

This case series describes 2 patients with coronavirus disease 2019 and orbital compartment syndrome, optic disc edema, and retinal hemorrhage in the setting of prolonged prone positioning in the intensive care unit.
Key Points
Question
What ophthalmic abnormalities are present in patients with coronavirus disease 2019 in the intensive care unit requiring prolonged prone-position ventilation?
Findings
In this case series, 2 patients with periorbital edema in the prone position had bilateral findings of optic disc edema and retinal hemorrhages as well as a substantial increase in intraocular pressure.
Meaning
Clinicians should be aware of the possible presence of elevated intraocular pressure from periorbital edema due to direct compression of the eye and orbit, and optic disc edema and retinal hemorrhages, which may be associated with a hypercoagulable state, in patients with coronavirus disease 2019 in prolonged prone position in the intensive care unit.
Abstract
Importance
Critically ill patients with coronavirus disease 2019 (COVID-19) who are unresponsive to maximum optimal ventilator settings may be in a prone position for at least 16 hours per day to improve oxygenation. This extended duration of prone positioning puts patients at risk of developing orbital compartment syndrome if direct pressure to the orbit and the globe occurs and concomitant protection of the eyes is not undertaken.
Objective
To report 2 cases of orbital compartment syndrome, as well as optic disc edema and retinal hemorrhages, in the setting of prolonged prone positioning of patients in the intensive care unit during the COVID-19 pandemic.
Design, Setting, and Participants
The cases took place from April 27, 2020, to May 4, 2020, at a COVID-19 intensive care unit of a tertiary care hospital. Four of 16 patients in the intensive care unit required prolonged prone-position ventilation. A bedside eye examination was performed on 4 selected patients due to the observed presence of substantial periorbital edema.
Main Outcomes and Measures
Intraocular pressures and fundus findings of 4 patients with periorbital edema.
Results
Two of 4 patients who were in the prone position for extended periods of time had bilateral fundoscopic findings of optic disc edema and retinal hemorrhages, possibly consistent with a papillophlebitis. Additionally, both patients had a substantial increase in intraocular pressure of 2- to 3-fold in the prone position compared with the supine position.
Conclusions and Relevance
Prolonged prone positioning of patients with COVID-19 can be associated with elevated intraocular pressure from periorbital edema, direct compression on the eye, and increased orbital venous pressure. Orbital compartment syndrome can be avoided by the use of protective cushioning around the eyes and maintaining the patient’s head position above heart level during prone positioning. Patients with COVID-19 may also develop papillophlebitis with optic disc edema and retinal hemorrhages, which may be associated with a hypercoagulable state caused by COVID-19. These observations suggest awareness for the possible presence of these ophthalmic findings while treating severely ill patients with COVID-19.
Introduction
Many severely ill patients with coronavirus disease 2019 (COVID-19) experience rapid progression of viral pneumonia leading to acute respiratory distress syndrome. Among those with severe acute respiratory distress syndrome unresponsive to maximum optimal ventilator settings, prolonged prone positioning (at least 16 hours per day) is one of the adjunctive strategies to improve oxygenation.1
COVID-19 is associated with a high prevalence of coagulopathy and thromboembolism that may contribute to respiratory deterioration.2 This hypercoagulable state, which occurs more often in patients with elevated fibrinogen and dimerized plasmin fragment D levels, can cause widespread systemic organ damage, raising the question as to if it could affect the eye as well.
It is recognized that patients in the prone position during surgery for extended periods of time are at risk of developing orbital compartment syndrome if the eyes are not protected and direct pressure to the orbit and the globe occurs. These patients may develop elevated intraocular pressure (IOP), periorbital edema, central retinal artery occlusion, central retinal vein occlusion, or ischemic optic neuropathy.3,4
Concern has been raised during the COVID-19 pandemic regarding the potential for developing vision loss with prone positioning in the intensive care unit (ICU) because of the extended duration of prone positioning if concomitant protection of the eyes is not undertaken. We report 2 cases of clinical examination findings most consistent with orbital compartment syndrome and papillophlebitis in patients who underwent prolonged prone positioning in the ICU during the COVID-19 pandemic.
