

Abstract
Background: Modifiable risk factors are associated with cardiovascular mortality (CVM) which is a leading form of global mortality. However, diverse nature of urbanization and its objective measurement can modify their relationship. This study aims to investigate the moderating role of urbanization in the relationship of combined exposure (CE) of modifiable risk factors and CVM.
Design and Methods: This is the first comprehensive study which considers different forms of urbanization to gauge its manifold impact. Therefore, in addition to existing original quantitative form and traditional two categories of urbanization, a new form consisted of four levels of urbanization was duly introduced. This study used data of 129 countries mainly retrieved from a WHO report, Non-Communicable Diseases Country Profile 2014. Factor scores obtained through confirmatory factor analysis were used to compute the CE. Age-income adjusted regression model for CVM was tested as a baseline with three bootstrap regression models developed for the three forms of urbanization.
Results: Results revealed that the CE and CVM baseline relationship was significantly moderated through the original quantitative form of urbanization. Contrarily, the two traditional categories of urbanization could not capture the moderating impact. However, the four levels of urbanization were objectively estimated the urbanization impact and subsequently indicated that the CE was more alarming in causing the CVM in levels 2 and 3 urbanized countries, mainly from low-middle-income countries.
Conclusion: This study concluded that the urbanization is a strong moderator and it could be gauged effectively through four levels whereas sufficiency of two traditional categories of urbanization is questionable.
Significance for public health.
WHO has set global targets for the control of CVDs and CVM, however, the required outcomes are only possible if implemented policies are aligned with customized regional needs. This study guides the health-care providers that urbanization, as a macro-level socio-demographic change, can substantially influence the relationship of modifiable risk factors and CVM if measured objectively. The efficacy of rural-urban dichotomy is questionable and needs precise measurement. The newly proposed effective classification of urbanization can act as risk strata which will improve the CVDs and CVM risk estimates. This will subsequently lead towards developing customized population-based strategies aimed at controlling the surge of CVM and its possible causes. This study advocates the public health-care providers that the rapid urbanization is a real challenge especially for low-middle-income countries which needs due diligence and a viable solution.
Key words: Modifiable risk factors, cardiovascular mortality, urbanization, forms of urbanization, moderation
Introduction
Cardiovascular diseases (CVDs) are the leading cause of mortality that shared approximately 31% of the global mortality in recent past.1 Modifiable risk factors such as diabetes, hypertension, obesity, smoking, alcohol consumption and cholesterol levels are responsible for much of the burden of global cardiovascular mortality (CVM)2 and demonstrated independent association with CVM.3 However, this is not a simple cause and effect phenomenon. It is a result of a complex interplay between macrolevel changes and micro-level human behaviours.4 The calamitous epidemiological and socio-demographic changes create vulnerable living conditions which deteriorate the healthy lifestyle that results in high CVM rates.5 Urbanization is one of these complex socio-demographic change that probably influences the modifiable risk factors and their impact on CVM.3 Urbanization growth is associated with an extensive adverse health outcomes,6 which are strongly related to the CVDs risk factors,7,8 but it is also possible to link it with greater health facilities9 that can potentially reduce the CVM. These mixed findings characterize the diversified role of urbanization that variably affects an array of modifiable risk factors and CVM which needs an in-depth exploration.
