

Abstract
The research describes willingness of urban and rural residents over age 40 to enter care homes and examines personal factors which impact their willingness. Trained investigators gathered survey responses on sociodemographic information, physical health status, lifestyle behaviors, willingness to enter care homes, and specific service needs. 34.8% of the 1186 survey participants expressed willingness to enter care homes, with lower percentage of rural residents (25.8%) expressing willingness compared to urban residents (41.6%). The decision to enter care homes is impacted by occupation for urban residents and education status for rural residents. Healthcare remains the top consideration when considering care homes.
Keywords: aging, care homes, China, urban–rural differences, willingness
Key Points
Compared to national policy goals, there is both a lack of supply of care home beds and an under-utilization of existing elder-care services in Dujiangyan, Sichuan Province, China.
There is a significant difference in willingness to enter care homes with 41.6% of urban residents and 25.8% of rural residents willing to consider institutional elder-care in the future.
Occupation (employed or not) is the main factor that affects urban residents’ willingness to live in an elder-care institution; the main demographic factor predicting rural residents’ willingness is level of education.
Policies should recognize differences between urban and rural populations with regard to elder-care needs, and provide a range of options for individuals seeking forms of institutional elder-care.
Further research is needed to understand possible cultural barriers to willingness to enter institutional elder-care; policies should look to international examples to provide multi-faceted and tiered elder-care, which involve family and social support to varying degrees.
1. Introduction
It is estimated that by 2030, the global population of people over 65 years old will exceed 1 billion, and the global population over 50 will be greater than the population of those under 17 years old[1]; in projected models, China's population of those over 65 years old will surpass that of Japan in having the highest proportion of elderly, and China is aging at a faster pace than Japan.[2] According to the 2018 National Economic and Social Development Statistics Bulletin issued by the National Bureau of Statistics of China, by the end of 2018, the population in China of those over 60-years-old was 949.49 million, surpassing the population of 0 to 15 years old by 248.6 million.[3] It is estimated that by 2020, the population of those over 60 years old will reach 255 million and the number of elderly living alone will reach 118 million.[4] The speed and scale of China's aging is unprecedented in the world. Although the number of care homes in China is increasing, only 2% of the elderly live in care homes.[5] As of 2017, there are 155,000 various types of elderly care service institutions and facilities in the country, with a total of 7.448 million beds in these elder-care institutions, or 30.9 elder-care beds for every 1000 elderly people. In 2017, the Chinese State Council released an official policy as part of the 13th Five Year Plan for the development and expansion of elderly care in China. This plan aims to develop and strengthen elderly care in China, with a specific goal of having 35 to 40 elder-care beds available for every 1000 elder over 60. Thus, there is a significant gap between the current status of elder-care and the proposed plan.[6]
China has a rapidly aging society, and children are often expected to care for their elderly parents, given Confucian values of filial piety.[7,8] Chinese society has undergone rapid changes in the past decades: the industrialization and urbanization brought about by China's rapid development,[9] and the family planning policy which limited each family to 2 children[10] have had significant impacts on the demography of China and present challenges to the former norms of children living with and caring for their aging parents.[11] Previous studies have shown that adult children who are willing to live with their parents are decreasing in number and proportion.[12,13] According to survey results, in large urban cities, the number of empty nesters with no children nearby has reached 70%.[14] In rural areas, as migrant workers enter the city and the hukou system is relaxed, elderly people in rural areas are rarely cared for by their children.[11] These studies indicate that as the demographics in China shift, the role of the nuclear family in caring for the elderly is shrinking and the ability for a family to care for elderly has been weakening.[15,16]
In China, due to traditional norms of children rearing and caring for the elderly,[17] many elderly people expect to be financially supported by their children.[18] For example, elderly people with more children are less likely to purchase insurance than those with fewer children.[19] The expectation that children will financially support their elderly parents is even greater in rural areas, where there are lower levels of state financial investment and support.[20] Thus, as the proportion of elderly people grow and the rate of inter-generational cohabitation continues to decline, the importance of institutional elder-care has become more prominent.[21,22] In China, nursing homes have traditionally had a negative reputation, as those individuals who resided in nursing homes were assumed to have no children, relatives, or income.[23] In the common “4–2–1” or “4–2–2” (4 grandparents, 2 parents, 1 or 2 children) family structures, adult children are under significant pressure to care for their aging parents and grandparents themselves, putting enormous pressure on only children. This pressure may lead to negative consequences including caregiver burnout and depression.[24,25] Because of this, the Chinese government has implemented a series of policies to support the development of institutional care as one of the important pillars of the 13th Five-Year Plan (2016–2020). The State Council has also issued a series of documents to support the development of care homes.[26]
In recent years, the numbers of old-age institutions in major cities such as Beijing, Shanghai, Wuhan, and Chongqing have steadily increased.[19,27,28] The purpose of this study is to analyze the current state of willingness of residents to choose care homes and the factors which influence their choices. Previous studies determined that willingness to enter elder-care correlated with age, gender, income, education, marital status, and presence of non-communicable diseases (NCDs), etc,[29–31] and studies have shown that poor health self-assessment is related to willingness to consider an care home.[32,33] Considering the impact of physical activity on the physical and mental health of the elderly, there are also studies that have focused on effects of physical activity. Previous research has focused on those over the age of 60.[34,35] However, as the one-child policy was implemented in 1982, those aged 40 to 59 are the first generation affected by this family planning policy and recent economic growth and urbanization; this generation will be soon entering the “aging population.” This study therefore expands previous research by including this critical population. Additionally, this study compares differences between urban and rural residents, given known differences in investment between urban and rural pensions and social benefits.[36] The purpose of this study is to study the personal factors affecting individuals’ willingness to consider care homes and the specific needs sought in elder-care, in order to provide policy recommendations for alleviating the gap between supply and demand for care homes and adjusting relevant policies to effect necessary change.
