

Abstract
Introduction
Fly ash is a waste product generated from burning coal for electricity. It is comprised of spherical particles ranging in size from 0.1 µm to over 100 µm in diameter that contain trace levels of heavy metals. Large countries such as China and India generate over 100 million tons per year while smaller countries like Italy and France generate 2 to 3 million tons per year. The USA generates over 36 million tons of ash, making it one of the largest industrial waste streams in the nation. Fly ash is stored in landfills and surface impoundments exposing communities to fugitive dust and heavy metals that leach into the groundwater. Limited information exists on the health impact of exposure to fly ash. This protocol represents the first research to assess children’s exposure to coal fly ash and neurobehavioural outcomes.
Methods
We measure indoor exposure to fly ash and heavy metals, and neurobehavioural symptoms in children aged 6 to 14 years old. Using air pollution samplers and lift tape samples, we collect particulate matter ≤10 µm that is analysed for fly ash and heavy metals. Toenails and fingernails are collected to assess body burden for 72 chemical elements. Using the Behavioural Assessment and Research System and the Child Behaviour Checklist, we collect information on neurobehavioural outcomes. Data collection began in September 2015 and will continue until February 2021.
Ethics and dissemination
This study was approved by the Institutional Review Boards of the University of Louisville (#14.1069) and the University of Alabama at Birmingham (#300003807). We have collected data from 267 children who live within 10 miles of two power plants. Children are at a greater risk for environmental exposure which justifies the rationale for this study. Results of this study will be distributed at conferences, in peer-reviewed journals and to the participants of the study.
Keywords: community child health, public health, epidemiology
Strengths and limitations of this study.
A major strength of this innovative study is that it is the first research to measure children’s indoor exposure to fly ash, which is an emerging environmental health concern throughout the world.
This study design includes children aged 6 to 14 years old, who are more susceptible to environmental exposures, like fly ash and heavy metals.
Multiple measures of fly ash and heavy metals from environmental (air and lift tape samples) and biological (toenails and fingernails) samples are being collected.
Neurobehavioural performance and symptoms are measured using two methods: the Behavioural Assessment and Research System and the Child Behaviour Checklist.
Although methods were used to reduce bias in the sample of participants, it is possible that some participants were more concerned about fly ash exposure and hence more likely to participate in the study.
Introduction
Coal ash is a waste product that is produced from coal-fired power plants. When coal is burned for energy in pulverised fuel combustion chambers, it generates heat, and produces a molten mineral residue. As heat is extracted by the boiler tubes, flue gas is cooled and the residue hardens and forms an ash. Larger, heavier ash particles fall to the bottom of the combustion chamber. Lighter ash particles remain in the flue gas and are collected in air pollution control devices. These lighter ash particles are termed fly ash and compose 40% to 80% of coal ash.1–5
Coal fly ash is a fine silt of spherical powdery particles with diameters ranging from less than 0.1 µm to over 100 µm.5–7 The average size range of the respirable fraction of fly ash is from 1.98 µm to 5.64 µm.8 Although fly ash is mainly composed of silicon, aluminium, iron, calcium and oxygen, trace elements such as arsenic, chromium and lead may be found in fly ash.1 5 8–13 The composition of fly ash depends on the geochemical properties of the coal, the preparation of the coal and the burning process, but research has shown that metal concentrations are much greater than those found in the parent coal.3 14 15
In 2018, over 36 million tons of fly ash were generated in the USA, making it one of the largest industrial waste streams nationwide.16 China and India generate more fly ash than the USA.17 Throughout the world, countries vary in the amount of fly ash that is beneficially used in products such as concrete and grout. In the USA, approximately 55% to 65% of fly ash is reused,16 17 however countries like China and India, where coal combustion is increasing, use less than 50% of fly ash.17 The fly ash that is not reused is stored in landfills and surface impoundments with limited regulations, which impose critical environmental and public health concerns.
Landfills and surface impoundments containing fly ash expose nearby communities to potentially harmful trace elements. Humans can be exposed to fly ash and the metals contained in the particles by inhaling fugitive dust and ingesting contaminated groundwater. Children have a higher risk for negative health outcomes related to fly ash exposure. Compared with adults, children are more likely to breathe through their mouth, breathe more air relative to their lung size and body weight, are physically closer to the ground-level, are more likely to engage in hand-to-mouth behaviours and are less likely to stop activity if they experience respiratory distress. Their brains and lungs are still developing.18–20
Although the toxicity and hazard potential of coal ash exposure is high due to potential exposure to trace elements, there is limited research on the health effects of chronic coal ash exposure among children. Researchers investigating health among children exposed to fly ash or living in proximity to power plants have reported greater neurodevelopment conditions, like attention deficit hyperactivity disorder (ADHD), increased sleep problems, increased respiratory conditions and increased gastrointestinal problems.21–23 These studies were limited in that residential location or distance from coal-fired power plants was used as a proxy for exposure to coal ash. None of the studies directly measured in-home exposure to fly ash.
Research has shown that Americans spend approximately 90% of their time indoors,24 where the concentrations of some pollutants can be 2 to 5 times higher than outdoor concentrations.25 Furthermore, fly ash can enter the home through windows, doors or ventilation systems. So, indoor exposure is a potential public health concern, especially for children. However, little research has investigated whether children who reside in the vicinity of coal-fired power plants with coal ash storage facilities are at greater risk of neurobehavioural problems using data on exposure collected in participants’ homes.
Study aims
The overall objective of this community-based study is to evaluate indoor fly ash exposure and the prevalence of neurobehavioural performance and symptoms of 300 children living within 10 miles of two power plants in Jefferson County, Kentucky. Fly ash exposure is measured in particulate matter ≤10 µm (PM10) samples and lift tape samples. Neurobehavioural outcomes are assessed by the Behavioural Assessment and Research System (BARS) and the Child Behaviour Checklist (CBCL). The two specific aims from the study that are emphasised in this protocol paper are to: (1) Characterise indoor exposure to fly ash and heavy metals in homes of children living within close proximity to power plants with coal ash storage facilities and (2) Assess if increased fly ash exposure and greater heavy metal body burden is associated with poorer neurobehavioural health.
Fly ash is a significant environmental problem with emerging public health impacts. This study is novel in that it is the first to measure fly ash in the homes of children. Furthermore, it is the first community-based study to use these exposure measures to understand the impact of exposure on children’s neurobehavioural health.
Methods and analysis
This is a cross-sectional study with an exposure assessment. Data collection began in September 2015 and will end on February, 2021. The study takes place in Jefferson County and Bullitt County, Kentucky.
Power plants in Jefferson County, Kentucky, USA
Jefferson County is home to two power plants that are approximately 10 miles apart and owned by the same parent company. The Cane Run Generating Station was built in the 1950s and began operation in November 1954. It is located approximately eight miles from downtown Louisville, Kentucky, and occupies over 500 acres along the Ohio river.26 This plant has five ponds, two of which stored coal ash. The main coal ash pond, which was opened in 1972 and sits approximately 1200 feet east of the Ohio River, has a surface area of approximately 50 acres, with a capacity of 2 million cubic years.27 28 This pond stored fly ash, bottom ash and other materials.27 28 It received a high hazard rating by the United States Environmental Protection Agency (EPA) indicating that collapse of the pond could lead to loss of life or major damage to dwellings, buildings or important utilities.29 In 2015 the plant was refitted for natural gas. In 2017, the main ash pond was closed and capped. In addition to the capped pond, Cane Run has a large on-site ash landfill that opened in the early 1980s30 and it is now capped.31 It was last estimated to be 110 acres and over 130 feet high.32
The Mill Creek Generating Station is located downstream from the Cane Run Plant. It began operating in the early 1970s, occupies over 500 acres and is the largest coal-fired power plant owned by Louisville Gas and Electric.33 The plant’s main coal ash pond, which opened at the same time as the plant,34 is in proximity to residential homes. The coal ash pond sits on over 40 acres and stores an estimated 6.4 million cubic yards of material.34 35 It has been given a high hazard rating by the EPA. Mill Creek’s coal ash landfill opened in the 1980s, has a maximum elevation of 598 feet and contains approximately 13.5 million cubic yards s of coal ash.36
Both the Cane Run and Mill Creek plants are pulverised coal, subcritical fired steam generators37 that receive coal from the Illinois Basin of Western Kentucky and Indiana by rail or barge.38 The coal from this area is mid-range sulphur, low moisture content, moderate ash content and high BTU (British Thermal Unit), bituminous thermal coal. Affolter and Hatch (2011) stated that the main coals in the Western Kentucky region consist of Danville-Baker, Herrin, and Springfield Coals.39 Table 1 reports the characteristics of these coals.