A surge in the urbanization trend of urbanization has posed a challenging situation, especially in low-middle-income countries (LMICs), and it is expected that 70% of the world population will be urbanized by 2050.10 As a macro-level factor, it transforms eating and sleeping patterns, physical activities, social structure and habits of residents that collectively modify the lifestyle-related outcomes.11 However, urbanization is strongly associated with the economic conditions of the countries where people from developed economies have easy access to better health and educational facilities which subsequently increase their life expectancy.12 At the same time, such a population can have a high prevalence of modifiable risk factors and CVM.9,13 However, LMICs have to bear more burden of CVM as compared to developed economies.14 This manifold role of urbanization motivates the researcher to assume its moderating role in the relationship between modifiable risk factors and the CVM. However, urbanization is difficult to define, and researchers have been used the term urbanization and urbanicity interchangeably. Urbanicity is a static condition of urban areas at a given time point,9 while urbanization is the proportion of the total national population living in urban areas.13,15 Therefore, this proportion helps in stratifying the countries into predominantly urbanized and less urbanized countries. 13,16,17 A country with more than 50% population living in urban settings is classified as predominantly urbanized country. This stratification and dichotomy are supposed to cover a vast heterogeneity of this macro-level demographic change in itself, but reality could probably be the otherwise. A handful of past studies have also posed questions on this rural-urban dichotomy.18,19 The basic premise of this study is to evaluate the more precise impact of urbanization as moderator by introducing four levels (strata) which is deemed as more explanatory approach for the relationship between modifiable risk factors and CVM.
The main objective of this study is to test the hypothesis of the moderating effect of urbanization on the association between a set of modifiable risk factors and CVM. Further, this study also attempts to provide empirical evidence that rural-urban stratification might not capture the true influence of urbanization and thus, need revision. This study has used four important modifiable risk factors for CVM, which are tobacco usage, alcohol consumption, hypertension, and obesity. Similar to risk score computation, multiple studies in the past suggested and preferred to study the combined effects of risk factors.20,21 Therefore, in this study, we will use this set of four risk factors to compute a combined exposure (CE) of study.
Design and Methods
Design and settings
This cross-sectional study was mainly based on secondary data from WHO which retrieved from the published report entitled “Non-communicable Diseases Country Profile 2014”. This report was consisting of 194 countries of the world. The report also included the country level prevalence of non-communicable diseases (NCDs) and associated modifiable risk factors which were estimated through national-level surveys and registration systems data sets.22
Variables and their measurement
All variables were selected from the WHO report which were classified into outcome, exposure, potential moderator and covariables of study (except average age in the country which will be discussed in section ‘covariables of study’). The outcome of the study was the percentage of cardiovascular mortality (CVM). The WHO used vital registration system of the countries to retrieve the information.
The exposure of the study was four modifiable risk factors already recognized in the literature and represented as a quantitative variable, “combined exposure of modifiable risk factors (CE)” and obtained through confirmatory factor analysis (CFA). The risk factors of the study are percentage of hypertension, percentage of obesity, percentage of tobacco usage and alcohol per capita consumption, in litres of pure alcohol. The WHO used the data provided by estimation of the prevalence of hypertension, obesity and alcohol consumption. However, tobacco usage estimates were based on information retrieved from national-level surveys by WHO. The computation of CE of modifiable risk factors for the countries is discussed in the subsequent section.
Computation of combined exposure based on modifiable risk factors
Initially, Pearson correlation analysis of four modifiable risk factors provided traces of similar nature of the selected modifiable risk factors and baseline for the computation of CE. All individual risk factors also have a significant relationship with the CVM. There are two reasons to compute the CE:
The literature discussed in the previous section has guided that these four selected risk factors could be grouped into the same group of risk factors.
The CE value is like an index and easy to interpret especially at the country level. Higher value of CE would indicate a high amount of exposure for causing CVDs and its related mortality due to selected modifiable risk factors and vice versa.
Based on these two reasons, the set of four risk factors was tested as a latent construct that would lead to compute the CE. The CFA was used to validate this latent construct and was performed using analysis of moments structure (AMOS), v. 21.0. All modifiable risk factors are significantly and positively contributed to this latent construct with significant factor loads and t-values. These findings showed the presence of unidimensionality in the latent construct. Overall model fitness was also assessed to confirm the validity of the latent construct. All four main criteria, goodness of fit index (GFI; reference value: GFI ≥0.90), adjusted goodness of fit index (AGFI; reference value: AGFI ≥0.90), Chi-square/ degree of freedom (χ2/df; reference value: χ2 /df ≤3.0) and root mean square error approximation (RMSEA; reference value: RMSEA ≤0.080)23 were used to evaluate the goodness of fit. The model fit was satisfactory (GFI= 0.984, AGFI= 0.921, χ2/df= 1.41 and RMSEA=0.057). After statistical validation of construct, factor score weights for selected four risk factors were also computed based on the imputed factor scores. Hereafter, this collective form of these scores was used as CE of the study. Equation (1) showed the relative weights of each risk factor which were used to compute the CE for each country.