Methods
During one of the author’s (L.S.) redeployment week (April 27, 2020, to May 4, 2020) in the COVID-19 ICU, the ICU team treated 16 patients receiving mechanical ventilation for acute hypoxemic respiratory failure due to COVID-19. Four of the 16 patients required prolonged prone-position ventilation: 18 hours in prone position followed by 6 hours in the supine position cycled every 24 hours. During prone positioning, the patient’s head was rotated 45° laterally to accommodate the endotracheal tube. Thus, one eye was always in a more dependent position than the other. The observation of periorbital edema was made in these patients, which prompted an eye examination. Of the 4 patients who were in the prone position for extended periods of time, we report 2 patients who had bilateral fundoscopic findings most consistent with a presumed COVID-19–associated papillophlebitis. These patients were also found to have substantially elevated IOP in the prone position when compared with the supine position. Both patients had abnormally elevated dimerized plasmin fragment D levels. These 2 patients’ relevant hospital course and ophthalmic findings are briefly described. The Northwell Health institutional review board approved this case series as minimal-risk research using data collected for routine clinical practice and waived the requirement for informed consent.
Results
Patient 1 was a man in his early 50s with no significant medical history. He had a total of 9 sessions of 18-hour ventilation in the prone position at the time the eye examination was performed. His IOP measured by Tono-Pen (Reichert Technologies) was 10 mm Hg in the right eye and 11 mm Hg in the left eye in the supine position and 30 mm Hg in the left eye in the prone position (the right eye was the dependent eye and there was complete contact of the right eyelid with the pillow, preventing safe measurement of IOP in the right eye while prone). Perioribital edema was present around the right eye. On fundus examination (Figure 1), his cup-disc ratio was 0.3 bilaterally. The right optic disc had sharp margins with nerve fiber layer hemorrhages superiorly and inferiorly near the optic disc. The left optic disc had mild inferior margin elevation, with a few intraretinal and subretinal hemorrhages in the mid-periphery.
Figure 1. Case 1: A Man in His Early 50s After 9 Sessions of 18-Hour Prone-Position Ventilation.
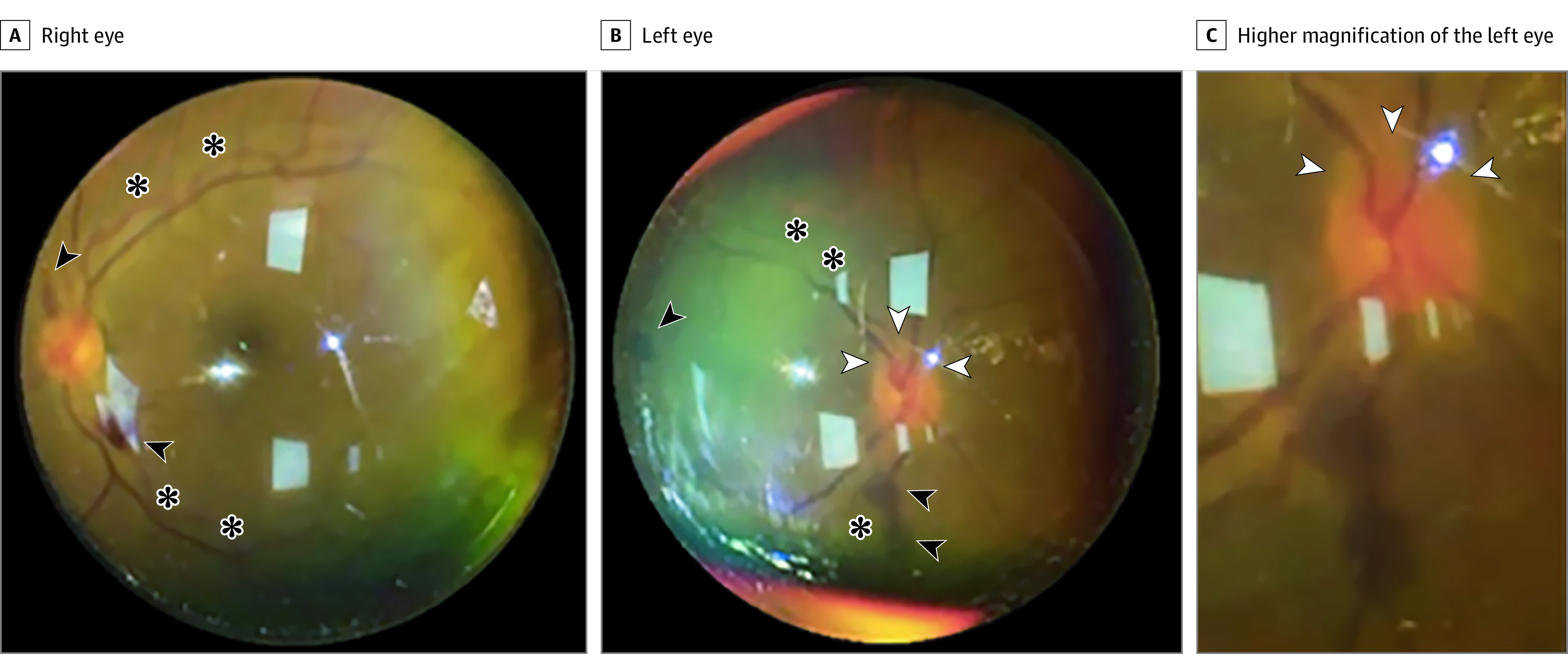
Fundus photograph taken with an iPhone 6S and 20-diopter lens at the intensive care unit bedside. The right eye (A) optic disc had sharp margins with nerve fiber layer hemorrhages (arrowheads) superiorly and inferiorly near the optic disc. There was tortuosity (asterisks) of the retinal veins. The left eye (B) optic disc had mild inferior margin elevation (white arrowheads), with a few intraretinal and subretinal hemorrhages (black arrowheads) in the midperiphery. There was tortuosity (asterisks) of the retinal veins. C, Higher magnification of the left optic disc showed mild inferior margin elevation (arrowheads).