2. Methods
2.1. Ethics consideration
The Ethical Committee of Sichuan University approved the study protocol. Participants were informed about the aim of the survey, the selection criterion of the sample, and the assurance that the information was only used for research. All participants gave written informed consent before inclusion in the study.
2.2. Study setting and study population
This cross-sectional study was conducted between August and October 2018 in Dujiangyan, Sichuan Province, China. Dujiangyan City is located northwest of Chengdu in Sichuan Province. In 2016, the resident population of Dujiangyan was 690,900, and the proportion of those over 65 reached 13.92%, higher than the national average of 10.8%. There were 132,000 people who were aged 60 and over, accounting for 20.1% of the total population. The old-age burden coefficient is 18.43% higher than the national level of 14.30%,[14,37] and there are 20.42 elder-care beds per 1000 elderly people, which is lower than the national level of 31.6 elder-care beds per 1000 in the country.[38] Given the population of elderly people, the demand for elder-care services is significant and the supply is insufficient. However, the occupancy rate of the public care homes in Dujiangyan City is 68.3% and the occupancy rate of private care homes is 41.8%,[37] evidence that residents are not yet willing to consider care homes.
Dujiangyan is composed of 10 rural townships (each of which has several villages) and 9 urban districts (which are each composed of several communities). We utilized a staged cluster sampling method, first randomly selecting 5 townships and 5 districts. From each township or district, 150 residents were randomly selected to participate in the survey from a resident database provided by local government. Residents were contacted by the investigator, and the significance and purpose of the research was explained to the participant. After obtaining informed consent, each participant was provided either a digital or paper-copy of the close-ended survey, and a graduate student from West China School of Public Health College of Sichuan University was present to provide clarification for any questions. The survey took an average of 30 minutes. All questionnaires were checked for completeness.
A total of 1500 residents were invited to participate in the survey and 27 refused to participate. Through this cross-sectional survey, 1473 questionnaires were obtained (98.2 response rate). 70 individuals did not provide complete sociodemographic data, 85 individuals did not provide physical health information, and 56 individuals did not answer questions regarding their preference regarding care homes. 76 individuals were excluded as they were younger than 40 years old. The remaining 1186 individuals were included in the analysis (Fig. 1).
Figure 1.
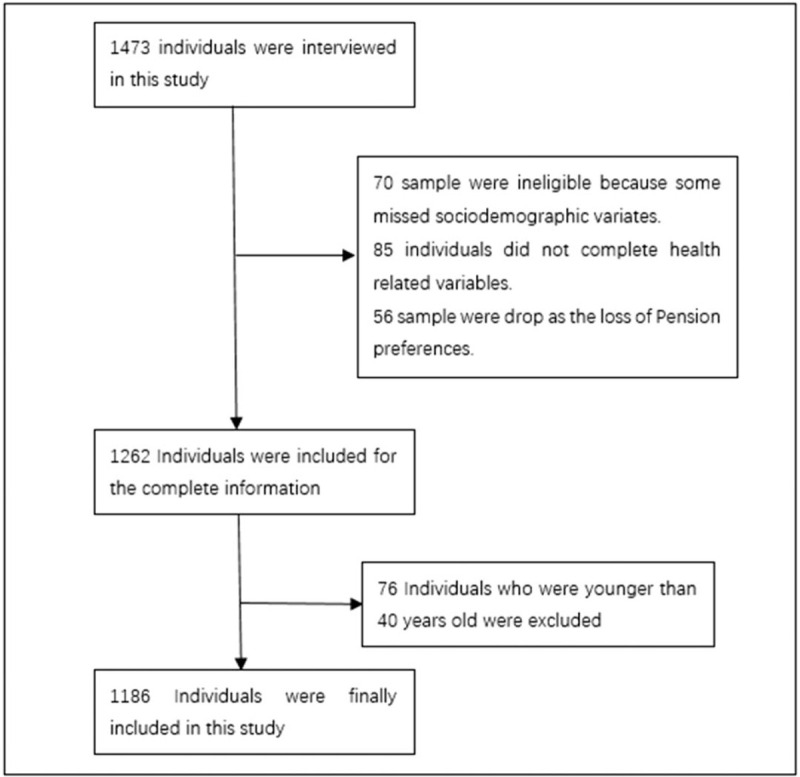
Participants’ flow in the study (there are no symbols and abbreviations that need to be noted in the figure).