| CE = 0.269 (Prevalence of tobacco usage) + 0.258 (Alcohol consumption) + 0.124 (Prevalence of hypertension) + 0.180 (Prevalence of obesity) eq. 1 |
Three different forms of urbanization were derived from the percentage of the population living in urban areas (PPLUA). These forms were tested as potential moderator for the exposure and outcome relationship. WHO retrieved the information on PPLUA from United Nations world urbanization prospects.24
Measurement of different forms of urbanization
The PPLUA was considered as the amount of urbanization in the country. This actual amount of urbanization was the first form of urbanization and represented by PPLUA in the study. Usually, this form of urbanization is not used in the literature. The demographic definition of urbanization is the increasing share of the country’s population living in urban areas.25 Countries with more than 50% population in the urban areas are considered pre-dominantly urbanized, otherwise less urbanized. Similarly, WHO also used the term rural and urban regions of the countries4 and sometimes it was mentioned by researchers as high and low urbanization.16 These two traditional categories (pre-dominantly urbanized and less urbanized) composed the second form of urbanization which was expressed in the study as urbanization status (US). Satterthwaite et al.25 discussed that the level of urbanization can be the share itself in the country. We used this argument and divided possible range (0.01-100%) of actual amount of urbanization into quartile which were i.e. ≤25% = level 1, 25.01-50% = level 2, 50.01-75% = level 3 and 75.01-100% = level 4. This form of urbanization is characterised in the study as the level of urbanization and act as the third form of urbanization. We hypothesised that these newly suggested levels would be more helpful to uncover the true influence of urbanization on the relationship between CE and CVM.
Covariables of study
The average age in the country (average expected age estimates) and income group of the country were the covariables of study. Information on average age in the country and income group of the country retrieved from the reports.22,26 However, the income group of the countries was based on gross national income (GNI) per capita as suggested by World Bank.27 The average age in the countries was measured in years and income group was measured in four categories; low, lower-middle, upper-middle and highincome countries. Literature has discussed that more developed countries are usually more urbanized with good health facilities that would lead to high average age.25 Further, a higher age is associated with a high prevalence of CVDs risk factors and CVM.28 Similarly, literature also argued that economic condition has a strong relationship with the urbanization in the country.13,29,30 Therefore, to control the possible confounding effect of these two covariables, the analysis of the study was statistically adjusted. However, before using these two covariables as confounders of study, regression analyses were also performed which confirmed their role as the confounders.
Study size
We extracted all the required information on study variables mainly from WHO22 and United Nations26 reports where needed. The data used in this study can be retrieved from https://www.who.int/nmh/publications/ncd-profiles-2014/en/ and (https://population.un.org/wpp/Publications/Files/WPP2017_Key Findings.pdf). The countries with complete information on these variables were retained in the analysis. This inclusion criterion provided us with data of 129 countries for the final analysis of the study. This criterion was used and considered in order to avoid missing data. Imputation on missing values could be used to deal with the issue, however, diverse information of countries can mislead the findings.
Data analysis
Age-income adjusted CVM analysis was performed for the CE, then this base model was tested for three forms of urbanization. For the assessment of the moderating effect for different forms of urbanization we computed cross-product interaction terms; mean centres CE and three forms of urbanization separately. We have discussed that in this study the impact of urbanization was analysed using three separate forms. Therefore, interaction terms were computed separately for these urbanization measurements. Then, we analyse the three age and income adjusted CVM regression by using mean centred CE, and each form of urbanization as moderator separately with their interaction term. In addition, the interaction graphs were also formed for better illustration of the moderation.
