

Abstract
The current IASP definition of pain as “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” was recommended by the Subcommittee on Taxonomy and adopted by the IASP Council in 1979. This definition has become accepted widely by health care professionals and researchers in the pain field and adopted by several professional, governmental, and nongovernmental organizations, including the World Health Organization. In recent years, some in the field have reasoned that advances in our understanding of pain warrant a re-evaluation of the definition and have proposed modifications. Therefore, in 2018, the IASP formed a 14-member, multinational Presidential Task Force comprising individuals with broad expertise in clinical and basic science related to pain to evaluate the current definition and accompanying note and recommend whether they should be retained or changed. This review provides a synopsis of the critical concepts, the analysis of comments from the IASP membership and public, and the committee’s final recommendations for revisions to the definition and notes, which were discussed over a 2-year period. The task force ultimately recommended that the definition of pain be revised to “An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage,” and that the accompanying notes be updated to a bulleted list that included the etymology. The revised definition and notes were unanimously accepted by the IASP Council early this year.
“Scientific and medical definitions are tools. Even when we recognize them as imperfect or provisional, awaiting replacement by an improved version, they perform work that cannot be accomplished by less precise instruments.”
David B. Morris [27]
1. Introduction
In 1978, after two years of deliberations, the International Association for the Study of Pain (IASP) Subcommittee on Taxonomy, chaired by Professor Harold Merskey and including representatives from diverse specialties, recommended definitions of “Pain Terms” to the IASP Council [19]. The subcommittee’s recommendations, which were strongly endorsed by then IASP president John J. Bonica and approved by the Council over four decades ago, included the current IASP definition of pain [7]. Pain was defined as “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage” (Text box 1). In the accompanying editorial, John Bonica emphasized that the “development and widespread adoption of universally accepted definitions of terms” was one of the primary objectives and responsibilities of the organization. The subcommittee report highlighted that the definitions may be modified as new knowledge is acquired and that the recommendations were intended to “serve as an operational framework, not as a constraint on future development” [7,19].
Text Box 1. IASP Definition of Pain (1979).
Pain
An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.
Note:
Pain is always subjective. Each individual learns the application of the word through experiences related to injury in early life. Biologists recognize that those stimuli which cause pain are liable to damage tissue. Accordingly, pain is that experience which we associate with actual or potential tissue damage. It is unquestionably a sensation in a part or parts of the body but it is also always unpleasant and therefore also an emotional experience. Experiences which resemble pain, e.g., pricking, but are not unpleasant, should not be called pain. Unpleasant abnormal experiences (dysaesthesiae) may also be pain but are not necessarily so because, subjectively, they may not have the usual sensory qualities of pain.
Many people report pain in the absence of tissue damage or any likely pathophysiological cause; usually this happens for psychological reasons. There is no way to distinguish their experience from that due to tissue damage if we take the subjective report. If they regard their experience as pain and if they report it in the same ways as pain caused by tissue damage, it should by accepted as pain. This definition avoids tying pain to the stimulus. Activity induced in the nociceptor and nociceptive pathways by a noxious stimulus is not pain, which is always a psychological state, even though we may well appreciate that pain most often has a proximate physical cause.
The IASP definition of pain has become accepted globally by health care professionals and researchers in the pain field, and has been adopted by several professional, governmental, and nongovernmental organizations, including the World Health Organization (WHO). Although subsequent revisions and updates have been made to the list of associated pain terms (1986, 1994, 2011), the IASP definition of pain itself has remained unchanged. However, in recent years, some in the field have contended that advances in our understanding of pain in its broadest sense warrant a re-evaluation of the definition [2,5,10,37]. Several proposed modifications to the current definition of pain have stimulated considerable discussion with strong, sometimes fervent, opinions favoring or opposing the need for revision [1,4,5,11,12,15,29,31,32,39,40]. Acknowledging these ongoing discussions, the IASP president, Judith Turner, formed a Presidential Task Force in the spring of 2018 to “evaluate IASP’s current definition of pain and the accompanying note” and to recommend whether they “should be retained or changed based on current evidence-based knowledge.” A 14-member task force was formed that comprised individuals from several nations who had broad expertise in clinical and basic science related to pain. The task force deliberated over a nearly 2-year period (2018–2020). This review provides a synopsis of the task force members’ discussions of the critical concepts, the analysis of the comments from the IASP membership and public, and the committee’s final recommendations for revisions to the definition and notes that were unanimously accepted by the IASP Council early this year.
