

Abstract
This study aimed to clarify whether low-load resistance training at a low frequency (twice a week) using body weight and elastic band improves muscle size, muscle strength, and physical functions and to compare the training effects between supervised training and a combination of supervised and unsupervised training in untrained older adults. Fifty-one older adults (ages: 57-75 years) selected to either a supervised (S) training group (n = 34) or a combined supervised and unsupervised (SU) group (n = 17). Both groups performed low-load resistance training composed of nine exercises for 12 weeks. The S group participated in supervised exercise sessions twice a week, and the SU group performed a supervised exercise session once a week and an unsupervised exercise session at home also once a week. For muscle thicknesses in the anterior aspects of the forearm, upper arm, and thigh and the posterior aspect of the thigh, group × time interactions were observed (p < 0.05). The hypertrophic effects were higher in the S group. Isometric knee extension strength and physical functions increased similarly in both groups. Low-load resistance training using body weight and elastic band twice a week for 12 weeks induces muscle hypertrophy and increases muscle strength and physical functions in older adults. Although the muscle hypertrophic effects are greater in the S group than in the SU group, the other effects were similar between the groups.
Key points.
Low-load resistance training using body weight and elastic bands even for only twice a week could induce muscle hypertrophy and increase muscle strength and physical functions in older adults after 12 weeks of training.
The muscle hypertrophic effects are greater in the supervised training group than in the combined supervised and unsupervised group.
The magnitude of increase in muscle strength and physical functions was similar between the groups.
Key words: Aged, strength training, body weight, elastic band, muscle adaptations
Introduction
Strategies to increase or maintain skeletal muscle mass and function throughout life are highly significant because skeletal muscle plays a crucial role in metabolism and performing activities of daily living (Helge et al., 2006; Holloszy, 2005). Skeletal muscle size and strength decrease with age (Clark and Manini, 2008), which in turn elevates the risk of developing a wide range of chronic disorders, including insulin resistance, hyperglycemia (Lee et al., 2011; Sanada et al., 2012), and atherosclerosis (Abe et al., 2012; Ochi et al., 2010), and results in disability, falls, and osteoporosis (Baumgartner et al., 1998; Walsh et al., 2006; Wolfson et al., 1995). One of the most notable problems is a reduction in ambulatory ability, which related to a decrease in lower limb muscle strength (Hayashida et al., 2014; Osawa et al., 2019). High-load resistance training has been primarily recommended as an effective countermeasure against these reductions (Borst, 2004; Garber et al., 2011), which are partly reversible by high external loads for older adults (Frontera et al., 1988; Nilwik et al., 2013). However, high-load resistance training generally requires a supervised program and involves expensive training equipment, and high external loads may present a major barrier for older adults. Hence, a more practical training method is required.
Our recent study in older adults has shown that muscle hypertrophy and increased muscle strength could result from supervised low-load resistance training (3 days a week), which includes exercises without additional external weight (i.e., body weight [BW]-based resistance training) and with the use of elastic bands (EB), even though that is necessarily not performed until concentric failure (Ozaki et al., 2017). As the magnitude of strength gain induced by BW-based resistance training is associated with the relative load on the working muscles (Ozaki et al., 2017; Yoshitake et al., 2011), such training would be especially effective for older adults who have relatively low strength. Moreover, a previous study investigated the effect of a combination of supervised (once a week in a local gym) and unsupervised (6 days a week at home) low-load resistance training and found that the approach significantly increased muscle strength (Yoshitake et al., 2011). However, no study comparing the effects on muscle size and strength between supervised and unsupervised training has been conducted. Furthermore, older adults generally performed low-load resistance training with a relatively high frequency (3-7 days per week) in previous studies (Fujiwara et al., 2010; Ozaki et al., 2017; Tsuzuku et al., 2018; Watanabe et al., 2015; Yoshitake et al., 2011). From the viewpoint of a more practical training, an investigation on the effect of low training frequency (e.g., twice per week) is essential.
Thus, this study aimed to clarify whether low-load resistance training using BW and EB at a low frequency (twice a week) improves muscle size, muscle strength, and physical functions and to compare the training effects between supervised training and combined supervised and unsupervised training in older adults.