Statistical package for social sciences (SPSS), v.21.0 and PROCESS, v.3.1 by Andrew F. Hayes, were used in this study to do the regression and moderation analysis respectively. Bootstrapping technique with a bias-corrected 95% confidence interval (CI) estimates were followed for the moderation analysis, using 5000 bootstraps resamples as suggested in the literature.31 Bootstrapping is a non-parametric technique that does not imply an assumption on the sample size and distribution of data. However, in the current study, we used this technique to avoid biased findings due to possible small sample sizes when the analysis was performed for different levels of urbanization. Mean ± SD for quantitative variables were also reported.
Results
The sample countries (n = 129) were heterogeneous regarding income as 17.8%, 23.3%, 26.4% and 32.6% were from low, lowermiddle, upper-middle and high-income groups, respectively. The average PPLUA in the sample countries was 58.53±22.24.
The average age in the countries substantially varied in different forms of urbanization (Table 1). Similarly, CE was also showed an increasing pattern in all forms of urbanization from the lowest urbanization categories and levels to highest except in the fourth level of urbanization. Mean CVM was 31.88% in the overall sample with a large amount (15.75%) of variation. In contrary to average age and CE, CVM pattern was very fluctuating in sub-groups of PPLUA and four levels of urbanization. However, it was not exposed through two categories of US. Two categories of US reflected that percentage of CVM was higher (37.43%) in predominantly urbanized countries as compared to less urbanized countries (22.14%). The average CVM (31.37%) at +1 SD PPLUA was lower than the average CVM (35.76%) in mean PPLUA level. Similarly, average CVM (31.30%) at the fourth level of urbanization portrayed relatively lower CVM as compared to CVM (41.57%) at the third level of urbanization. The decreasing trends of CVM at the highest level of urbanization and PPLUA indicated the traces of moderation effect and need to be explored.
Table 1.
Descriptive statistics of CE, CVM and quantitative covariable in the overall sample and different forms of urbanization.
| Overall sample and different forms of urbanization | Average age in the countries | CVM, % | CE |
|---|---|---|---|
| Overall sample (n = 129) | 71.70±8.07 | 31.88±15.75 | 14.53±4.52 |
| PPLUA | |||
| - 1 SD PPLUA (n = 23) | 64.65±6.38 | 18.47±9.45 | 10.40±3.02 |
| Mean PPLUA (n = 82) | 71.63±7.62 | 35.76±16.65 | 15.10±4.69 |
| + 1 SD PPLUA (n = 24) | 78.68±4.24 | 31.37±8.87 | 16.38±2.38 |
| US | |||
| Less urbanized (n = 47) | 65.44±7.24 | 22.14±14.26 | 11.48±3.70 |
| Pre-dominantly urbanized (n =82) | 75.28±6.11 | 37.43±13.72 | 16.23±4.02 |
| Level of urbanization | |||
| Level 1 (n = 12) | 63.25±6.61 | 15.33±9.71 | 10.44±3.77 |
| Level 2 (n =35) | 66.20±7.38 | 24.48±14.92 | 11.84±3.66 |
| Level 3 (n =49) | 73.12±6.31 | 41.57±15.23 | 16.40±4.76 |
| Level 4 (n = 33) | 78.52±4.10 | 31.30±7.99 | 15.97±2.63 |
Assessment of the relationship between CE and CVM and moderation impact
Before the assessment of moderation, multiple linear regression analysis was performed to assess the baseline relationship between the CE and CVM. The findings of the baseline relationship were reported in Table 2 and expressed by Model 1 (M1). For the assessment of the role of PPLUA, US and level of urbanization as moderator for above-mentioned baseline relationship, three bootstrap based interaction models were also reported in Table 2. Results of all models were adjusted for covariables of the study to control their possible confounding effect.