Patient 2 was a man in his mid 40s with a history of non–insulin-dependent type 2 diabetes. He had a total of 4 sessions of 18-hour ventilation in the prone position at the time of initial eye examination. His IOP measured by Tono-Pen (Reichert Technologies) was 10 mm Hg in each eye in the supine position and 26 mm Hg in the right eye and 20 mm Hg in the left eye in the prone position (the right eye was the dependent eye). Periorbital edema was present around the dependent eye. Fundoscopic examination findings (Figure 2) were significant for bilateral inferior optic disc elevation with associated flame-shaped hemorrhages. The cup-disc ratio was 0.3 bilaterally. A few scattered Roth spots were present in the right eye as well. On repeated fundus examination 6 days later, there was progression of retinal hemorrhages near both optic discs (Figure 3). During this interim period, the patient had 2 additional sessions of 18-hour ventilation in the prone position, alternating with 6 hours of supine positioning.
Figure 2. Case 2: A Man in His Mid-40s After 4 Sessions of 18-Hour Prone-Position Ventilation.

Fundus photograph taken with an iPhone 6S and 20-diopter lens at the intensive care unit bedside. The right eye (A) and left eye (B) had inferior optic disc elevation (white arrowheads) with associated flame-shaped hemorrhages (black arrowheads).
Figure 3. Case 2: A Man in His Mid-40s After 6 Sessions of 18-Hour Prone-Position Ventilation.

Fundus photograph taken with an iPhone 6S and 20-diopter lens at the intensive care unit bedside. The right eye (A) had mild elevation of inferior optic disc (white arrowheads) with associated retinal hemorrhages superiorly and inferiorly (black arrowheads). The left eye (B) had sharp margins with flame-shaped hemorrhages (arrowheads) inferiorly near the optic disc and extending along the inferior arcade.
Two other patients in the prone position with periorbital edema in the ICU were also examined. Both had normal fundus examination findings and fewer cycles of alternating prone and supine positioning (1 and 3 prior sessions, respectively) at the time of eye examination.
Discussion
Because all 4 of these patients were deeply sedated, their visual acuity could not be assessed. The ophthalmic findings for the 2 patients described here are most consistent with papillophlebitis, possibly related to the combined effects of increased orbital venous pressure during prolonged prone positioning and COVID-19–associated coagulopathy.5,6,7 However, the design of this study and its findings do not provide strong evidence that the prone position itself is the cause for the fundus findings. Patients who are placed in the prone position for long periods of time are more ill, have more hypoxia, and are in a greater inflammatory state, which could also be contributing to these findings. Therefore, the design of the study does not determine cause and effect but rather provides associations that would require further evaluation or randomized clinical trial designs to provide strong evidence supporting cause and effect.
