

Abstract
Background
ADHD poses risk for problematic alcohol use through adulthood. Perceived peer alcohol use, one of the strongest correlates of individuals’ own alcohol use, is especially salient for adolescents with ADHD. The extent to which this risk extends into young adulthood is unknown, as well as how change in these constructs is associated throughout young adulthood.
Methods
In the Pittsburgh ADHD Longitudinal Study, 358 individuals with childhood-diagnosed ADHD and 239 without were prospectively followed from age 18–29. Piecewise, bivariate longitudinal growth modeling was used to examine change in both peer alcohol use and individuals’ heavy drinking (binge drinking frequency), their between-person associations, and differences by ADHD group. The addition of structured residuals probed within-person year-to-year change in peer and personal alcohol use and their prospective associations.
Results
Perceived peer alcohol use and individuals’ heavy drinking frequencies changed together over time concurrently – from ages 18–21 (piece 1) and 21–29 (piece 2). Prospectively, individuals who increased the most in heavy drinking from ages 18–21 reported more friends using alcohol at age 29, regardless of ADHD history. Within-person increases in personal alcohol use likewise predicted increased perceived peer use the subsequent year within each age group (piece), regardless of ADHD history. However, while decreasing perceived peer use from ages 21–29 was related to more frequent heavy drinking at age 29 for those without ADHD, increasing perceived peer use from ages 18–21 predicted more frequent heavy drinking at age 29 for those with ADHD.
Conclusions
Young adult heavy drinking changes in tandem with perceived peer alcohol use across individuals and predicts selection of alcohol-using peers from year to year within individuals, further into adulthood than previously documented. Findings suggest the centrality of relationships with alcohol-consuming friends in relation to one’s heavy drinking, especially for young adults with ADHD histories, through the twenties.
Keywords: ADHD, alcohol, young adulthood, peers, longitudinal
Introduction
Young adulthood (i.e., ages 18–25), when heavy alcohol consumption peaks (i.e., 5 or more drinks in a single episode; Center for Behavioral Health Statistics and Quality), is a high-risk developmental period. Childhood attention-deficit/hyperactivity disorder (ADHD) confers heightened risk for alcohol outcomes in young adulthood either directly (Charach et al., 2011; Lee, Humphreys, Flory, Liu, & Glass, 2011) or indirectly via early substance exposure in adolescence (Howard et al., in press; Molina et al., 2018). Perceived peer alcohol use, a strong predictor of problematic alcohol use in young adulthood (Andrews, Tildesley, Hops, & Li, 2002; Haller, Handley, Chassin, & Bountress, 2000; Overbeek et al., 2011), may be a contributing factor. Peers are potent socializing agents in young adulthood as individuals seek autonomy from their parents, driving young people to align their drinking behaviors with peers from whom they desire acceptance and with whom they spend most of their time (Overbeek et al., 2011). Notably, regardless of how much peers actually drink, young adults’ perceptions of alcohol use among their peers predict their own alcohol consumption (Schulte, Monreal, Kia-Keating, & Brown, 2010). Given that young people with ADHD are more likely than their typically developing peers to be impulsive, to have social difficulties, and to be prone to poor decision-making in high-risk settings (Molina et al., 2012), they may be especially vulnerable to the influence of alcohol-using peers on their own heavy drinking (Merrill et al., 2018). In addition to yielding to peer influences (socialization), young adults may also curate their friend groups by drifting toward peers who engage in similar drinking habits to their own (selection; Becker, Marceau, Hernandez, & Spirito, 2019; Curran, Stice, & Chassin, 1997). Assortative peer selection may likewise be accentuated in individuals with ADHD who might compensate for lacking social skills with involvement in risky drinking to seek out, attract, and select friends who value such behavior (Marshal et al, 2003).
Indeed, several findings from prospective longitudinal studies indicate that the association between perceived peer substance use and individuals’ own alcohol use (“personal use”) is stronger for adolescents with, versus without, ADHD histories (Belendiuk et al., 2016; Marshal et al., 2003). For instance, Belendiuk and colleagues (2016) found in the Pittsburgh ADHD Longitudinal Study that growth in perceived friend alcohol use across adolescence (age 14–17) was associated with growth in personal alcohol use frequency during the same period – but only for those with ADHD. Moreover, personal alcohol use frequency at age 14 was more strongly associated with growth in friend alcohol use for those with ADHD than for those without, though relations were significant for both groups. Thus, at least in adolescence, individuals with ADHD are especially likely to use alcohol when they perceive that their friends are using, and vice versa. However, the extent to which heightened ADHD-related risk for peer influence continues through young adulthood, when access to alcohol widens, is unknown and could have important implications for prevention and treatment (i.e., whether targeting socially-mediated risk is especially critical for adults with ADHD).
Research examining the role of peers in young adults’ alcohol use in the context of ADHD is minimal. The results of one cross-sectional study among college students demonstrated that perceived peer substance use mediated the link between ADHD symptoms and alcohol use (Van Eck et al., 2014). However, only 9% of participants reported clinically significant symptoms, which precludes generalizations to clinical ADHD populations. Moreover, the mean age was 20, but developmentally typical alcohol use does not decline until the late 20s. Hence, research is needed to determine whether peer alcohol use may perpetuate ADHD-related risk further into adulthood, beyond the peak period of normative use (age 18–25; Center for Behavioral Health Statistics and Quality, 2015; Derefinko et al., 2016). Further, like most research on peer alcohol use (Borsari & Carey, 2003; 2006; Mason et al., 2014; Overbeek et al., 2011; White et al., 2006), the Van Eck et al. sample comprised only college students, which underrepresents individuals with ADHD who are less likely than their peers to attend college (Hechtman et al., 2016). College provides unique social contexts in which perceived peer alcohol use may operate differently from other environments, necessitating expansion to broader populations of young adults. Additionally, longitudinal studies are needed that can test the relation between perceived peer and personal alcohol use as they unfold throughout young adulthood to identify whether perceived peer alcohol use is associated with the development of problematic personal alcohol use as individuals age beyond the period of greatest risk for heavy drinking. Understanding these associations among individuals with ADHD is critical to identify appropriate interventions for this vulnerable group.
The Current Study
The Pittsburgh ADHD Longitudinal Study (PALS) was designed to study the course and predictors of alcohol outcomes among individuals with well-characterized histories of childhood ADHD. As such, it provides the unique opportunity to longitudinally examine the relations between changes in perceived peer alcohol use and personal alcohol use among young adults aged 18–29 with and without ADHD histories. We hypothesized that: (1) changes in perceived peer alcohol use across early adulthood would be associated with changes in heavy drinking frequency for individuals with and without childhood ADHD; and (2) this association would be stronger for individuals with versus without childhood ADHD. As the first study to examine associations between change over time in peer and personal alcohol use as a function of ADHD through the end of the 20s, this study aimed to elucidate whether and how the peer context may track with heavy drinking beyond the period of peak alcohol use for this vulnerable group.
Materials and Methods
Participants
Participants in the PALS study were diagnosed with ADHD (DSM-III-R or DSM-IV criteria) and participated in a summer treatment program in childhood between 1987 and 1996 (Pelham et al., 2005). Average age at diagnostic evaluation was 9.40 years old (SD=2.27, range=5.0–16.92, 90% were ages 5–12).