2.3. Dependent variable
The dependent variable was willingness to consider a care home. Interviewers first defined care homes as institutions for elderly to receive comprehensive services such as food, cleaning, health care, health management, and social and recreational activities.[26] The interviewer then asked the respondent whether he or she understood the concept and could explain the concept to others. The interviewer then asked: “Would you be willing to reside in a care home in the future?” If the respondent answered yes, follow-up questions included: why would you choose a care home? What services do you think are necessary in a care home? Each of these questions had set responses validated and according to National Healthy City Questionnaires,[39] which include Beijing, Suzhou, Shanghai Healthy Cities Questionnaires, and the National Healthy Cities Evaluation Index System (China, 2018), the members of the research team selected items about elderly care. These questions developed via pilot qualitative interviews with on-the-ground researchers. A total of 30 subjects from public care homes, and the Civil Affairs Bureau participated in the pilot survey. The options in the questionnaire were pilot tested iteratively; the category of “other” captured all remaining responses. Respondents could select as many of the options as they felt were relevant or none of the options. Those who answered that they would not be willing to reside in a care home were not asked further questions.
2.4. Independent variables
The independent variables consist of sociodemographic information, physical health status, and lifestyle behavior.
Sociodemographics: We collected the age (age 40–59, ≥60 years old), gender (male, female), education, (elementary school and below, junior high school, high school, undergraduate or junior college), marital status (married, not married), occupation (employed, unemployed), and monthly income (<$141, $141–$564, ≥$564) of the respondents.
Physical health: Data regarding chronic disease state (e.g., hypertension, diabetes, coronary heart disease, stroke, and primary malignant respiratory diseases) were collected from participants. Participants were organized according to whether they had fewer than 2 chronic diseases (less than 2), 2 or more chronic disease, or no chronic diseases.[40]
Lifestyle and behavior: Researchers recorded who the respondent currently resides with, as well as whether or not they smoke or drink, and their physical activity levels. Physical activity levels over the past 2 weeks were calculated with the validated Chinese version of the International Physical Activity Long Volume (IPAQ-L).[41]
2.5. Statistical analysis
Chi-square tests were used to analyze categorical variables, logistic regression was used to analyze the relationships between independent variables, and descriptive analysis was used to illustrate the reasons for people choosing institutions and the services needed. All P values were two-sided, and a P-value of <.05 was considered statistically significant. All survey data were entered using Epi data 3.1. Statistical analysis was performed using STATA 15.0.
3. Results
3.1. Sample characteristics
Characteristics of our study sample are shown in Table 1. A total of 1186 participants (489, 41.2% male) were enrolled in the study, with an average age of 52.4 years (range 40–89 years). 1048 participants were married (88.4%). Of the survey respondents, 697 are employed (58.8%). 397 (33.5%) received college education and 320 (27.0%) received high school education. 770 (64.9%) reported a monthly average income of $141 to $564. 64 people (5.4%) had 2 or more common chronic non-communicable diseases, 272 (22.9%) were smokers, and 240 (20.2%) drink alcohol. 74.2% of the respondents were highly or somewhat physically active.
Table 1.
Demographic and social characteristics of the respondents and factors associated with willing to enter a care home.
| Total (n = 1185) | City (n = 670) | Rural (n = 515) | |||||||
| Variable | Willing | Unwilling | P | Willing | Unwilling | P | Willing | Unwilling | P |
| Total | 34.8% | 65.2% | 41.6% | 58.4% | 25.8% | 74.2% | |||
| Age | <.001∗ | .006∗ | .003∗ | ||||||
| Age 40–59 | 38.2% | 61.8% | 44.2% | 55.8% | 29.4% | 70.6% | |||
| ≥60 yr old | 23.4% | 76.6% | 31.0% | 69.0% | 16.7% | 83.3% | |||
| Gender | .322 | .108 | .826 | ||||||
| Male | 36.4% | 63.6% | 45.5% | 54.5% | 26.3% | 73.7% | |||
| Female | 33.6% | 66.4% | 39.2% | 60.8% | 25.4% | 74.6% | |||
| Marriage | .616 | .293 | .538 | ||||||
| Married | 35.0% | 65.0% | 42.4% | 57.6% | 25.4% | 74.6% | |||
| Not married | 32.8% | 67.2% | 36.0% | 64.0% | 29.0% | 71.0% | |||
| Education | <.001∗ | .015∗ | <.001∗ | ||||||
