

Abstract
Objectives
The aims of the study are to describe the injury patterns among recreational skiers and snowboarders in China and to provide primary data to guide the reconstruction of regional healthcare facilities to deal with the increasing number of participants in snow sports.
Design
Retrospective cross-sectional study.
Methods
A retrospective study was performed in Wanlong Ski Resort in Chongli, China. Data of all injured skiers and snowboarders treated in the resort clinic during the 2018–2019 season were collected. Patients’ information, including sex, age, equipment, skill level and injured body part, was analysed.
Results
A total of 753 sports injuries were recorded. The estimated incidence of injury was 1.98 per 1000 skier days. 453 cases (60.2%) were associated with skiing. The mean age of skiers was older than snowboarders (35.1±14.5 vs 29.0±8.9, p<0.01). Injury not involving others constituted 67.9% of all injuries. The most common injured body part among skiers was lower extremity, contrary to injury in the upper extremity among snowboarders. Head and cervical injury was identified in 13.7% of skiers and 13.6% of snowboarders.
Conclusion
The incidence of skiing/snowboarding injury in China was similar to other countries. Injury pattern differed among different sports and causes of injury.
Keywords: sports medicine, public health, orthopaedic sports trauma
Strengths and limitations of this study.
The present study is the first epidemiological study to investigate injury patterns in a Chinese ski resort.
Severity of injury and accurate diagnosis were not recorded and patients were not followed up for prognosis.
The incidence of injury may be underestimated because patients might visit local or tertiary hospitals instead of the resort clinic or did not receive any medical help for mild injuries.
Introduction
Skiing and snowboarding are popular winter sports worldwide but carry a substantial risk of sports injuries, with reported incidence of 0.5–1.35 injuries per 1000 skier/snowboarder days among recreational skiers/snowboarders1–3 and 6.9 injuries per 1000 runs (or 26.8 injuries per 100 athletes per season)4 among professional alpine skiers in recent years. During the latest Winter Olympic Games in PyeongChang, 12% of athletes incurred at least one injury, equivalent to 12.6 injuries per 100 athletes over a 17-day period.5
Since Beijing was selected to host the 2022 Winter Olympics, the skiing and snowboarding population in China has risen from 8 million in 2015 to 13.2 million in 2018 (WuBin, 2019 China Ski Industry White Book, 2019). Large-scale ski resorts in China are often located in areas remote from major cities, where medical capacity cries for improvement in order to accept and manage large number of winter sports injuries and manage severe injuries.
The aims of this study are to describe the injury patterns among recreational skiers and snowboarders in China by investigating the largest ski resort in the host city of the 2022 Winter Olympic Games and to provide primary data to guide the reconstruction of local hospitals to deal with the increasing number of participants in snow sports.
Patients and methods
Data for this retrospective study were collected from the resort clinic of the Wanlong Ski Resort in Chongli during the 2018–2019 ski season. The Wanlong Ski Resort is a destination ski resort in Northern China which has various terrains and has the largest number of annual visits. The resort clinic is staffed by a registered general practitioner and a nurse and provides primary care to all injured visitors, whether self-presented or sent by patrols. The clinic is also responsible for treating mild injuries, transferring patients to local hospitals and carrying out basic life support for life-threatening injuries. The 2018–2019 season in Wanlong Ski Resort lasted for 158 days, from 1 November 2018 to 7 April 2019. A total of 388 606 visits (379 503 skier days) were recorded.