M1 reported that there was a significant positive impact of CE on CVM (ß1= 1.932, p<0.001) in the overall sample of the study. Additionally, both covariables were also significant in the tested relationship. The regression coefficient and significance of the interaction term is the main focus in moderation analysis. The presence of significant interaction term (ß3= -0.026, p=0.043) in Model 2 (M2) revealed that PPLUA had a moderating impact on the relationship between CE and CVM. The negative value of the regression coefficient of interaction term illustrates that the impact of CE on CVM reduces as PPLUA increases. However, in Model 3 (M3), the insignificant interaction term (ß5= -0.439, p=0.418) indicated the absence of moderation impact of US on the relationship of the CE and CVM.
In contrary to M3 and in continuation to M2, interaction terms in Model 4 (M4) (ß9= 2.401, p=0.007; ß10= 1.850, p=0.024), which were yielded by level 2 and 3 level of urbanization, were significantly affect the relationship of CE and CVM. Level 1 was the baseline level of urbanization in M4. The positive interaction terms in these two levels reflected that the CE causes more CVM on these levels of urbanization. Apart from, the interaction term of level 4 countries was insignificant which revealed that at this level of urbanization relationship of CE and CVM was not influenced by the urbanization. Surprisingly, the negative interaction term at level 4 explored that the highest level of urbanization became protective for the baseline relationship. The different magnitude and directions of interaction terms estimated through M4 explain the inconsistent relationship of CE and CVM on different levels of urbanization. This description reflected that four-levels of urbanization have more explanatory power to demonstrate the moderation impact as compared to PPLUA and US. The single interaction term in PPLUA just identified the presence of moderation impact of urbanization but did not provide a detailed idea about the thresholds of PPLUA at which the role of urbanization is changing.
Interaction graphs
Figures 1-3 are the interaction graphs for in which parallel regression lines would indicate the absence of moderation impact or insignificance of interaction terms. Figure 1 for PPLUA was created at three levels of urbanization i.e mean and ± 1SD due to the quantitative nature of PPLUA. The intersection of regression lines showed the changes in regression coefficients at different levels of PPLUA that confirmed the unequal impact of CE on the CVM at different values of PPLUA. However, Figure 2 for the US, which was consisted of almost parallel lines which showed that the relationship between CE and CVM was in a positive direction under the influence of both categories of US. Currently, there was no intersection of lines that reflected the absence of moderation impact of US on the baseline relationship of CE and CVM. Figure 3 showed that the relationship between CE and CVM was strongly influenced at levels 2 and 3 of urbanization using level 1 as a baseline. Levels 1 and 4 countries have the lowest impact of CE on CVM and their slopes were significantly different from level 2 and level 3 countries. It shows that at levels 2 and 3 of urbanization CE had a very strong positive impact on CVM.
Discussion
This examination based on WHO aggregated data supported our propositions and objective of the study. First, we found that latent construct CE was strongly associated with CVM after adjustment of average age and income in the countries. Second, we found that the impact of CE on CVM is moderated by urbanization when it is measured objectively. Two strata of US could not capture the moderating impact of urbanization while four levels of urbanization explained this influence more comprehensively. The significant impact of the original measure of urbanization (PPLUA) on the relationship between CE and CVM provided us with the rationale for detailed exploration. Our findings based on four levels suggested that the impact of CE on CVM is more noticeable in levels 2 and 3 urbanized countries. However, levels 1 and 4 countries were having a negative effect on the relationship between CE and CVM, but with completely different reasons. Further, the present study extends the usage of modifiable risk factors in a collective form instead of individual usage. This CE was computed due to the similar nature of actions of these risk factors on the CVDs and CVM.
Table 2.
Multiple regression and moderation analysis.