2. Pro and con arguments for updating the IASP definition
Pain can range widely in intensity, quality, and duration and has diverse pathophysiologic mechanisms and meanings. Therefore, defining the concept of pain in a concise and precise manner presents a challenge. Several prominent leaders in the last century have alluded to this problem, including Sir Thomas Lewis, who wrote in the preface to his monograph entitled PAIN, “Reflection tells me that I am so far from being able to define pain that the attempt could serve no useful purpose” [23]. Merskey, the chair of the IASP Subcommittee on Taxonomy, recognized that pain was “a psychological concept and not a physical measure” and that the experience of pain had to be distinguished from noxious stimulation [25,26]. Thus, the current IASP definition acknowledges that although tissue injury is a common antecedent to pain, pain can be present even when tissue damage is not discernible. The strengths of the definition include its recognition of the multidimensional aspects of pain, its brevity, and its simplicity. The definition has helped provide a common understanding of the term pain to clinicians, researchers, and persons with pain across the globe and has influenced health policy, research, and clinical care [21,27].
Criticisms of the definition and note:
Criticisms of the IASP definition have included that it is “Cartesian,” ignoring the multiplicity of mind-body interactions [27], and that it neglects “the ethical dimensions of pain” and does not adequately address pain in disempowered and neglected populations, such as neonates and the elderly [3,13]. It has been argued that the current definition emphasizes verbal self-report at the expense of nonverbal behaviors that may provide vital information, especially in non-human animals and humans with impaired cognition or language skills [2,13]. A concern expressed recently about the current definition was that it excluded cognitive and social factors that are integral to the experience of pain [37]. In addition, the term “unpleasant” has been debated as potentially trivializing the severe pain and suffering associated with many acute and chronic clinical pain states and fails to capture “the full range of words that could be used to describe the experience” and its associated suffering [8,10,17,37]. Finally, it has also been argued that pain is more than a symptom, that chronic pain may be a disease with its own clinical course [24,33], and hence the definition should reflect this perspective.
In recent years, several alternate definitions have been proposed (Table 1). Williams and Craig [37] defined pain as “a distressing experience associated with actual or potential tissue damage with sensory, emotional, cognitive and social components.” Cohen et al. [10] offered the following revised definition: “Pain is a mutually recognizable somatic experience that reflects a person’s apprehension of threat to their bodily or existential integrity.” Other definitions and modifications to the IASP definition have been proposed by Wright [39] and Aydede [5] (Table 1).
Table 1.
A word matrix comparing the current IASP definition of pain with other proposed revisions, and the task force’s initial and revised final definitions.
| Current (IASP), 1979 | unpleasant | sensory and emotional | experience | associated with | actual or potential tissue damage | or described in terms of such damage |
|---|---|---|---|---|---|---|
| Wright, 2011 | unpleasant | sensation | that has evolved to motivate behavior | which avoids or minimizes tissue damage, or promotes recovery | ||
| Williams & Craig, 2016 | distressing | [with sensory, emotional, cognitive and social components] | experience | associated with | actual or potential tissue damage | |
| Cohen et al., 2018 | mutually recognized | somatic | experience | that reflects | a person’s apprehension of threat to their bodily or existential integrity | |
| Aydede, 2019 | unpleasant | sensory and emotional | experience | that para-digmatically results from | actual or potential tissue damage | or is of the same kind or similar to such an experience. |
| Initial IASP task force proposition, 2019 | aversive | sensory and emotional | experience | typically caused by | actual or potential tissue injury | [or resembling that caused by] |
| Revised IASP task force definition, 2020 | unpleasant | sensory and emotional | experience | associated with | actual or potential tissue damage | or resembling that associated with |
The note that accompanies the current definition has also been criticized as redundant, (i.e., reiterating concepts that are already present in the definition), outdated (statements such as “pain in the absence of tissue damage or any likely pathophysiological cause” usually has “psychological reasons”), and lacking precision [10,39].
3. Methods
The task force adopted multiple approaches, including a modified Delphi survey method, accompanied by monthly web conferencing, e-mail discussions, and face-to-face meetings of its members. The task force sought external advice from bioethicists, philosophers, and a linguistic expert. In addition, the task force sought comments from a broader community that included the IASP membership and the public. An initial definition and accompanying notes were published on the IASP website in August 2019 with an invitation for written feedback from the public during a 1-month period. The task force conducted a qualitative content analysis of the comments received, and then discussed them further. A revised recommendation, taking all sources of feedback into consideration, was submitted to IASP Council for approval in November 2019. Based on the feedback from the Council, minor edits to the note were made and a final recommendation (Text Box 2) submitted in January 2020.
Text Box 2. Revised IASP Definition of Pain (2020).
Pain
An unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage.
Notes
Pain is always a personal experience that is influenced to varying degrees by biological, psychological, and social factors.
Pain and nociception are different phenomena. Pain cannot be inferred solely from activity in sensory neurons.
Through their life experiences, individuals learn the concept of pain.
A person’s report of an experience as pain should be respected.*
Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
Verbal description is only one of several behaviors to express pain; inability to communicate does not negate the possibility that a human or a non-human animal experiences pain.