Methods
Participants
Untrained fifty-one older adults (ages: 57-75 years) volunteered to participate in this study. They were recruited through printed advertisements and by word of mouth in the Inba area. Some participants selected a supervised training group (S) (n = 34 [7 men and 27 women], age 65.6 ± 5.1 years, height 1.57 ± 0.08 m, body weight 56.9 ± 12.7 kg), whereas the others selected a combined supervised and unsupervised group (SU) (n = 17 [4 men and 13 women], age 68.8 ± 3.8 years, height 1.56 ± 0.08 m, body weight 54.2 ± 9.4 kg). None of the subjects had participated in any regular resistance training for at least 1 year. Participants were instructed to avoid switching to other physical activities and changing their dietary patterns throughout the study. We excluded individuals who failed to follow our instructions and those with chronic orthopedic conditions or any health or medical conditions that limited their ability to perform low-load resistance training. In addition, the participants completed a self-report questionnaire regarding medical history and comorbid conditions. All participants were informed about the methods, procedures, and risks and provided informed consent before participating. This study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee for Human Experiments of the University (Approval Number: 27-52). Muscle thicknesses (MT), muscle strength, and physical function of the participants before (PRE) and 12 weeks after (POST) the start of the training program were evaluated. Subsequently, the training effects were compared between the S and SU groups.
Training program
Both training groups performed low-load resistance training (twice a week for 12 weeks) composed of the following nine exercises: squat, split squat, push-up, heel raise, crunch, hip lift, seated row, shoulder press, and arm curl. The first six exercises were resistance exercises that use BW, without any additional external weight, and the last three exercises were resistance exercises that use EB (Thera-Band®; The Hygenic Corporation, Akron, OH, USA). Each participant selected the color and length of EB for each exercise such that the rate of perceived exertion score was approximately 13 at the end of each set throughout the training period. For the first 2 weeks, the participants performed three sets of eight repetitions for four BW-based exercises with a 60-s rest between sets, and they were instructed to complete the concentric and eccentric phases of each repetition over 3 s. As shown in Table 1, the number of exercises per session, repetitions, sets per exercise, and exercise time were gradually increased, and the rest interval was gradually decreased every 2 weeks throughout the training period. The S group participated in supervised exercise sessions twice a week, and the SU group participated in a supervised exercise session once a week and performed an unsupervised exercise session at home also once a week. The participants in the SU group were asked to submit their recording of the training they performed at home.
Table 1.
Training program.
| Week | Load | Exercises | Reps | CON-ECC | Sets | Interval (s) | Frequency (days/week) |
|---|---|---|---|---|---|---|---|
| 1 | BW | SQ, PU, C, HL | 8 | 3-3 | 3 | 60 | 2 |
| 2 | BW | SQ, PU, C, HL | 8 | 3-3 | 3 | 60 | 2 |
| 3 | BW | SQ, PU, HR, C, HL | 10 | 3-3 | 3 | 60 | 2 |
| 4 | BW | SQ, PU, HR, C, HL | 10 | 3-3 | 3 | 60 | 2 |
| 5 | BW+EB | SQ, PU, HR, SR, C, HL | 10 | 4-4 | 3 | 60 | 2 |
| 6 | BW+EB | SQ, PU, HR, SR, C, HL | 10 | 4-4 | 3 | 60 | 2 |
| 7 | BW+EB | SSQ, PU, SQ, SR, HR, C, HL | 10 | 4-4 | 3 | 45 | 2 |
| 8 | BW+EB | SSQ, PU, SQ, SR, HR, C, HL | 10 | 4-4 | 3 | 45 | 2 |
| 9 | BW+EB | SSQ, PU, SQ, SR, HR, SP, C, HL | 15 | 3-3 | 3 | 45 | 2 |
| 10 | BW+EB | SSQ, PU, SQ, SR, HR, SP, C, HL | 15 | 3-3 | 3 | 45 | 2 |
| 11 | BW+EB | SSQ, PU, SQ, SR, HR, SP, AC, C, HL | 15 | 3-3 | 3 | 30 | 2 |
| 12 | BW+EB | SSQ, PU, SQ, SR, HR, SP, AC, C, HL | 15 | 3-3 | 3 | 30 | 2 |
BW, body-weight based resistance exercises; EB, resistance exercises using elastic bands; SQ, squat; PU, push-up; C, crunch; HL, hip lift; HR, heel raise; SR, seated row; SSQ, split squat; SP, shoulder press; AC, arm curl; CON-ECC, the time (seconds) in the concentric phase and eccentric phase of each repetition.