Diagnostic information was collected using standardized parent and teacher symptom rating scales (Pelham et al., 1992) and a standardized semi-structured diagnostic interview administered to parents by a Ph.D-level clinician. Two Ph.D.-level clinicians independently reviewed all ratings and interviews to confirm diagnoses; when disagreement occurred, a third clinician reviewed the file and the majority decision was used. Exclusion criteria included full-scale IQ<80, history of seizures or other neurological problems, and/or history of pervasive developmental disorder, schizophrenia, or other psychotic or significantly impairing mental disorders.
Of those eligible for enrollment into PALS (n=516), 70.5% participated (n=364; Mage=17.75, SDage=3.39). Enrollment occurred an average of 8.35 (SD=2.79) years after childhood diagnosis. Enrolled PALS participants differed from non-enrolled individuals on only one out of 14 childhood demographic and diagnostic variables: parent/teacher ratings of conduct disorder symptoms were lower (t=3.09, p<.01) for participants (M=2.13; SD=1.93) versus nonparticipants (M=2.74; SD=2.19; Cohen’s d=.30).
Participants without ADHD were recruited from the greater Pittsburgh area from several sources (e.g., pediatric practices, university hospital staff newsletter, schools). A telephone screening with parents gathered basic demographics, history of diagnosis and treatment for ADHD and other behavior problems, presence of exclusionary criteria for the ADHD participants, and a checklist of ADHD symptoms. Young adults (age 18+) also provided self-report of the same information. In addition to the exclusion criteria listed for the ADHD sample, individuals who met DSM-III-R criteria for ADHD (presence of 8 or more symptoms reported by either the parent or young adult), currently or historically, were excluded from the non-ADHD sample. Subthreshold ADHD symptoms and other psychiatric disorders were not exclusions. By design, the ADHD and non-ADHD samples were demographically similar (Molina et al., 2007).
Of the 604 PALS participants, the subsample for these analyses (N=597) consisted of participants with any data between the ages of 18–29 (n=358 with and n=239 without ADHD histories). Within this sample, 583 (97.7%) participants contributed data in at least two time points between ages 18 to 29, 572 (95.9%) in at least three time points, and 560 (93.9%) in at least four time points. Most (89%) participants were male, given the higher incidence of ADHD in male than female children, and 82% identified as White (not Hispanic). At age 29, 15% of the ADHD and 27% of the non-ADHD groups were married; 3% vs. 1.5% of these groups, respectively, were divorced. The proportion of participants living in their parents’/guardians’ homes was 19% in the ADHD and 6% in the non-ADHD groups. Forty-two percent of the ADHD and 57% of the non-ADHD groups were working full-time, 8% and 6% were working part-time, and 18% and 9% were unemployed, respectively. Eighteen percent of the ADHD group and 62% of the non-ADHD group had a college degree by age 29. These group differences, as well as persistence of symptoms consistent with DSM-5 diagnosis for 23% of the sample, have been extensively reported elsewhere (e.g., Altszuler et al., 2016; Pelham III et al., 2020).
Procedure
Initial enrollment occurred from 1999–2003. Annual interviews occurred until 2008; assessments have since been age-based (annually to 23, and then at approximately ages 25, 27, and 29, with some assessments at ages 24, 26, and 28 depending on precisely when participants completed their age-based assessments). Interviews were conducted by post-baccalaureate research staff following informed consent. Participants were assured confidentiality of all disclosed material except in cases of impending danger to self or others (reinforced with a DHHS Certificate of Confidentiality).
Measures
Perceived peer alcohol use.
Two items were adapted from the Monitoring the Future Study (Johnston, O’Malley, & Bachman, 1988). Participants reported how many of their friends they estimated used alcohol (1) occasionally and (2) regularly. Response options ranged on a 5-point scale from 1 (none) to 6 (all). Correlations between regular and occasional alcohol use ranged from .63 to .77 from age 18 to 29. Given their high correlations and in line with previous research (Belendiuk et al., 2016), responses on the two items were averaged to create a composite peer alcohol use scale. From ages 18 to 29, means ranged from 3.08 (where 3=some) to 3.75 (where 4=many; SDs=1.30–1.46.
Heavy alcohol use.
Past-year frequency of binge drinking was assessed with one item (“In the past 12 months, how often did you drink 5 or more drinks when you were drinking?”) on a 12-point scale ranging from 0 (not at all) to 11 (several times a day). From age 18 to 29, means ranged from 1.77 (where 2=4–7 times) to 3.31 (where 3=8–11 times; SDs=2.39–2.87).
Covariates.
Baseline demographic covariates (measured at study entry) included gender, race, the highest educational level achieved by the participant’s parents at baseline (mean-centered), and whether or not the participant met diagnostic criteria for Conduct Disorder (CD) or Oppositional Defiant Disorder (ODD) at baseline (per parent and teacher report on standardized rating scales and structured parent interview). Additionally, we controlled for the proportion of time that participants were living at home with parents/caregivers and the proportion of time during which they were attending college/university from ages 18–29, given the ADHD group differences we have observed in these variables (Altszuler et al., 2016).
Analytic Plan
We first estimated unconditional growth trajectories separately for perceived peer alcohol use and individuals’ own heavy drinking frequency between ages 18–29 in a structural equation modeling framework. Age was centered at 29, the “end point” of the age range for these analyses, so that the intercepts reflected values of perceived peer alcohol use and heavy drinking frequency at age 29. A visual inspection of the age-specific means of these variables revealed increases from ages 18–21 and decreases thereafter. We compared fit statistics of linear, quadratic, and piecewise growth curves to select the optimal functional form for each trajectory. A piecewise linear function with an inflection point at age 21 (Flora, 2008) was selected for both perceived peer alcohol use and individuals’ heavy drinking frequency (Figure 1), which separately modeled rates of change during the transition from adolescence to adulthood, from ages 18–21 (slope 1), and across young adulthood, from ages 21–29 (slope 2). The unconditional growth trajectory models fit the data well for both perceived peer alcohol use (χ2(66)=1576.79, p<.001; CFI1=.98; TLI=.98; RMSEA=.03; SRMR=.06) and individuals’ own heavy drinking frequency (χ2(66)=2009.77, p<.001; CFI=.95; TLI=.95; RMSEA=.05; SRMR=.06).
Figure 1.

Unconditional latent growth trajectories and observed mean growth in (a) perceived peer alcohol use and (b) individuals’ own heavy drinking frequency.
Next, we conducted a multiple-group bivariate (“parallel process”) latent growth curve analysis in which we covaried all slope and intercept factors to test their between-person associations, adjusting for covariates (Figure 2). To test ADHD/non-ADHD group differences, we began by testing a model in which all covariances freely varied between groups. We then sequentially constrained each model parameter to be equal between groups starting with each growth factor mean individually, followed by their variances, then each individual covariance between growth factors, followed by paths between each growth factor and all covariates as a block. Model comparisons yielding significant chi-square difference tests suggested a decrement in model fit and a significant group difference in the parameter; in such cases, the given parameter equality constraint was freed before testing the next parameter until all parameter constraints had been tested and a final model was reached. Analyses were conducted in Mplus (Version 8.1; Muthén & Muthén, 1998–2017) using full information maximum likelihood estimation.