Table 1.
Characteristics of coal from the Illinois Basin of Western Kentucky
| Coal type | Mean ash yield, % (range, %) |
Mean sulphur content, % (range, %) |
Mean calorific value, BTU/lb range (BTU/lb) |
| Danville-Baker | 11.9 (4.2 to 44.2) | 2.9 (0.3 to 9.7) | 10 920 (5800 to 12 990) |
| Herrin | 10.9 (2.4 to 43.6) | 3.0 (0.3 to 14.5) | 11 170 (5770 to 13 420) |
| Springfield | 11.2 (2.8 to 49.7) | 3.5 (0.5 to 19.5) | 11 280 (4810 to 13 910) |
BTU, British Thermal Unit.
Before coal is burned for energy, it is washed to remove or decrease impurities. In Western Kentucky coal, sulphur and ash are the two predominate impurities that are removed during the coal washing process. Washing the coal reduces sulphur content by 0.5% to 2.5% and reduces ash content by 9% to 13%.40As previously noted, elements that may be harmful to human health can become concentrated in coal ash.3 5 14 15 Affolter and Hatch (2011) reported mean elemental concentrations of 13 different potentially harmful elements found in coals throughout the Illinois Basin.39 Table 2 presents the ranges of these elements.
Table 2.
Range of potentially toxic elements found in coals throughout the Illinois Basin
| Element | Range (ppm) |
| Antimony | 0.7 to 2.3 |
| Arsenic | 5.8 to 34 |
| Beryllium | 1.6 to 3.7 |
| Cadmium | 0.14 to 1.3 |
| Chromium | 15 to 20 |
| Cobalt | 3.6 to 9.2 |
| Lead | 7.7 to 24 |
| Manganese | 17 to 62 |
| Mercury | 0.08 to 0.14 |
| Nickel | 12 to 36 |
| Selenium | 1.3 to 3.7 |
| Thorium | 1.7 to 2.5 |
| Uranium | 1.3 to 3.3 |
Patient and public involvement
During the design of the grant proposal and this resulting protocol manuscript, no patients or the public were involved.
Participant recruitment and sample size
Our study area represents more than 12 zip codes throughout southwestern Jefferson County and northern Bullitt County, Kentucky. To ensure participants are representative of the population throughout the study area, we used Geographical Information Systems (GIS) methods to identify and recruit study participants.41 First, we stratified the study area using a series of buffer zones at 2 mile intervals from 0 to 10 miles from the centroid of the straight line that connects the two power plants. Additionally, buffer zones were stratified by wedge-shaped quadrants. This method divided our study area into 20 sampling units. Prevalence estimates of neurobehavioural conditions for exposed children were selected to range between 20% and 30%, based on findings from a cross-sectional study that assessed children’s health in four communities residing near a coal-fired power plant.23 The prevalence of symptoms in the non-exposed children, were estimated at values of 5% and 10%. These values represent a range for neurobehavioural conditions in the USA, such as ADHD (6.8%) and behavioural conduct problems (3.5%).42 Based on a simulated power calculation, we determined that 300 children needed to be recruited for this study to achieve near 80% power in most scenarios (table 3).
Table 3.
Power for varying scenarios of sample size per zone, exposures for each zone and probabilities of symptoms for exposed and unexposed individuals.
| Sample size/zone | Sample size total | Exposure/zone | Pr (sym|exposed) and Pr (sym|unexposed) | |||
| 0.3, 0.1 | 0.3, 0.05 | 0.25, 0.1 | 0.25, 0.05 | |||
| 60 | 300 | 1, 0.8, 0.5, 0.2, 0 | 0.80 | 0.97 | 0.62 | 0.91 |
| 0.8, 0.7, 0.5, 0.2, 0 | 0.92 | 1.00 | 0.75 | 0.98 | ||
| 0.7, 0.5, 0.3, 0.1, 0 | 0.91 | 1.00 | 0.73 | 0.97 | ||
| 0.6, 0.5, 0.4, 0.3, 0 | 0.92 | 1.00 | 0.83 | 0.99 | ||
| 0.6, 0.5, 0.4, 0.3, 0.2 | 0.99 | 1.00 | 0.88 | 1.00 | ||
Recruitment methods vary and include ‘shoe-leather’ methods, where the research team goes door-to-door talking with participants about the study and/or leaving flyers at their homes. Additionally, we mail letters and flyers to potential participants in the zip codes in our study area, and have used social media, newspaper articles and television appearances to publicise the study. Furthermore, we have used snowballing methods, asking current participants to ask their friends and neighbours to recruit additional households that are eligible for this study.
Inclusion and exclusion criteria of study participants
For this study, both children and their parents/guardians are being recruited. To be included in the study, the family must have lived at their address or within the sampling units for at least 2 years. Most of the families in our study are non-transient and remain within the study area. In order for parents/guardians to participate, they have to consent for their child to take part in the study, complete three questionnaires, help their child collect fingernails and toenails, allow a registered nurse into their home to take the vitals of the child and complete a paediatric health history and home inspection and permit the research team to conduct the in-home exposure assessment. Additionally, if parents/guardians are smokers, they must agree to smoke outside during the week that the air pollution samplers are running inside the home.
In order for the child to take part in this study, he/she must assent to participate, allow researchers to take dust samples in his/her room, agree to assist his/her parents with toenail and fingernail collection, take a battery of computer tests and manual tests that measure neurobehavioural performance. Children are excluded from this study if they have a genetic disorder that is known to cause neurobehavioural problems, such as Down syndrome.
For this study, we assent all children. If their parent/guardian wants to participate, but the child does not assent, we do not enrol the child or parent/guardian into the study.
Exposure assessment methods
For this study, we conduct air monitoring and collect lift samples to quantify exposure to PM10 and identify fly ash particles inside children’s home environments. In these samples, we also analyse the composition of metals and metalloids in particulate matter and fly ash particles. Additionally, toenails and fingernails are collected from children to assess elemental body burden. A registered nurse (RN) visits the homes and collects the child’s vital signs, completes a paediatric health history and conducts a home exposure assessment. Multiple questionnaires are used to collect additional information. Analytical methods used include proton-induced X-ray emissions (PIXE), scanning electron microscopy (SEM) and energy dispersive X-ray (EDX). Figure 1 details the exposure assessment and analysis methods of the samples, which is provided in detail below.
Figure 1.
