

Abstract
Young adults who experienced child abuse and neglect (CAN) are at significant risk for callous-unemotional traits and substance use problems. Research shows that compromised self-regulation may increase risk for these maladaptive outcomes. In the present cross-sectional study, we examined the moderating role of self-regulation, indexed by heart rate variability reactivity, in the indirect link between CAN and alcohol and other drug use problems via callous-unemotional traits. We utilized a sample of mostly female undergraduate students (N = 130, 81% Female; Mage = 20.72). We hypothesized that (a) CAN and alcohol or other drug use problems would be associated indirectly via elevations in callous-unemotional traits, and (b) that this indirect association would be exacerbated by elevated heart rate variability reactivity. Results indicated that increased callous-unemotional traits underlain in the link between CAN and alcohol or other drug use problems. Further, this indirect link was exacerbated among youth with elevated heart rate variability reactivity. These findings have significant implications for prevention by demonstrating that physiological self-regulation is important to target in substance use prevention among collegiate samples.
Keywords: Substance use disorders, Personality, Psychophysiology, Child maltreatment, Self-regulation
Introduction
Child abuse and neglect (CAN) comprises a significant risk for the development of callous-unemotional (CU) traits (Dackis et al. 2015), a stable personality characteristic with links to deficits in emotional processing (Frick et al. 2014; Loney et al. 2003; Marsh et al. 2008). Individuals with elevated CU traits exhibit increased psychiatric conduct problems, including substance abuse issues (Blair et al. 2014; Frick and White 2008). Based on prior empirical research and conceptualizations from a developmental psychopathology perspective, the connection between adverse rearing environments and alcohol and other drug (AOD) use problems is expected to be underlain by CU traits (Carlson et al. 2015). Furthermore, research suggests that self-regulation problems may intensify maltreated youths’ risk for developing AOD use problems (Oshri et al. 2018). Thus, the present study examines the role of self-regulation in the indirect link between CAN and AOD use problems through elevated CU traits by utilizing a measure of heart rate variability reactivity (HRV-R) as an indirect biomarker of self-regulation (Beauchaine 2015). Filling this empirical knowledge gap is increasingly relevant to young adults whose history of maltreatment is pronouncedly linked to a wide range of substance use problems (Kim and Williams 2009).
CAN, CU, and Risk Behaviors
CAN confers significant risk for the development of maladaptive behaviors in youth and young adults (Fang and Corso 2007; Oshri et al. 2011). Growing research suggests that the link between adverse rearing environments and risk behaviors among youth is partially mediated by personality traits (Oshri et al. 2013). This developmental pathway is further supported by theory and research on the relations among CAN, CU traits, and risk behaviors among youth (Hawes et al. 2019) and young adults in college (Carlson et al. 2015). Recent evolutionary–developmental models suggest that an individual’s stress response system evolves to facilitate synchrony between physiology and local environmental conditions, e.g., the rearing environment (Ellis, Oldehinkel, & Nederhof, 2017). Based on this model, the adaptation of the stress response system underlies variability in individual personality traits. Accordingly, personality traits in young adulthood represent stable patterns of responsiveness to environmental demands, which become consolidated throughout development. Thus, some young adults with early experiences of adverse rearing environments may adapt to these contexts by developing CU traits that are hypothesized to promote coping with subsequent encounters of acute stress.
The connection between CAN and CU is further buttressed by empirical studies. Research suggests that youths who experience harsh parenting often display CU traits that are characterized by dysregulation (i.e., hypo- or hyper-responsiveness) to stressful stimuli (Blair et al. 2014). Specifically, some youths exposed to CAN may develop a stress response pattern and corresponding personality traits that are hypo-vigilant to stress (Dackis et al. 2015), which are characteristic of individuals with increased levels of CU traits. Moreover, studies show that adverse rearing environments can disrupt the ability to ascribe desires, feelings, thoughts, and beliefs to others (Fanti et al. 2013; Oshri et al. 2015; Rogosch and Cicchetti 2004), which eventuates in reduced empathy and a lack of emotional response to others’ pain. Although these traits and related responses to stress during childhood might be adaptive in the context of childhood adversity, they are also are linked to psychopathology and antisocial behaviors (Frick and White 2008; Kimonis et al. 2013a). Moreover, research demonstrates that psychopathic individuals who have elevated levels of CU traits are more likely to engage in risky behavior because they fail to become risk-averse after experiencing negative outcomes (Fanti et al. 2016). Accordingly, maltreated youths report increased levels of CU traits and are at risk for conduct problems and AOD use problems (Carlson et al. 2015).
HRV Reactivity and Self-Regulation
Youth self-regulation in situations of acute social stress can reduce the risk for substance use (Oshri et al. 2018). Self-regulation in response to environmental stress is modulated by the autonomic nervous system (ANS), which is divided into two main branches: the sympathetic and the parasympathetic nervous system (PNS). The PNS is responsible for resting and digesting, and for maintaining homeostasis. The tenth cranial nerve, called the vagus nerve, is a key component in modulating cardiac activity as part of the PNS. The functioning of the vagal nerve can be altered through both internal factors and external reinforcing processes, such as early life stress, leading to varied patterns of ANS responsivity to stressors (Beauchaine 2015).