Muscle thickness
MT was measured via a B-mode ultrasound using a 5 to 18-MHz scanning head (Noblus; Aloka, Tokyo, Japan) in the following eight locations of the right side of the body: the anterior forearm (AF) at 30% proximal between the styloid process and the head of the radius, the anterior and posterior aspects of the upper arm (AA and PA, respectively) at 60% distal between the lateral epicondyle of humerus and the acromial process of the scapula, the abdomen (A) at approximately 2 cm to the right of the umbilicus, the anterior and posterior aspects of the thigh (AT and PT, respectively) at the midway between the lateral condyle of the femur and the greater trochanter, and the anterior and posterior aspects of the lower leg (AL and PL, respectively) at 30% proximal between the lateral malleolus of the fibula and the lateral condyle of the tibia. Before the scans, the participants were resting in the sitting position for at least 30 min. To avoid the influence of fluid shifts within the muscle, the measurements were performed at about the same time. All measurements were performed by the same operator, with the participants in the supine/prone position. The subcutaneous adipose tissue–muscle interface and the muscle–bone interface were identified on ultrasound images, and the distance between the two interfaces was recorded as the MT. Test–retest (inter-session) reliabilities were calculated using intraclass correlation coefficient (ICC), standard errors of measurement (SEM), and minimal difference. The ICC, SEM, and minimal difference for MT in the eight locations were determined in 10 older men and women: AF: 0.987, 0.28 mm, 0.78 mm; AA: 0.986, 0.39 mm, 1.08 mm; PA: 0.998, 0.15 mm, 0.42 mm; A: 0.998, 0.09 mm, 0.25 mm; AT: 0.992, 0.37 mm, 1.03 mm; PT: 0.994, 0.37 mm, 1.03 mm; AL: 0.993, 0.21 mm, 0.58 mm; PL: 0.998, 0.22 mm, 0.61 mm.
Maximal isometric strength
Maximal voluntary isometric knee extensor strength of the right leg was determined using a dynamometer (Takei, Tokyo, Japan). During the test, each participant was seated on a chair with the hip joint angle positioned at 90° flexion (0° equals full hip extension). The ankle was firmly strapped to the distal pad of the lever arm. Subsequently, the participants were instructed to perform maximal isometric knee extension for approximately 5 s at a fixed knee joint angle of 90°. A knee joint angle of 0° corresponded to full knee extension. Several warm-up contractions (2–3 submaximal contractions and 1–2 near-maximal contractions) were performed before each testing. Two or three maximal efforts for the isometric measurement were performed, and the peak torque was used in the data analysis. All measurements were performed by the same operator. The test–retest (inter-session) reliabilities using ICC, SEM, and minimal difference for knee extension strength was 0.945, 3.41 kg, and 9.45 kg, respectively.
Physical functions
Physical functions were evaluated using the following tests: the 10-m walk test, the 30-s repeat sit-to-stand test (CS-30), and the 30-s sit-up test. The walking performance was evaluated by timing each participant as they walked across a 10-m corridor on a hard-surfaced floor. The width of the corridor was set at 1 m. The participants performed two timed trials and were encouraged to maintain a straight course. They were asked to walk down the corridor as fast as possible. Their times were measured using a mat switch (Takei, Tokyo, Japan), and the best time was used in the data analysis. For the CS-30 test, they were asked to complete the maximum number of sit-to-stand trials using a chair (40-cm height) with both arms held across the chest. For the 30-s sit-up test, they were asked to lie in the supine position on a mat with knees flexed to 90° and both arms held across the chest and to perform as many sit-ups as possible for 30 s with an assistant stabilizing both knees. The test–retest (inter-session) reliabilities using the ICC, SEM, and minimal difference were 0.833, 0.29 s, and 0.80 s, respectively, for the 10-m walking test; 0.780, 1.48 n, 4.10 n, respectively, for the CS-30 test; and 0.987, 0.59 n, 1.64 n, respectively, for the 30-s sit-up test.