Etymology:
Middle English, from Anglo-French peine (pain, suffering), from Latin poena (penalty, punishment), in turn from Greek poinē (payment, penalty, recompense).
* The Declaration of Montréal, a document developed during the First International Pain Summit on September 3, 2010, states that “Access to pain management is a fundamental human right.”
4. Concepts, discussions, and initial recommendations
During early discussions among the task force members, consensus was achieved regarding certain basic premises. The definition should be valid for acute and chronic pain and apply to all pain conditions, regardless of their pathophysiology (e.g., nociceptive, neuropathic, and nociplastic) [20,22]. Secondly, the definition of pain should be applicable to humans and non-human animals. Thirdly, pain was to be defined whenever possible from the perspective of the one experiencing the pain, rather than an external observer. The goal was to develop a clear, concise, and unambiguous statement that describes the varied experiences of pain, while recognizing its diversity and complexity [31]. The task force acknowledged from its early deliberations that the note section would benefit from revision. The task force members agreed that the note was not meant to be a treatise on the biology of pain, nor the diagnostic criteria for pain, but should emphasize important aspects of the complexity of pain that were difficult to capture in a brief definition.
Considerable discussion centered on whether to include the social aspects of pain in the definition. Although task force members appreciated how important social aspects of both the acute and chronic pain experience are, the majority opinion was that they were worthy of highlighting in the note but not an essential component of the definition. One argument made was that the influence of the social context was not unique to pain, but was shared by other sensory experiences, including vision and hearing. Rolf-Detlef Treede rhetorically questioned in his commentary, “Can a person alone on a desert island not experience pain?” [32]. The use of the phrase “associated with” to express the relationship between the experience and tissue damage in the current definition has also been criticized as lacking in clarity [39]. The phrase “typically caused by” was considered as a replacement to clarify this relationship between tissue damage and the experience of pain. A major concern regarding the current definition related to the phrase “described in terms of such damage.” Several potential replacements for this phrase, which implies a requirement for verbal communication, were debated. Alternative verbs that were considered in an effort to encompass nonverbal behaviors by humans and animals included “expressed,” “perceived,” “interpreted,” “inferred,” and “apprehended.” In the early deliberations, a majority of task force members preferred the verb “perceived.” An early definition proposed by the task force was thus, “An unpleasant sensory and emotional experience associated with actual or potential tissue damage, or perceived as such damage.” However, this initial preference for the phrase “perceived as such damage” as a replacement for “described in terms of such damage” was subsequently criticized as problematic and potentially having the unintended consequence of excluding the same groups of individuals that the task force was attempting to include in its revision (neonates, people with severe developmental and intellectual disabilities, and most non-human animals).* Based on feedback from the IASP Council on the preliminary definition and note in November 2018, the task force obtained further consultations with experts in ethics and philosophy, and held additional discussions on refining the language. The task force also agreed to seek feedback from the broader community on its initial recommendation and to revise the definition and note based on the comments received.
4.1. Consultation with ethicists and philosophers in response to IASP Council’s initial feedback
A detailed critique of its then-proposed definition of pain was submitted to the task force by Professor Murat Aydede, a regular contributor to the philosophy of pain-related psychology and cognitive science [4,5]. Some task force members agreed with Aydede that replacing “described in terms of” with the proposed language “perceived as” may have unintended negative consequences. Because of the importance of fully considering the nuanced philosophical and linguistic underpinnings of the criticisms, the task force approached Professor Peter Singer (Princeton University) for his comments upon this critique. Professor Singer also enlisted Professors Adam Shriver and Nicholas Shea of Oxford, UK, and University of London, respectively.
Their deliberations were summarized in a concise letter to the task force dated February 13, 2019. The letter asserted that the current IASP definition of pain runs together the question of what it is for someone to be in pain with the separate question of how to tell if someone is in pain. Singer and colleagues proposed this definition: “To be in pain is to have a particular conscious experience that is in important respects similar, qua experience, to the conscious experience that is typically caused by tissue damage, and easily regarded by the experiencing subject as undesirable.” They suggested that this definition be supplemented with a list of “signs of pain [whether] verbal, physiological, behavioral or neural” and include “a clear statement to the effect that a verbal description is not the only kind of evidence for pain, and that there can be evidence of pain in the absence of tissue damage.”
4.2. Initial recommendation to IASP Council and broader community for feedback
The task force welcomed these insights from the philosophers and considered whether these concepts were largely present in a revised definition. The task force agreed that the term “aversive” may be equally applicable to humans and animals experiencing pain, whereas “undesirable” and “unpleasant” may be less applicable to certain animal species. Hence, the term “unpleasant” in the current definition was replaced by “aversive.” Many of the task force members considered that defining pain from the perspective of an observer was controversial and political [35]. The issue of who has the authority to judge who is in pain: “doctors, sufferers, pharmaceutical companies, politicians, the federal government, the states, lawyers, or judges” is contentious [35]. The task force agreed that the primary focus of the definition should be that of the individual experiencing pain.