| Elementary school and below | 18.8% | 81.2% | 28.4% | 71.6% | 14.3% | 85.7% | |||
| Junior high school | 27.2% | 72.8% | 33.9% | 66.1% | 21.9% | 78.1% | |||
| High school | 40.0% | 60.0% | 45.9% | 54.1% | 31.9% | 68.1% | |||
| Undergraduate or junior college | 56.2% | 43.8% | 44.9% | 55.1% | 40.4% | 59.6% | |||
| Occupation | <.001∗ | <.001∗ | <.001∗ | ||||||
| Employed | 42.9% | 57.1% | 46.6% | 53.4% | 36.4% | 63.6% | |||
| Unemployed | 23.2% | 76.8% | 25.6% | 74.4% | 15.4% | 84.6% | |||
| Monthly income ($) | <.001∗ | .064 | .001∗ | ||||||
| <$141 | 19.7% | 80.3% | 33.3% | 66.7% | 16.9% | 83.1% | |||
| $141–$564 | 36.0% | 64.0% | 60.0% | 40.0% | 28.7% | 71.3% | |||
| ≥$564 | 46.0% | 54.0% | 50.0% | 50.0% | 37.9% | 62.1% | |||
| Physical activity level | .025∗ | .126 | .190 | ||||||
| High | 30.9% | 69.1% | 38.0% | 62.0% | 22.3% | 77.7% | |||
| Medium | 36.8% | 63.2% | 42.3% | 57.7% | 28.0% | 72.0% | |||
| Low | 39.7% | 60.3% | 47.6% | 52.4% | 30.2% | 69.8% | |||
| Non-infectious chronic disease | .543 | .684 | .300 | ||||||
| Greater than or equal to 2 | 31.3% | 68.8% | 45.2% | 54.8% | 18.2% | 81.8% | |||
| Less than 2 | 35.0% | 65.0% | 41.5% | 58.5% | 26.3% | 73.7% | |||
| Smoking | .95 | .053 | .116 | ||||||
| Yes | 34.9% | 65.1% | 48.9% | 51.1% | 20.7% | 79.3% | |||
| No | 34.7% | 65.3% | 39.8% | 60.2% | 27.6% | 72.4% | |||
| Drinking | .409 | .612 | .118 | ||||||
| Yes | 32.5% | 67.5% | 43.7% | 56.3% | 20.2% | 79.8% | |||
| No | 35.3% | 64.7% | 41.2% | 58.8% | 27.4% | 72.6% | |||
P < .05.
Overall, 34.8% of respondents would choose care homes; 41.6% of the urban residents and 25.8% of the rural residents are willing to choose institutional elder-care. Differences in respondents’ willingness to live in care homes were affected by age, education, occupation, monthly average income, and physical activity level among the whole population (P < .05). When analyzed independently, significant factors for the urban population included age, occupation, and education. For the rural population, significant factors included age, education status, occupation, and monthly income (P < .05).
3.2. Multivariate logistic regression results
Significant variables include age, gender, marriage, education, occupation, monthly income, physical activity level, and smoking (Table 2). Overall regression results showed that participants with higher education levels were more likely to be willing to live in care homes. The employed were more likely to choose care home compared to the unemployed (odds ratio (OR) = 1.69, 95% confidence interval (CI): 1.17–2.44); participants with monthly income(≥$564) were more likely to choose care homes (OR = 1.72, 95% CI: 1.03–2.89), and as the level of physical activity decreases, participants are more likely to be willing to choose care homes, controlling for income, education, and occupation. The regression results of urban participants and rural participants showed that the factors affecting urban participants’ choice of care homes are mainly occupation (OR = 1.56, 95% CI: 0.96–2.56), while for the rural population, the most significant factor was education (elementary school and below) (OR = 2.44, 95% CI: 1.01–5.88).
Table 2.
Multivariate logistic regression analysis of willingness to enter elder-care facilities among urban and rural residents.
| Total | City | Rural | |||||||
| Variable | OR | 95% CI | OR | 95% CI | OR | 95% CI | |||
| Age (ref = more than 60 yr old) | 0.91 | 0.59 | 1.39 | 1.02 | 0.56 | 1.84 | 1.01 | 0.51 | 2.02 |
| Gender (ref = female) | 0.95 | 0.69 | 1.29 | 1.03 | 0.69 | 1.55 | 0.75 | 0.46 | 1.24 |
| Marital status (ref = not married) | 0.89 | 0.59 | 1.35 | 1.09 | 0.64 | 1.85 | 0.68 | 0.35 | 1.32 |
| Employed (ref = unemployed) | 1.69∗ | 1.17 | 2.44 | 1.56 | 0.96 | 2.56 | 1.69 | 0.93 | 3.09 |
| Education | Ref | Ref | Ref | ||||||
| Junior high school | 1.49 | 0.91 | 2.44 | 1.13 | 0.55 | 2.32 | 1.68 | 0.82 | 3.45 |
| High school | 1.99∗ | 1.19 | 3.32 | 1.56 | 0.76 | 3.19 | 1.94 | 0.87 | 4.31 |
| Undergraduate or junior college | 1.94∗ | 1.13 | 3.33 | 1.25 | 0.61 | 2.62 | 2.44∗ | 1.01 | 5.88 |
| Monthly income ($) | Ref | Ref | Ref | ||||||
| $141–$564 | 1.32 | 0.87 | 2.02 | 0.96 | 0.45 | 2.05 | 1.01 | 0.56 | 1.82 |
| ≥$564 | 1.72∗ | 1.03 | 2.89 | 1.33 | 0.57 | 3.08 | 1.23 | 0.55 | 2.74 |
| Physical activity level | Ref | Ref | Ref | ||||||
| Medium | 1.21 | 0.91 | 1.95 | 1.13 | 0.77 | 1.65 | 1.28 | 0.77 | 2.14 |
| Low | 1.33 | 0.99 | 1.81 | 1.34 | 0.91 | 1.98 | 1.33 | 0.82 | 2.19 |
| Smoking (ref = no) | 0.99 | 0.69 | 1.42 | 0.77 | 0.48 | 1.24 | 1.46 | 0.82 | 2.62 |
CI = confidence interval, OR = odds ratio. All models adjusted for age, gender, marital status, education, monthly income, physical activity level, smoking.
