [Cited 23 July 2020.] Available from URL: https://www.theguardian.com/world/live/2020/mar/22/coronavirus‐updates‐live‐australia‐nsw‐victoria‐qld‐tasmania‐cases‐government‐stimulus‐latest‐update‐news
- 5. Business.gov.au Commonwealth of Australia . Restrictions on services. 2020. [Cited 23 July 2020.] Available from URL: https://www.business.gov.au/risk‐management/emergency‐management/coronavirus‐information‐and‐support‐for‐business/restrictions‐on‐non‐essential‐services
- 6. McCauley D. Morrison launches COVID‐19 Coordination Commission, cancels non‐urgent surgery. The Sydney Morning Herald. 2020. [Cited 23 July 2020.] Available from URL: https://www.smh.com.au/politics/federal/morrison‐launches‐covid‐19‐coordination‐commission‐cancels‐non‐urgent‐surgery‐20200325‐p54dpx.html
- 7. NSW Health . COVID‐19 weekly surveillance in NSW. 2020. [Cited 23 May 2020.] Available from URL: https://www.health.nsw.gov.au/Infectious/covid‐19/Documents/covid‐19‐surveillance‐report‐20200422.pdf
- 8. Daoud E. Monash Medical Centre treating first Australian case of coronavirus. 7 News. 2020. [Cited 28 July 2020.] Available from URL: https://7news.com.au/news/health/first‐australian‐coronavirus‐case‐confirmed‐in‐victoria‐c‐664530
- 9. Daoud E. Western Australian man becomes first person in Australia to die from coronavirus. 7 News. 2020. [Cited 28 July 2020.] Available from URL: https://7news.com.au/travel/coronavirus/western‐australian‐man‐becomes‐first‐person‐in‐australia‐to‐die‐from‐coronavirus‐c‐723547
- 10. Department of Health, Commonwealth of Australia . Government response to the COVID‐19 outbreak. 2020. [Cited 28 July 2020.] Available from URL: https://www.health.gov.au/news/health‐alerts/novel‐coronavirus‐2019‐ncov‐health‐alert/government‐response‐to‐the‐covid‐19‐outbreak
- 11. Department of Health, Commonwealth of Australia . Coronavirus (COVID‐19) current situation and case numbers. 2020. [Cited 28 July 2020.] Available from URL: https://www.health.gov.au/news/health‐alerts/novel‐coronavirus‐2019‐ncov‐health‐alert/coronavirus‐covid‐19‐current‐situation‐and‐case‐numbers
- 12. NHS England . Clinical guide for the management of trauma and orthopaedic patients during the coronavirus pandemic version 2. 2020. [Cited 23 July 2020.] Available from URL: https://www.england.nhs.uk/coronavirus/wp‐content/uploads/sites/52/2020/03/C0274‐Specialty‐guide‐Orthopaedic‐trauma‐v2‐14‐April.pdf
- 13. Park C, Sugand K, Nathwani D, Bhattacharya R, Sarraf KM. Impact of the COVID‐19 pandemic on orthopedic trauma workload in a London level 1 trauma center: the “golden month”. Acta Orthop. 2020; 91: 1–6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14. Bram JT, Johnson MA, Magee LC et al. Where have all the fractures gone? The epidemiology of pediatric fractures during the COVID‐19 pandemic. J. Pediatr. Orthop. 2020; 40: 373–9. [DOI] [PubMed] [Google Scholar]
- 15. Nunez JH, Sallent A, Lakhani K et al. Impact of the COVID‐19 pandemic on emergency traumatology service: experience at a tertiary trauma centre in Spain. Injury 2020; 51: 1414–8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16. Maryada VR, Mulpur P, Guravareddy AV, Pedamallu SK, Vijay Bhasker B. Impact of COVID‐19 pandemic on orthopaedic trauma volumes: a multi‐Centre perspective from the state of Telangana. Indian J. Orthop. 2020: 1–6. Published online 13 August 2020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Citimapper Limited UK . Citimapper mobility index. 2020. [Cited 23 May 2020.] Available from URL: https://citymapper.com/cmi
- 18. Aharonoff GB, Dennis MG, Elshinawy A, Zuckerman JD, Koval KJ. Circumstances of falls causing hip fractures in the elderly. Clin. Orthop. Relat. Res. 1998; 348: 10–4. [PubMed] [Google Scholar]
- 19. Australian & New Zealand Hip Fracture Registry . ANZHFR Annual Report 2019. 2019. [Cited 16 Sept 2020.] Available from URL: https://anzhfr.org/reports
- 20. Bureau of Infrastructure, Transport and Regional Economics. Commonwealth of Australia . Road Fatalities Australia Monthly Bulletin. 2020. [Cited 23 May 2020.] Available from URL: https://www.bitre.gov.au/sites/default/files/documents/rda_apr_2020.pdf
- 21. City of Sydney News . Cycling bucks the trend as a safer way to travel. 2020. [Cited 23 May 2020.] Available from URL: https://news.cityofsydney.nsw.gov.au/articles/sydney‐cycling‐bucks‐the‐trend‐as‐a‐safer‐way‐to‐travel
- 22. Clarke B. Australians join global coronavirus cycling boom as bikes become key social distancing tool. SBS News. 2020. [Cited 23 May 2020.] Available from URL: https://www.sbs.com.au/news/australians‐join‐global‐coronavirus‐cycling‐boom‐as‐bikes‐become‐key‐social‐distancing‐tool
- 23. Wade M. Boom time: the council areas with the biggest surge in food delivery. The Sydney Morning Herald. 2020. [Cited 23 May 2020.] Available from URL: https://www.smh.com.au/business/the‐economy/boom‐time‐the‐council‐areas‐with‐the‐biggest‐surge‐in‐food‐delivery‐20200429‐p54o8g.html
- 24. Keoghan S. Surge in Sydney food couriers raises safety concerns. The Sydney Morning Herald. 2020. [Cited 23 May 2020.] Available from URL: https://www.smh.com.au/national/nsw/they‐cross‐in‐front‐of‐the‐car‐surge‐in‐sydney‐food‐couriers‐raises‐safety‐concerns‐20200415‐p54jza.html
- 25. Department of Health, Commonwealth of Australia . Elective surgery restrictions eased. 2020. [Cited 28 July 2020.] Available from URL: https://www.health.gov.au/ministers/the‐hon‐greg‐hunt‐mp/media/elective‐surgery‐restrictions‐eased
- 26. Royal Australasian College of Surgeons . COVID‐19 disruption will lead to 28 million surgeries being cancelled worldwide. 2020. [Cited 23 May 2020.] Available from URL: https://www.surgeons.org/news/media‐releases/covid‐19‐disruption‐will‐lead‐to‐28‐million‐surgeries‐being‐cancelled‐worldwide