Besides patients’ sex and age information, we also recorded equipment, skill level, date and time of injury, cause of injury, slope difficulty and injured body part. Equipment was classified into skis and snowboards. Special equipment such as cross-country skis and skiboards is rare in China and has not been seen in recorded injured people. Patients were classified according to self-reported years of participation in skiing and snowboarding: beginner (first season), medium (1–5 years), advanced (5–10 years) and expert (≥10 years). Date of injury was divided into weekdays and weekends/holidays according to the Chinese government holiday arrangement. Wanlong Ski Resort’s business hours start from 08:00 to 16:00, so we split the time of injury into four periods of 2 hours each, morning (first 2 hours of business), noon, afternoon and late afternoon (last 2 hours of business). We summarised causes of injury into two types according to the subjective description of the scene of injury: not involving others, defined as falling or crashing without any body contact with others; and involving others, defined as crashing that involves two or more people. Slope difficulty was categorised into beginner trail, medium trail and advanced trail according to the official data of slope inclination angle. Injured body parts were categorised into the following four anatomical body regions: (1) head/cervical, (2) torso, (3) upper extremity and (4) lower extremity. Acromioclavicular joint injuries were classified as upper limb injury, while other clavicle injuries were classified as torso injury.6 Injuries involving the gluteal region were classified as torso injury. Whether patients have multipart injuries was also recorded, while each injured body part was counted in one of the above groups. The relationship between injured body part and sex, age, equipment and cause of injury was further determined by subgroup analysis.
Informed consent was waived considering that the study was epidemiological and anonymous.
Statistical analysis
All statistical analyses were performed with SPSS V.24.0. Continuous variables were presented as mean and SD, while categorical data were presented as frequency count and percentages. For comparison between subgroups, χ2 test was used for categorical variables and Student’s t-test was used for continuous variables. Where there are missing data, the available case was analysed to determine the difference between groups. P<0.05 was considered to indicate statistical significance.
Results
During the study period, there were 388 606 visits (379 503 skier days) and 753 cases of injury recorded in Wanlong Ski Resort. The estimated incidence of injury was 1.98 per 1000 skier days.
Features of injury
The mean age of injured visitors was 32.5±12.9 years (range 3–73 years). Paediatric patients under 15 years old took up 9.3% while senior patients (over the age of 60) took up 3.0% of all injured population. The number of male patients was twice as female patients. Among the injuries, 453 cases (60.2%) were associated with skiing. Table 1 shows more detailed demographic and sports-related profiles of these injuries.
Table 1.
Demographic and sports-related information of the injured population
| n (%) | |
| Sex | |
| Male | 475 (63.3) |
| Female | 278 (36.7) |
| Age (years) | |
| <15 | 68 (9.3) |
| 15–60 | 643 (87.7) |
| >60 | 22 (3.0) |
| Equipment | |
| Ski | 453 (60.6) |
| Snowboard | 294 (39.4) |
| Skill level | |
| Beginner | 211 (29.5) |
| Medium | 246 (34.0) |
| Advanced | 122 (22.8) |
| Expert | 64 (13.7) |
| Slope difficulty | |
| Beginner trail | 111 (15.3) |
| Medium trail | 206 (26.5) |
| Advanced trail | 425 (58.1) |
The 2018–2019 season in Wanlong Ski Resort consisted of 107 weekdays and 51 weekends/holidays according to the Chinese government arrangement. The average daily number of injuries was 3.38 on weekdays and 7.65 on weekends/holidays. A peak of paediatric cases was noted in January and February (figure 1). In a day, the percentage of injury that occurred in the morning, noon, afternoon and late afternoon was 9.7%, 31.6%, 22.0% and 36.7%, respectively.
Figure 1.
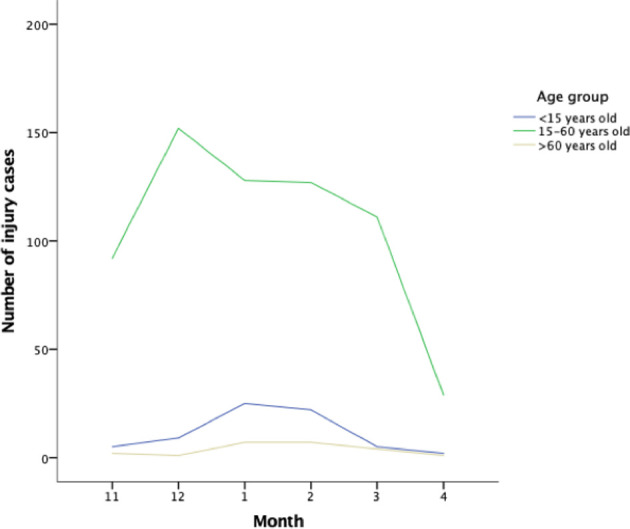
Number of injury cases in different age groups during the 2018–2019 season.