P < .05.
3.3. Demands for the care homes
We describe reasons why participants would be willing to choose care homes and described elder-care needs in Table 3. The results showed that participants who chose care homes ranked the following reasons as important: good medical care (78.2%), reduced burden for children (68.4%), assistance with daily activities (66.7%), good living atmosphere (53.1%), food and residential conditions (51.9%), low cost (25.7%). Among all of the participants, the health services that they considered to be most urgently needed were medical care (43.8%), physical exercise (35.7%), recreational activities (32.9%), spiritual comfort and psychological support (27.1%), assistance with daily activities (26.4%), participation in social activities (24.7%), emergency assistance (21.2%), senior learning and training (18.2%), and domestic services (9.1%).
Table 3.
Descriptive analysis on the demands for care home.
| Total | City | Rural | ||||
| Cases | % | Cases | % | Cases | % | |
| Why do you choose a institution to support your aged? | ||||||
| Good medical condition | 322 | 78.2 | 222 | 79.6 | 100 | 75.2 |
| Good care of life | 275 | 66.7 | 191 | 68.5 | 84 | 63.2 |
| Good food and shelter conditions | 214 | 51.9 | 158 | 56.6 | 56 | 42.1 |
| Reduce the burden on children | 282 | 68.4 | 194 | 69.5 | 88 | 66.2 |
| Good living atmosphere | 219 | 53.1 | 156 | 55.9 | 63 | 47.4 |
| Low cost | 106 | 25.7 | 76 | 27.2 | 30 | 22.6 |
| What do you think is the most urgently needed pension service project? | ||||||
| Life care | 312 | 26.4 | 168 | 25.1 | 143 | 27.8 |
| Medical insurance | 518 | 43.8 | 282 | 42.1 | 236 | 45.8 |
| Emergency assistance | 250 | 21.2 | 135 | 20.1 | 115 | 22.3 |
| Mental comfort and psychological support | 320 | 27.1 | 168 | 25.1 | 152 | 29.5 |
| Recreational activities | 389 | 32.9 | 227 | 33.9 | 162 | 31.5 |
| Seniors learning training | 215 | 18.2 | 105 | 15.7 | 110 | 21.4 |
| Physical Exercise | 422 | 35.7 | 230 | 34.3 | 192 | 37.3 |
| Participate in social activities | 294 | 24.9 | 167 | 24.9 | 127 | 24.7 |
| Housekeeping | 107 | 9.1 | 64 | 9.6 | 43 | 8.4 |
4. Discussion
Our survey results show that 41.6% of the urban residents and 25.8% of the rural residents are willing to choose institutional elder-care. Given the context of Dujiangyan City, where care homes are clustered in cities[37] and in prior research has shown that elder-care decisions are impacted by concerns about distance,[34] rural residents may be reluctant to live in elder-care facilities because most are far away in urban areas. As China's urbanization continues, and the young and middle-aged rural population migrate to urban settings, the rate of rural aging will be higher than the rate of urban aging,[11] and the current supply and demand of elder-care services in rural and urban areas will continue to be imbalanced. The government should introduce incentives to encourage care homes to be set up in rural areas, as care homes must address the specific needs of rural elderly.