Statistical analyses
Statistical tests were performed using SPSS version 23.0 software (SPSS Inc., Chicago, IL, USA). Results are expressed as means and standard deviations. Changes in scores are represented by means and 95% confidence intervals. For all variables, a repeated measures analysis of variance of time (PRE and POST) with a between-participant factor of group (S and SU) was used. If there was a significant interaction, post-hoc tests were performed using t-test. Statistical significance was set at p < 0.05.
Results
All participants completed the study, and the mean training executing rate was 89.3% in the S group and 94.9% in the SU group (no significant difference was noted between the two groups). The participants with a rate of >90% were included in the analysis (S, n = 22 [6 men and 16 women]; SU, n = 13 [4 men and 9 women]). Before training, no significant differences in age, anthropometric variables, MT, strength, and physical functions between the two groups were observed. For body mass and body mass index, group × time interactions were noted (p < 0.01); only the values in the S group showed significance, which slightly increased from PRE to POST (0.7 [0.2, 1.1] kg, p = 0.003; 0.3 [0.2, 0.5] kg·m-2, p < 0.001).
Muscle thickness
The main effects of group and time and group × time interactions were not significant in AL and PL (Table 2). For PA and A, significant group × time interactions were not observed; however, main effects of time (p < 0.01) with the MT increasing from PRE to POST (PA 1.6 [0.7, 2.6] mm, p = 0.001; A 0.6 [0.3, 1.0] mm, p = 0.02) were noted. For the other four locations, group × time interactions were observed (p < 0.05). AT significantly increased from PRE to POST in both groups (S 3.5 [2.6, 4.4] mm; SU 1.8 [0.6, 2.9] mm); however, the increase was greater in the S group. For the rest of the locations, only the values in the S group significantly increased (AF 0.6 [0.3, 1.0] mm, p = 0.001; AA 0.7 [0.2, 1.2] mm, p = 0.005; PT 2.2 [1.1, 3.2] mm, p < 0.001).
Table 2.
Changes in muscle thicknesses in both groups. Data are presented as means±SD.
| S | SU | p value | |||||
|---|---|---|---|---|---|---|---|
| PRE | POST | PRE | POST | Time | Group | Interaction | |
| AF, mm | 33.8 ± 5.0 | 34.4 ± 4.7 †† | 34.2 ± 3.8 | 33.8 ± 3.6 | 0.482 | 0.950 | <0.01 |
| AA, mm | 23.9 ± 4.7 | 24.6 ± 4.7 †† | 24.6 ± 4.5 | 24.4 ± 4.2 | 0.180 | 0.869 | <0.05 |
| PA, mm | 20.0 ± 6.6 | 22.1 ± 6.5 | 17.7 ± 5.1 | 18.8 ± 5.3 | <0.01 | 0.191 | 0.294 |
| A, mm | 7.9 ± 2.5 | 8.3 ± 2.3 | 8.9 ± 2.3 | 9.8 ± 2.4 | <0.01 | 0.138 | 0.198 |
| AT, mm | 26.8 ± 5.9 | 30.3 ± 5.9 †† | 26.4 ± 6.8 | 28.2 ± 6.6†† | <0.01 | 0.571 | <0.05 |
| PT, mm | 49.1 ± 8.0 | 51.3 ± 8.8 †† | 50.2 ± 7.4 | 50.0 ± 7.5 | <0.05 | 0.973 | <0.05 |
| AL, mm | 22.3 ± 3.9 | 22.8 ± 3.5 | 21.8 ± 3.6 | 21.8 ± 3.3 | 0.145 | 0.566 | 0.170 |
| PL, mm | 57.1 ± 7.6 | 58.0 ± 7.9 | 57.1 ± 6.6 | 56.8 ± 6.8 | 0.273 | 0.804 | 0.055 |
S, supervised training; SU, combination of supervised and unsupervised training; PRE, before training; POST, after 12 weeks of training; AF, the anterior aspect of the forearm; AA, the anterior aspect of the upper arm; PA, the posterior aspect of the upper arm; A, the abdomen; AT, the anterior aspect of the thigh; PT, the posterior aspects of the thigh; AL, the anterior aspect of the lower leg; PL, the posterior aspect of the lower leg.