It would be difficult to describe in detail the nuances of all discussions that went into refining the current note. A brief summary of the essence of the discussions is provided here. It was generally agreed that the key concepts that help highlight our improved understanding of pain in its biopsychosocial context should be indicated as concise statements in a bulleted format. The task force rephrased many of the concepts from the note accompanying the current definition, reorganized their sequence, introduced certain changes, and bulleted the notes to highlight these points. For example, the concept that pain and nociception were not synonymous was considered to be worthy of emphasis. Nociception, in contrast to pain, refers to activity that occurs in the nervous system in response to a noxious stimulus. The role of cognition in pain was discussed and the general opinion was that this was implied in the statements that pain is subjective and modified by life experiences. The concept of the maladaptive nature of chronic pain, in contrast to the protective role of acute pain, was introduced by describing the associated adverse effects of pain on function and social and psychological well-being. The etymology of the word “pain” was also added to raise awareness among readers of its transactional, punitive meaning in contrast to other archaic words that emphasized the location of pain or its negative effect upon mood.
After considerable deliberation, and based on the majority opinion, the task force presented the following recommendation for the definition and note to the IASP Council in July, 2019, published the recommendation on the IASP website, and sought input from the public.
Pain:
An aversive sensory and emotional experience typically caused by, or resembling that caused by, actual or potential tissue injury.
Notes:
Pain is always a subjective experience that is influenced to varying degrees by biological, psychological, and social factors.
Pain and nociception are different phenomena: the experience of pain cannot be reduced to activity in sensory pathways.
Through their life experiences, individuals learn the concept of pain and its applications.
A person’s report of an experience as pain should be accepted as such and respected.
Although pain usually serves an adaptive role, it may have adverse effects on function and social and psychological well-being.
Verbal description is only one of several behaviors to express pain; inability to communicate does not negate the possibility that a human or a non-human animal experiences pain.
Etymology:
Middle English, from Anglo-French peine, from Latin poena (penalty, punishment), in turn from Greek poinē (payment, penalty, recompense).
5. Analysis of feedback from the global pain community
A public consultation on the proposed new definition of pain and accompanying notes was open from August 7, 2019, until September 11, 2019 (See Supplement 1 for further information on the consultation methods and summary of results). Members of the global pain community were invited to submit feedback on the proposed definition of pain via a web-based survey. The survey was in English and included five demographic questions, one question on satisfaction with the proposed definition (rated on a 5-point Likert scale), and two open-ended questions related to feedback on the definition and the notes. The survey was posted on the IASP website and distributed to IASP members through email and to the public over social media. Descriptive statistics were used to summarize demographic characteristics and satisfaction. Responses to the open-ended questions were analyzed by using inductive content analysis [16].
We received 808 responses from individuals across 46 countries. Fifty-eight percent of the respondents self-identified themselves as clinicians, clinical and basic science researchers, administrators, educators, or trainees/students. The remaining 42% identified themselves as an individual living with pain, an individual with pain-related disability, or a care provider for a person living with pain. The proportion of respondents who were very satisfied or satisfied (41.7%) with the proposed definition was nearly equal to the proportion who were dissatisfied or very dissatisfied (41.5%). Of those who were dissatisfied or very dissatisfied, 49.7% were patients and/or their caregivers, and only 32.4% were clinicians, researchers, administrators, educators, and students/trainees. Task force members were provided with a detailed summary of the survey responses along with the individual written comments before additional discussions were held to consider revisions to the initial proposed definition and notes.
All qualitative comments were organized by using the process of open coding for both the definition and notes. Four overarching categories were generated to describe respondents’ feedback to the proposed new definition of pain (see Figure 1 and Supplement 1 for further details). The four categories (and 10 subcategories) were as follows: 1) the definition of pain should be simple and practical (wording is cumbersome, reading level should be lowered to facilitate translation to other languages); 2) the definition should better capture the personal experience of pain (“aversive” as a descriptor of pain, impact of pain on quality of life, and subjectivity of pain); 3) the definition should provide more specificity regarding the various components of pain (pain comes in many forms and pain is influenced by many factors); and 4) the definition’s reference to tissue injury should be better aligned with modern conceptualizations of pain (tissue injury as a cause of pain, pain as an interpretation, and pain resembling tissue injury).
Figure 1.