Single-factor chi-square test results show that whether in urban or rural areas, age, education, occupation, and monthly income are all factors that affect the willingness of residents to join care homes. After multi-factor binary logistic regression, factors such as higher education, employees, higher monthly income, and lower physical activity levels are correlated with positive attitude toward care homes, which is consistent with previous research finding.[29,30] However, regression results of urban residents show that employees are more inclined to care homes. This may due to employed people tends to have higher social and economic status than retirees. Though reported in other studies,[5,42] this research found no significant difference in willingness to join care homes based on the presence of non-infectious chronic diseases, which may be due to different disease measurement methods. Though physical activity level is correlated with willingness to enter a care home, the daily activities differ between urban and rural areas. Rural residents are mostly farmers,[41] and have a higher physical-activity level. Our survey results show that the top factors which influence individual's willingness to consider care homes are medical conditions, reducing the burden on their children and good care, and low cost. The top 3 services demanded of care homes are medical care, physical exercise, and recreational activities. Health care and medical care are the priority for care homes, which is consistent with previous research findings.[34,35]
The Chinese government advocates a combined approach to providing medical and social services in cooperation with long-term care institutions. However, it is important to acknowledge that care homes should be heterogeneous in character, quality, and services. Elderly with differing occupations, education levels, and cultural backgrounds have differing expectations and needs. Institutions should provide tiered care services[1] to adequately address the differing needs of individuals, after assessing each individual's health status and requirements for care and services.[34] In Dujiangyan, there is both insufficient supply of care homes given the National goals and increasingly aging population, and insufficient use of existing care homes. The findings of this study agree with prior research which found this coexisting insufficient supply and demand in other regions of China. This may be because the existing care homes are mostly government-designed and determined by government policies rather than the needs of the elderly. Single types of care homes cannot address the multi-faceted needs of those who seek institutional elder-care. In the United States, the government is not directly responsible for the operation of elder services, and rather, funds elder-support through a number of different organizations. The US government, rather than providing elder services themselves, serves as an in-between, helping elderly access resources, and choose an appropriate institution. In Singapore, the United Kingdom, and Germany, the introduction governmental family support benefits encourages children of elderly to provide regular elder-care services.[43] This helps reduce pressure on the public elderly-care services and institutions, while also promoting family unity.
The results of this survey show that urban and rural residents not only differ in their willingness to live in care homes, but also are influenced by different factors in their decision. The government should explore the establishment of a rural elder-care system that not only encourages the establishment of care homes in rural areas, but also develops community care centers and alternative options for partial care models where family members can also participate with care. This may be more in line with the norms of traditional Chinese Confucian culture. Government policies should take into account differences between rural and urban population needs and their different decision factors. The circumstance in China is different from that of western developed countries. For most Chinese cases, the dependent older persons have to depend on their family member because they have no other choices. Government policies should support family caregivers to reduce their burden. Prior research found that while in Western countries, decisions to participate in care homes were often based on health conditions, in China decisions considered family resources and cultural norms and that many elderly people did not in fact require assistance with daily activities.[8,44] We hypothesized that those under the age of 60 have been significantly affected by strict National family planning policies, and as most people have very few children, there is less family support. Additionally, due to China's rapid industrialization and urbanization, this age group is uniquely impacted by these demographic changes and their children are more likely to be urban workers. Due to these demographic shifts, we hypothesized that this population would be more inclined to consider care homes. The chi-square results show that differences are significant between urban and rural residents, but regression results show that age (younger than 60 or older than 60) is not a significant factor. Significant factors included occupation and education level. Given differences in willingness based on education level, the government should consider education campaigns or increasing awareness[45,46] around care homes to eliminate the stigma surrounding care homes.
With the trend of population aging and declining fertility, the issue of elderly care is increasingly a global concern. Some Asian countries, such as Japan, South Korea, and Singapore, are as deeply influenced by Confucian culture as China, and their population is also aging. To address the challenges of aging, it is necessary to simultaneously provide multi-faceted social support and to recognize the differences between urban and rural residents in their understanding of and acceptance of certain institutional and societal supports. By recognizing these differences, policymakers can better establish an elder-care system which will adequately and appropriately serve the diverse aging population in China.
There are several limitations of this study. As respondents in this survey were not currently at care homes, there may be biases in the response, as these responses were hypothetical. As Liu[47] discusses, individuals tend to prefer their current living arrangements, leading to limitations in studies. To further investigate the impact of the family planning policies on the willingness for individuals to enter elder-care facilities, a longitudinal study examining changes in willingness over time could be considered. Additional limitations of the study were that we did not ask those who were not willing to enter a care home the factors which impacted their negative response. Lastly, as this research utilized structured, close-ended surveys, we were not able to assess in-depth qualitative responses from participants to understand the complexity of their decision-making regarding care homes.
5. Conclusion
This study showed that difference in the willingness to care for the elderly between urban and rural areas. These differences may be due to the differing distribution of urban and rural care homes and the differences in education level and economic status between these populations. Despite epidemiological and economic changes between generations, this study found no evidence of difference between the willingness of 40 to 59 years old individuals and individuals over 60 years old, if controlling for occupation, or education and income levels. The decision to enter care homes is more impacted by occupation for urban residents and by education level for rural residents. Overall, healthcare remains the top priority when considering care homes.
Acknowledgments
We thank all the study participants and the school personnel that participated in the study and our collaborators who have contributed to the study.
Author contributions
Conceptualization: Xiaoyang Dong, Li Zhao.
Data curation: Bonnie O Wong.
Funding acquisition: Fengying Zhang, Yi Liu.
Investigation: Xiaoyang Dong, Li Zhao.
Methodology: Bonnie O Wong, Chunsong Yang, Li Zhao.
Supervision: Bonnie O Wong, Chunsong Yang, Fengying Zhang, Fei Xu, Li Zhao, Yi Liu.
Validation: Bonnie O Wong.
Writing – original draft: Xiaoyang Dong.
Writing – review & editing: Xiaoyang Dong.