| Variables | Baseline model | PPLUA as moderator | US as moderator | Level of urbanization as moderator | ||||
|---|---|---|---|---|---|---|---|---|
| Model 1 (M1) | Model 2 (M2) | Model 3 (M3)* | Model 4 (M4)° | |||||
| β's | p-value | β's | p-value | β's | p-value | β's | p-value | |
| Average age in the countries | 1.02 | <0.001 | 1.03 | <0.001 | 0.95 | <0.001 | 1.13 | <0.001 |
| Income group of the country | -4.69 | 0.005 | -4.72 | 0.0145 | -6.09 | <0.001 | -5.02 | 0.002 |
| β1 = CE | 1.93 | <0.001 | 1.93 | <0.015 | 1.90 | <0.001 | -0.04 | 0.964 |
| β2 = PPLUA | -0.04 | 0.557 | ||||||
| β3 =CE ×PPLUA | -0.03 | 0.043 | ||||||
| β4 = US | 5.64 | 0.049 | ||||||
| β5 = CE ×US | -0.44 | 0.418 | ||||||
| β6 = Level 2 | 15.17 | <0.001 | ||||||
| β7 = Level 3 | 20.19 | <0.001 | ||||||
| β8 = Level 4 | 11.22 | 0.037 | ||||||
| β9 = CE ×Level 2 | 2.40 | 0.007 | ||||||
| β10 = CE ×Level 3 | 1.85 | 0.024 | ||||||
| β11 = CE ×Level 4 | -0.17 | 0.867 | ||||||
PPLUA, percentage of population living in urban areas; US, urbanization status
*less urbanized countries is a baseline category
°level 1 countries is a baseline category; CE, combined exposure.
There is a vast of literature that confirms the individual impact of hypertension,32 obesity,33,34 tobacco usage2,35 and alcohol consumption36 on CVM. These studies reported that the high prevalence of these risk factors associated with a high rate of CVM. Our study also explained the same relationship of modifiable risk factors and CVM, but through a unique way of the CE which was obtained through the imputed score by CFA. The current study found that there was a strong positive influence of CE on CVM after adjusting the impact of average age and income of countries as confounders. The countries with high CE would have more chances of high CVM and vice versa. However, this phenomenon of effect transference from CE to CVM is not simple and moderated through the urbanization.
The results of PPLUA indicated the strong interactive effect of urbanization with CE. The impact of CE on CVM was modified under the influence of PPLUA that confirms the presence of moderation impact. The negative impact of moderator and interaction term reflects that high urbanization would reduce the impact of CE on CVM. A recent study also concluded that high-income countries with large urbanization showed decreased trends of CVM due to a better health system and other preventive interventions.5 We also found surprisingly insignificant findings for the moderation impact of US when measured in two traditional categories. The dichotomy of the US probably merges the low and high effects of true urbanization as a moderator within these categories and could not cause any substantial changes in these two categories of urbanization. Therefore, both regression lines are slightly different and not able to capture the true effects. This situation justified our proposition and findings of the evaluation of the true impact of urbanization in more than two categories. Some past studies indirectly mentioned that these two categories might merge the true impact within the categories and could not reflect the potential of urbanization.18,19
To the best of our knowledge, no previous study has measured urbanization in more than two categories and studied their interaction effects with modifiable risk factors or their CE. Conditional effects of CE have been more alarming for levels 2 and 3 urbanized countries. These countries were mainly from LMICs having less economic stability, but they are more eager to adopt the rapid urbanization which indeed agitates the demand and supply of health facilities; and preventive strategies for the residents. Consequently, these countries are continuously crippling in the adverse effects of urbanization. A recent study also argued that urbanization is now a challenge for LMICs because of their transition phase towards urbanization.37 These countries cannot make strong hold on the outcomes of urbanization due to less economic sustainability which resulted in high environmental degradation, water contamination, injuries, NCDs and epidemics associated risk.38 Results also exhibited that this tragic living environment is adversely affecting the level 2 countries as compared to level 3 countries. This decrease in negative effects in the level 3 countries was due to comparatively better economic condition and better health facilities than level 2 countries. However, the high CVM average in level 3 countries is still an alarming situation. A recent study also found that upper-middle-income countries with high urbanization have comparatively less access to four main cardiovascular medicines to high-income countries39 that might result in high CVM.
Figure 1.