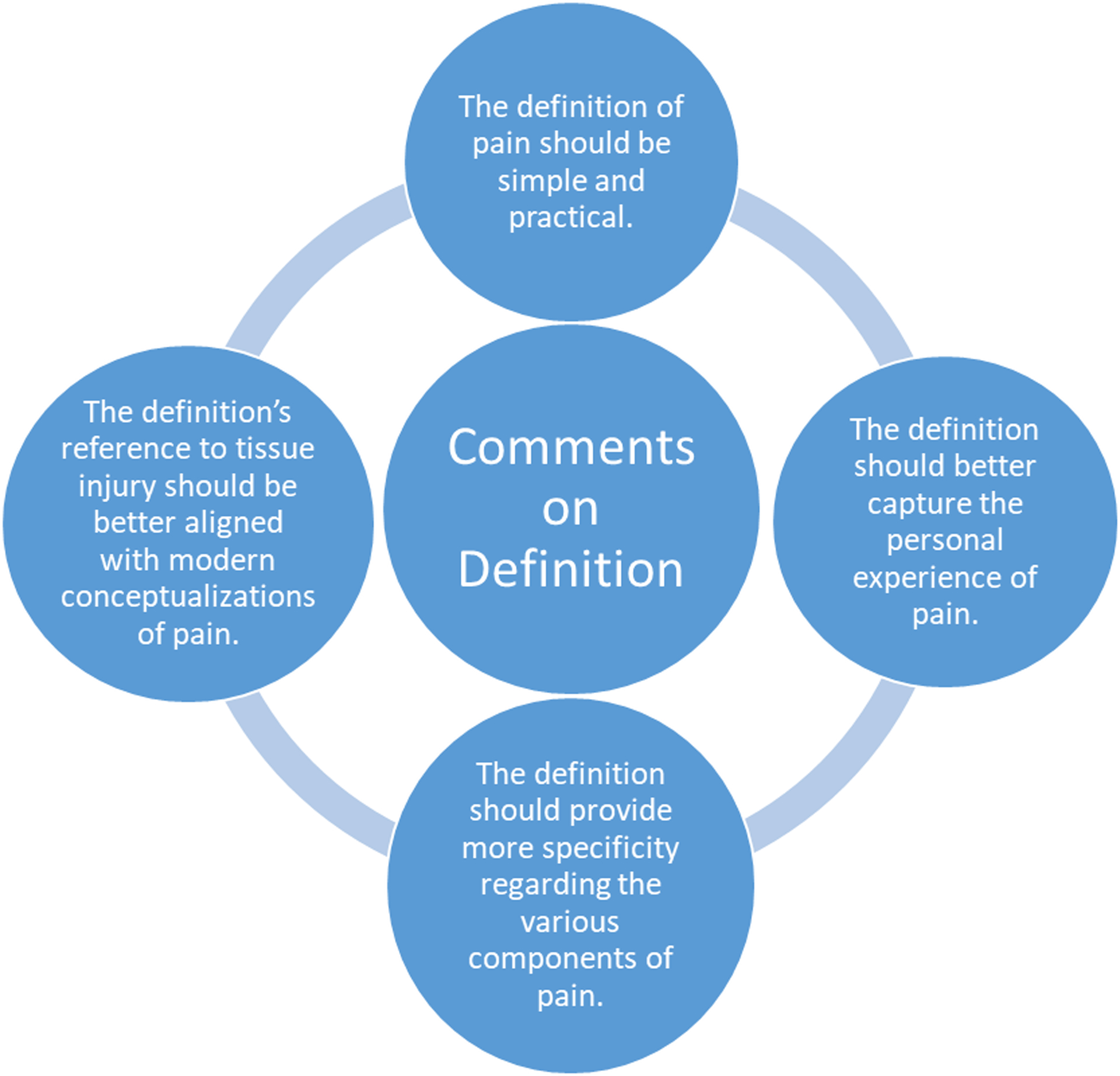
Summary of the key comments received from IASP members and the public on the initial recommended definition, based on a qualitative content analysis conducted by the task force.
Seven overarching categories were generated to describe respondents’ feedback on the notes to the proposed new definition of pain. The seven categories (and 14 subcategories) included: 1) overall comments on the proposed notes (format, clarity, and relevance, level of exposure, and importance of pain management); 2) comments related to the first note (subjectivity of pain and pain is influenced by many factors); 3) comments related to the second note (relationship between pain and nociception and clarity of “sensory pathways”); 4) comments related to the third note (lack of clarity about meaning and implications for neonates and infants); 5) comments related to the fourth note (personal experience of pain and misrepresentation of pain for secondary gain); 6) comments related to the fifth note (not all pain is adaptive); and 7) comments related to the sixth note (communication of pain and inclusion of non-human animals) (see Supplement 1 for details).