Correction
When originaly published, Bonnie O. Wong's degree appeared incorrectly as PhD and has since been corrected to MSc.
Footnotes
Abbreviations: CI = confidence interval, OR = odds ratio.
How to cite this article: Dong X, Wong BO, Yang C, Zhang F, Xu F, Zhao L, Liu Y. Factors associated with willingness to enter care homes for the elderly and pre-elderly in west of China. Medicine. 2020;99:47(e23140).
The study is funded in part by National Nature Science Foundation of China (NSFC: 71871147), National Social Science Foundation (NSSFC: 17BRK009), study on the construction of healthy city in Dujiangyan City (Nos: H180516), research on innovation and implementation of health care model in Panzhihua City (2019CDPZH-16). The content of the paper is solely the responsibility of the authors and does not necessarily represent the official views of the funders.
The Ethical Committee of Sichuan University approved the study protocol. Participants were informed about the aim of the survey, the selection criterion of the sample, and the assurance that the information was only used for research. All participants gave written informed consent before inclusion in the study.
The authors have no conflicts of interest to disclose.
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
- [1].Feng Z. Global convergence: aging and long-term care policy challenges in the developing world. J Aging Soc Policy 2019;31:1–7. [DOI] [PubMed] [Google Scholar]
- [2].Chen R, Xu P, Song PP, et al. China has a faster pace than Japan in population aging in next 25 years. Biosci Trends 2019;13:287–91. [DOI] [PubMed] [Google Scholar]
- [3].China NBoSo. Statistical Communique of the People's Republic of China on National Economic and Social Development in 2018 http://www.stats.gov.cn/tjsj/zxfb/201902/t20190228_1651265.html2018. [Google Scholar]
- [4].Wang TX, Han J. The status quo, problems and countermeasures of the cultivation of elderly care service talents in China. Tax Econ 2018;221:55–60. [Google Scholar]
- [5].Gu D, Dupre M, Liu G. Characteristics of the institutionalized and community-residing oldest-old in China. Soc Sci Med 2007;64:871–83. [DOI] [PubMed] [Google Scholar]
- [6].China NBoSo. Statistical Bulletin of National Economic and Social Development. 2017. [Google Scholar]
- [7].Chou KL, Chi I. Reciprocal relationship between social support and depressive symptoms among Chinese elderly. Aging Ment Health 2003;7:224–31. [DOI] [PubMed] [Google Scholar]
- [8].Zhang L, Ding Z, Qiu L. Old age care preferences among chinese middle-aged single-child parents and the related policy implications. J Aging Soc Policy 2019;1–22. [DOI] [PubMed] [Google Scholar]
- [9].Fowler AR, Gao J, Carlson L. Public policy and the changing Chinese family in contemporary China: the past and present as pro-logue for the future. J Macromarketing 2010. [Google Scholar]
- [10].Zeng Y. Options for fertility transition in China. Popul Dev Rev 2007;33:215–46. [Google Scholar]
- [11].Gustafson K, Baofeng H. Elderly care and the one-child policy: concerns, expectations and preparations for elderly life in a rural Chinese township. J Cross Cult Gerontol 2014;29:25–36. [DOI] [PubMed] [Google Scholar]
- [12].Chen F, Liu G. Population aging in China. Bangkok Thailand U 2009;1:157–72. [Google Scholar]
- [13].Lin G, Langen S. Making the transition from family support for the elderly to social support for the elderly. Chin Sociol Anthropol 2002;34:35–48. [Google Scholar]
- [14].Aging CNCo. National aging policy switch preference to aging in place due to doubled aging population 2015. [Google Scholar]
- [15].Ku LJE, Liu LF, Wen MJ. Trends and determinants of informal and formal caregiving in the community for disabled elderly people in Taiwan. Arch Gerontol Geriatr 2013;56:370–6. [DOI] [PubMed] [Google Scholar]
- [16].Zhang H. Who will care for our parents? Changing boundaries of family and public roles in providing care for the aged in urban China. Care Manag J 2007;8:39–46. [DOI] [PubMed] [Google Scholar]
- [17].Zeng Y. Causes and implications of the recent increase in the reported sex ratio at Birth in China. Popul Dev Rev 1993;19:283–302. [Google Scholar]
- [18].Cong Z, Silverstein M. A vignette study of older adults’ preferences for intergenerational transfers in the context of competition between grandparents and grandchildren in rural China. J Gerontol: Series B 2017;74:496–505. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [19].Zhang CC. Children, old-age support and pension in rural China. China Agric Econ Rev 2015;7:405–20. [Google Scholar]
- [20].Liang Y, Lu P. Medical insurance policy organized by Chinese government and the health inequity of the elderly: longitudinal comparison based on effect of New Cooperative Medical Scheme on health of rural elderly in 22 provinces and cities. Int J Equity Health 2014;13:37. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [21].Yuesheng W. An analysis of changes in the Chinese family structure between urban and rural areas: on the basis of the 2010 National Census Data. Soc Sci China 2014;35:100–16. [Google Scholar]