†† p < 0.01 vs. PRE.
Muscle strength and physical functions
For both absolute and relative values (to body mass) of isometric knee extension strength (Figure 1), group × time interactions were not observed; however, main effects of time (p < 0.001), which increased from PRE to POST (3.1 [1.7, 4.6] kg, p < 0.001; 0.6 [0.3, 0.8] kg/kg, p < 0.001), were noted. Similarly, main effects of time (p < 0.05), but no group × time interactions, were observed in the 10-m walk, CS-30, and 30-s sit-up tests. All values significantly increased from PRE to POST (10-m walk -0.2 [-0.4, -0.06] s, p = 0.007; CS-30 2.6 [1.2, 4.0] n, p = 0.001; 30-s sit-up 2.9 [2.0, 3.8] n, p < 0.001).
Figure 1.
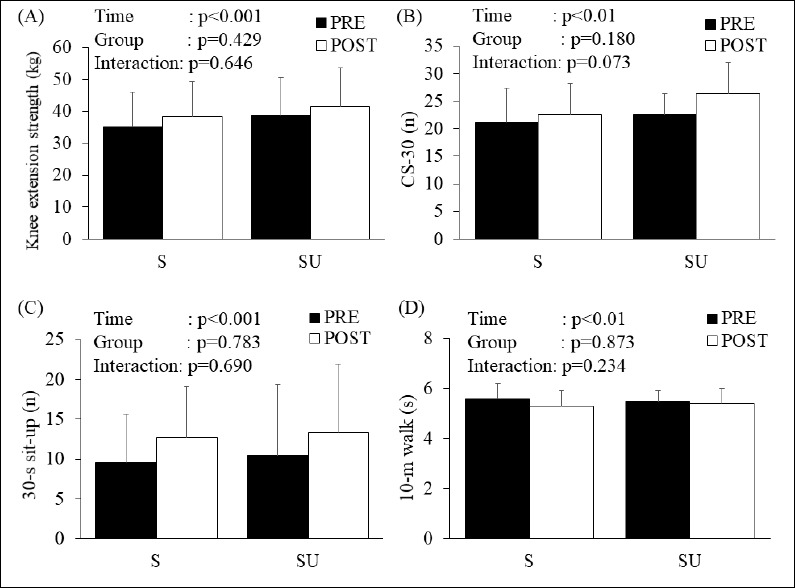
Changes in knee extension strength and physical functions in both groups. Data are presented as mean C standard deviation. (A) Knee extension strength, (B) CS-30; 30-s repeat sit-to-stand test, (C) 30-s sit-up test, (D) 10-m walk test. PRE, before training; POST, after 12 weeks of training.
Discussion
The major finding of this study was that, in older adults, muscle hypertrophy and increased muscle strength and physical functions could be induced by low-load resistance training using BW and EB (both S and SU training) even when performed for only twice a week. Given that the exercises in previous studies were generally performed with higher frequency (3–7 days per week) (Fujiwara et al., 2010; Ozaki et al., 2017; Tsuzuku et al., 2018; Watanabe et al., 2015; Yoshitake et al., 2011), the exercise program in our study is more practical. Furthermore, although the muscle hypertrophic effects were generally greater in the S group, the magnitude of increase in muscle strength and physical functions was similar between the S and SU groups.
In this study, we showed that the hypertrophic effects were site-specific. The hypertrophic effects (i.e., MT) in AF, AA, AT, and PT were greater in the S group; a significant muscle hypertrophy was observed only in the S group and the magnitude of increase in muscle size was greater in the S group. Given that the provided training variables (the number of exercises per session, repetitions, sets per exercise, and exercise time) were the same between the S and SU groups, one of the factors resulting in the difference in hypertrophic effects may be the differences in the form of each exercise, such as the less range of motion in the SU group. However, further studies are needed to clearly identify the factors. In addition, only within-group changes across time were observed; no differences between both groups at PRE and POST were found, suggesting that the changes in MT may need to be interpreted with caution. Moreover, MT in PA and A, which are locations that are stimulated mainly by push-up and crunch, respectively, increased similarly in both groups. A previous study demonstrated that a single set of 10–15 reps push-up and knee to chest exercises three times a week (once in supervised exercise and twice at home) does not result in muscle hypertrophy in PA and A in older adults (Watanabe et al., 2015); in another study, three sets of push-up three times a week (all supervised exercises) significantly increased PA muscle size, even among young men (Kikuchi and Nakazato, 2017). Hence, multiple sets of exercises stimulating PA and A muscles performed more than twice a week could result in muscle hypertrophy in older adults, regardless of whether the training is S or SU. Furthermore, heel raise exercise did not induce muscle hypertrophy for PL in our study. Fujiwara et al. (2010) showed that PA muscle hypertrophy in older adults when a set of heel raise with 100 repetitions is performed almost every day for 2 months. Thus, to induce muscle hypertrophy in the lower limbs, which is frequently used in activities of living, greater training volume may be required.