Figure 2.
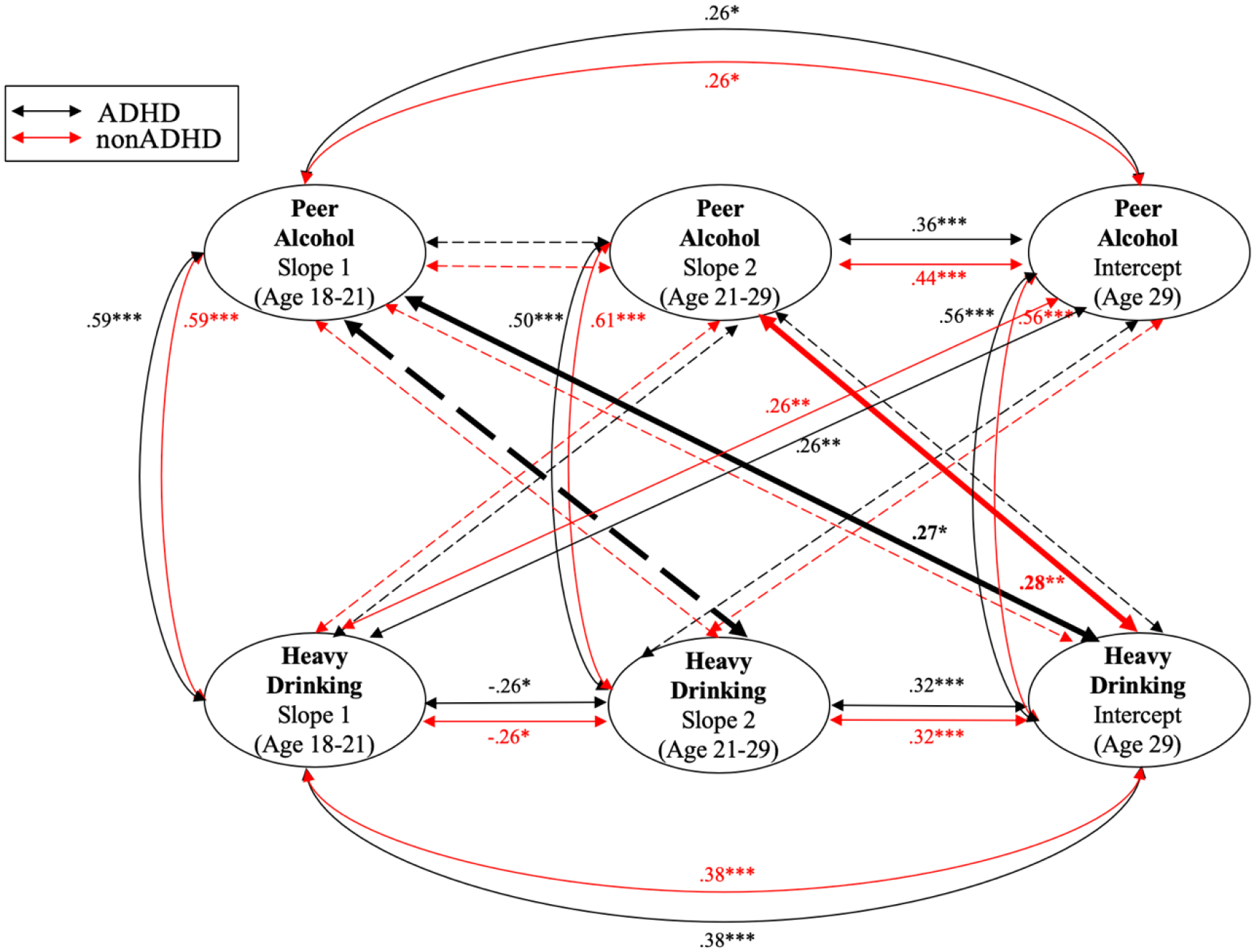
Multiple-group bivariate latent growth curve model results. Note. Standardized coefficients are displayed. Black = ADHD group, red = non-ADHD group. Solid lines = significant association, dashed lines = nonsignificant association (for which coefficients are not displayed for simplicity). Bolded lines = significant group difference, with a stronger relation for the group whose color is displayed in the bolded line. Covariates not displayed here include gender, race, parental education at baseline, Conduct Disorder or Oppositional Defiant Disorder diagnosis at baseline, proportion of time between age 18–29 during which participants were living at home with parents, and proportion of time when participants were in college/university.
A post-hoc within-subjects analysis, testing prospective associations between the time-specific residuals of the latent growth curves, is described below.
Results
Growth in Perceived Peer Alcohol Use and Heavy Drinking Frequency
The final multiple-group bivariate latent growth curve model, shown in Figure 2, fit the data adequately (χ2(752) = 1371.150, p<.001; CFI=.91; TLI=.90; RMSEA=.05; SRMR=.08). Perceived peer alcohol use levels increased, on average, between ages 18–21 (βADHD=.61, p<.05; βnon-ADHD=.62, p<.05)2, and significant variance in slope 1 indicated variability across individual trajectories. From ages 21 to 29 (slope 2), perceived peer alcohol use significantly declined on average (βADHD=−.48, p<.01; βnon-ADHD=−.59, p<.01), but again, significant variance reflected individual variability. Likewise, individuals’ own trajectories of heavy drinking frequency significantly increased from ages 18 to 21 (βADHD=.76, p<.01; βnon-ADHD=.81, p<.01) and significantly declined from ages 21 to 29, on average (βADHD=−.39, p<.05; βnon-ADHD=−.39, p<.05).
Several growth factors were significantly associated with covariates. In both the ADHD and non-ADHD groups, the perceived peer alcohol use intercept and the heavy drinking intercept were significantly related to gender (peer use: βADHD/non-ADHD= −.12, ps<.05; heavy drinking: βADHD/non-ADHD= −.18, ps<.001), race (peer use: βADHD/non-ADHD= −.13 – −.14, ps<.05; heavy drinking: βADHD/non-ADHD= −.20 – −.21, ps<.001), childhood CD/ODD diagnosis (peer use: βADHD/non-ADHD= −.02 – −.12, ps<.05; heavy drinking: βADHD/non-ADHD= −.02 – −.12, ps<.01), time living at home with parents/guardians (peer use: βADHD/non-ADHD= −.20 – −.23, ps<.001; heavy drinking: βADHD/non-ADHD= −.13 – −.15, ps<.01), and – for heavy drinking (but not peer use) intercept– college/university attendance (βADHD/non-ADHD= −.15 – −.18, ps<.01). Specifically, perceived peer alcohol use and individuals’ own heavy drinking frequency at age 29 were higher among men, White participants, participants without a childhood CD or ODD diagnosis, participants who spent a smaller proportion of time between ages 18–29 living with parents/guardians, and – for heavy drinking only – those who spent a smaller proportion of time between ages 18–29 in college/university. Participants without childhood CD/ODD also tended to experience less of an increase in perceived peer alcohol use from ages 18–21 (slope 1; βADHD/non-ADHD= −.03 – −.17, p<.01).