Accidents not involving other skiers took up 67.9% of all injuries. The most common injured body parts were upper (28.4%) and lower (37.6%) limbs, followed by head and cervical injury (13.1%).
Injury pattern in subgroups
The mean age of skiers was 35.1±14.5 years, whereas the mean age of snowboarders was 29.0±8.9 years (p<0.01). There was no significant difference in the sex profile between skiers and snowboarders.
The injured body parts showed different patterns between skiers and snowboarders. More than half of the skier patients sustained lower extremity injuries, while the most common injury among snowboarders was upper extremity injury. Head and cervical injury was identified in 13.7% of skiers and 13.6% of snowboarders. Multipart injury took up 5.3% of injuries among skiers and 3.4% among snowboarders (table 2). The cause of injury was also found to be related to the injured body parts in both skiers and snowboarders. Head injury took up a significantly higher rate in accidents involving others. In skiers, lower extremity injury was the most common injury whether the accidents involved others or not. However, the rate of lower extremity was significantly higher in accidents not involving others (table 3). In snowboarders, head, cervical and torso injuries took up a greater portion in accidents involving others (table 4). The correlation between age, sex, skill level and injured body parts was not significant (online supplemental tables 1–6).
Table 2.
Details of injured skiers and snowboarders
| Skiers (n=453) |
Snowboarders (n=294) |
P value | |
| Sex, n (%) | |||
| Male | 281 (63.3) | 184 (62.6) | 0.846 |
| Female | 163 (36.7) | 110 (37.4) | |
| Age (years), n (%) | |||
| <15 | 44 (10.3) | 22 (7.5) | <0.01* |
| 15–60 | 363 (84.6) | 270 (92.5) | |
| >60 | 22 (5.1) | 0 (0) | |
| Skill level, n (%) | |||
| Beginner | 110 (29.5) | 101 (37.5) | <0.01* |
| Medium | 127 (34.0) | 118 (43.9) | |
| Advanced | 85 (22.8) | 37 (13.8) | |
| Expert | 51 (13.7) | 13 (4.8) | |
| Date of injury, n (%) | |||
| Weekdays | 223 (50.2) | 134 (45.7) | 0.232 |
| Weekends/holidays | 221 (49.8) | 159 (54.3) | |
| Time of injury, n (%) | |||
| Morning | 44 (10.1) | 28 (9.9) | 0.466 |
| Noon | 137 (31.6) | 89 (31.3) | |
| Afternoon | 86 (19.8) | 69 (24.3) | |
| Late afternoon | 167 (38.5) | 98 (34.5) | |
| Slope difficulty, n (%) | |||
| Beginner trail | 67 (15.3) | 42 (14.4) | 0.868 |
| Medium trail | 116 (26.5) | 82 (28.2) | |
| Advanced trail | 254 (58.1) | 167 (57.4) | |
| Cause of injury, n (%) | |||
| Involving others | 153 (32.5) | 97 (30.6) | 0.680 |
| Not involving others | 291 (67.5) | 197 (69.4) | |
| Injured body part, n (%) | |||
| Head and cervical | 57 (13.7) | 36 (13.6) | <0.01* |
| Torso | 83 (19.9) | 63 (23.8) | |
| Upper extremity | 79 (18.9) | 125 (47.2) | |
| Lower extremity | 222 (53.2) | 50 (18.9) | |
| Multipart | 22 (5.3) | 9 (3.4) |
* The data has significant difference between groups.
Table 3.
Relationship between cause of injury and injured body part in skiers
| Injury not involving others, n (%) (n=291) |
Injury involving others, n (%) (n=126) |
P value | |
| Head and cervical | 21 (7.2) | 36 (28.6) | <0.01 |
| Torso | 54 (18.6) | 29 (23.0) | |
| Upper extremity | 53 (18.2) | 26 (20.6) | |
| Lower extremity | 172 (59.1) | 50 (49.7) | |
| Multipart injury | 9 (3.1) | 13 (10.3) |
Table 4.