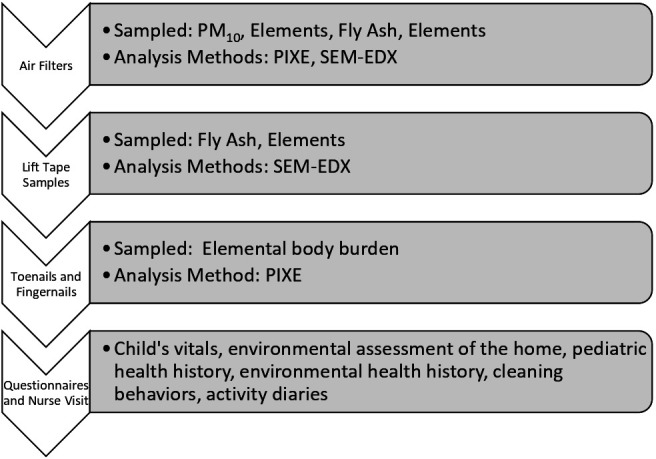
Exposure assessment, analytical methods used and outcomes from the assessment. EDX, energydispersive X-ray; PIXE, proton-induced X-ray emissions; PM10, particulate matter ≤10 µm; SEM, scanning electron microscopy.
Indoor air measurements
Indoor PM10 is measured using both continuous particle monitors (EPAM-7500) and a single-stage personal modular impactor (PMI) (SKC Inc) connected to an AirChek XR5000 pump. The EPAM is a portable particulate monitor that provides real-time measurement and display of PM10, particulate matter ≤2.5 µm and particulate matter ≤1.0 µm. The EPAM uses optical light scattering for real-time measurements. It is placed in participant’s homes and configured to measure PM10 every minute. The EPAM runs for 1 week.
Inside the cassette of the PMI is a 37 mm polycarbonate filter that collects PM10. A 25 mm pre-oiled disposable impaction disc is inserted onto the top of the filter cassette to decrease particle bounce and allow for more efficient particle collection. Polycarbonate membrane filters were selected because of their properties that allow for analysis by optical microscopy techniques. To determine the total mass of PM10 that is collected, gravimetric analysis is conducted. Prior to being inserted into the cassette of the PMI, each polycarbonate filter is weighed three times using a BM-20 analytical microbalance. The average of these measurements is known as the pre-weight. Once the PMI is removed from the field, the filter is weighed three times. The average of these measurements is known as the post-weight. Subtracting the pre-weight from the post-weight provides the total mass of PM10 that is collected from the home.
The PMI is connected to an AirChek XR5000 air sampling pump via ¼ inch diameter tygon tubing. These small, lightweight pumps are specifically designed to provide accurate (±5% of set-point) airflows between 1 to 5 liters per minute (L/min) by using an isothermal closed loop flow sensor. The isothermal closed loop flow sensor directly measures and constantly maintains the set flow rate. To compensate for fluctuations in temperature after the pump has been calibrated, the AirChek XR5000 has a built-in sensor. In the case of excessive backpressure, for example, if the filter becomes overloaded, the AirChek XR5000 is designed to stop after >15 s. The pump will display a flow fault icon on the screen and attempt to restart up to five times every 15 s. Before placing the pumps into the homes, they are calibrated using a MesaLabs DryCal Defender 510 in the laboratory. After calibration, three flow rate readings are taken 1 min apart and recorded. All readings are within ±5% of 3 L/min, which is the recommended flow rate for optimal PMI performance. The initial flow rate is calculated by averaging these three readings.
Using tripod stands, the PMI is placed roughly 1 to 1.5 metres above the ground to simulate the breathing zone of an average child. Additionally, strategic placement of the PMI and air pump avoids windows, doors to the outside, air vents, fireplaces, stoves and electronic devices to avoid re-suspension of particles. Once in place, the PMI and air pump are turned on and continue to run in the participant’s home for approximately 1 week. At the end of the air sampling period, three to four flow rate measurements are taken with the DryCal and recorded. The average of these measurements is known as the final flow rate. The overall flow rate is determined by taking the average of the sum of the initial flow rate and final flow rate. Using the overall flow rate and the total mass of PM10, as determined by gravimetric analysis, the concentration of PM10 is determined. Calculating the mass concentration on the filters is a vital step in determining the elemental distribution in subsequent laboratory methods. To determine the elemental composition of PM10, PIXE is used. To determine the presence of fly ash and the composition of fly ash, SEM/EDX is used.
Analytical methods used
Proton induced X-ray emission spectroscopy
PIXE is useful if the elemental concentrations are low or if the elements are present at unknown concentrations. PIXE is an analytical method in which energetic protons transfer kinetic energy to the inner shell electrons of the target atom, forcing the electrons from the atom resulting in X-ray production.43 The X-ray spectrum and energies are unique to the element from which they were emitted and the amount of X-rays emitted corresponds to the mass of the particular element being assessed in the sample.43 There are several advantages to PIXE analysis. First, because it is a non-destructive analysis method, errors from sample digestion and preparation are alleviated. Second, PIXE is capable of simultaneously analysing 72 inorganic elements from sodium to uranium in liquid, solid and aerosol filter samples.
Scanning electron microscopy with energy dispersive X-ray
Fly ash particles are distinguished from other particles by their morphological and chemical properties. Fly ash particles are smoothly spherical, which are very distinct from other metallurgical emissions. Therefore, fly ash particles can be identified through microscopic methods. In addition to morphological differences, fly ash is chemically different than other particulate matter. For example, metallurgical emissions are characterised by the elements, Fe (iron), Mn (manganese) and Si (silicon). Particles from the steel industry are characterised by Fe, Mn, Si and aluminium (Al). Fly ash particles are characterised by Si, sulphur (S), potassium (K), calcium (Ca) and Fe. This metal ‘fingerprint’ is used to identify the presence of fly ash in our samples.
SEM/EDX is a quick, non-destructive surface analytical technique that creates high resolution images of surface topography. Primary electrons, produced from the scanning electron beam, bombard the sample’s surface and thus generate secondary electrons. The secondary electron’s low energy intensity is greatly affected by the surface topography of the sample. The surface image is generated by measuring the intensity of the secondary electron as a function of the scanning electron beam’s position. Because of the primary electron beam’s ability to focus on an area <10 nm in size, high resolution images are possible. Primary electron bombardment from the scanning beam also creates backscattered electrons that indicate the elements in the sample.44 Identification of an element is possible because the backscatter electron intensity is associated with the atomic number of a specific element.
In addition to secondary and backscattered electrons, the scanning electron beam creates X-rays. As previously discussed in the PIXE section, X-rays are unique to the corresponding element. Therefore, analysis of the X-ray can provide semi-quantitative information on the elements in the sample.44
Lift tape samples
During the first home visit, lift tape sampling is conducted. Lift sampling is a simple method for removing particles from a surface to determine their number and size distribution. We use Stick-to-it Lift Tape (SKC, Inc) to identify the presence of fly ash on multiple surfaces in children’s bedrooms. Stick-to-it Lift Tape is a flexible plastic microscope slide with an adhesive area that can be used for sampling inorganic dust contamination on surfaces. These lift tapes are non-destructible and have a consistent sample area. In each child’s bedroom, three standard locations, a bedframe, window and dresser, are sampled. The lift tape samples undergo optical microscopy to determine the presence or absence of fly ash in the dust samples and provide the per cent of fly ash on the samples, as well as the elemental concentration of fly ash particles.
Activity assessment
In addition to air sampling and lift sampling, an activity diary is filled out by each participant. The types of activities recorded include: cooking, use of secondary heating sources, use of indoor fans, burning candles or incense, cleaning activities and use of chemicals, construction, presence of pets, open/closed windows and smoking. This information will provide insight into differences in fly ash and metal concentrations that occur among the samples.
Registered nurse visit
After air sampling and lift sampling is completed, an RN schedules an appointment with the parents/guardians to visit the home. The nurse’s visit takes approximately 1 hour to complete. While at the home, the RN measures the child’s height, weight and blood pressure, and completes the Paediatric Health History Interview and Environmental Home Assessment.