Associations Between Growth in Perceived Peer Alcohol Use and Heavy Drinking Frequency (Full Sample)
A number of cross-variable associations were statistically significant. All concurrent associations between growth in perceived peer and personal alcohol use were significant, positive, and strong, indicating that changes in perceived peer alcohol use track with simultaneous changes in heavy drinking frequency. Specifically, Figure 2 shows that increases in perceived peer alcohol use from ages 18 to 21 were associated with increases in heavy drinking frequency during the same developmental period. Likewise, decreases in perceived peer alcohol use from ages 21 to 29 were correlated with similar decreases in heavy drinking frequency during the same period. Moreover, perceived peer alcohol use at age 29 was significantly and positively correlated with age 29 heavy drinking frequency. All of these associations between growth in peer and personal alcohol use were strong in magnitude, ranging from .50 to .61. One prospective association was statistically significant for the entire sample: Increases in heavy drinking frequency from ages 18 to 21 (slope 1) were associated with higher levels of perceived peer alcohol use at age 29 (intercept).
ADHD vs Non-ADHD Group Differences
Figure 2 highlights several of the growth model parameters that significantly differed between the ADHD groups. Although heavy drinking frequency significantly increased from ages 18 to 21 (slope 1) for both groups, the slope was significantly steeper for those without ADHD histories (Δχ2=4.71, p<.05), indicating that individuals without ADHD histories accelerated in their rate of heavy drinking more quickly during this transition from adolescence to young adulthood. Additionally, the intercept at age 29 for perceived peer alcohol use was higher for the non-ADHD group (β=4.12, p<.001) than the ADHD group (β=3.78, p<.001; Δχ2=5.73, p<.05). Thus, at age 29, individuals without ADHD histories reported that more of their friends used alcohol, on average, than did individuals with ADHD histories. Lastly, one variance significantly differed by group (Δχ2=5.60, p<.05), such that there was more variability in how much individuals decreased (or increased) from ages 21 to 29 in the number of peers using alcohol among individuals with ADHD histories compared to those without (not shown in Figure 2).
Pertinent to our second hypothesis, several prospective associations between growth in perceived peer alcohol use and growth in personal alcohol use differed by ADHD history. First, perceived peer alcohol use slope 1 (ages 18 to 21) was positively associated with individuals’ own heavy drinking frequencies at age 29 – for those with ADHD histories only (Δχ2=4.09, p<.05). Individuals in the ADHD group who reported increasingly more peers using alcohol from ages 18 to 21 tended to experience more frequent heavy drinking later in adulthood, at age 29. However, for those without ADHD, whether or not perceived peer alcohol use increased from ages 18 to 21 was unrelated to their eventual heavy drinking at age 29.
Second, perceived peer alcohol use slope 2 (ages 21 to 29) was significantly and positively associated with individuals’ own heavy drinking frequencies at age 29 – for those without ADHD histories only (Δχ2=6.81, p<.01). Since perceived peer alcohol use declined, on average, from ages 21 to 29, this association indicates that individuals without ADHD who declined more quickly in the number of their peers using alcohol from ages 21 to 29 endorsed the lowest frequencies of heavy drinking at age 29. In contrast, declining perceived peer alcohol use from ages 21 to 29 was unrelated to age 29 heavy drinking for those with ADHD histories.
Lastly, although there was not a significant association overall between perceived peer alcohol use slope 1 (ages 18 to 21) and heavy drinking frequency slope 2 (ages 21 to 29), there was a significant group difference: the association was stronger and positive among individuals with ADHD histories compared to those without, for whom it was negative (Δχ2=4.22, p<.05). Thus, those with ADHD who perceived an increasing number of alcohol-using peers from ages 18 to 21 tended to decrease less than those without ADHD in their own heavy drinking frequency from ages 21 to 29 (βADHD=.22, p=.13; βnon-ADHD= −.08, p=.54.
Post-Hoc Within-Person Analyses
We conducted additional modeling to explicitly disaggregate the within- from the between-person components of change over time in peer and personal alcohol use and to estimate their unique cross-lagged associations throughout the age span examined here. Specifically, we extended the growth analyses using a latent curve model with structured residuals (LCM-SR; Curran et al., 2014), in which we estimated individuals’ age-specific deviations in perceived peer and personal alcohol use (the residuals) from their average trajectories over time (the growth curves). We regressed each residual value on the prior age’s residual value for the same construct, and we constrained these to be equal within piece 1 (ages 18–21) and within piece 2 (ages 21–29). Importantly, we also simultaneously regressed each residual on the prior age’s residual for the counterpart construct (the cross-lagged associations), and we likewise constrained these to be equal within each piece. Finally, we tested the interaction between each cross-lagged association and ADHD (a full multiple-group LCM-SR was overly complex for the data and failed to converge).
Accounting for the stability of perceived peer and personal alcohol use, within-person increases in individuals’ own alcohol use above their average tendencies predicted increases in their number of alcohol-using peers the following year from ages 18 to 21 (B=.06, p<.05) and from ages 21 to 29 (B=.04, p<.05).3 However, the cross-lagged associations between perceived peer use and individuals’ alcohol use the next year were not statistically significant. None of the cross-lagged associations significantly differed by ADHD history.
Discussion
In this longitudinal study of young adults rigorously diagnosed with ADHD in childhood and a non-ADHD comparison group, we found that perceived peer alcohol use tracked with individuals’ own heavy drinking frequency across young adulthood. In particular, after a period of increasing perceived peer and personal alcohol use from ages 18–21, developmentally normative declines occurred through the late 20s in both groups. Change (slopes) in these variables were associated over time, and post-hoc analyses suggested selection effects, such that young adults choose peers to support their drinking behavior. Moreover, we found that several longitudinal associations between perceived peer and personal alcohol use differed by ADHD history, suggesting potentially different processes involved in heavy drinking in this vulnerable population.
Perceived Peer and Individual Alcohol Use Are Correlated Throughout Young Adulthood
A wealth of literature documents robust links between perceived peer and individual alcohol use in adolescence and in the transition to adulthood (e.g., Andrews et al., 2002; Curran et al., 1997; Patrick & Schulenberg, 2010), but not at older ages. As expected, growth in peer alcohol use was strongly related to simultaneous growth in individuals’ own heavy drinking frequencies with correlations as high as .61. Thus, from ages 18–21, those who reported increases in perceived peer use also increased in their own heavy drinking frequencies. Likewise, those who experienced greater stability (i.e., less change) in their perceived number of alcohol-using peers across this period experienced less change (i.e., less increase) in their own heavy drinking frequencies. Following the peak period of use, those reporting greater declines in perceived peer alcohol use from age 21 to 29 reported greater declines in their own use as well, culminating in correlated levels of peer and individuals’ alcohol use at age 29.