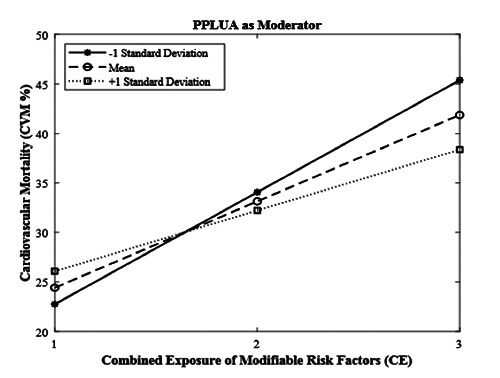
Percentage of population living in urban areas (PPLUA) as moderator for combined exposure and cardiovascular mortality.
Figure 2.
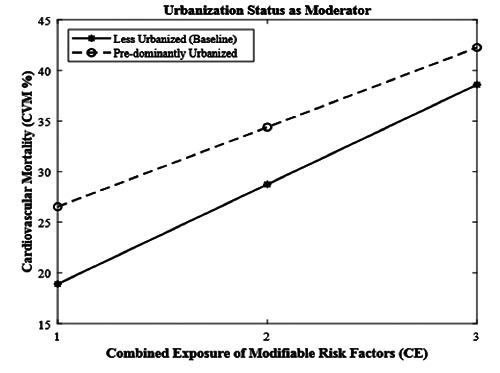
Urbanization status as moderator for combined exposure and cardiovascular mortality.
Figure 3.
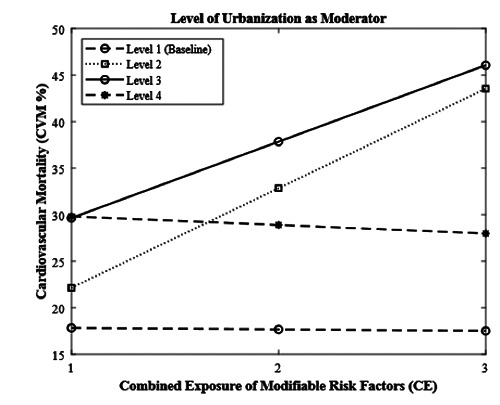
Level of urbanization as moderator for combined exposure and cardiovascular mortality.
Moderation analysis also found that the CE and CVM relationship was not influenced by urbanization at levels 1 and 4 and demonstrated negative conditional effects. Level 1 and level 4 urbanized countries had a similar pattern of relationship in CE and CVM, but possibly with entirely different reasons. It is a simple comparison of have and have not. The developed countries were in a fight with lifestyle-related problems and underdeveloped countries were busy in the panorama of communicable and infectious diseases that shared a major number of deaths rather than NCDs.40 Level 4 countries had the highest average life as compared to level 1 which had the lowest. People with advanced ages are more prone to have CVM risk factors,28 therefore, level 4 countries (where the average age is 78 years) have shown high CE but the efficient health system is reducing the chances of CVM in these countries. Further, these countries have improved social conditions and effective mechanisms for creating awareness about reducing the impact of these risk factors as discussed in the literature.3 Besides, level 1 countries reported the lowest average age (63 years) and more likely to have a low CE. However, the negative relationship between CE and CVM in these countries was possibly due to a large number of deaths caused by poverty-related diseases.3,40 It means a significant share of communicable diseases reduces the NCDs share in these countries. However, they are still sharing a greater number of CVDs related deaths due to large population sizes.14. Overall, the behaviour of countries towards CE and CVM is obvious in the presence of four levels of urbanization which was not highlighted by two traditional categories.
Although, the study has well demonstrated the moderating role of urbanization for CE and CVM. However, one of the limitations is that it could not include other modifiable risk factors which are physical inactivity, psychological stress and dietary habits owing to non-availability of data in secondary sources. The current study reported statistically adjusted findings with respect to the average age and income of the countries to minimize the possible confounding effect. Nonetheless, the findings of the study can be partially different after addition of average years of education in the countries which could not be covered in the current study due to limitations of secondary data.