Paediatric health history interview
The Paediatric Health History Interview form includes demographic information about the participant and parents, current and past health conditions, past hospitalisations, current medications use, parents’ perception of health and behaviour, immunisations history, details of pregnancy complications and use of substances during pregnancy and delivery, breastfeeding, early childhood development, the child’s current participation in school activities and behaviour at school and at home and a brief health history of the immediate family living in the home. The interview form was developed by investigators of the study, after evaluating several standard paediatric health assessment forms.
Environmental home assessment
A visual assessment of the home is conducted using the publicly-available Paediatric Environmental Home Assessment (PEHA) tool developed by the National Centre for Healthy Housing. The PEHA includes a subjective determination of general home characteristics and indoor pollutants and observation of the general home environment, the sleep environment and home safety.45 Information such as type of house, age of home, type of foundation, number of floors, sources of heating and cooling, the presence of indoor pollutants (presence of moulds, lead-based paints, asbestos, radon, environmental smoke), the RN’s assessment of the cleanliness of the home environment, details of the participants sleep environment (number of beds in room, allergens, pillows, bedding, flooring and so on) and home safety (renovations, lighting, poison control, fire hazards, appropriate storage of chemicals and hot liquids, window guards and so on) is collected.
Toenails and fingernails
Heavy metal body burden is assessed by collecting toenails and fingernails from the child participants. Toenails and fingernails are a useful measure of metals because they represent long-term exposure given the slow growth rate, are less likely to be contaminated, are non-invasive and are easy to collect and store. Toenails and fingernails reflect exposure integrated over the preceding 3 to 12 months and concentrations of elements may vary due to age, gender, behaviours and diet. 46 47
Parents/guardians are asked to begin collecting their child’s toenails and fingernails during the initial phone conversation, prior to the initial visit. During the initial visit, any nails the child had already cut are collected, in addition to any nails the child cuts during the visit. For each participant, approximately 150 mg of nails are collected over.
Once the total amount of nails is collected, they are cleaned using one acetone wash and two deionised water washes. The nails are then dried and weighed a final time before being placed in a container to transport to the laboratory for analysis. Children’s nails are cryogenically frozen, ground and bound into a 3/8-inch pellet, with the natural binding agent Somar-Mix Power #210, a mixture of boric acid and water. The pellet is then analysed by PIXE to determine the amount and type of elements in the sample.
Study questionnaires
Parents or guardians of the participating children complete the Environmental Health History Questionnaire (EHH) and Home Cleaning Questionnaire (HC). The EHH consists of 108 questions and is based on five existing paediatric environmental exposure history guides including the Paediatric Environmental History,48 the paediatric exposure history questions to be included in a well-child visit49 and the American Academy of Pediatrics guidance on taking an environmental history50 as well as The Agency for Toxic Substances and Disease Registry’s ‘Taking an Exposure History’,51 and the rapid questionnaire of environmental exposures to pregnant women.52 The HC has nine questions related to cleaning behaviours. The questionnaires are left with the parents or guardians for approximately 1 week and returned on completion.
Study outcomes being measured
To assess neurobehavioural performance and symptoms, we use the BARS and the. Both were completed at the participant’s home.
Child Behaviour Checklist
Although there are several instruments available that assess problem behaviours in children, the CBCL is among the most respected and widely used; it has been translated into over 90 languages.53 54 The CBCL is a psychometrically-sound, research tool for evaluating children’s emotional, behavioural and social functioning. Although there are CBCL forms available for different age groups, this study focusses on the CBCL for ages 6 to 18 years of age. There are parent, teacher and child report forms. For this study, we are using the parent-report form. The CBCL’s questions are associated with problems on a syndrome scale in eight different categories: anxious/depressed, withdrawn/depressed, somatic complaints, social problems, thought problems, attention problems, rule-breaking behaviour and aggressive behaviour.
Anxious/depressed, withdrawn/depressed and somatic complaints are broadly categorised as internalising behaviours. Rule-breaking behaviours and aggressive behaviours are broadly categorised as externalising behaviours. Overall, the CBCL yields scores for internalising and externalising behaviours, total problems and six Diagnostic and Statistical Manual of Mental Disorders (DSM)-oriented subscales. The six DSM-oriented subscales include attention deficit/hyperactivity problems, anxiety problems, oppositional defiant problems, affective problems, conduct problems and somatic problems.55 Based on age and sex, these scores are compared with clinical cut-off points for the particular comparison group.
The CBCL is left with the parents/guardians for 1 week and returned on completion. Based on parents’/guardians’ responses to the 124-item questionnaire, t-scores are calculated using standardised norms for age and gender. If a participant scores in the clinical or borderline range on any of the CBCL subscales, the child psychologist follows-up with the parents/guardians of the child by conducting a Structured Clinical Interview for Diagnosis of DSM Disorders.
Behaviour Assessment and Research System
Neurobehavioural performance is assessed in all children using the BARS.56 BARS, which administers a series of neurobehavioural tests, includes a 9-button device that sits on top of a standard laptop. Child participants hit a button from 1 to 9 corresponding to their answer. BARS was developed by the Oregon Health and Science University to provide a series of neurobehavioural tests that are optimised to detect neurotoxicity.56 It has been adapted for use with children as young as preschool age.57–59 BARS has been used for children exposed to neurotoxic chemicals (pesticides) but has not previously been used for children exposed to fly ash in their community.57 58
The six BARS tests that are used to assess neurobehavioural performance are displayed in table 4. Comparisons in formal studies have shown that BARS tests have comparable test–retest reliabilities with the tests given in their original testing formats.56 In addition to the BARS tests, three additional tests are used: the Recall of Objects Immediate and Recall of Objects Delayed, Purdue Pegboard and Beery-Buktenica Developmental Test of Visual-Motor Integration. These nine tests cover a range of neurobehavioural performance.
Table 4.
neurobehavioural tests
| Test | Measured functions |
| BARS tests | |
| Symbol digit | Speed, attention/integration |
| Finger tapping | Response speed and coordination |
| Digit span | Memory and attention |
| Continuous performance | Attention |
| Matching-to-sample | Visual memory |
| Selective attention | Attention |
| Additional tests | |
| Recall of objects immediate and recall of objects delayed | Recall and recognition memory |
| Purdue pegboard | Dexterity |
| Visual motor integration | Hand-eye coordination |
Behavioural Assessment and Research System.
A child psychologist administers the nine tests in the evening hours during the weekdays or on a Sunday afternoon. The BARS tests are administered continuously as the child sits comfortably at a table. While the study team members are present throughout the entire test and answer questions as they arise, there is minimal interaction with the children during the BARS tests. The children interact with the computer. These tests are given continuously and in the same order for each child. When the BARS is completed, the psychologist administers the other three tests. It takes approximately 40 min to complete the testing.
Planned statistical analysis
Characterisation of the metal concentrations on filters and in nail samples will be stratified by sampling zone and evaluated using exploratory data analysis methods including boxplots, histograms and kernel density estimates. Sampling units will be grouped into exposure zones on the basis of the minimal distance from either of the two plants. Differences between these exposure zones will be evaluated using one-way analysis of variance (ANOVA) or the Kruskal-Wallis test, depending on whether the data are normally distributed. The use of transformations (eg, log, Box-Cox power transformation) will be explored. Additionally, associations between metal concentrations and individual distance from the nearest plant for each household will be explored using Pearson/Spearman correlations and linear regression models.