According to Porges’ polyvagal theory (Porges et al. 1996), emotion regulation abilities are indirectly linked to the functioning of the PNS. Although the stress response is activated by the SNS, the PNS must initially engage in vagal withdrawal to enable the “fight or flight” state. It is this vagal withdrawal that is theorized to proxy emotion regulation ability. Indeed, coordination of the PNS, SNS, and specific neural pathways is the foundation for self-regulation, as proposed by the model of neurovisceral integration (Thayer and Lane 2009). According to Thayer, neuroanatomical connections between the ANS and regions of the cortex and limbic system are significantly associated with emotional regulation. Common to both Thayer’s and Porges’ theories is the idea that effective functioning of the vagus nerve via the PNS serves as an indirect bio-marker of self-regulation ability. Thus, excessive or blunted withdrawal is indicative of a lack of stress response system regulation, which can lead to emotional reactivity and is associated with emotional dysregulation (Beauchaine 2015). In the empirical literature, vagal withdrawal is commonly operationalized by measuring heart rate variability reactivity (HRV-R).
HRV-R, CU, and Risk-Taking Behaviors
Individuals who display elevated levels of CU traits have deficits in affective processing, particularly in response to acute stress (Fanti et al. 2016). These affective processing problems are purported to reduce risk aversion and increase participation in risk behaviors such as abuse of alcohol or other drugs. Moreover, theories on biological sensitivity to context suggest that specific neurobiological systems may result in even more risk related to specific environmental input (Ellis et al., 2017). Based on biological sensitivity to context theory, variability in PNS activity, as indexed by HRV-R, can moderate individual reactivity to acute stress (Obradović et al. 2010). Excessive levels of HRV-R can be indicative of over-withdrawal of the parasympathetic system, resulting in less regulated responses to stress and greater risk for psychopathology and adjustment problems (Beauchaine et al. 2007; Obradović 2012). Hence, stress response dysregulation indicated by excessively high HRV-R may operate as a psychophysiological risk factor that potentiates the link between CU traits and attendant vulnerability for participation in risk behaviors.
The Present Study
A prevalent hypothesis in the developmental psychopathology literature suggests that personality traits, such as callous-unemotional, underlie the link between childhood adversity and the development of risk-taking behaviors in adolescence and young adulthood (Beauchaine et al. 2007; Obradović 2012). Further, biological sensitivity to context theories suggest that the neurobiology of stress reactivity may operate as a biologically embedded factor that moderates this developmental risk (Beauchaine 2015; Obradović et al. 2010). Little research, however, has examined the potential for HRV-R to moderate the paths linking exposure to CAN, CU traits, and AOD use problems. The present study is designed to address this gap. We obtained HRV-R during a manipulated social stress condition to test the hypothesis that high HRV-R can exacerbate the indirect link between child maltreatment and risk behaviors via CU traits. We hypothesized that (a) CAN would be significantly associated with higher levels of CU traits, (b) higher CU traits would be associated with increased AOD use problems, and (c) there would be an indirect effect from CAN to AOD use problems via increased levels of CU traits. Lastly, we hypothesized that excessive levels of HRV-R would exacerbate the association between CU traits and AOD use problems.
Methods
Participants and Procedures
Participants were 130 undergraduate students in a Southeastern U.S. public university (81% female; Mage = 20.72; 63.02% Caucasian). The average yearly family income bracket was $50,000 to $100,000. Eligibility criteria for study participation included being a student with no current or prior history of heart problems. The Institutional Review Board for ethical conduct in research reviewed and granted approval to this study, and informed consent was obtained from all individual participants included in the study. Participants completed a questionnaire using a computer in a research lab on campus.
Participants were attached to an electrocardiogram via dermal electrodes for the duration of the survey. One electrode was placed on each side of the bottom rib cage, each side of the clavicle, below the sternum, and the upper and lower spine. Biometric data were acquired using the BioLab software provided through MindWare Technologies. Acute stress was induced using the mental arithmetic protocol of the modified Trier Social Stress Test (Kirschbaum et al. 1993). In this task, participants were expected to participate in a five-minute mental arithmetic stress task in front of a peer-audience of trained research assistants selected from a body of students at the hosting university. Research assistants were instructed to remain neutral and give no feedback to the participant during the mental arithmetic performance task. Participants were asked to quickly and accurately answer increasingly difficult arithmetic questions verbally. To maximize stress, the difficulty of the tasked was tailored to the participants’ arithmetic level. At the end of the task, all participants were debriefed. This task has been shown to produce a significant physiological reaction (Berntson et al. 1996), and has been used extensively in research examining vagal tone and heart rate variability to assess physiological stress reactions.
Measures
Basal HRV and HRV Reactivity
HRV was used to index parasympathetic nervous system activity and was calculated using standard procedures and guidelines (Berntson et al. 1997). HRV data were digitized using the MindWare HRV 3.1.0 Software module (MindWare Technologies, Ltd., Gahanna, OH). Per the ECG signal, interbeat intervals (IBIs) were quantified in 120-s segments. Physiologically improbable IBIs were detected by MindWare software using the MAD/MED artifact detection algorithm (Berntson et al. 1990). Furthermore, trained research assistants used video recordings to cross-inspect and correct abnormal R-R intervals, such as inadvertent cardiac fluctuations and ectopic beats due to physical movement or breathing. The procedure of HRV data cleaning followed the instructions of MindWare Technologies (Gahanna, OH). Specifically, we deleted abnormal R beats and inserted midbeats. Sections with more than one third abnormal R-R intervals were excluded from data analyses.
After data cleaning, HRV was calculated as the natural log of the high-frequency power (.15–.40 Hz), a validated method for isolating the parasympathetic influence on the heart (Ernst et al. 1999). Mean values of HRV across segments were then calculated. Baseline HRV level was determined based on data obtained during a five-minute period in which participants answered non-stressful questionnaires. Overall, this approach accords with current guidelines on frequency-domain methods for heart rate variability analysis (Task Force of the European Society of Cardiology, 1996) and is well suited for short-term recordings.