Both patients had periorbital edema and a substantial increase in IOP of 2- to 3-fold in prone positioning compared with the pressure in the supine position suggestive of an orbital compartment syndrome. Amorim Correa and Acioly8 reported 1 case and reviewed 3 other cases of orbital compartment syndrome in patients undergoing lumbar spinal surgery in the prone position for extended periods of time, in which periorbital edema and a tense orbit were present.
At the time of this writing, the mortality rate for critically ill patients with COVID-19 who receive mechanical ventilation remains extremely high at 76.4% for patients aged 18 to 65 years and 97.2% for patients older than 65 years.9 Thus, the incidence of vision loss caused by prone positioning for all patients will be difficult to determine. However, for ICU patients who undergo prolonged prone-positioning ventilation, it would be devastating to wake up and experience permanent vision loss that was caused by orbital compression that could have been prevented.
Limitations
The selection of patients for this study was limited to those patients in the ICU during 1 physician’s (L.S.) deployment. The fundus findings described in this study may not be representative of all possible fundus abnormalities seen in patients with COVID-19.
Conclusions
The current COVID-19 crisis is still unfolding. As we continue forward and improve treatment protocols for COVID-19, we must also focus attention on modifiable risk factors to ensure a safe visual acuity outcome for patients. We recommend (1) raising awareness of the potential risk of vision loss following prolonged prone positioning, (2) encouraging the use of protective cushioning of the eyes to avoid mechanical pressure on the globe during prone positioning, (3) if appropriate, maintaining the patient’s head position above heart level, and (4) consideration of performing a fundus examination to evaluate for the presence of optic disc or retinal abnormalities in prone-positioned patients in the ICU.
References
- 1.Guérin C, Reignier J, Richard JC, et al. ; PROSEVA Study Group . Prone positioning in severe acute respiratory distress syndrome. N Engl J Med. 2013;368(23):2159-2168. doi: 10.1056/NEJMoa1214103 [DOI] [PubMed] [Google Scholar]
- 2.Iba T, Levy JH, Levi M, Connors JM, Thachil J. Coagulopathy of coronavirus disease 2019. Crit Care Med. 2020;48(9):1358-1364. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Epstein NE. Perioperative visual loss following prone spinal surgery: a review. Surg Neurol Int. 2016;7(suppl 13):S347-S360. doi: 10.4103/2152-7806.182550 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Nickels TJ, Manlapaz MR, Farag E. Perioperative visual loss after spine surgery. World J Orthop. 2014;5(2):100-106. doi: 10.5312/wjo.v5.i2.100 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Insausti-García A, Reche-Sainz JA, Ruiz-Arranz C, Vázquez ÁL, Ferro-Osuna M. Papillophlebitis in a COVID-19 patient: inflammation and hypercoagulable state. Eur J Ophthalmol. 2020;1120672120947591. doi: 10.1177/1120672120947591 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Marinho PM, Marcos AAA, Romano AC, Nascimento H, Belfort R Jr. Retinal findings in patients with COVID-19. Lancet. 2020;395(10237):1610. doi: 10.1016/S0140-6736(20)31014-X [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Landecho MF, Yuste JR, Gandara E, et al. COVID-19 retinal microangiopathy as an in vivo biomarker of systemic vascular disease? J Intern Med. Published online July 30, 2020. doi: 10.1111/joim.13156 [DOI] [PubMed] [Google Scholar]
- 8.Amorim Correa JL, Acioly MA. The enigma of orbital compartment syndrome after lumbar spine surgery in the prone position: case report and literature review. World Neurosurg. 2018;110:309-314. doi: 10.1016/j.wneu.2017.11.111 [DOI] [PubMed] [Google Scholar]
- 9.Richardson S, Hirsch JS, Narasimhan M, et al. ; the Northwell COVID-19 Research Consortium . Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052-2059. doi: 10.1001/jama.2020.6775 [DOI] [PMC free article] [PubMed] [Google Scholar]