For toenails and fingernail samples, if the majority (eg, ≥75%) of children have levels below the Limit of Detection (LOD), concentrations will be dichotomised as present/absent and analysed for differences between zones using logistic regression. If the majority of concentrations are detectable, then differences between children within each exposure zone will be evaluated using either one-way ANOVA or the non-parametric Kruskal-Wallis test. If there is a mixture of detectable and below the LOD concentrations, a total metal score will be calculated, similar to the method of Cave et al, 2010. Briefly, since metal concentrations are on different scales, each metal concentration will be ranked and then aggregated and grouped into quartiles of overall metal concentration.60
Presence of fly ash found in the filter samples will be analysed in a similar fashion to the metal concentrations. Presence of fly ash will also be dichotomised into present/absent, and evaluated for differences between exposure zones. Adjustment for other environmental factors and activities potentially influencing metal concentrations (eg, smoking,) will be accounted for using multivariable regression models.
Association between the BARS tests/CBCL t-scores and exposure zone/distance from the plant will be evaluated using a linear regression model, with possible transformations (Box-Cox) when responses are non-normally distributed. A similar model will be used to investigate potential associations between BARS and CBCL scores and fly ash exposure/heavy metal body burden. In addition to investigating associations with continuous CBCL scores, CBCL scores will be dichotomised at a level indicative of a disorder and analysed for association with fly ash exposure using either logistic regression or the Cochran-Mantel-Haenszel test (with exposure zone or sampling unit as the strata). Initially, each exposure variable (fly ash, heavy metal concentration) will be analysed individually to determine significant marginal associations with BARS/CBCL t-scores, with p values adjusted for multiple comparisons to control the false-discovery rate using the Benjamini-Hochberg approach.61 After any significant marginal associations have been identified, potential confounding variables (demographics, exposure and activity history) will be adjusted for using multivariable regression models. Since missing values can have a compounding effect in multivariable regression models, percentage of missing values will be evaluated for each variable and checked for association with zone and other important covariates. If found to depend on these variables, multiple imputation strategies will be used to impute missing values and fit multivariable regression models.
Geographical Information Systems and GeoSpatial methods
In addition to facilitating the spatial sampling procedure described above, GIS and advanced geospatial statistical methods will be used in the analysis stage of this project. GIS will be used to geocode participants’ residential addresses and measure distance from participant’s residence to the two power plants, as well as spatially interpolate and integrate the exposure observations (ie, fly ash, PM10 and heavy metals) and health outcome data.
Geospatial statistical techniques such as Hotspot Analysis and bivariate local Moran’s I will be used to investigate the clustering patterns of fly ash and heavy metals and explore the associations between these patterns and children’s neurobehavioural problems across the study area. These analyses will help characterise the geospatial patterns in neurobehavioural problems related with indoor fly ash exposure in the vicinity of the power plants and coal ash storage facilities.
Furthermore, exposure modelling will be used to investigate the spatial dispersion of pollutants in the study area while considering local meteorological factors (eg, temperature, wind speed, wind direction and so on). To estimate the spatial dispersion of air pollution from the two plants, we will use fate and transport modelling via map algebra62 and the AERSCREEN model, which is based on the EPA’s AERMOD.63 AERSCREEN produces estimates of ‘worse-case’ concentrations of pollutants from a single source, for many times intervals, ranging from 1 hour, 3 hours, 8 hours, 24 hours up to annual. We anticipate that AERSCREEN will be particularly useful for estimating overlapping exposures from both power plants and storage facilities. In general, these geospatial analysis methods will allow us to examine distance decay effects on exposure to air toxicants and identify areas that may have the highest levels of exposure to pollutants from the power plants.
Ethics and dissemination
Ethics
Written informed consent is obtained from the parents/guardians and written informed assent is obtained from all participating children. Trained study personnel explain the informed consent documents to the parents/guardians and the assent document to the children. After the explanation, parents/guardians and children sign the documents. Two copies of the consent/assent documents are signed; one copy is kept by the parents/guardians and one copy is kept by the researchers. These consenting procedures were approved by the Institutional Review Board of the University of Louisville (IRB # 14.1069) and the University of Alabama at Birmingham (IRB#:300003807), where the principal investigator (PI) of the grant is currently employed.
Dissemination
All findings from this study will be disseminated through publications in peer-reviewed journals and presentations at national and international conferences. In addition, results will be provided to the participants of the study. Within 3 months, the child psychologist makes multiple attempts to contact and discuss the neurobehavioural outcomes with parents/guardians if the child has scored poorly on the CBCL. The environmental results will be returned after the study concludes with the final enrolment. At this time, the researchers will create summary statistics based on the community that can be compared.
Strengths and limitations
This protocol paper describes our research that represents the first study to assess children’s exposure to in-home fly ash and prevalence neurobehavioural outcomes. The health impacts of fly ash are unknown, but the potential risks are immense. Currently most countries of the world do not consider fly ash as a hazardous waste, so the regulations regarding its storage and disposal are limited. Disposal methods permit fugitive dust to escape leading to increases in ambient air pollution. Numerous epidemiological studies have associated particulate matter with cancer, heart disease, asthma and/or increased mortality. The potential impact of this innovative study is great as it will provide evidence to describe the environmental health impacts of fly ash exposure. Better understanding the exposure that communities living near fly ash storage facilities may help to provide impetus for better regulations for its storage.
Strengths
This study has several strengths. Regarding exposure, we are able to quantify indoor PM10 concentrations and determine if fly ash is found in the home. Children spend the majority of time indoors24 and the EPA reports that concentrations of pollutants can be 2 to 5 times higher indoors than outdoors.25 For measurement of fly ash, we are using both air sampling and lift tape sampling which provides us a characterisation of in-home exposure. For the assessment of the outcomes, we are using several measures of neurobehavioural assessment including BARS and the CBCL. BARS is administered at the homes of the participating children by a child psychologist. The same psychologist conducts all the testing, assuring consistency in the protocol. Community members were involved in recruitment of participants for this study. Research has shown that studies that involve community members have lowered attrition, increased compliance, improved accuracy and greater applicability and usability in the settings where community-based research occurs.64–68
Limitations
Although there are many strengths of this innovative study, there are some limitations. First, we assume that a week-long in-home air sample is representative of children’s chronic exposure. While children spend hours in their homes, they also spend times in other indoor locations, such as schools. In Jefferson County, Kentucky, children do not necessarily attend their neighbourhood schools, so exposure may be increased or decreased depending on location of their school. Second, during the week-long sampling period, participants may have interfered with the sampling equipment. Although the pumps require a series of steps to be physically shut down and they were contained in soundproof cases which make turning on and off the pumps difficult, participants could have turned the pump off by the electrical switch that was connected to the outlet where the pump was plugged in. Additionally, children could have put their hands over the impactor, which would have changed the flow rates and hence the amount of PM10 collected. When we installed the samplers in the homes of the participants, several things were done to prevent participant interference. We ensured that the sampling equipment was placed in a location that was not in the way of the family’s general movement, such as in a corner of the room with the impactor facing the main area. Furthermore, we checked the flow rate of the pumps in the middle of the week and again at the end of the sampling period. This ensured that they were running at the 3 L/min required for the sampler and that they were still running. In a few instances, we believed that participants did interfere with the sampler, because (1) the pump shut off early in the sampling week, or (2) the filter became overloaded and the pump shut off. In these instances, the participant was either removed from the study, or agreed to allow us to conduct the sampling again.
Third, we are not directly measuring temperature, humidity and air velocity in the home. These conditions could have an effect on PM10 measurement. We do ask participants to keep an activity diary of events around the home, including the opening and closing of windows. Fourth, we are not measuring exposure to other pollutants in the home. We are only focussing on fly ash, PM10 and metals. Other potential pollutants such as volatile organic compounds could explain some neurobehavioural symptoms in children. Fifth, participants who are more concerned about fly ash pollution or whose children have pre-existing health problems may be more likely to enrol in this study. To address this potential bias, recruitment materials do not have references to the health outcome we are assessing.