In order to measure HRV reactivity, a residualized change score was created using baseline (measured 3 min after watching a relaxation video) and acute stress task HRV segments (equation below), allowing us to adjust for baseline differences in the computation of HRV reactivity. These segments of data were chosen based on pilot physiological data and participant feedback about their relaxation and acute stress experiences during the tasks. A lower HRV residualized change score indicates a decrease from baseline to the stress task (i.e., vagal withdrawal), and thus high levels of HRV reactivity may reflect emotional dysregulation in the form of emotional reactivity.
Child Abuse and Neglect
A sum score of five items from the Adverse Childhood Experiences Questionnaire (ACE; Felitti et al. 1998) was used to assess experiences of child abuse and neglect (i.e., physical abuse, sexual abuse, emotional abuse, physical neglect, and emotional neglect). Each item began with the stem, “While you were growing up, during your first 18 years of life…” Because ACE is a cumulative measure, internal reliability is not a meaningful index (Felitti et al. 1998). However, the questionnaire had satisfactory internal consistency (α = .62).
Callous-Unemotional Traits
CU traits were assessed using the Inventory of Callous-Unemotional Traits (Frick 2004). The ICU is a 24-item self-report instrument designed to assess callous-unemotional traits in adolescents and young adults and has shown acceptable validity and reliability in undergraduate samples (see Kimonis et al. 2013c). Three subscales were utilized in order to measure CU traits: callousness, uncaring, and unemotional. The overall measure had good internal consistency (α = .81).
AOD Use Problems
Alcohol use problems were assessed with ten items from the Alcohol Use Disorders Identification Test (AUDIT; Babor et al. 2001; α = .85). Drug use problems were assessed with 11 items from the Drug Use and Disorders Identification Test (DUDIT; Berman et al. 2005). Both the AUDIT and DUDIT have been found to have acceptable validity and reliability in undergraduate samples (Hildebrand and Noteborn 2015; Kokotailo et al. 2004).
Covariates
Due to their potential influence on our outcomes of interest, we controlled for participants’ gender, age, family income, and minority status, which were all self-reported. Gender was coded categorically (0 = Male, 1 = Female). Respondents reported on their family’s approximate total yearly income with a Likert-type scale from one (less than $20,000) to five (more than $100,000). Minority status was coded dichotomously according to how participants identified their race/ethnicity (1 = non-minority, 2 = minority).
Analytic Plan
Structural equation modeling (SEM) via Mplus version 7.3 (Muthén and Muthén 2010) was used to test the links between child abuse and neglect, CU traits, and substance use problems. The moderating role of HRV reactivity was examined using a latent variable interaction (Klein and Moosbrugger 2000). The moderated mediation was tested using the RMediation software, which produces a confidence interval for the product of two normal random variables using three methods: the distribution of the product of coefficients, Monte Carlo, and asymptotic normal theory with the multivariate-delta standard error method (Tofighi and MacKinnon 2011). In order to interpret the moderated mediation, the Johnson-Neyman technique was utilized, which identifies the range of values of the moderator for which the indirect effect was significant (Preacher et al. 2006).
Results
Descriptive statistics and bivariate correlations of study constructs are presented in Table 1, and distributions of CAN are presented in Tables 2 and 3. As expected, child abuse and neglect was significantly correlated with callousness and uncaring traits, and CU traits, in turn, were significantly correlated with drug and alcohol use problems. Approximately 23.8% of the sample had an ACE score of 1 or higher for the CAN items.
Table 1.
Bivariate correlations, means, and standard deviations of study variables (N = 130)
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Child abuse and neglect | – | ||||||||||
| 2. Callousness | .22* | – | |||||||||
| 3. Uncaring | .24** | .43** | – | ||||||||
| 4. Unemotional | .08 | .44** | .29** | – | |||||||
| 5. Alcohol use | .01 | .25** | .12 | .00 | – | ||||||
| 6. Drug use | .02 | .31** | .13 | .06 | .52** | – | |||||
| 7. ΔHRV | .14 | .15 | .05 | .01 | .08 | −.11 | – | ||||
| 8. Gender | .02 | −.32** | −.10 | −.27** | −.26** | −.15 | −.10 | – | |||
| 9. Age | −.06 | −.06 | .09 | −.16 | −.04 | −.01 | −.15 | .03 | – | ||
| 10. Minority Status | .13 | .05 | .22* | .15 | −.25** | −.10 | −.15 | .04 | −.04 | – | |
| 11. SES | .03 | −.01 | .04 | −.04 | .21 | .01 | .10 | −.03 | −.06 | −.39** | – |
| Mean | .42 | 10.15 | 6.11 | 9.07 | 4.82 | 1.35 | 1.35 | .82 | 20.72 | 1.37 | 3.84 |
| SD | .86 | 2.20 | 3.47 | 3.30 | 5.08 | 3.06 | 1.32 | .39 | 4.18 | .48 | 1.12 |
ΔHRV Residualized change score of heart rate variability. Gender coded as 0 = male, 1 = female. SES = Socio-economic status. SD Standard Deviation. *p < .05; **p < .01
Table 2.
Types of ACE by sex
| Male (%) | Female (%) | Total (%) | |
|---|---|---|---|
| None | 20 (83.3) | 79 (74.5) | 99 (76.2) |
| Verbal Abuse | 4 (16.7) | 15 (14.2) | 19 (14.6) |
| Physical Abuse | 2 (8.3) | 9 (8.5) | 11 (8.5) |
| Sexual Abuse | 1 (4.2) | 7 (6.6) | 8 (6.2) |
| Emotional Neglect | 2 (8.3) | 12 (11.3) | 14 (10.8) |
| Physical Neglect | 0 (0.0) | 2 (1.9) | 2 (1.5) |
| 24 (18.4) | 106 (81.5) | 130 |
Table 3.