In contrast to the muscle hypertrophic effects, isometric knee extension strength and physical functions increased similarly in both the S and SU training groups. Muscle strength is greatly affected by the training load (Ozaki et al., 2015). Increased knee extension strength would result mainly from the stimuli, such as squat and split squat, which are exercises using BW. The relative training load on working muscles during BW exercises is determined by the ratio of body weight to the strength, which at the start of the training period is associated with the magnitude of strength gain (Ozaki et al., 2017; Yoshitake et al., 2011). In our study, the significant correlation between the ratio of body weight of isometric knee extension strength at the start of the training period and the training-induced change in the strength was also observed (r = -0.545, p < 0.01). Meanwhile, no significant differences in body weight and knee extension strength at PRE between both groups were found; thus, a difference in the magnitude of increase in muscle strength appears not plausible. Furthermore, sit-to-stand and walking speed are correlated with knee extension strength in older adults in previous cross-sectional studies (Samson et al., 2000; Nakatani et al., 2002), and an interventional study showed that these improvements tend to correlate with knee joint strength (Ozaki et al., 2011). Hence, as no difference in the improvement of knee extension strength was noted between the groups in our study, it seems reasonable that physical functions increased similarly between the S and SU groups. Given that there are differences in muscle hypertrophic effects between S and SU training, trainers and therapists or their clients may need to select the most suitable training approach, which would depend on the purpose, time pressure, and motivation.
A control group was not used, which is a limitation of our study. Thus, the training effects need to be interpreted with caution. However, substantial effects of subtle changes in activities of daily living over 12 weeks on muscle size and strength are highly unlikely. Furthermore, participants were instructed to avoid switching to other physical activities and changing their dietary patterns throughout the study period.
Conclusion
Low-load resistance training using BW and EB even for only twice a week could induce muscle hypertrophy and increase muscle strength and physical functions in older adults after 12 weeks of training. Although the muscle hypertrophic effects are greater in the S group than in the SU group, the magnitude of increase in muscle strength and physical functions was similar between the groups.
Acknowledgements
This work was supported by the Center of Innovation Program from Japan Science and Technology Agency (JST) and the Juntendo University Institute of Health and Sports Science & Medicine. The authors have no conflicts of interests to declare. The experiments comply with the current laws of the country in which they were performed.