This set of findings extends prior findings that perceived peer and personal alcohol use track together over time (Chassin, Pitts, & Prost, 2002) by revealing that this association continues throughout young adulthood (to age 29) – later than previously examined (Chassin et al., 2002; Kennedy et al., 2019; Neighbors et al., 2007; Van Eck et al., 2014; White et al., 2006). This novel finding suggests that even as aging young adults shift their social efforts toward romantic partners and spouses, peers remain a strong presence in relation to heavy drinking. Perhaps because young adults are delaying marriage compared to previous generations (Kreider & Ellis, 2011), their peers maintain a salient role in individuals’ drinking behavior – whether via socialization by peers into heavy drinking, selection of peers who engage in similar drinking habits to one’s own, or a combination of both (Becker et al., 2019). Further, whereas most peer alcohol use research has been conducted in college populations, this sample included an alcohol risk group (ADHD) unlikely to complete college (Altszuler et al., 5% vs. 33% for non-ADHD). As such, a tight connection between perceived peer and personal alcohol use in young adulthood is not limited to college students. Peer-focused intervention and prevention efforts should reach beyond the college campus into the larger community. It is also noteworthy that this study focused on heavy drinking – a particularly risky behavior that is prognostic of long-term alcohol problems (Chassin et al., 2002) – and expands the peer use literature beyond simple drinking frequency or quantity (e.g., Belendiuk et al., 2016; Neighbors et al., 2007; Overbeek et al., 2011; Van Eck et al., 2014).
Faster growth in heavy drinking frequency from ages 18 to 21 was longitudinally associated with a greater perceived number of peers using alcohol at age 29. Reciprocally, faster growth in peer alcohol use from ages 18 to 21 was associated with more frequent heavy drinking at age 29 (though only among those with ADHD histories, as described below). Thus, escalating patterns of drinking – both one’s own and one’s perception of peers’ – during the transition to adulthood may serve as a warning sign for continued peer and heavy drinking. These long-term reciprocal associations could reflect a combination of peer selection and socialization effects. However, our post-hoc analyses testing within-person, prospective year-to-year relations supported only peer selection effects. Specifically, individuals whose heavy drinking at a given age exceeded their typical level reported more alcohol-using peers the following year, above and beyond both the general tendency for these constructs to change together across people as well as individuals’ year-to-year stability in perceived peer and personal alcohol use. This within-person pattern was observed throughout young adulthood, from ages 18–29, suggesting that young adults continue to seek out peers with similar drinking patterns to their own throughout the 20s, beyond the peak period of alcohol use.
In contrast, the reciprocal within-person prospective relations from perceived peer alcohol use to subsequent personal alcohol use were not significant. Thus, peer socialization into drinking from one year to the next within a given person was not supported in the current data. This may suggest that the process of socialization in young adulthood results from the build-up of individuals’ peer contexts over time, and potentially in adolescence, rather than time-limited, age-specific alterations from their overall young adulthood trajectory. These findings substantively sharpen our understanding of selection and socialization processes in young adulthood: complementing prior evidence of both selection and socialization (Becker et al., 2019; Curran et al., 1997), the current study extends further into young adulthood than prior studies. It is the first to disaggregate between- from within-person associations, and indicates the importance of both average-level, long-term trends in peer and personal alcohol use, as well as individuals’ year-to-year aberrations from these trajectories as they expand their alcohol-using social circles following increases in their own drinking.
ADHD-Related Risk for Worsening Heavy Drinking Across Young Adulthood
We further sought to test whether growth in perceived peer and individual alcohol use were more strongly associated across young adulthood for those with versus without ADHD histories. Although group differences were not found in concurrent trajectory associations or the within-person, prospective associations among age-specific deviations from these trajectories, the pattern of ADHD group differences in the longitudinal trajectory associations appears to reflect long-term risk among those with ADHD histories. Specifically, in line with our second hypothesis, for participants with ADHD only, individuals with more steeply increasing trajectories of peer use during the transition to young adulthood (ages 18 to 21) reported higher ultimate levels of heavy drinking at age 29. This finding extends those of Belendiuk and colleagues (2016) by showing that the ADHD-specific linkage between growth in friends’ and individuals’ own alcohol use across adolescence continues to the peak period of use at age 21 and suggests longer-term associations through young adulthood. Importantly, this finding goes beyond a two-timepoint longitudinal analysis by highlighting that an increase over time in perceived peer alcohol use in this emerging adulthood period, but not absolute level at any given age as revealed by the within-person results, may portend heightened heavy drinking later in adulthood. This peer-related signal of risk for later heavy drinking therefore appears to reflect a developmental process that unfolds over time (between ages 18–21), suggesting that intervening at any point prior to or during this process may have the potential to interrupt this trajectory. One possible explanation for this finding is that accruing increasingly more alcohol-consuming friends during this key developmental transition shapes individuals’ own drinking patterns through especially salient peer socialization for those with ADHD. In this case, efficacious alcohol interventions that correct young adults’ overestimations of how much their peers are drinking might be indicated (Dotson, Dunn, & Bowers, 2015; Schulte et al., 2010). These interventions may shift perceived social norms and choice of peers, and thereby decrease personal drinking levels – important given our finding of especially rapid escalating drinking in the ADHD group from ages 18–21. The current findings suggest that such interventions might be especially useful for young adults with ADHD during this developmental period, and that they should be implemented as early as possible in the transition to young adulthood. Importantly, the nonsignificant peer-to-personal alcohol use associations in the within-person analyses suggest that such interventions would need to effect lasting change in order to meaningfully impact drinking outcomes, by de-escalating one’s trajectory of peer alcohol use entirely rather than merely producing time-limited reductions.
The lack of association between declining perceived peer alcohol use from ages 21 to 29 and heavy drinking at age 29 for the ADHD group may also reflect ADHD-specific risk. The results of another longitudinal study similarly showed that perceived peer substance use was less strongly associated with heavy drinking at mean age 25 for those with ADHD than for those without (Kennedy et al., 2019). Together, these findings may reflect weaker socialization of those with ADHD for maturing out of heavy drinking as they age through their 20s. Numerous functional impairments in adulthood starkly differentiate the ADHD group from the non-ADHD group despite relatively low levels of persistent diagnosable ADHD (Pelham III et al., 2020), indicating clinically meaningful problems in life functioning emanating from childhood ADHD that may play a role in these findings. Specifically, delayed assumption of adult roles and responsibilities in the ADHD group may partly underlie the detachment of their drinking behaviors from the declining patterns of their peers. For instance, adults with versus without ADHD are less likely to be married, report fewer familial connections, have less stable employment, and are less financially independent (Barkley, 2015; Biederman et al., 1993; Hechtman et al., 2016; Klein et al., 2012; Michielsen et al., 2015; Murphy & Barkley, 1996; Pelham III et al., 2020), which may afford relatively more time and opportunity for heavy drinking. These and other factors, such as increasing rates of depression among young adults with ADHD during this time period (Wang et al., 2019) and the manifestation of familial risk for alcoholism (Molina et al., 2016), may contribute to sustained heavy drinking even when their peers begin to decrease their drinking behaviors.
Another explanation for these findings may be that young adults with ADHD relative to those without ADHD underestimate their own drinking risk when they compare themselves to their peers, and therefore continue high-risk drinking patterns even as their peers mature out of these patterns with age. Positive bias by individuals with ADHD, shown for perception of their own symptoms (Owens et al., 2007; Sibley, Campez, & Raiker, 2017), may generalize to a misperception of their risk for heavy drinking in the context of peer alcohol use. Interventions in which individuals receive personalized feedback about their own levels of drinking (Riper et al., 2009; Suffoletto et al., 2015) might be especially useful in this case.