Cumulative ACEs
| Male (%) | Female (%) | Total (%) | |
|---|---|---|---|
| 0 | 20 (83.3) | 79 (74.5) | 99 (76.2) |
| 1 | 2 (8.3) | 13 (12.3) | 15 (11.5) |
| 2 | 0 (0.0) | 11 (10.4) | 11 (8.5) |
| 3 | 1 (4.2) | 2 (1.9) | 3 (2.3) |
| 4 | 1 (4.2) | 1 (.9) | 2 (1.5) |
| 5 | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| 24 (18.4) | 106 (81.5) | 130 |
Measurement and Structural Equation Models
Confirmatory factor analysis was used to assess the latent factor of CU traits. The CU traits subscales (i.e., callousness, uncaring, unemotional) were used as indicators for the latent factor. Age, gender, family income, and minority status were included as covariates in this and subsequent analyses. Resulting model fit was good: χ2 (4) = 9.20, p = .06; CFI = .93; RMSEA = .10; SRMR = .05. All factor loadings were significant (p < .001) and larger than .50, confirming that each indicator was an appropriate component of the latent construct (Brown 2014).
SEM was used to examine the associations between CAN, CU traits, and AOD use problems. Model fit was good: χ2 (11) = 19.86, p = .05; CFI = .94; RMSEA = .08; SRMR = .06 (Brown 2015). Females reported lower CU traits (β = −.37, p < .001) compared to males. In addition, minorities (β = −.26, p < .01) reported lower alcohol use problems compared to non-minorities. Child abuse and neglect was associated with increased levels of CU traits (β = .27, p < .01), and higher CU traits were significantly associated with greater drug (β = .35, p < .01) and alcohol use (β = .23, p < .05) problems, after adjusting for variance associated with the direct effect of CAN on AOD use problems. Figure 1 and Table 4 presents the model evaluating the associations between CAN, CU traits, and AOD use problems.
Fig. 1.
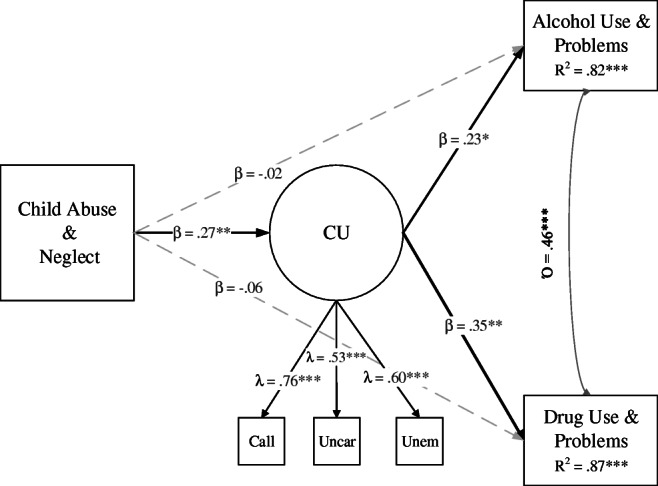
Mediation Model. Note. CU = Callous-unemotional traits; Call = Callousness, Uncar = Uncaring, Unem = Unemotional. Gender and minority status were controlled for. Covariates were removed for clarity. Model fit was very good: χ2 (11) = 19.86, p = .05; CFI = .94; RMSEA = .08; SRMR = .06. * p < .05; ** p < .01; ***p < .001
Table 4.
Parameter estimates of direct and indirect effects (N = 130)
| Measurement Model | B (SE) | β | 95% CI |
|---|---|---|---|
| CU → Callousness | 1.00 (.00) | .76 | [1.00, 1.00]*** |
| CU → Uncaring | 1.11 (.26) | .53 | [.61, 1.61]*** |
| CU → Unemotional | 1.18 (.28) | .60 | [.63, 1.74]*** |
| Mediation Model | B (SE) | β | 95% CI |
| CAN → CU | .59 (.20) | .27 | [.20, .98]** |
| CU → Alcohol | .62 (.30) | .23 | [.04, 1.20]* |
| CU → Drug | .56 (.19) | .35 | [.18, .94]** |
| CAN → Alcohol | −.09 (.51) | −.02 | [−1.09, .91] |
| CAN → Drug | −.21 (.32) | −.06 | [−.83, .42] |
| Covariates | |||
| Minority → Alcohol | −2.73 (.86) | −.26 | [−4.41, −1.05]*** |
| Gender → Alcohol | −2.23 (1.18) | −.17 | [−4.54, .07] |
| Minority → Drug | −.78 (.54) | −.12 | [−1.83, .27] |
| Gender → Drug | −.13 (.74) | −.02 | [−1.58, 1.32] |
| Gender → CU | −1.79 (.45) | −.37 | [−2.67, −.91]*** |
| Moderated Mediation Model | B (SE) | β | 95% CI |
| CAN → CU | .68 (.19) | .34 | [.32, 1.05]*** |
| CU → Alcohol | 1.14 (.61) | .44 | [−.05, 2.34] |
| ΔHRV → Alcohol | −.50 (.68) | −.14 | [−1.82, .82] |
| CU*ΔHRV → Alcohol | −.33 (.29) | −.17 | [−.89, .24] |
| CAN → Alcohol | −.40 (.56) | −.08 | [−1.40, .69] |
| CU → Drug | 1.17 (.46) | .67 | [.27, 2.06]* |
| ΔHRV → Drug | −.99 (.37) | −.42 | [−1.73, −.25]** |
| CU*ΔHRV → Drug | −.39 (.15) | −.29 | [−.68, −.09]* |
| CAN → Drug | −.08 (.36) | −.02 | [−.78, .62] |
| Covariates | |||
| Minority → Alcohol | −2.08 (.79) | −.22 | [−3.62, −.54]** |
| Gender → Alcohol | −2.08 (1.45) | −.17 | [−4.95, .80] |
| Minority → Drug | −.65 (.55) | −.10 | [−1.73, .42] |
| Gender → Drug | −.27 (.95) | −.03 | [−2.13, 1.60] |
| Gender → CU | −1.67 (.57) | −.35 | [−2.78, −.56]** |
| Conditional Indirect Effect | |||
| CAN → CU*ΔHRV → Drug | −.26 (.13) | −.11 | [−.55, −.05]* |
ΔHRV Residualized change score of heart rate variability; CAN Child abuse and neglect; CU Callous-unemotional traits; SE Standard Error; CI Confidence Interval for unstandardized coefficients.