Biographies
Hayao OZAKI
Employment
School of Sport and Health Science, Tokai Gakuen University, Miyoshi, Aichi, Japan
Degree
PhD
Research interests
Exercise physiology, Training science
E-mail: ozaki.hayao@gmail.com
Shuji SAWADA
Employment
COI Project Center, Juntendo University, Hongo, Bunkyo-ku, Tokyo, Japan
Degree
PhD
Research interests
Exercise physiology
E-mail: sh-sawada@juntendo.ac.jp
Takuya OSAWA
Employment
Faculty of Sports and Health Sciences, Japan Women’s College of Physical Education, Setagaya-ku, Tokyo, Japan
Degree
PhD
Research interest
Exercise physiology
E-mail: osawa.takuya@jwcpe.ac.jp
Toshiharu NATSUME
Employment
COI Project Center, Juntendo University, Hongo, Bunkyo-ku, Tokyo, Japan
Degree
PhD
Research interests
Exercise physiology
E-mail: natsumetoshiharu@gmail.com
Toshinori YOSHIHARA
Employment
Graduate School of Health and Sports Science, Juntendo University, Inzai, Chiba, Japan
Degree
PhD
Research interests
Exercise physiology
E-mail: t-yoshih@juntendo.ac.jp
Pengyu DENG
Employment
Graduate School of Health and Sports Science, Juntendo University, Inzai, Chiba, Japan
Degree
PhD
Research interests
Exercise physiology
E-mail: deng@juntendo.ac.jp
Shuichi MACHIDA
Employment
Graduate School of Health and Sports Science, Juntendo University, Inzai, Chiba, Japan
Degree
PhD
Research interests
Exercise physiology
E-mail: machidas@juntendo.ac.jp
Hisashi NAITO
Employment
Graduate School of Health and Sports Science, Juntendo University, Inzai, Chiba, Japan
Degree
PhD
Research interests
Exercise physiology
E-mail: hnaitou@juntendo.ac.jp
References
- Abe T., Thiebaud R.S., Loenneke J.P., Bemben M.G., Loftin M., Fukunaga T. (2012) Influence of Severe Sarcopenia on Cardiovascular Risk Factors in Nonobese Men. Metabolic Syndrome and Related Disorders 10, 407-412. [DOI] [PubMed] [Google Scholar]
- Baumgartner R.N., Koehler K.M., Gallagher D., Romero L., Heymsfield S.B., Ross R.R., Garry P.J., Lindeman R.D. (1998) Epidemiology of sarcopenia among the elderly in New Mexico. American Journal of Epidemiology 147, 755-763. [DOI] [PubMed] [Google Scholar]
- Borst S.E. (2004) Interventions for sarcopenia and muscle weakness in older people. Age and Ageing 33, 548-555. [DOI] [PubMed] [Google Scholar]
- Clark B.C., Manini T.M. (2008) Sarcopenia =/= dynapenia. The Journals of Gerontology Series A Biological Sciences and Medical Sciences 63, 829-834. [DOI] [PubMed] [Google Scholar]
- Frontera W.R., Meredith C.N., O’Reilly K.P., Knuttgen H.G., Evans W.J. (1988) Strength conditioning in older men: skeletal muscle hypertrophy and improved function. Journal of Applied Physiology 64, 1038-1044. [DOI] [PubMed] [Google Scholar]
- Fujiwara K., Toyama H., Asai H., Maeda K., Yaguchi C. (2010) Regular heel-raise training focused on the soleus for the elderly: evaluation of muscle thickness by ultrasound. Journal of Physiological Anthropology 29, 23-28. [DOI] [PubMed] [Google Scholar]
- Garber C.E., Blissmer B., Deschenes M.R., Franklin B.A., Lamonte M.J., Lee I.M., Nieman D.C., Swain D.P. (2011) American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healthy adults: guidance for prescribing exercise. Medicine and Science in Sports and Exercis 43, 1334-1359. [DOI] [PubMed] [Google Scholar]
- Hayashida I., Tanimoto Y., Takahashi Y., Kusabiraki T., Tamaki J. (2014) Correlation between muscle strength and muscle mass, and their association with walking speed, in community-dwelling elderly Japanese individuals. PLoS One 9, e111810. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Helge J.W., Biba T.O., Galbo H., Gaster M., Donsmark M. (2006) Muscle triacylglycerol and hormone-sensitive lipase activity in untrained and trained human muscles. European Journal of Applied Physiology 97, 566-572. [DOI] [PubMed] [Google Scholar]
- Holloszy J.O. (2005) Exercise-induced increase in muscle insulin sensitivity. Journal of Applied Physiology (1985) 99, 338-343. [DOI] [PubMed] [Google Scholar]