Despite these riskier average-level patterns within the ADHD group, the within-person links between personal alcohol use and subsequent year perceived peer alcohol use were not higher for individuals with ADHD, indicating that they are no more affected by time-limited shifts off of their drinking trajectories than are those without ADHD. Additionally, the lack of group differences in heavy drinking at age 29 may suggest that the outcomes of the processes investigated here on individuals’ own drinking may not fully manifest until later adulthood. In other words, a potentially riskier process may be involved in the drinking patterns of young adults with versus without ADHD at age 29, even though they have similar levels of drinking – which may diverge only later in adulthood. Factors not examined herein may be important. These include a tightening of the significant association between depression and alcohol use over time for those with ADHD (Wang et al., 2019) and specific facets of impulsivity, including negative and positive urgency (Pedersen et al., 2016). This possibility necessitates longitudinal studies that extend further into adulthood, beyond the 20s, when ADHD-related risk for alcohol use may more starkly differentiate individuals.
Limitations & Future Directions
Several limitations to the current study suggest potential avenues for future work. Despite the unique strengths of the PALS, including a prospective longitudinal design in a large sample, the racial and gender diversity of the sample is limited. Moreover, all participants with ADHD were clinic-referred and participated in a summer treatment program in childhood, and findings may not generalize to the broader ADHD population at large. Further, because enrolled PALS participants had lower CD symptoms than non-enrolled participants, the sample may have excluded children with greater long-term risk for heavy alcohol use, potentially limiting the generalizability of the findings; however, the effect size of this difference was small. Another limitation includes the potentially questionable reliability of heavy drinking frequency, which was measured using a single item. Future research should integrate related constructs, such as frequency of drunkenness, to enhance reliability. Moreover, given the high prevalence of cannabis use among young adults (SAMHSA, 2019), and both cannabis and other substances among young adults with ADHD histories (Molina et al., 2018), extended study of these associations to other substances should be conducted. Such work would importantly advance the peer substance use literature, which has centered primarily on alcohol.
Of note, our findings center on individuals’ subjective perceptions of their peers’ alcohol use. Nonetheless, prior research has shown that these perceptions themselves strongly influence individuals’ own drinking behavior, regardless of peers’ actual alcohol use (Schulte et al., 2010). Lastly, although most peer use studies have measured perceived alcohol use among one’s peers generally, some research has shown that the differential quality/closeness of one’s relationships affects their influence, with closer friendships exerting stronger effects (e.g., Hussong, 2002; Overbeek et al., 2011). In this study, we took relationship closeness into account by assessing how many of the participants’ friends used alcohol rather than asking about peers their age more generally. However, future work should differentiate between alcohol use by peers generally, friends, and best friends to test potential moderating effects of relationship closeness. This approach may be especially important for individuals with ADHD, as they may have fewer close friends owing to their social impairments that cause difficulty making and keeping friends (McQuade & Hoza, 2015; Murphy, 2015).
Conclusions
Latent growth modeling showed that between person, peer alcohol use changed in tandem with individuals’ own heavy drinking frequency across young adulthood, from ages 18 to 29. Moreover, within-person analyses underscored the importance of peer selection over socialization effects on a year-to-year basis. Importantly, a general pattern of developmentally atypical associations between perceived peer alcohol use and individuals’ own heavy drinking suggested the possibility of a riskier pathway to drinking outcomes in the ADHD group. This was reflected in several group differences: (1) faster escalation in heavy drinking frequency early on in adulthood (age 18–21) in the ADHD group; (2) an association between increasing perceived peer alcohol use from ages 18–21 and more frequent heavy drinking at age 29 for the ADHD group only; and (3) failure of the ADHD group to model the declining, maturing out process of their peers from ages 21–29. Interventions that target selection of social contexts by individuals with ADHD in the early years of adulthood, especially when drinking is escalating, may be needed to prevent worsening patterns of heavy drinking by the end of young adulthood.
Table 1.
Perceived Peer Alcohol Use and Individuals’ Own Heavy Drinking Frequency Descriptive Statistics by Age and ADHD Status
| Perceived Peer Alcohol Use | Heavy Drinking Frequency | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| ADHD | non-ADHD | ADHD | non-ADHD | |||||||
| Age | M | SD | M | SD | t | M | SD | M | SD | t |
| 18 | 2.97 | 1.52 | 3.22 | 1.37 | 1.55 | 1.79 | 2.48 | 1.75 | 2.27 | −0.16 |
| 19 | 3.20 | 1.44 | 3.78 | 1.30 | 4.08*** | 2.50 | 2.71 | 2.91 | 2.79 | 1.46 |
| 20 | 3.25 | 1.55 | 4.00 | 1.21 | 5.34*** | 2.60 | 2.87 | 3.30 | 2.81 | 2.48* |
| 21 | 3.45 | 1.46 | 4.14 | 1.13 | 5.42*** | 3.10 | 2.98 | 3.60 | 2.71 | 1.85 |
| 22 | 3.35 | 1.39 | 4.16 | 1.23 | 6.43*** | 2.94 | 2.81 | 3.56 | 2.75 | 2.41* |
| 23 | 3.38 | 1.38 | 4.03 | 1.27 | 5.21*** | 2.74 | 2.76 | 3.43 | 2.67 | 2.75** |
| 24 | 3.45 | 1.47 | 4.16 | 1.21 | 4.65*** | 2.75 | 2.77 | 3.65 | 2.69 | 3.04** |
| 25 | 3.28 | 1.36 | 4.00 | 1.32 | 5.23*** | 2.37 | 2.53 | 3.04 | 2.56 | 2.62** |
| 26 | 3.27 | 1.40 | 3.98 | 1.24 | 3.77*** | 2.57 | 2.71 | 3.04 | 2.71 | 1.27 |
| 27 | 3.31 | 1.32 | 3.94 | 1.24 | 4.99*** | 2.44 | 2.65 | 2.98 | 2.45 | 2.10* |
| 28 | 3.24 | 1.41 | 3.69 | 1.28 | 1.71 | 2.46 | 2.61 | 2.43 | 2.66 | −0.05 |
| 29 | 3.06 | 1.27 | 3.95 | 1.18 | 7.15*** | 2.34 | 2.62 | 2.81 | 2.38 | 1.87 |
Note. t statistics and associated p-values reflect the results of independent samples t-tests between ADHD and non-ADHD groups within each age.
p<.05;
p<.01;
p<.001.
Acknowledgments
This research was principally supported by AA00202, AA011873, and DA12414. Additional support was provided by AA007453. The authors declare no conflicts of interest.
The authors are grateful to Patrick Curran for instrumental consultation and guidance on the analyses for this study and to Frances Wang for valuable input on this paper. We also thank Heather Joseph and Teague Henry for their assistance.
Footnotes
CFI, comparative fit index; TLI, Tucker-Lewis index; RMSEA, root mean square error of approximation; SRMR, standardized root mean square residual.
Although unstandardized coefficients were equal between the ADHD and non-ADHD group (except where noted below), standardized coefficients are reported to aid interpretation, which may differ between groups due to differing variances and group sizes.
Unstandardized estimates are presented for the LCM-SR results, as standardized coefficients were not available for this model.
Contributor Information
Traci M. Kennedy, University of Pittsburgh.
Christine A. P. Walther, University of Houston – Clear Lake
Sarah L. Pedersen, University of Pittsburgh
Kirsten M. P. McKone, University of Pittsburgh.