* p < .05; ** p < .01; *** p < .001. Gender was coded as 0 = Male, 1 = Female
Testing for Moderation
The moderating role of HRV reactivity on the paths from CU traits to drug and alcohol use problems was tested. ΔHRV was introduced into the model, and the prediction of alcohol and drug use problems by the interaction between the latent factor of CU traits and ΔHRV was tested. Results indicated that ΔHRV had a direct negative effect on drug use problems (β = −.42, p < .01) but was unrelated to alcohol use problems (β = −.14, p = .47). ΔHRV moderated the link between CU traits and drug use (β = −.29, p < .05) but not alcohol use problems (β = −.17, p = .27).
Examining Moderated Mediation
The distribution of the product of coefficients method was used to assess for the moderating role of HRV reactivity on the path from childhood maltreatment to AOD use problems via CU traits. Results indicated that the mediation was significant and conditional on the moderation effect (α*β = −.26, p < .05; Fig. 2 and Table 4). The conditional indirect effect was probed using the Johnson-Neyman technique (Preacher et al. 2006). Figure 3 suggests that for participants with higher levels of HRV reactivity (indicated by lower ΔHRV), the indirect effect of CAN on drug use problems through callous-unemotional traits was significant.
Fig. 2.

Moderated Mediation Model. Note. HRV = Residualized change score of heart rate variability. CU = Callous-unemotional traits; Call = Callousness, Uncar = Uncaring, Unem = Unemotional. HRV X CU is a latent variable interaction. Gender and minority status were controlled for. Covariates were removed for clarity. * p < .05; ** p < .01; ***p < .001
Fig. 3.

Johnson-Neyman Plot of the Indirect Effect of HRV Reactivity X Callous-Unemotional Traits on Drug Use Problems. Note. ΔHRV = Residualized change score of heart rate variability. The shadowed region indicates that for participants with higher levels of HRV reactivity (i.e. lower ΔHRV scores), the indirect effect of child maltreatment on drug use problems through callous-unemotional traits is significant
Discussion
Young adults in college who report CAN are at significant risk for substance use problems, partly due to problems in self-regulation (Blair et al. 2014). The present study showed that the severity of CAN experiences was indirectly associated with AOD use problems via elevations in CU traits. Further, stress response dysregulation, indexed by high HRV-R, exacerbated theindirect link between CAN and drug but not alcohol use problems via CU traits. This is consistent and elaborated on previous research that has shown an indirect connection between CAN and AOD use problems via CU trait severity among college students (Carlson et al. 2015). The current study expands on previous research by using psychophysiological data to demonstrate that high levels of HRV-R intensified the indirect link between CU severity and drug use. These findings bear significant implications for the development of preventive intervention programs to reduce the risk for drug use among young adults who report adverse childhood experiences.
Notably, our investigation supported the hypothesis that elevated CU traits are associated with increased AOD use problems. This finding corroborates research suggesting that antisocial youths with CU traits may have deficits in emotional processing and thus, increased propensity for risk behaviors (Kimonis et al. 2013b; Marsh et al. 2008; Pardini et al. 2003). Accordingly, youths with elevated CU traits appear to exhibit a temperament characterized by deficits in emotional responses to stress and fear (Woodworth & Waschbusch, 2008), leading to less risk aversion and participation in more risk behaviors (Fanti et al. 2013; Humphreys and Lee 2011). Youths with a blunted emotional response may also be more impulsive regarding attention-seeking behaviors, such as substance use during college. Indeed, growing literature reports associations between child abuse, personality traits, and psychopathology (Fanti et al. 2013; Oshri et al. 2015; Rogosch and Cicchetti 2004).
Consistent with biological sensitivity to context theories and our hypothesis, the paths from CAN to AOD use problems use changed as a function of HRV reactivity. These results suggest that the risk incurred by CU traits intensify among youth with higher stress reactivity patterns. Similarly, the finding that excessive HRV reactivity exacerbates youth’s risks seems to be aligned with the vigilant pattern (hyper-reactivity) well, documented by research models (Such as the adaptive calibration model) of the biological sensitivity to context (Del Giudice et al. 2011). For example, a recent study found that the vigilant pattern is associated with youth’s externalizing problems (Ellis et al. 2017) which significantly associated with substance use problems across the lifespan. These results suggest that the sequelae of risky personality traits, such as CU traits, can be modified by a young adults’ self-regulation in response to socially stressful stimuli.
Young adults with excessive stress response reactivity were at significant risk for drug but not alcohol use problems. Although we did not hypothesize a differential effect of HRV reactivity on alcohol compared to drug abuse, this difference might further suggest that the link between CU and alcohol abuse does not depend on emotional processing during social stress. The disparity in the results for drug versus alcohol use problems may reflect the fact that motives for drinking and doing drugs are different for college students. Alcohol use problems are more normative in college populations, and the motivation for drinking might not be strongly associated with social stress, but with coping (Park & Levenson, 2002) or conduct problems (Verweij et al., 2016).