6. Additional discussions based on feedback leading to recommendations for the revised definition
Definition:
As indicated above, the term “aversive” was criticized as being not easily understood, especially by the lay public, and not readily translatable into many languages. The suggestion was put forward that in some situations, pain, despite being unpleasant, may not be avoided (e.g., athletes). The term unpleasant highlights the negative affect associated with pain, whereas aversive refers to the negative affect that results in a motivational change. A description of the “unpleasantness” of pain has a long history, with discussions by Hardy, Wolff, and Goodell (1952) in their classic text on pain sensations [18]. Although both terms “aversive” and “unpleasant” were applicable, the committee opted for the simpler term, unpleasant, that was likely to be more easily understood by the broader audience (see Table 1). Another common comment was that the definition should have less emphasis on tissue injury. Partly in response to this concern, the phrase “typically caused by” was reverted back to “associated with,” which does not imply a direct cause-and-effect relationship and reduces the emphasis on tissue injury.
Notes:
A few additional modifications to the notes were made based on the feedback received. It was pointed out that although pain and nociception were clearly not the same, the additional phrase “the experience of pain cannot be deduced from activity in sensory pathways” may not be precise, as recent studies suggest that a multivariate pattern signature in brain regions may predict pain above and beyond nociceptive input [38]. The present role of brain imaging as a “pain-o-meter” is, however, controversial. Davis et al. [14] provide the consensus of an IASP task force that while brain imaging has the potential to increase the understanding of the neural mechanisms of pain and its treatment, it is not a replacement for the verbal report of pain in humans. The description in the note of pain as a “subjective” experience was of concern to many respondents. The concern raised was that it could be interpreted with negative connotations, such as “not objective” or “not real.” The feedback received was that pain is “unique to each individual” and hence personal. The task force accepted this suggestion and rephrased pain as a “personal experience” in the note.
7. Discussion of controversial issues where decisions were based on majority opinion
The revised definition retains from the current definition an emphasis on pain as an experience. The note explicitly distinguishes pain as a personal experience distinct from nociception. Although the task force reverted to the use of the term “unpleasant” to replace “aversive,” the new definition retains a reference to tissue injury: “…associated with, or resembling that associated with, actual or potential tissue injury” to distinguish pain from other aversive experiences (e.g., nausea, itch, and dizziness).
A number of task force members agreed with a prominent theme in the public feedback that tissue injury was given too much prominence in the new definition. Although tissue injury certainly plays a role in nociceptive pain, neuropathic pain is a direct consequence of a lesion or disease of the somatosensory nervous system and may be felt in areas with no tissue damage. In neuropathic pain, pain may be experienced far from the nervous system lesion or disease (e.g., in the leg and foot for those with nerve root compression, or phantom pain for those with a missing limb). Similarly, tissue injury plays no proven role in nociplastic pain. In addition, it has been argued that in chronic pain, the relationship between pain and the state of the tissues is less predictable [6,30,36]. An illustrative example is the discordance between reports of pain and the structural abnormalities visualized by imaging in patients with knee osteoarthritis [6,30,36]. The IASP has defined nociplastic pain as “pain that arises from altered nociception despite no clear evidence of actual or threatened tissue damage causing the activation of peripheral nociceptors or evidence for disease or lesion of the somatosensory system causing the pain [22].” Nociplastic pain is thought to be common and to play a role in many common chronic pain conditions such as fibromyalgia, low back pain, and headache. While many of the task force members opined that nociplastic pain is captured in the revised definition by the phrase “or resembling that caused by, actual or potential tissue injury,” other task force members countered that this was inadequate. The latter group thought that a definition that did not more specifically embrace nociplastic pain syndromes would not fully encompass the complexity of human chronic pain. Some members also argued that a role for social injury, such as psychological trauma or abuse, needed to be included in the new definition so as to address all of the clinically important forms of chronic pain.
8. Potential benefits of this new definition for both research and patient care
In 2013, IASP formed a task force to produce and update a classification of pain diseases for international use [28,33]. As a result of this work, the new edition of the International Classification of Diseases (ICD-11), which the WHO adopted in 2019, includes a chronic pain classification for the first time. In the coming years, ICD-11 will be adopted in several countries. Thus, a revised definition of pain is very timely and aligns with this and other current efforts to advance ontological frameworks within which pain resides [9,34]. These combined efforts of IASP are important steps for recognizing pain as an important health condition and will transform pain research and the care of persons with pain worldwide.
9. Final Recommendations
The final recommendation of the task force that was approved unanimously by the IASP Council members, along with minor edits based on feedback from reviewers of the manuscript, is provided in Text Box 2. Consistent with the vision of the founding members of the IASP and the first IASP Subcommittee on Taxonomy, this task force hopes that the revised definition and the accompanying notes will be a living document that is updated in concert with future progress in the field.