Elizabeth M. Gnagy, Florida International University
William E. Pelham, Jr., Florida International University
Brooke S. G. Molina, University of Pittsburgh
References
- Altszuler AR, Page TF, Gnagy EM, Coxe S, Arrieta A, Molina BSG, Pelham WE Jr (2016) Financial dependence of young adults with childhood ADHD. Journal of Abnormal Child Psychology 44:1217–1229. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Andrews JA, Tildesley E, Hops H, Li F (2002) The influence of peers on young adult substance use. Health Psychology 21:349–357. [DOI] [PubMed] [Google Scholar]
- Barkley RA (2015) Educational, occupational, dating and marital, and financial impairments in adults with ADHD, in Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis & Treatment, 4th Edition (Barkley RA eds), pp 314–342. Guilford: New York. [Google Scholar]
- Becker SJ, Marceau K, Hernandez L, & Spirito A (2019) Is it selection or socialization? Disentangling peer influences on heavy drinking and marijuana use among adolescents whose parents received brief interventions. Substance Abuse: Research and Treatment 13:1–9. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Belendiuk KA, Pedersen SL, King KM, Pelham WE, Molina BSG (2016). Change over time in adolescent and friend alcohol use: differential associations for youth with and without childhood attention-deficit/hyperactivity disorder (ADHD). Psychology of Addictive Behaviors 30:29–38. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Biederman J, Faraone S, Spencer T, Wilens T, Norman D, Lapey KA, Mick E, Lehman BK, Doyle A (1993) Patterns of psychiatric comorbidity, cognition, and psychosocial functioning in adults with attention deficit hyperactivity disorder. American Journal of Psychiatry 150:1792–1798. [DOI] [PubMed] [Google Scholar]
- Borsari B, Carey KB (2003) Descriptive and injunctive norms in college drinking: a meta-analytic integration. Journal of Studies on Alcohol 64:331–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Borsari B, Carey KB (2006) How the quality of peer relationships influences college alcohol use. Drug and Alcohol Review 25:361–370. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Center for Behavioral Health Statistics and Quality (2015) Behavioral health trends in the United States: Results from the 2014 National Survey on Drug Use and Health (HHS Publication No. SMA 15- 4927, NSDUH Series H-50). Available at http://www.samhsa.gov/data/s
- Charach A, Yeung E, Climans T, Lillie E (2011) Childhood Attention-Deficit/Hyperactivity Disorder and future substance use disorders: comparative meta-analyses. Journal of the American Academy of Child & Adolescent Psychiatry 50:9–21. [DOI] [PubMed] [Google Scholar]
- Chassin L, Pitts SC, Prost J (2002) Binge drinking trajectories from adolescence to emerging adulthood in a high-risk sample: predictors and substance abuse outcomes. Journal of Consulting and Clinical Psychology 70:67–78. [PubMed] [Google Scholar]
- Curran PJ, Howard AL, Bainter SA, Lane ST, & McGinley JS (2014) The separation of between-person and within-person components of individual change over time: A latent curve model with structured residuals. Journal of Consulting and Clinical Psychology 82: 879–894. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Curran PJ, Stice E, Chassin L (1997) The relation between adolescent alcohol use and peer alcohol use: a longitudinal random coefficients model. Journal of Consulting and Clinical Psychology 65:130–140. [DOI] [PubMed] [Google Scholar]
- Derefinko KJ, Charnigo RJ, Peters JR, Adams ZW, Milich R, Lynam DR (2016) Substance use trajectories from early adolescence through the transition to college. Journal of Studies on Alcohol and Drugs 77:924–935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dotson KB, Dunn ME, Bowers CA (2015) Stand-alone personalized normative feedback for college student drinkers: a meta-analytic review, 2004 to 2014. PLOS One 10:e0139518. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Flora DB (2008) Specifying piecewise latent trajectory models for longitudinal data. Structural Equation Modeling: A Multidisciplinary Journal 15:513–533. [Google Scholar]
- Haller M, Handley E, Chassin L, Bountress K (2010) Developmental cascades: linking adolescent substance use, affiliation with substance use promoting peers, and academic achievement to adult substance use disorders. Development and Psychopathology 22:899–916. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hechtman L, Swanson JM, Sibley MH, Stehli A, Owens EB, Mitchell JT, Arnold LE, Molina BSG, Hinshaw SP, Jensen PS, Abikoff HB, Perez Algorta G, Howard AL, Hoza B, Etovitch J, Houssais S, Lakes KD, Nichols JQ for the MTA Cooperative Group (2016) Functional adult outcomes 16 years after childhood diagnosis of Attention-Deficit/Hyperactivity Disorder: MTA results. Journal of the American Academy of Child and Adolescent Psychiatry 55:945–952. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Howard AL, Kennedy TM, Mitchell JT, Sibley M, Hinshaw SP, Arnold LE, Roy A, Stehli A, Swanson JM, Molina BSG (in press). ADHD-related risk for young adult substance use is rooted in early-onset, developmentally atypical adolescent substance involvement. Psychology of Addictive Behaviors. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Hussong AM (2002) Differentiating peer contexts and risk for adolescent substance use. Journal of Youth and Adolescence 31:207–220. [Google Scholar]
- Jessor R, Jessor S, Donovan J (1981) Young Adult Follow-up Study: 1981 Annual Questionnaire. Institute of Behavioral Science, Boulder, CO. [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG, Schulenberg JE (2006) Monitoring the Future: National results on adolescent drug use. Overview of key findings 2005. NIH Publication No. 06–5882. National Institute on Drug Abuse, Bethesda, MD. [Google Scholar]
- Kennedy TM, Howard AL, Mitchell JT, Hoza B, Arnold LE, Hechtman LT, Swanson JM, Stehli A, Molina BSG (2019) Adult substance use as a function of growth in peer use across adolescence and adulthood in the context of ADHD: findings from the MTA. Addictive Behaviors 99 (online first). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Klein RG, Mannuzza S, Olazagasti MAR, Roizen E, Hutchison JA, Lashua EC, Castellanos FX (2012) Clinical and functional outcome of childhood attention-deficit/hyperactivity disorder 33 years later. Archives of General Psychiatry 69:1295–1303. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kreider RM, Ellis R (2011) Number, timing, and duration of marriages and divorces: 2009 Current Population Reports, P70–125, U.S. Census Bureau, Washington, DC. [Google Scholar]
- Lee SS, Humphreys KL, Flory K, Liu R, Glass K (2011) Prospective association of childhood attention-deficit/hyperactivity disorder (ADHD) and substance use and abuse/dependence: a meta-analytic review. Clinical Psychology Review 31:328–341. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Marshal MP, Molina BSG, Pelham WE Jr (2003) Childhood ADHD and adolescent substance use: An examination of deviant peer group affiliation as a risk factor. Psychology of Addictive Behaviors 17:293–302. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Mason MJ, Zaharakis N, Benotsch EG (2014) Social networks, substance use, and mental health in college students. Journal of American College Health 62:470–477. [DOI] [PubMed] [Google Scholar]