- Kikuchi N., Nakazato K. (2017) Low-load bench press and push-up induce similar muscle hypertrophy and strength gain. Journal of Exercise Science & Fitness 15, 37-42. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lee C.G., Boyko E.J., Strotmeyer E.S., Lewis C.E., Cawthon P.M., Hoffman A.R., Everson-Rose S.A., Barrett-Connor E., Orwoll E.S., Study O.F.M. (2011) Association Between Insulin Resistance and Lean Mass Loss and Fat Mass Gain in Older Men without Diabetes Mellitus. Journal of the American Geriatrics Society 59, 1217-1224. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Nakatani T., Nadamoto M., Mimura K., Itoh M. (2002) Validation of a 30-sec chair-stand test for evaluating lower extremity muscle strength in Japanese adults. Japan Journal of Physical Education, Health and Sport Sciences 47, 451-461. (In Japanese: English abstract). [Google Scholar]
- Nilwik R., Snijders T., Leenders M., Groen B.B.L., van Kranenburg J., Verdijk L.B., van Loon L.J.C. (2013) The decline in skeletal muscle mass with aging is mainly attributed to a reduction in type II muscle fiber size. Experimental Gerontology 48, 492-498. [DOI] [PubMed] [Google Scholar]
- Ochi M., Kohara K., Tabara Y., Kido T., Uetani E., Ochi N., Igase M., Miki T. (2010) Arterial stiffness is associated with low thigh muscle mass in middle-aged to elderly men. Atherosclerosis 212, 327-332. [DOI] [PubMed] [Google Scholar]
- Osawa Y., Chiles Shaffer N., Shardell M.D., Studenski S.A., Ferrucci L. (2019) Changes in knee extension peak torque and body composition and their relationship with change in gait speed. Journal of Cachexia, Sarcopenia and Muscle 10, 1000-1008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ozaki H., Abe T., Alan E., Mikesky, Sakamoto A., Machida S., Naito H. (2015) Physiologocal stimuli necessary for muscle hypertrophy. The Journal of Physical Fitness and Sports Medicine 4, 43-51. [Google Scholar]
- Ozaki H., Kitada T., Nakagata T., Naito H. (2017) Combination of body mass-based resistance training and high-intensity walking can improve both muscle size and V O2 peak in untrained older women. Geriatrics & Gerontology International 17, 779-784. [DOI] [PubMed] [Google Scholar]
- Ozaki H., Sakamaki M., Yasuda T., Fujita S., Ogasawara R., Sugaya M., Nakajima T., Abe T. (2011) Increases in thigh muscle volume and strength by walk training with leg blood flow reduction in older participants. The Journals of Gerontology Series A: Biological Sciences and Medical Sciences 66, 257-263. [DOI] [PubMed] [Google Scholar]
- Samson M.M., Meeuwsen I.B.A.E., Crowe A., Dessens J.A.G., Duursma S.A., Verhaar H.J.J. (2000) Relationships between physical performance measures, age, height and body weight in healthy adults. Age and Ageing 29, 235-242. [DOI] [PubMed] [Google Scholar]
- Sanada K., Iemitsu M., Murakami H., Gando Y., Kawano H., Kawakami R., Tabata I., Miyachi M. (2012) Adverse effects of coexistence of sarcopenia and metabolic syndrome in Japanese women. European Journal of Clinical Nutrition 66, 1093-1098. [DOI] [PubMed] [Google Scholar]
- Tsuzuku S., Kajioka T., Sakakibara H., Shimaoka K. (2018) Slow movement resistance training using body weight improves muscle mass in the elderly: A randomized controlled trial. Scandinavian Journal of Medicine & Science in Sports 28, 1339-1344. [DOI] [PubMed] [Google Scholar]
- Walsh M.C., Hunter G.R., Livingstone M.B. (2006) Sarcopenia in premenopausal and postmenopausal women with osteopenia, osteoporosis and normal bone mineral density. Osteoporosis International 17, 61-67. [DOI] [PubMed] [Google Scholar]
- Watanabe Y., Tanimoto M., Oba N., Sanada K., Miyachi M., Ishii N. (2015) Effect of resistance training using bodyweight in the elderly: Comparison of resistance exercise movement between slow and normal speed movement. Geriatrics & Gerontology International 15, 1270-1277. [DOI] [PubMed] [Google Scholar]
- Wolfson L., Judge J., Whipple R., King M. (1995) Strength Is a Major Factor in Balance, Gait, and the Occurrence of Falls. Journals of Gerontology Series a-Biological Sciences and Medical Sciences 50, 64-67. [DOI] [PubMed] [Google Scholar]
- Yoshitake Y., Takai Y., Kitamura T., Kawanishi M., Kanehisa H. (2011) Body mass-based exercise in middle-aged and older women. International Journal of Sports Medicine 32, 924-928. [DOI] [PubMed] [Google Scholar]