As young adults leave their nuclear families, they enter into a developmental stage in which peer relations are central and have more influence on risk-taking behaviors (Albert, Chein, & Steinberg, 2013). In the present study, the link between CU and drug use was exacerbated by high levels of HRV reactivity during social stress. These findings bear important implications for substance use prevention efforts among young adults in a college environment. Young adults in college are surrounded by a social environment that is fraught with the normative use of substances. The ability to regulate emotions associated with social stress might be critical to buffer such risky social contexts. Therefore, the efficacy of treatment aimed at preventing substance use among young adults may be improved by targeting peers (Silva, Chein, & Steinberg, 2016) or emotion regulation strategies (Houck et al., 2016). Additionally, substance abuse treatment programs for college students may benefit by incorporating psychoeducation on self-regulation strategies.
The findings of the current study corroborate a growing body of research on the impact of early life stress on risk behaviors via emotion regulation (Oshri et al. 2018). Based on the adaptive calibration model of stress (Del Giudice et al. 2011), personality traits are believed to serve as stress response systems that developed to adapt to adverse environmental conditions, such as the context of child abuse and neglect. The results also provide support to theories on the role of emotions in risk behaviors. For example, the Somatic Marker Hypothesis (SMH; Bechara & Damasio, 2005) suggests that the decision to take risks is significantly affected by emotional processing. When weighing the future consequences of an action, executive functions must trigger somatic responses about possible future consequences (Reimann & Bechara, 2010), which can be undermined among maltreated youth. The SMH proposes that risk-taking is rooted in one’s ability to process emotions; it rests on the assumption that decision-making is a process that is regulated by emotionally driven marker signals that arise through bio-regulatory processes. In the present study, emotion regulation problems, indexed by high HRV-R, are shown to be associated with intensified engagement in drug use behaviors. Hence, risk-taking behaviors are purported to be exacerbated by bio-regulatory systems of emotion regulation that signal emotional cues about the anticipated consequences of taking risks. The present study provides further support to the SMH hypothesis by showing that emotion dysregulation can serve as an important neurobiological vulnerability for risk-taking behaviors, although this was found for drug abuse and not alcohol abuse.
Limitations
Several limitations and strengths of the current study should be noted. First, the data utilized in this study are cross-sectional. Hence, any causal inferences should be limited. The examined traits may lead to participation in risk behaviors, while the inverse might also be true. However, this study supports the need for longitudinal and experimental studies to investigate trait development and its role in the mechanisms that mediate the link between diverse types of child abuse and neglect and risk behaviors among young adults. Although the study uses self-report measures, the study also utilizes an experimental procedure to induce social stress and record HRV reactivity using heart rate variability data. Moreover, the study is limited by the fact that the ACE measure used does not specify whether the CAN occurred within or outside of the family. This is especially relevant to sexual abuse, which can occur outside of the immediate family, and it highlights the need for increased specificity when measuring ACEs via self-report. In conclusion, the current study suggests that the association between child abuse and neglect and AOD use problems is mediated via personality traits and moderated by emotion regulation. Therefore, targeting self-regulation in young adults who self-report child abuse and neglect histories will improve intervention efficacy and orient prevention and intervention to vulnerable young adults.
Acknowledgments
Funding: This work was partially supported by NIH through NIDA (5K01DA045219-02) grant awarded to Dr. Assaf Oshri.
Compliance with Ethical Standards
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional research committee, and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards.
Informed Consent
Informed consent was obtained from all individual adult participants included in the study; assent was obtained from children.
Conflict of Interest
All authors of the manuscript declare that they have no potential conflicts of interest.
Footnotes
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
References
- Babor, T. F., Higgins-Biddle, J. C., Saunders, J. B., Monteiro, M. G., & Organization, W. H. (2001). AUDIT: The alcohol use disorders identification test: Guidelines for use in primary health care.
- Beauchaine TP. Future directions in emotion dysregulation and youth psychopathology. Journal of Clinical Child & Adolescent Psychology. 2015;44(5):875–896. doi: 10.1080/15374416.2015.1038827. [DOI] [PubMed] [Google Scholar]
- Beauchaine TP, Gatzke-Kopp L, Mead HK. Polyvagal theory and developmental psychopathology: Emotion dysregulation and conduct problems from preschool to adolescence. Biological Psychology. 2007;74(2):174–184. doi: 10.1016/j.biopsycho.2005.08.008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berman AH, Bergman H, Palmstierna T, Schlyter F. Evaluation of the drug use disorders identification test (DUDIT) in criminal justice and detoxification settings and in a Swedish population sample. European Addiction Research. 2005;11(1):22–31. doi: 10.1159/000081413. [DOI] [PubMed] [Google Scholar]
- Berntson GG, Quigley KS, Jang JF, Boysen ST. An approach to artifact identification: Application to heart period data. Psychophysiology. 1990;27(5):586–598. doi: 10.1111/j.1469-8986.1990.tb01982.x. [DOI] [PubMed] [Google Scholar]
- Berntson GG, Cacioppo JT, Fieldstone A. Illusions, arithmetic, and the bidirectional modulation of vagal control of the heart. Biological Psychology. 1996;44(1):1–17. doi: 10.1016/S0301-0511(96)05197-6. [DOI] [PubMed] [Google Scholar]
- Berntson GG, Thomas Bigger J, Eckberg DL, Grossman P, Kaufmann PG, Malik M, Stone PH. Heart rate variability: Origins, methods, and interpretive caveats. Psychophysiology. 1997;34(6):623–648. doi: 10.1111/j.1469-8986.1997.tb02140.x. [DOI] [PubMed] [Google Scholar]
- Blair RJR, Leibenluft E, Pine DS. Conduct disorder and callous–unemotional traits in youth. New England Journal of Medicine. 2014;371(23):2207–2216. doi: 10.1056/NEJMra1315612. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Brown, T. A. (2014). Confirmatory factor analysis for applied research. New York: Guilford Publications.