Supplementary Material
Acknowledgements:
The task force members thank the IASP presidents, Judy Turner and Lars Arendt-Nielsen, for their continued support and encouragement. The authors thank the IASP council members and the numerous individuals who provided feedback on the preliminary task force recommendations, including Drs. Murat Aydede and Andrew Wright, which resulted in further revisions to the definition and note. The task force also acknowledges the valuable input from Peter Singer (Ira W. DeCamp Professor of Bioethics, Princeton University), Adam Shriver (Uehiro Center for Practical Ethics, Oxford University), and Nicholas Shea (Professor, Institute of Philosophy, School of Advanced Study, University of London). The task force also thanks Dr. Llevelyn Morgan (Professor of Classical Languages and Literature, Brasenose College, University of Oxford) for his contributions on the etymology of the word pain. The task force is grateful to Mathew D’Uva (ex-CEO) and Yulanda Grant of the IASP office for their administrative support, and to Claire F. Levine, MS, ELS (scientific editor, Department of Anesthesiology/Critical Care Medicine, Johns Hopkins University), for her assistance in editing the manuscript. Srinivasa Raja acknowledges support from National Institutes of Health, NIH-NS26363. Francis J. Keefe thanks the following National Institutes of Health (NIH) grants for financial support: NIH P30AG064201, NIH R01 AG058702, NIH UG1 CA189824, and NIH U2C NR014637.
Disclosure of funding: The authors have no conflicts of interests related to the manuscript.
Footnotes
Conflict of Interests:
None of the authors have expressed conflicts directly related to this manuscript. SNR is a consultant for Allergan, Lexicon Pharmaceuticals, Inc., and is a co-investigator in a grant from Medtronic, Inc. NBF is part of the IMI (Innovative Medicines Initiative) project PainCare, an EU public-private consortium, and the companies involved are Grunenthal, Bayer, Eli Lilly, Esteve, and Teva. NBF has been a consultant for Mitsubishi Tanabe Pharma, Merck, Almirall, and NeuroPN. MR has received research grant funding from Merck.
Letter to the task force from M. Aydede titled “On the IASP Presidential Task Force’s proposal for a new definition of ‘pain’,” dated November 25, 2018.
References
- [1].Alcock MM. Defining pain: past, present, and future. Pain 2017;158:761–2. [DOI] [PubMed] [Google Scholar]
- [2].Anand KJ, Craig KD. New perspectives on the definition of pain. Pain 1996;67:3–6. [DOI] [PubMed] [Google Scholar]
- [3].Anand KJS, Rovnaghi C, Walden M, Churchill J. Consciousness, behavior, and clinical impact of the definition of pain. Pain Forum 1999;8:64–73. [Google Scholar]
- [4].Aydede M Defending the IASP definition of pain. Monist 2017;100:439–64. [Google Scholar]
- [5].Aydede M Does the IASP definition of pain need updating? Pain Rep 2019;4:e777. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [6].Bedson J, Croft PR. The discordance between clinical and radiographic knee osteoarthritis: a systematic search and summary of the literature. BMC Musculoskelet Disord 2008;9:116. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [7].Bonica JJ. The need of a taxonomy. Pain 1979;6:247–8.460931 [Google Scholar]
- [8].Carr DB, Loeser JD, Morris DB. Narrative, Pain and Suffering. Seattle, WA: IASP Press, 2005. [Google Scholar]
- [9].Ceusters W, Michelotti A, Raphael KG, Durham J, Ohrbach R. Perspectives on next steps in classification of oro-facial pain - part 1: role of ontology. J Oral Rehabil 2015;42:926–41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [10].Cohen M, Quintner J, van RS. Reconsidering the International Association for the Study of Pain definition of pain. Pain Rep 2018;3:e634. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [11].Craig KD, de CWA. Reply. Pain 2017;158:363–5. [DOI] [PubMed] [Google Scholar]
- [12].Cunningham N Comments on Derbyshire, PAIN, 67 (1996) 210–211. Pain 1998;74:102–6. [DOI] [PubMed] [Google Scholar]
- [13].Cunningham N Primary requirements for an ethical definition of pain. Pain Forum 1999;8:93–9. [Google Scholar]
- [14].Davis KD, Flor H, Greely HT, Iannetti GD, Mackey S, Ploner M, Pustilnik A, Tracey I, Treede RD, Wager TD. Brain imaging tests for chronic pain: medical, legal and ethical issues and recommendations. Nat Rev Neurol 2017;13:624–38. [DOI] [PubMed] [Google Scholar]