- McQuade JD, Hoza B (2015) Peer relationships of children with ADHD, in Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis & Treatment, 4th edition (Barkley RA eds) pp 210–222. Guilford, New York. [Google Scholar]
- Merrill BM, Molina BSG, Coxe S, Gnagy EM, Altszuler AR, Macphee FL, Morrow AS, Trucco EM, & Pelham WE Jr (2019) Functional outcomes of young adults with childhood ADHD: A latent profile analysis. Journal of Clinical Child & Adolescent Psychology (advance online publication). [DOI] [PMC free article] [PubMed] [Google Scholar]
- Michielsen M, Comijs HC, Aartsen MJ, Semijn EJ, Beekman ATF, Deeg DJH, Kooij JJ (2015) The relationships between ADHD and social functioning and participation in older adults in a population-based study. Journal of Attention Disorder 19:368–379. [DOI] [PubMed] [Google Scholar]
- Molina BSG, Howard AL, Swanson JM, Stehli A, Mitchell JT, Kennedy TM, Epstein JN, Arnold LE, Hechtman L, Vitiello B, Hoza B (2018) Substance use through adolescence into early adulthood after childhood-diagnosed ADHD: findings from the MTA longitudinal study. Journal of Child Psychology and Psychiatry 59:692–702. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molina BSG, Gnagy EM, Joseph HM, Pelham WE Jr (2016) Antisocial alcoholism in parents of adolescents and young adults with ADHD. Journal of Attention Disorders 24: 1295–1304. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molina BSG, Pelham WE Jr (2003) Childhood predictors of adolescent substance use in a longitudinal study of children with ADHD. Journal of Abnormal Psychology 112:497–507. [DOI] [PubMed] [Google Scholar]
- Molina BSG, Pelham WE Jr, Cheong J, Marshal MP, Gnagy EM, Curran PJ (2012) Childhood Attention-Deficit/Hyperactivity Disorder (ADHD) and growth in adolescent alcohol use: the roles of functional impairments, ADHD symptom persistence, and parental knowledge. Journal of Abnormal Psychology 121:922–935. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Molina BSG, Pelham WE Jr, Gnagy EM, & Marshal MP (2007) Attention-Deficit-Hyperactivity Disorder risk for heavy drinking and Alcohol Use Disorder is age specific. Alcoholism: Clinical & Experimental Research 31:643–654. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Murphy KR (2015) Psychological counseling of adults with ADHD, in Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis & Treatment, 4th edition (Barkley RA eds) pp 741–756. Guilford, New York. [Google Scholar]
- Murphy K, Barkley RA (1996) Attention deficit hyperactivity disorder in adults: Comorbidity and adaptive impairments. Comprehensive Psychiatry 37:393–401. [DOI] [PubMed] [Google Scholar]
- Muthén LK, Muthén BO (1998–2017). Mplus user’s guide (8th ed.). Muthén & Muthén, Los Angeles. [Google Scholar]
- Neighbors C, Lee CM, Lewis M, Fossos N, Larimer ME (2007) Are social norms the best predictor of outcomes among heavy-drinking college students? Journal of Studies on Alcohol and Drugs 68:56–565. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Overbeek G, Bot SM, Meeus WHJ, Sentse M, Knibbe RA, Engels R (2011) Where it’s at! The role of best friends and peer group membership in young adults’ alcohol use. Journal of Research on Adolescence 21:631–638. [Google Scholar]
- Owens JS, Goldfine ME, Evangelista NM, Hoza B, & Kaiser NM (2007) A critical review of self-perceptions and the positive illusory bias in children with ADHD. Clinical Child and Family Psychology Review 10:335–351. [DOI] [PubMed] [Google Scholar]
- Pedersen SL, Walther CAP, Harty SC, Gnagy EM, Pelham WE Jr, Molina BSG (2016) The indirect effects of childhood attention deficit hyperactivity disorder on alcohol problems in adulthood through unique facets of impulsivity. Addiction 111:1582–1589. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pelham Jr WE, Fabiano GA, Gnagy EM, Greiner AR, Hoza B (2005) The role of summer treatment programs in the context of comprehensive psychosocial treatment for attention-deficit/hyperactivity disorder In Hibbs E & Jensen P (Eds.), Psychosocial treatments for child and adolescent disorders: Empirically based strategies for clinical practice (2nd ed., pp. 377–411). Washington, DC: American Psychiatric Association. [Google Scholar]
- Pelham WE Jr., Gnagy EM, Greenslade KE, Milich R (1992) Teacher ratings of DSM-III-R symptoms for the disruptive behavior disorders. Journal of the American Academy of Child & Adolescent Psychiatry 31: 210–218. [DOI] [PubMed] [Google Scholar]
- Pelham III WE, Page TF, Altszuler AR, Gnagy EM, Molina BSG, & Pelham WE Jr (2020) The long-term financial outcome of children diagnosed with ADHD. Journal of Consulting and Clinical Psychology 88:160–171. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Riper H, van Straten A, Keuken M, Smit F, Schippers G, & Cuijpers P (2009) Curbing problem drinking with personalized-feedback interventions: A meta-analysis. American Journal of Preventive Medicine 36:247–255. [DOI] [PubMed] [Google Scholar]
- SAMHSA (2019) Key substance use and mental health indicators in the United States: Results from the 2018 National Survey on Drug Use and Health (HHS Publication No. PEP19 5068, NSDUH Series H 54). Rockville, MD: Center for Behavioral Health Statistics and Quality, Substance Abuse and Mental Health Services Administration. [Google Scholar]
- Schulte MT, Monreal TK, Kia-Keating M, Brown SA (2010) Influencing adolescent social perceptions of alcohol use to facilitate change through a school-based intervention. Journal of Child & Adolescent Substance Abuse 19:372–390. [Google Scholar]
- Sibley MH, Campez M, & Raiker JS (2019). Reexamining ADHD-related self-reporting problems using polynomial regression. Assessment 26:305–314. [DOI] [PubMed] [Google Scholar]
- Sibley MH, Pelham WE Jr., Molina BSG, Gnagy EM, Waxmonskey JG, Waschbusch DA, Derefinko KJ, Wymbs BT, Garefino AC, Babinski DE, Kuriyan AB (2012) When diagnosing ADHD in young adults emphasize informant reports, DSM items, and impairment. Journal of Consulting and Clinical Psychology 80: 1052–1061. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Suffoletto B, Kristan J, Chung T, Jeong K, Fabio A, Monti P, & Clark DB (2015) An interactive text message intervention to reduce binge drinking in young adults: A randomized controlled trial with 9-month outcomes. PLoS ONE 10: e0142877. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Van Eck K, Markle RS, Dattilo L, Flory K (2014) Do peer perceptions mediate the effects of ADHD symptoms and conduct problems on substance use for college students? Psychology of Addictive Behaviors 28:431–442. [DOI] [PubMed] [Google Scholar]
- Wang FL, Pedersen SL, Joseph H, Gnagy EM, Curran P, Pelham WE, Molina BSG (2019) Role of ADHD in the co-occurrence between heavy alcohol use and depression trajectories in adulthood. Alcoholism: Clinical and Experimental Research 43: 342–352. [DOI] [PMC free article] [PubMed] [Google Scholar]
- White HR, McMorris BJ, Catalano RF, Fleming CB, Haggerty KP, Abbott RD (2006) Increases in alcohol and marijuana use during the transition out of high school into emerging adulthood: the effects of leaving home, going to college, and high school protective factors. Journal of Studies on Alcohol 67:810–822. [DOI] [PMC free article] [PubMed] [Google Scholar]