- Brown, T. A. (2015). Confirmatory factor analysis for applied research. Guilford Publications.
- Carlson M, Oshri A, Kwon J. Child maltreatment and risk behaviors: The roles of callous/unemotional traits and conscientiousness. Child Abuse & Neglect. 2015;50:234–243. doi: 10.1016/j.chiabu.2015.07.003. [DOI] [PubMed] [Google Scholar]
- Dackis MN, Rogosch FA, Cicchetti D. Child maltreatment, callous–unemotional traits, and defensive responding in high-risk children: An investigation of emotion-modulated startle response. Development and Psychopathology. 2015;27(4pt2):1527–1545. doi: 10.1017/S0954579415000929. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Del Giudice M, Ellis BJ, Shirtcliff EA. The adaptive calibration model of stress responsivity. Neuroscience & Biobehavioral Reviews. 2011;35(7):1562–1592. doi: 10.1016/j.neubiorev.2010.11.007. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Ellis BJ, Oldehinkel AJ, Nederhof E. The adaptive calibration model of stress responsivity: An empirical test in the tracking Adolescents' individual lives survey study. Development and Psychopathology. 2017;29(3):1001–1021. doi: 10.1017/S0954579416000985. [DOI] [PubMed] [Google Scholar]
- Ernst JM, Litvack DA, Lozano DL, Cacioppo JT, Berntson GG. Impedance pneumography: Noise as signal in impedance cardiography. Psychophysiology. 1999;36(3):333–338. doi: 10.1017/S0048577299981003. [DOI] [PubMed] [Google Scholar]
- Fang X, Corso PS. Child maltreatment, youth violence, and intimate partner violence: Developmental relationships. American Journal of Preventive Medicine. 2007;33(4):281–290. doi: 10.1016/j.amepre.2007.06.003. [DOI] [PubMed] [Google Scholar]
- Fanti KA, Demetriou CA, Kimonis ER. Variants of callous-unemotional conduct problems in a community sample of adolescents. Journal of Youth and Adolescence. 2013;42(7):964–979. doi: 10.1007/s10964-013-9958-9. [DOI] [PubMed] [Google Scholar]
- Fanti KA, Panayiotou G, Lombardo MV, Kyranides MN. Unemotional on all counts: Evidence of reduced affective responses in individuals with high callous-unemotional traits across emotion systems and valences. Social Neuroscience. 2016;11(1):72–87. doi: 10.1080/17470919.2015.1034378. [DOI] [PubMed] [Google Scholar]
- Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, Marks JS. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults: The adverse childhood experiences (ACE) study. American Journal of Preventive Medicine. 1998;14(4):245–258. doi: 10.1016/S0749-3797(98)00017-8. [DOI] [PubMed] [Google Scholar]
- Frick, P. J. (2004). The inventory of callous-unemotional traits. Unpublished rating scale.
- Frick PJ, White SF. Research review: The importance of callous-unemotional traits for developmental models of aggressive and antisocial behavior. Journal of Child Psychology and Psychiatry. 2008;49(4):359–375. doi: 10.1111/j.1469-7610.2007.01862.x. [DOI] [PubMed] [Google Scholar]
- Frick PJ, Ray JV, Thornton LC, Kahn RE. Can callous-unemotional traits enhance the understanding, diagnosis, and treatment of serious conduct problems in children and adolescents? A comprehensive review. Psychological Bulletin. 2014;140(1):1–57. doi: 10.1037/a0033076. [DOI] [PubMed] [Google Scholar]
- Hawes, S. W., Waller, R., Thompson, W. K., Hyde, L. W., Byrd, A. L., Burt, S. A., . . . Gonzalez, R. (2019). Assessing callous-unemotional traits: Development of a brief, reliable measure in a large and diverse sample of preadolescent youth. Psychological Medicine, 1–9. [DOI] [PMC free article] [PubMed]
- Hildebrand, M., & Noteborn, M. G. (2015). Exploration of the (interrater) reliability and latent factor structure of the Alcohol Use Disorders Identification Test (AUDIT) and the Drug Use Disorders Identification Test (DUDIT) in a sample of Dutch probationers. Substance use & misuse, 50(10), 1294–1306 [DOI] [PubMed]
- Humphreys KL, Lee SS. Risk taking and sensitivity to punishment in children with ADHD, ODD, ADHD+ ODD, and controls. Journal of Psychopathology and Behavioral Assessment. 2011;33(3):299–307. doi: 10.1007/s10862-011-9237-6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kim J, Williams S. Linking childhood maltreatment to substance use in college students: The mediating role of self-worth contingencies. Journal of Aggression, Maltreatment & Trauma. 2009;18(1):88–105. doi: 10.1080/10926770802616399. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kimonis ER, Cross B, Howard A, Donoghue K. Maternal care, maltreatment and callous-unemotional traits among urban male juvenile offenders. Journal of Youth and Adolescence. 2013;42(2):165–177. doi: 10.1007/s10964-012-9820-5. [DOI] [PubMed] [Google Scholar]
- Kimonis ER, Fanti KA, Isoma Z, Donoghue K. Maltreatment profiles among incarcerated boys with callous-unemotional traits. Child Maltreatment. 2013;18(2):108–121. doi: 10.1177/1077559513483002. [DOI] [PubMed] [Google Scholar]
- Kimonis, E. R., Branch, J., Hagman, B., Graham, N., & Miller, C. (2013c). The psychometric properties of the Inventory of Callous–Unemotional Traits in an undergraduate sample. Psychological Assessment, 25(1), 84. [DOI] [PubMed]