Relationship between cause of injury and injured body part in snowboarders
| Injury not involving others, n (%) (n=197) |
Injury involving others, n (%) (n=68) |
P value | |
| Head and cervical | 17 (8.6) | 19 (27.9) | <0.01 |
| Torso | 39 (19.8) | 24 (35.3) | |
| Upper extremity | 107 (54.3) | 18 (26.5) | |
| Lower extremity | 37 (18.8) | 13 (19.1) | |
| Multipart injury | 3 (1.5) | 6 (8.8) |
bmjopen-2020-037834supp001.pdf (28.7KB, pdf)
Discussion
We found that the incidence of sports injury in the Chinese recreational skiing and snowboarding population was 1.98 per 1000 skier days, which was comparable with the reported incidence of 0.5–3.7 per 1000 skier days in European and North American countries in recent years.1 7–9 According to government report, the total number of visits in ski resorts in Chongli hit nearly one million in the 2018–2019 ski season, which means an estimated number of 2000 sports injuries in one season if such finding is extrapolated to the whole region. Therefore, a better understanding of injury pattern in Chinese population will guide the reform of local healthcare facilities to deal with the increasing number of participants in snow sports.
The mean age of injured visitors was 32.5±12.9 years (range 3–73 years). Of the injured population, 9.3% were younger than 15 years old. In China, students’ winter vacation lasts for about 4 weeks around the Chinese New Year. We found that sports injury among teenagers peaked in January and February and constituted nearly 15% of all injuries that occurred in these 2 months. The incidence of ski injury was reported higher in teenagers than in adults.10 As more young people participate in these activities, an increase in paediatric patients with snow sports injuries will be seen in the future.
Previous studies have found female skiers are more susceptible to lower extremity injuries, especially knee injuries, with nearly 50% of injured female skiers suffering from knee injury.11 The present study found that the lower extremity was the most common injured body part among female skiers. However, there was no significant difference in terms of injured body parts between male and female skiers and snowboarders. Girardi et al 12 found that men experienced more severe injuries than women, which may be due to higher speed, body weight and trail difficulties in men.
Snowboarders accounted for nearly 40% of the injured population during the latest season. Previously published data showed an increase in the percentage of snowboarders in total and injured winter sports populations.7 13 This young sport appeals to more young people and at the same time reshapes injury profile. In a study conducted in the Big Sky area in the USA, snowboarders took up 42.8% of injured visitors in the 2009–2010 season, while between 1995 and 2000 only 23.0% of injured people were snowboarders.14 Many studies reported that snowboarders had significantly more injuries to the head, spine and upper extremity when compared with skiers, whereas skiers sustained significantly more lower extremity injuries.7 14 15 The present study revealed the same patterns, with higher rates of head and upper extremity injuries in snowboarders and lower rates of lower extremity injuries. In a study comparing injury severity in different sports, the authors reported that the percentage of mild, moderate and severe injuries in skiing was 41%, 44% and 15%, respectively, while the percentage of injuries in snowboarding was 34%, 53% and 13%.9 Maat et al 15 reported that skiers were more seriously injured, with Injury Severity Scale scores higher than 9.