The final potential limitation of this study is that we have only included the parent form of the CBCL. The validity and reliability of the CBCL is high for assessing childhood behaviour and emotional problems and has been addressed in many studies.69–72 Chrombach’s alpha’s of the CBCL range from a low of 0.72 for anxiety problems to a high of 0.97 for total problems. However, we did not use the teacher report of behaviour which is commonly used to ascertain behavioural problems such as ADHD.73 Problems such as attentiveness are often most apparent in school and teacher input may have improved identification of children with behavioural problems.
Supplementary Material
Acknowledgments
The authors would like to acknowledge and thank Lindsay Tompkins, Chisom Odoh, Jack Pfeiffer, Carol Norton, Jillian Winn and Paula Kingsolver for their assistance with the overall study. We would like to thank the community and community leaders for their participation in this study. In addition, the authors would like to acknowledge C Hanchette (deceased, October 2017) for her contributions to the overall study.
Footnotes
Contributors: KMZ is the principal investigator of the study, conceptualised the initial project design and led the writing of this manuscript. CGS and ANH made substantial contributions to the writing of the manuscript and editing. LS, GNB, CZ and BJP are co-investigators of the study and contributed to the conceptualisation of the project and assisted in the writing and editing of the manuscript. All authors read and approved the final manuscript.
Funding: This work was supported by the National Institutes of Health, National Institute of Environmental Health Sciences (R01ES024757, PI: Zierold).
Competing interests: None declared.
Patient and public involvement: Patients and/or the public were not involved in the design, or conduct, or reporting, or dissemination plans of this research.
Patient consent for publication: Not required.
Provenance and peer review: Not commissioned; externally peer reviewed.
References
- 1. Hatori Y, Matsuyama S, Ishii K, et al. Pixe analysis of individual particles in coal fly ash. Int J PIXE 2010;20:57–62. 10.1142/S0129083510001975 [DOI] [Google Scholar]
- 2. Li J, Zhuang X, Querol X, et al. A review on the applications of coal combustion products in China. Int Geol Rev 2018;60:671–716. 10.1080/00206814.2017.1309997 [DOI] [Google Scholar]
- 3. Yao ZT, Ji XS, Sarker PK, et al. A comprehensive review on the applications of coal fly ash. Earth Sci Rev 2015;141:105–21. 10.1016/j.earscirev.2014.11.016 [DOI] [Google Scholar]
- 4. Ahmaruzzaman M. A review on the utilization of fly ash. Prog Energy Combust Sci 2010;36:327–63. 10.1016/j.pecs.2009.11.003 [DOI] [Google Scholar]
- 5. Zierold KM, Odoh C. A review on fly ash from coal-fired power plants: chemical composition, regulations, and health evidence. Rev Environ Health 2020:reveh-2019-0039. 10.1515/reveh-2019-0039 [DOI] [PubMed] [Google Scholar]
- 6. Temuujin J, Surenjav E, Ruescher CH, et al. Processing and uses of fly ash addressing radioactivity (critical review). Chemosphere 2019;216:866–82. 10.1016/j.chemosphere.2018.10.112 [DOI] [PubMed] [Google Scholar]
- 7. Kumar S, Singh J, Mohapatra SK. Role of particle size in assessment of physico-chemical properties and trace elements of Indian fly ash. Waste Manag Res 2018;36:1016–22. 10.1177/0734242X18804033 [DOI] [PubMed] [Google Scholar]
- 8. Brown P, Jones T, BéruBé K. The internal microstructure and fibrous mineralogy of fly ash from coal-burning power stations. Environ Pollut 2011;159:3324–33. 10.1016/j.envpol.2011.08.041 [DOI] [PubMed] [Google Scholar]
- 9. Liberda EN, Chen LC. An evaluation of the toxicological aspects and potential doses from the inhalation of coal combustion products. J Air Waste Manag Assoc 2013;63:671–80. 10.1080/10962247.2013.777374 [DOI] [PubMed] [Google Scholar]
- 10. Bednar AJ, Averett DE, Seiter JM, et al. Characterization of metals released from coal fly ash during dredging at the Kingston ash recovery project. Chemosphere 2013;92:1563–70. 10.1016/j.chemosphere.2013.04.034 [DOI] [PubMed] [Google Scholar]
- 11. Patra KC, Rautray TR, Tripathy BB, et al. Elemental analysis of coal and coal ash by PixE technique. Appl Radiat Isot 2012;70:612–6. 10.1016/j.apradiso.2011.12.013 [DOI] [PubMed] [Google Scholar]
- 12. Mokhtar MM, Taib RM, Hassim MH. Understanding selected trace elements behavior in a coal-fired power plant in Malaysia for assessment of abatement technologies. J Air Waste Manage Assoc 2014;64:867–78. 10.1080/10962247.2014.897271 [DOI] [PubMed] [Google Scholar]
- 13. Jambhulkar HP, Shaikh SMS, Kumar MS. Fly ash toxicity, emerging issues and possible implications for its exploitation in agriculture; Indian scenario: a review. Chemosphere 2018;213:333–44. 10.1016/j.chemosphere.2018.09.045 [DOI] [PubMed] [Google Scholar]
- 14. Le Seur Spencer L, Drake LD. Hydrogeology of an alkaline fly ash landfill in eastern Iowa. Ground Water 1987;25:519–26. 10.1111/j.1745-6584.1987.tb02881.x [DOI] [Google Scholar]
- 15. Bhangare RC, Ajmal PY, Sahu SK, et al. Distribution of trace elements in coal and combustion residues from five thermal power plants in India. Int J Coal Geol 2011;86:349–56. 10.1016/j.coal.2011.03.008 [DOI] [Google Scholar]
- 16. The American Coal Ash Association Coal combustion product (CCP) production and use survey report, 2018. Available: https://www.acaa-usa.org/Portals/9/Files/PDFs/2018-Survey-Results.pdf [Accessed 13 Feb 2020].
- 17. Bhatt A, Priyadarshini S, Acharath Mohanakrishnan A, et al. Physical, chemical, and geotechnical properties of coal fly ash: a global review. Case Studies in Construction Materials 2019;11:e00263 10.1016/j.cscm.2019.e00263 [DOI] [Google Scholar]
- 18. Etzel RA. Air pollution hazards to children. Otolaryngol Head Neck Surg 1996;114:265–6. 10.1016/S0194-5998(96)70180-8 [DOI] [PubMed] [Google Scholar]
- 19. World Health Organization Air pollution and child health: prescribing clean air. Available: https://www.who.int/ceh/publications/Advance-copy-Oct24_18150_Air-Pollution-and-Child-Health-merged-compressed.pdf?ua=1 [Accessed 20 Feb 2020].