- [22].Zhang Y, Goza FW. Who will care for the elderly in China? J Aging Stud 2006;20:151–64. [Google Scholar]
- [23].Avebury, Chen S. Social Policy of the Economic State and Community Care in Chinese Culture: Aging, Family, Urban Change, and the Socialist Welfare Pluralism. 1996. [Google Scholar]
- [24].Hajek A, König HH. The effect of intra-and intergenerational caregiving on subjective well-being-evidence of a population based longitudinal study among older adults in Germany. PLoS One 2016;11:e0148916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [25].Hajek A, König HH. Informal caregiving and subjective well-being: evidence of a population-based longitudinal study of older adults in Germany. J Am Med Dir Assoc 2016;17:300–5. [DOI] [PubMed] [Google Scholar]
- [26].China Mocaotpsro. Opinions of the State Council on accelerating the development of the pension service industry [October, 23, 2013] http://jnjd.mca.gov.cn/article/zyjd/zcwj/201310/20131000534003.shtml2018. [Google Scholar]
- [27].Fang YY. Experience and reflection on the experience of home-based care for the aged in Wuhan Community. J Changsha Soc Work Coll 2016;23:25–7. [Google Scholar]
- [28].Wang Y. An analysis of the status quo and problems of institutions with the integration of pension service and medical service in Shanghai. Stat Sci Pract 2016;8:31–3. [Google Scholar]
- [29].Gao R, Guo J, Shen Y, et al. Willingness and influential factors of the urban aged to be supported by institutional care: based on the survey of Shandong province. J Community Med 2014;12:9–17. [Google Scholar]
- [30].Yao Z, Wang S. Willingness and influencial factors of the rural aged to be supported by institutional care: based on the survey of 749 rural aged in the east region. J Hunan Agric Univ 2012;13:39–44. [Google Scholar]
- [31].Wang YTF, Fan N, Pan J. Elderly residents’ awareness, attitude and willingness-to-pay for elderly care medical institutions: an empirical analysis based on Chengdu. Chin J Health Policy 2017;10:18–22. [Google Scholar]
- [32].Min JW. Preference for long-term care arrangement and its correlates for older Korean Americans. J Aging Health 2005;17:363–95. [DOI] [PubMed] [Google Scholar]
- [33].Wang ZSX, Su S, Xing Y, et al. The willingness to provide for the aged and its influencing factors in urban young and old people. Chin J Gerontol 2019;39:5101–4. [Google Scholar]
- [34].Huang Z, Liu Q, Meng H, et al. Factors associated with willingness to enter long-term care facilities among older adults in Chengdu, China. PLoS One 2018;13: [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Jiang N, Lou WQ, Lu N. Does social capital influence preferences for aging in place? Evidence from urban China. Aging Ment Health 2016;22:405–11. [DOI] [PubMed] [Google Scholar]
- [36].Wu L. Inequality of pension arrangements among different segments of the labor force in China. J Aging Soc Policy 2013;25:181–96. [DOI] [PubMed] [Google Scholar]
- [37].Government DCPs. Statistical Communique of the National Economic and Social Development of Dujiangyan City. 2016. [Google Scholar]
- [38].Commission DaR. The Ministry of Civil Affairs and the National Development and Reform Commission Printed the Thirteenth Five-year Plan for the Development of Civil Affairs. 2016. [Google Scholar]
- [39].Chen ZJ. A study of the system s of criteria for assessing healthy cities. Health Res (China) 2013;9–13. [Google Scholar]
- [40].Dhalwani NN, O’Donovan G, Zaccardi F, et al. Long terms trends of multimorbidity and association with physical activity in older English population. Int J Behav Nutr Phys Act 2016;13:8. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [41].Zhou P, Hughes AK, Grady SC, et al. Physical activity and chronic diseases among older people in a mid-size city in china: a longitudinal investigation of bipolar effects. BMC Public Health 2018;18:486. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [42].Organization for Economic Co-operation and Development (OECD), Lafortune G, Balestat G. Trends in Severe Disability Among Elderly People: Assessing the Evidence in 12 OECD Countries and the Future Implications. 2007. [Google Scholar]
- [43].Hildebrandt T. The one-child policy, eldercare, and lgb chinese: a social policy explanation for family pressure. J Homosex 2018;66:590–608. [DOI] [PubMed] [Google Scholar]
- [44].Shuqin LXF. Risk factors of living arrangement of urban elderly-analysis of four cities in Jiangsu province. Soc Sci Nanjing 2007;1:98–105. [Google Scholar]
- [45].Zhan H, Liu G, Bai HG. Recent development in Chinese elder homes: are conciliation of traditional culture. Ageing Int 2005;30:167–87. [Google Scholar]
- [46].Zhan HJ. Population aging and long-term care in China. Generations 2013;37:53–8. [Google Scholar]
- [47].Liu TY, Hao XN. Identifying community healthcare supports for the elderly and the factors affecting their aging care model preference: evidence from three districts of Beijing. BMC Health Serv Res 2016;16:626. [DOI] [PMC free article] [PubMed] [Google Scholar]