Beginners and medium-level skiers (63.5%) and snowboarders (81.4%) made up the majority of injured visitors. In a study involving 19 539 injured snowboarders in Japan, the proportion of trunk and multiple injuries was found to increase with higher skill level; injury severity was also found to increase with skill level.16 Another study found no relationship between skill level and injury severity in skiing and snowboarding population once unconscious patients (who cannot report their skill level) were ruled out.13
In our study, the rate of injuries not involving others was 67.9%, which is lower than the reported rate on Austrian ski slopes.3 The difference is likely attributed to the higher density of skiers/snowboarders on the slope in China, which implied the fact that the rate of crash accident was extremely high on medium trails (see online supplemental table 7). Yet no available studies provide conclusive evidence on the influencing factors of the rate of self-inflicted and crash injuries.17
The cause of injury was also found to be related to injured body parts among both skiers and snowboarders. Head injury took up a significantly more portion in accidents involving others. Sports-specific injuries, such as shoulder injury in snowboarding and knee injury in skiing,7 were more frequent in accidents not involving others. These findings can be attributed to different injury mechanisms, with non-contact injury often causing ligament and tendon tear, and contact injury causing bony injury and concussion.18
From an epidemiological view, the present study provides strategies that can guide the restructure of local hospitals and unload the burden during the winter season. First, establish a paediatric orthopaedic department to cope with paediatric patients, who took up nearly 10% of the whole injury population, especially the surge during the winter vacation in China. Second, establish a department of neurosurgery and a department of oral and maxillofacial surgery to deal with head and face injuries, which took up 13% of all injuries. Third, rearrange the worktime schedule according to the time-related ‘tide’ of winter sports injury to increase effectiveness with limited manpower. For example, during the winter season, weekends can be set as work days and another two weekdays as rest days to cope with the traumatic cases in weekends, which are twice as many as in weekdays. Fourth, intensive care units are crucial in managing severe injuries as the population at higher risk for severe injuries including snowboarders, of higher skill level and of young participants is growing bigger. Fifth, build up communication and cooperation network with nearby ski resorts to allow access to critical patient information in advance and guide prehospital care. Although the present study did not provide information about injury severity and number of patients who needed transfer and further treatment, based on existing literature up to 60% of injured skiers and snowboarders seen in resort clinics require transfer to hospitals.9 To date, the local hospital in Chongli has reinforced its orthopaedics and sports medicine department by seeking cooperation with higher level hospitals in Beijing. An evidence-based restructuring of local hospitals may increase accessibility to healthcare among injured skiers and snowboarders in nearby ski resorts.
Several limitations exist in this study. First, severity of injury and accurate diagnosis were not recorded and patients were not followed up for prognosis. Second, although medical providers in the ski resort collected injury cases as thorough as possible, there were still patients who went to local or tertiary hospitals directly or did not receive any type of medical help for mild injuries. In this case, the incidence of injury may be underestimated. Additionally, data on injury severity and number of patients who needed transfer were incomplete, so we were unable to estimate the burden in local hospitals during the skiing season. We are currently conducting a large-scale survey on the demographics of Chinese winter sports participants and a prospective research of winter sports injury in the skiing population in China to fill the gap. The effectiveness of hospital restructuring will be reported as well.
Supplementary Material
Acknowledgments
The medical director of Wanlong Ski Resort, Zhang Jinwei, provided help in the collection of injury data.
Footnotes
NC and YY contributed equally.
Contributors: NC designed the study, carried out the data analysis and drafted the manuscript. YY carried out the design of patient information registration chart and helped draft the manuscript. YJ helped to connect with relevant staff in Wanlong Ski Resort and revise the manuscript. YA conceived of the study and participated in its design.
Funding: The study was supported by the National Key Research and Development Program of China (2018YFF0301100).
Competing interests: None declared.
Patient consent for publication: Not required.
Ethics approval: This study was approved by the Peking University Third Hospital Medical Science Research Ethics Committee.
Provenance and peer review: Not commissioned; externally peer reviewed.
Data availability statement: Data from the present study are deidentified participant data, which are available upon reasonable request. Please contact the first author for permission to reuse the original data (email: albert_west@163.com).
Supplemental material: This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.