- 20. Johnson SB, Blum RW, Giedd JN. Adolescent maturity and the brain: the promise and pitfalls of neuroscience research in adolescent health policy. J Adolesc Health 2009;45:216–21. 10.1016/j.jadohealth.2009.05.016 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21. Tang D, Lee J, Muirhead L, et al. Molecular and neurodevelopmental benefits to children of closure of a coal burning power plant in China. PLoS One 2014;9:e91966. 10.1371/journal.pone.0091966 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22. Tang D, Li T-yu, Liu JJ, et al. Effects of prenatal exposure to coal-burning pollutants on children's development in China. Environ Health Perspect 2008;116:674–9. 10.1289/ehp.10471 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 23. Sears CG, Zierold KM. Health of children living near coal ash. Glob Pediatr Health 2017;4:2333794X1772033 10.1177/2333794X17720330 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 24. US Environmental Protection Agency Report to Congress on indoor air quality: volume 2. assessment and control of indoor air pollution. Available: https://nepis.epa.gov/Exe/ZyNET.exe/9100LMBU.TXT?ZyActionD=ZyDocument&Client=EPA&Index=1986+Thru+1990&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery=&File=D%3A%5Czyfiles%5CIndex%20Data%5C86thru90%5CTxt%5C00000022%5C9100LMBU.txt&User=ANONYMOUS&Password=anonymous&SortMethod=h%7C-&MaximumDocuments=1&FuzzyDegree=0&ImageQuality=r75g8/r75g8/x150y150g16/i425&Display=hpfr&DefSeekPage=x&SearchBack=ZyActionL&Back=ZyActionS&BackDesc=Results%20page&MaximumPages=1&ZyEntry=1&SeekPage=x&ZyPURL [Accessed 05 Oct 2020].
- 25. US Environmental Protection Agency The total exposure assessment methodology (team) study: summary and analysis. volume I. Available: https://nepis.epa.gov/Exe/ZyNET.exe/2000UC5T.TXT?ZyActionD=ZyDocument&Client=EPA&Index=1986+Thru+1990&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery=&File=D%3A%5Czyfiles%5CIndex%20Data%5C86thru90%5CTxt%5C00000013%5C2000UC5T.txt&User=ANONYMOUS&Password=anonymous&SortMethod=h%7C-&MaximumDocuments=1&FuzzyDegree=0&ImageQuality=r75g8/r75g8/x150y150g16/i425&Display=hpfr&DefSeekPage=x&SearchBack=ZyActionL&Back=ZyActionS&BackDesc=Results%20page&MaximumPages=1&ZyEntry=1&SeekPage=x&ZyPURL [Accessed 05 Oct 2020].
- 26. Louisville Gas & Electric Plant-wide odor, Fugitive dust, and maintenance emissions control plan cane run generating station. Available: https://louisvilleky.gov/sites/default/files/air_pollution_control_district/documents/boardorders/20130816lgecanerunodorandfugitivedustcontrolplan.pdf [Accessed 05 Oct 2020].
- 27. Martin L. Assessment of dam safety coal combustion surface Impoundments (task 3) final report. Available: https://archive.epa.gov/epawaste/nonhaz/industrial/special/fossil/web/pdf/duke_belews_final.pdf [Accessed 05 Oct 2020].
- 28. AECOM Technical Services Annual groundwater monitoring and corrective action report, August 1 – December 31, 2019, 2019. Available: https://lge-ku.com/sites/default/files/ccr/W_CR_GNST_GMCA_ANGWCA_022120.pdf [Accessed 05 Oct 2020].
- 29. United States Environmental Protection Agency (EPA) Fact sheet: coal combustion residuals (CCR) surface impoundments with high hazard potential ratings. Available: https://nepis.epa.gov/Exe/ZyNET.exe/P10048EX.TXT?ZyActionD=ZyDocument&Client=EPA&Index=2006+Thru+2010&Docs=&Query=&Time=&EndTime=&SearchMethod=1&TocRestrict=n&Toc=&TocEntry=&QField=&QFieldYear=&QFieldMonth=&QFieldDay=&IntQFieldOp=0&ExtQFieldOp=0&XmlQuery=&File=D%3A%5Czyfiles%5CIndex%20Data%5C06thru10%5CTxt%5C00000009%5CP10048EX.txt&User=ANONYMOUS&Password=anonymous&SortMethod=h%7C-&MaximumDocuments=1&FuzzyDegree=0&ImageQuality=r75g8/r75g8/x150y150g16/i425&Display=hpfr&DefSeekPage=x&SearchBack=ZyActionL&Back=ZyActionS&BackDesc=Results%20page&MaximumPages=1&ZyEntry=1&SeekPage=x&ZyPURL [Accessed 05 Oct 2020].
- 30. Adnams K, Stellato A, Harris W. Assessment of dam safety coal combustion surface impoundments (task 3) final report; cane run power station. Available: https://archive.epa.gov/epawaste/nonhaz/industrial/special/fossil/web/pdf/eon-cane-final.pdf [Accessed 05 Oct 2020].
- 31. Louisville Gas & Electric, & Kentucky Utilities LG&E to invest more than $300 million in additional environmental improvements. Available: https://lge-ku.com/node/9796 [Accessed 05 Oct 2020].
- 32. Bruggers J. LG&E to cap Cane Run coal ash. Available: https://www.courier-journal.com/story/tech/science/environment/2015/03/05/lge-makes-plans-close-cap-louisville-ash-pond-landfill-cane-run-plant/24436013/ [Accessed 05 Oct 2020].
- 33. Louisville Gas & Electric Mill creek generating station. Available: https://lge-ku.com/our-company/community/neighbor-neighbor/mill-creek-generating-station [Accessed 05 Oct 2020].
- 34. Bowers R, Cormier S. Dam safety assessment report of CCW impoundments – LG&E Mill Creek Station. Available: https://archive.epa.gov/epawaste/nonhaz/industrial/special/fossil/web/pdf/mill-creek-draft.pdf [Accessed 05 Oct 2020].
- 35. Zimmerman P. CCR Rule annual inspection report – Louisville Gas & Electric Mill Creek ash treatment basin, 2016. [Google Scholar]
- 36. Hurt RP. Ccr rule annual inspection report. Available: https://lge-ku.com/sites/default/files/ccr/W_MC_LF_OR_ANPEINS_012020.pdf [Accessed 05 Oct 2020].
- 37. Black & Veatch Corporation EON technical due diligence summary report (final draft). Available: https://psc.ky.gov/pscscf/2011%20cases/2011-00162/20110923_LGEs%20Response%20to%20Commission%20Staffs%201st%20Info%20Request%20Question%20No%2032(h).pdf [Accessed 05 Oct 2020].
- 38. Kentucky Energy and Environment Cabinet Kentucky energy profile. 6 ed, 2017. https://eec.ky.gov/Energy/KY%20Energy%20Profile/Kentucky%20Energy%20Profile%202017.pdf [Google Scholar]
- 39. Affolter RH, Hatch JR, Chapter E. Characterization of the quality of coals from the Illinois Basin. in resource assessment of the Springfield, Herrin, Danville, and baker coals in the Illinois Basin. Available: https://pubs.usgs.gov/pp/p1625d/ [Accessed 05 Oct 2020].
- 40. Kentucky Coal Association and Kentucky Geological Survey Kentucky coal facts In: Pocket guide. 11th ed, 2011. https://www.yumpu.com/en/document/read/30184386/11th-edition-pocket-guide-kentucky-coal-facts [Google Scholar]
- 41. Allpress JLE, Curry RJ, Hanchette CL, et al. A GIS-based method for household recruitment in a prospective pesticide exposure study. Int J Health Geogr 2008;7:18. 10.1186/1476-072X-7-18 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 42. Perou R, Bitsko RH, Blumberg SJ, et al. Mental health surveillance among children--United States, 2005-2011. MMWR Suppl 2013;62:1–35. [PubMed] [Google Scholar]
- 43. Bombelka E, Richter FW, Stroh A, et al. Analysis of the Cu, Fe, and Zn contents in cytochrome c oxidases from different species and tissues by proton-induced X-ray emission (PixE). Biochem Biophys Res Commun 1986;140:1007–14. 10.1016/0006-291X(86)90735-7 [DOI] [PubMed] [Google Scholar]
- 44. Surface Science Western Scanning electron microscopy coupled with energy dispersive X-ray (SEM/EDX) spectroscopy. Available: https://www.surfacesciencewestern.com/analytical-services/scanning-electron-microscopy-coupled-with-energy-dispersive-x-ray-semedx-spectroscopy/ [Accessed 20 Feb 2020].