- [15].Derbyshire SWG. Comment on editorial by Anand and Craig. Pain 1996;67:210–1. [Google Scholar]
- [16].Elo S, Kyngas H. The qualitative content analysis process. J Adv Nurs 2008;62:107–15. [DOI] [PubMed] [Google Scholar]
- [17].Fields HL. Pain: an unpleasant topic. Pain 1999;Suppl 6:S61–S69. [DOI] [PubMed] [Google Scholar]
- [18].Hardy JD, Wolff HG, Goodell H. Pain Sensations and Reactions. Baltimore: Williams & Wilkins, 1952. [Google Scholar]
- [19].IASP Subcommittee on Taxonomy. Pain terms: a list with definitions and notes on usage. Recommended by the IASP Subcommittee on Taxonomy. Pain 1979;6:249–52. [PubMed] [Google Scholar]
- [20].Jensen TS, Baron R, Haanpaa M, Kalso E, Loeser JD, Rice AS, Treede RD. A new definition of neuropathic pain. Pain 2011;152:2204–5. [DOI] [PubMed] [Google Scholar]
- [21].Jensen TS, Gebhart GF. New pain terminology: a work in progress. Pain 2008;140:399–400. [DOI] [PubMed] [Google Scholar]
- [22].Kosek E, Cohen M, Baron R, Gebhart GF, Mico JA, Rice AS, Rief W, Sluka AK. Do we need a third mechanistic descriptor for chronic pain states? Pain 2016;157:1382–6. [DOI] [PubMed] [Google Scholar]
- [23].Lewis ST. Pain. New York: Macmillan, 1942. [Google Scholar]
- [24].Loeser JD, Treede RD. The Kyoto protocol of IASP Basic Pain Terminology. Pain 2008;137:473–7. [DOI] [PubMed] [Google Scholar]
- [25].Merskey H Logic, truth and language in concepts of pain. Qual Life Res 1994;3 Suppl 1:S69–S76. [DOI] [PubMed] [Google Scholar]
- [26].Merskey H History and definition of chronic pain In: Rashiq S, Schopflocher D, Taenzer P, Jonsson E, editors. Chronic Pain: A Health Policy Perspective Wiley-VCH Verlag GmbH & Co. KGaA, 2008. pp. 19–28. [Google Scholar]
- [27].Morris DB. The challenges of pain and suffering In: Jensen TS, Wilson PR, Rice ASC, editors. Clinical Pain Management: Chronic Pain. London: Arnold, 2003. pp. 3–14. [Google Scholar]
- [28].Nugraha B, Gutenbrunner C, Barke A, Karst M, Schiller J, Schafer P, Falter S, Korwisi B, Rief W, Treede RD. The IASP classification of chronic pain for ICD-11: functioning properties of chronic pain. Pain 2019;160:88–94. [DOI] [PubMed] [Google Scholar]
- [29].Osborn M Situating pain in a more helpful place. Pain Rep 2018;3:e642. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [30].Schiphof D, Kerkhof HJ, Damen J, de Klerk BM, Hofman A, Koes BW, van Meurs JB, Bierma-Zeinstra SM. Factors for pain in patients with different grades of knee osteoarthritis. Arthritis Care Res (Hoboken) 2013;65:695–702. [DOI] [PubMed] [Google Scholar]
- [31].Tesarz J, Eich W. A conceptual framework for “updating the definition of pain”. Pain 2017;158:1177–8. [DOI] [PubMed] [Google Scholar]
- [32].Treede RD. The International Association for the Study of Pain definition of pain: as valid in 2018 as in 1979, but in need of regularly updated footnotes. Pain Rep 2018;3:e643. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [33].Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, Cohen M, Evers S, Finnerup NB, First MB, et al. Chronic pain as a symptom or a disease: the IASP Classification of Chronic Pain for the International Classification of Diseases (ICD-11). Pain 2019;160:19–27. [DOI] [PubMed] [Google Scholar]
- [34].Treede RD, Rief W, Barke A, Aziz Q, Bennett MI, Benoliel R, Cohen M, Evers S, Finnerup NB, First MB, et al. A classification of chronic pain for ICD-11. Pain 2015;156:1003–7. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [35].Wailoo K Pain: A Political History. Baltimore, MD: Johns Hopkins University Press, 2014. [Google Scholar]
- [36].Wenham CY, Conaghan PG. Imaging the painful osteoarthritic knee joint: what have we learned? Nat Clin Pract Rheumatol 2009;5:149–58. [DOI] [PubMed] [Google Scholar]
- [37].Williams AC, Craig KD. Updating the definition of pain. Pain 2016;157:2420–3. [DOI] [PubMed] [Google Scholar]
- [38].Woo CW, Schmidt L, Krishnan A, Jepma M, Roy M, Lindquist MA, Atlas LY, Wager TD. Quantifying cerebral contributions to pain beyond nociception. Nat Commun 2017;8:14211. [DOI] [PMC free article] [PubMed] [Google Scholar]
- [39].Wright A A criticism of the IASP’s definition of pain. J Conscious Stud 2011;18:19–44. [Google Scholar]
- [40].Wright A, Aydede M. Critical comments on Williams and Craig’s recent proposal for revising the definition of pain. Pain 2017;158:362–3. [DOI] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.