References
- 1. Ekeland A, Ro̸dven A, Johnson RJ, et al. Skiing and boarding injuries on Norwegian slopes during two winter seasons. J ASTM Int 2010;7:102817 10.1520/JAI102817 [DOI] [Google Scholar]
- 2. Castellani C, Singer G, Eibisberger M, et al. An epidemiologic analysis of winter sport accidents on Ski slopes comparing two seasons. J Sports Med Phys Fitness 2019;59:648–54. 10.23736/S0022-4707.18.08665-6 [DOI] [PubMed] [Google Scholar]
- 3. Ruedl G, Philippe M, Sommersacher R, et al. [Current incidence of accidents on Austrian ski slopes]. Sportverletz Sportschaden 2014;28:183–7. 10.1055/s-0034-1385244 [DOI] [PubMed] [Google Scholar]
- 4. Haaland B, Steenstrup SE, Bere T, et al. Injury rate and injury patterns in FIS world cup alpine skiing (2006-2015): have the new Ski regulations made an impact? Br J Sports Med 2016;50:32–6. 10.1136/bjsports-2015-095467 [DOI] [PubMed] [Google Scholar]
- 5. Soligard T, Palmer D, Steffen K, et al. Sports injury and illness incidence in the PyeongChang 2018 Olympic winter games: a prospective study of 2914 athletes from 92 countries. Br J Sports Med 2019;53:1085–92. 10.1136/bjsports-2018-100236 [DOI] [PubMed] [Google Scholar]
- 6. Asadollahi S, Bucknill A. Acute medial clavicle fracture in adults: a systematic review of demographics, clinical features and treatment outcomes in 220 patients. J Orthop Traumatol 2019;20:24. 10.1186/s10195-019-0533-3 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Kim S, Endres NK, Johnson RJ, et al. Snowboarding injuries: trends over time and comparisons with alpine skiing injuries. Am J Sports Med 2012;40:770–6. 10.1177/0363546511433279 [DOI] [PubMed] [Google Scholar]
- 8. Langran M, Selvaraj S. Snow sports injuries in Scotland: a case-control study. Br J Sports Med 2002;36:135–40. 10.1136/bjsm.36.2.135 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9. Stenroos A, Handolin L. Incidence of recreational alpine skiing and Snowboarding injuries: six years experience in the largest Ski resort in Finland. Scand J Surg 2015;104:127–31. 10.1177/1457496914532249 [DOI] [PubMed] [Google Scholar]
- 10. Provance AJ, Daoud AK, Tagawa A, et al. Pediatric and adolescent injury in skiing. Res Sports Med 2018;26:150–65. 10.1080/15438627.2018.1438282 [DOI] [PubMed] [Google Scholar]
- 11. Ruedl G, Linortner I, Schranz A, et al. Distribution of injury mechanisms and related factors in ACL-injured female carving skiers. Knee Surg Sports Traumatol Arthrosc 2009;17:1393–8. 10.1007/s00167-009-0860-7 [DOI] [PubMed] [Google Scholar]
- 12. Girardi P, Braggion M, Sacco G, et al. Factors affecting injury severity among recreational skiers and snowboarders: an epidemiology study. Knee Surg Sports Traumatol Arthrosc 2010;18:1804–9. 10.1007/s00167-010-1133-1 [DOI] [PubMed] [Google Scholar]
- 13. Coury T, Napoli AM, Wilson M, et al. Injury patterns in recreational alpine skiing and snowboarding at a mountainside clinic. Wilderness Environ Med 2013;24:417–21. 10.1016/j.wem.2013.07.002 [DOI] [PubMed] [Google Scholar]
- 14. Wasden CC, McIntosh SE, Keith DS, et al. An analysis of skiing and snowboarding injuries on Utah slopes. J Trauma 2009;67:1022–6. 10.1097/TA.0b013e3181b0d559 [DOI] [PubMed] [Google Scholar]
- 15. Maat SC, Luppino FS, Schipper IB, et al. Injury patterns after skiing and snowboarding sports accidents. J Sports Med Phys Fitness 2020;60:119–24. 10.23736/S0022-4707.19.09753-6 [DOI] [PubMed] [Google Scholar]
- 16. Ogawa H, Sumi H, Sumi Y, et al. Skill level-specific differences in snowboarding-related injuries. Am J Sports Med 2010;38:532–7. 10.1177/0363546509348763 [DOI] [PubMed] [Google Scholar]
- 17. Ruedl G, Kopp M, Burtscher M, et al. [Causes and factors associated with collisions on ski slopes]. Sportverletz Sportschaden 2013;27:100–4. 10.1055/s-0032-1330767 [DOI] [PubMed] [Google Scholar]
- 18. Davey A, Endres NK, Johnson RJ, et al. Alpine skiing injuries. Sports Health 2019;11:18–26. 10.1177/1941738118813051 [DOI] [PMC free article] [PubMed] [Google Scholar]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
bmjopen-2020-037834supp001.pdf (28.7KB, pdf)