- 45. National Health Homes and Training Network The scenario is fictional. The photos are taken from a variety of homes to highlight key issues. Available: https://healthyhousingsolutions.com/wp-content/uploads/2014/12/CHW_PEHA_Materials_Oct2017.pdf [Accessed 25 Feb 2020].
- 46. Hulka BS, Wilcosky TC, Griffith JD. Biological markers in epidemiology. New York, NY: Oxford University Press, 1990. [Google Scholar]
- 47. Slotnick MJ, Nriagu JO. Validity of human nails as a biomarker of arsenic and selenium exposure: a review. Environ Res 2006;102:125–39. 10.1016/j.envres.2005.12.001 [DOI] [PubMed] [Google Scholar]
- 48. National Environmental Education Foundation Pediatric environmental history. Available: https://www.neefusa.org/resource/pediatric-environmental-history [Accessed 25 Feb 2020].
- 49. Agency for Toxic Substances and Disease Registry (ATSDR) Taking a PediatricExposure history. what exposure questions should be included in a WellChild visit? Available: http://www.atsdr.cdc.gov/csem/csem.asp?csem=26&po=7 [Accessed 25 Feb 2020].
- 50. Etzel RA. Balk SJ, Pediatric environmental health. 3rd ed American Academy of Pediatrics, 2011. [Google Scholar]
- 51. Agency for toxic substances and disease registry (ATSDR) Case studies in environmental medicine. taking an exposure history, 2000. https://www.atsdr.cdc.gov/hec/csem/exphistory/docs/exposure_history.pdf [Google Scholar]
- 52. Eskenazi B, Bradman A, Finkton D, et al. International Fetal and Newborn Growth Consortium for the 21st Century. A rapid questionnaire assessment of environmental exposure to pregnant women in the INTERGROWTH 21st project. BJOG 2013;120:129–38. [DOI] [PubMed] [Google Scholar]
- 53. Seligman LD, Ollendick TH, Langley AK, et al. The utility of measures of child and adolescent anxiety: a meta-analytic review of the revised children's manifest anxiety scale, the State-Trait anxiety inventory for children, and the child behavior checklist. J Clin Child Adolesc Psychol 2004;33:557–65. 10.1207/s15374424jccp3303_13 [DOI] [PubMed] [Google Scholar]
- 54. Guttmannova K, Szanyi JM, Cali PW. Internalizing and externalizing behavior problem scores - Cross-ethnic and longitudinal measurement invariance of the Behavior Problem Index. Educ Psychol Meas 2008;68:676–94. [Google Scholar]
- 55. Muller BE, Erford BT. Choosing assessment instruments for depression outcome research with school-age youth. J Couns Dev 2012;90:208–20. 10.1111/j.1556-6676.2012.00026.x [DOI] [Google Scholar]
- 56. Rohlman DS, Gimenes LS, Eckerman DA, et al. Development of the behavioral assessment and research system (bars) to detect and characterize neurotoxicity in humans. Neurotoxicology 2003;24:523–31. 10.1016/S0161-813X(03)00023-8 [DOI] [PubMed] [Google Scholar]
- 57. Rohlman DS, Villanueva-Uy E, Ramos EAM, et al. Adaptation of the behavioral assessment and research system (bars) for evaluating neurobehavioral performance in Filipino children. Neurotoxicology 2008;29:143–51. 10.1016/j.neuro.2007.10.006 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 58. Rohlman DS, Arcury TA, Quandt SA, et al. Neurobehavioral performance in preschool children from agricultural and non-agricultural communities in Oregon and North Carolina. Neurotoxicology 2005;26:589–98. 10.1016/j.neuro.2004.12.002 [DOI] [PubMed] [Google Scholar]
- 59. Rohlman DS, Gimenes LS, Ebbert C, et al. Smiling faces and other rewards: using the behavioral assessment and research system (bars) with unique populations. Neurotoxicology 2000;21:973–8. [PubMed] [Google Scholar]
- 60. Cave M, Appana S, Patel M, et al. Polychlorinated biphenyls, lead, and mercury are associated with liver disease in American adults: NHANES 2003-2004. Environ Health Perspect 2010;118:1735–42. 10.1289/ehp.1002720 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 61. Benjamini Y, Hochberg Y. Controlling the false discovery rate: a practical and powerful approach to multiple testing. J R Stat Soc B 1995;57:289–300. 10.1111/j.2517-6161.1995.tb02031.x [DOI] [Google Scholar]
- 62. Pistocchi A. A GIS-based approach for modeling the fate and transport of pollutants in Europe. Environ Sci Technol 2008;42:3640–7. 10.1021/es071548+ [DOI] [PubMed] [Google Scholar]
- 63. United States Environmental Protection Agency Air quality dispersion modeling – preferred and recommended models. Available: https://www.epa.gov/scram/air-quality-dispersion-modeling-preferred-and-recommended-models#aermod [Accessed 5 Oct 2020].
- 64. Polivka BJ, Chaudry R, Crawford JM, et al. Application and modification of the integrative model for environmental health. Public Health Nurs 2013;30:167–76. 10.1111/j.1525-1446.2012.01050.x [DOI] [PMC free article] [PubMed] [Google Scholar]
- 65. Green LW, Mercer SL. Can public health researchers and agencies reconcile the push from funding bodies and the pull from communities? Am J Public Health 2001;91:1926–9. 10.2105/AJPH.91.12.1926 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 66. Jordan C, Lee P, Shapiro E. Measuring developmental outcomes of lead exposure in an urban neighborhood: the challenges of community-based research. J Expo Sci Environ Epidemiol 2000;10:732–42. 10.1038/sj.jea.7500130 [DOI] [PubMed] [Google Scholar]
- 67. Corburn J. Environmental justice, local knowledge, and risk: the discourse of a community-based cumulative exposure assessment. Environ Manage 2002;29:451–66. 10.1007/s00267-001-0013-3 [DOI] [PubMed] [Google Scholar]
- 68. Lynn FM. Community-Scientist collaboration in environmental research. Am Behav Sci 2000;44:649–63. 10.1177/00027640021956305 [DOI] [Google Scholar]
- 69. Achenbach TM, Rescorla LA. Manual for the ASEBA school-age forms & profiles. Burlington, VT: University of Vermont, Research Center for Children, Youth and Families, 2001. [Google Scholar]
- 70. Chang L-Y, Wang M-Y, Tsai P-S. Diagnostic accuracy of rating scales for attention-deficit/hyperactivity disorder: a meta-analysis. Pediatrics 2016;137:e20152749. 10.1542/peds.2015-2749 [DOI] [PubMed] [Google Scholar]
- 71. Ebesutani C, Bernstein A, Nakamura BJ, et al. Concurrent validity of the child behavior checklist DSM-Oriented scales: correspondence with DSM diagnoses and comparison to syndrome scales. J Psychopathol Behav Assess 2010;32:373–84. 10.1007/s10862-009-9174-9 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 72. Raiker JS, Freeman AJ, Perez-Algorta G, et al. Accuracy of Achenbach scales in the screening of attention-deficit/hyperactivity disorder in a community mental health clinic. J Am Acad Child Adolesc Psychiatry 2017;56:401–9. 10.1016/j.jaac.2017.02.007 [DOI] [PMC free article] [PubMed] [Google Scholar]
- 73. Nimh National Institute of mental health attention deficit hyperactivity disorder. Available: https://www.nimh.nih.gov/health/topics/attention-deficit-hyperactivity-disorder-adhd/index.shtml [Accessed 05 Oct 2020].
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.