- Kirschbaum, C., Pirke, K. M., & Hellhammer, D. H. (1993). The ‘Trier Social Stress Test’–a tool for investigating psychobiological stress responses in a laboratory setting. Neuropsychobiology, 28(1-2), 76–81. [DOI] [PubMed]
- Klein A, Moosbrugger H. Maximum likelihood estimation of latent interaction effects with the LMS method. Psychometrika. 2000;65(4):457–474. doi: 10.1007/BF02296338. [DOI] [Google Scholar]
- Kokotailo, P. K., Egan, J., Gangnon, R., Brown, D., Mundt, M., & Fleming, M. (2004). Validity of the alcohol use disorders identification test in college students. Alcoholism: Clinical and Experimental Research, 28(6), 914–920. [DOI] [PubMed]
- Loney BR, Frick PJ, Clements CB, Ellis ML, Kerlin K. Callous-unemotional traits, impulsivity, and emotional processing in adolescents with antisocial behavior problems. Journal of Clinical Child and Adolescent Psychology. 2003;32(1):66–80. doi: 10.1207/S15374424JCCP3201_07. [DOI] [PubMed] [Google Scholar]
- Marsh AA, Finger EC, Mitchell DG, Reid ME, Sims C, Kosson DS, Blair R. Reduced amygdala response to fearful expressions in children and adolescents with callous-unemotional traits and disruptive behavior disorders. American Journal of Psychiatry. 2008;165(6):712–720. doi: 10.1176/appi.ajp.2007.07071145. [DOI] [PubMed] [Google Scholar]
- Muthén, L. K., & Muthén, B. O. (2010). Mplus User's Guide: Statistical Analysis with Latent Variables: User'ss Guide: Muthén & Muthén.
- Obradović J. How can the study of physiological reactivity contribute to our understanding of adversity and resilience processes in development? Development and Psychopathology. 2012;24(02):371–387. doi: 10.1017/S0954579412000053. [DOI] [PubMed] [Google Scholar]
- Obradović, J., Bush, N. R., Stamperdahl, J., Adler, N. E., & Boyce, W. T. (2010). Biological sensitivity to context: The interactive effects of stress reactivity and family adversity on socioemotional behavior and school readiness. Child development, 81(1), 270–289. [DOI] [PMC free article] [PubMed]
- Oshri A, Rogosch FA, Burnette ML, Cicchetti D. Developmental pathways to adolescent cannabis abuse and dependence: Child maltreatment, emerging personality, and internalizing versus externalizing psychopathology. Psychology of Addictive Behaviors. 2011;25(4):634–644. doi: 10.1037/a0023151. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oshri A, Rogosch FA, Cicchetti D. Child maltreatment and mediating influences of childhood personality types on the development of adolescent psychopathology. Journal of Clinical Child & Adolescent Psychology. 2013;42(3):287–301. doi: 10.1080/15374416.2012.715366. [DOI] [PubMed] [Google Scholar]
- Oshri A, Sutton TE, Clay-Warner J, Miller JD. Child maltreatment types and risk behaviors: Associations with attachment style and emotion regulation dimensions. Personality and Individual Differences. 2015;73:127–133. doi: 10.1016/j.paid.2014.09.015. [DOI] [Google Scholar]
- Oshri A, Liu S, Duprey EB, MacKillop J. Child maltreatment, delayed reward discounting, and alcohol and other drug use problems: The moderating role of heart rate variability. Alcoholism: Clinical and Experimental Research. 2018;42(10):2033–2046. doi: 10.1111/acer.13858. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pardini DA, Lochman JE, Frick PJ. Callous/unemotional traits and social-cognitive processes in adjudicated youths. Journal of the American Academy of Child & Adolescent Psychiatry. 2003;42(3):364–371. doi: 10.1097/00004583-200303000-00018. [DOI] [PubMed] [Google Scholar]
- Porges SW. Orienting in a defensive world: Mammalian modifications of our evolutionary heritage. A polyvagal theory. Psychophysiology. 1995;32(4):301–318. doi: 10.1111/j.1469-8986.1995.tb01213.x. [DOI] [PubMed] [Google Scholar]
- Porges SW, Doussard-Roosevelt JA, Portales AL, Greenspan SI. Infant regulation of the vagal “brake” predicts child behavior problems: A psychobiological model of social behavior. Developmental Psychobiology. 1996;29(8):697–712. doi: 10.1002/(SICI)1098-2302(199612)29:8<697::AID-DEV5>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- Preacher, K. J., Curran, P. J., & Bauer, D. J. (2006). Computational tools for probing interactions in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of educational and behavioral statistics, 31(4), 437–448.
- Rogosch FA, Cicchetti D. Child maltreatment and emergent personality organization: Perspectives from the five-factor model. Journal of Abnormal Child Psychology. 2004;32(2):123–145. doi: 10.1023/B:JACP.0000019766.47625.40. [DOI] [PubMed] [Google Scholar]
- Thayer, J. F., & Lane, R. D. (2009). Claude Bernard and the heart–brain connection: Further elaboration of a model of neurovisceral integration. Neuroscience & Biobehavioral Reviews, 33(2), 81–88. [DOI] [PubMed]
- Tofighi D, MacKinnon DP. RMediation: An R package for mediation analysis confidence intervals. Behavior Research Methods. 2011;43(3):692–700. doi: 10.3758/s13428-011-0076-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Zapolski TC, Cyders MA, Smith GT. Positive urgency predicts illegal drug use and risky sexual behavior. Psychology of Addictive Behaviors. 2009;23(2):348–354. doi: 10.1037/a0014684. [DOI] [PMC free article] [PubMed] [Google Scholar]