Conclusion
This study set out to investigate and test the hypothesis of the moderating role of urbanization on the relationship between CE of modifiable risk factors and the CVM. This study concludes that urbanization has a strong influence as a moderator. We also revealed that stratification of urbanization in two categories is not able to gauge the moderating role of urbanization which veritably identified by the original quantitative form of urbanization. However, the newly suggested four levels of urbanization objectively unfold the diversified moderating role of urbanization in the relationship between CE and CVM. This study has raised a question about the validity of the stratification of urbanization in two traditional categories as discussed in the literature. The present study based on aggregated data tries to answer this question and provide the first comprehensive assessment of urbanization role in four levels which found to be plausible as compared to two categories. We propose that future researchers may test the efficacy of the latent construct of CE and four levels of urbanization in primary data.
Acknowledgements
The authors acknowledge the support of Ministry of Higher Education of Malaysia and Universiti Malaysia Pahang, Malaysia.
Funding Statement
Funding: This Research was funded by a grant from Ministry of Higher Education of Malaysia (FRGS Grant RDU 1901190) (FRGS/1/2019/STG06/UMP/02/11).
References
- 1.Benjamin EJ, Virani SS, Callaway CW, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation 2018;137:e67-e492.29386200 [Google Scholar]
- 2.Patel SA, Winkel M, Ali MK, et al. Cardiovascular mortality associated with 5 leading risk factors: national and state preventable fractions estimated from survey data. Ann Intern Med 2015;163:245-53. [DOI] [PubMed] [Google Scholar]
- 3.Sani MU, Wahab KW, Yusuf BO, et al. Modifiable cardiovascular risk factors among apparently healthy adult Nigerian population-a cross sectional study. BMC Res Notes 2010;3:11. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Sliwa K, Acquah L, Gersh BJ, Mocumbi AO. Impact of socioeconomic status, ethnicity, and urbanization on risk factor profiles of cardiovascular disease in Africa. Circulation 2016;133:1199-208. [DOI] [PubMed] [Google Scholar]
- 5.Roth GA, Forouzanfar MH, Moran AE, et al. Demographic and epidemiologic drivers of global cardiovascular mortality. N Engl J Med 2015;372:1333-41. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 6.Vlahov D, Galea S, Gibble E, Freudenberg N. Perspectives on urban conditions and population health. Cad Saude Publica 2005;21:949-57. [DOI] [PubMed] [Google Scholar]
- 7.Allender S, Wickramasinghe K, Goldacre M, et al. Quantifying urbanization as a risk factor for noncommunicable disease. J Urban Health 2011;88:906. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Ramachandran A, Mary S, Yamuna A, et al. High prevalence of diabetes and cardiovascular risk factors associated with urbanization in India. Diabetes Care 2008;31:893-8. [DOI] [PubMed] [Google Scholar]
- 9.Cyril S, Oldroyd JC, Renzaho A. Urbanisation, urbanicity, and health: a systematic review of the reliability and validity of urbanicity scales. BMC Public Health 2013;13:513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.City BL, Assessment E. Urbanization and health. Bull World Health Organ 2010;88:245-46. [Google Scholar]
- 11.Kearney J. Food consumption trends and drivers. Philos Trans R Soc Lond B Biol Sci 2010;365:2793-807. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Phelan JC, Link BG, Tehranifar P. Social conditions as fundamental causes of health inequalities: theory, evidence, and policy implications. J Health Soc Behav 2010;51:S28-S40. [DOI] [PubMed] [Google Scholar]
- 13.Gong P, Liang S, Carlton EJ, et al. Urbanisation and health in China. Lancet 2012;379:843-52. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.WHO. Noncommunicable diseases country profiles 2018. Available from: https://www.who.int/nmh/publications/ncdprofiles-2018/en/ [Google Scholar]
- 15.Tacoli C, McGranahan G, Satterthwaite D. Urbanisation, ruralurban migration and urban poverty. IIED: London; 2015. p. 36. [Google Scholar]
- 16.Chan F, Adamo S, Coxson P, et al. Projected impact of urbanization on cardiovascular disease in China. Int J Public Health 2012;57:849-54. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17.Mathenge W, Foster A, Kuper H. Urbanization, ethnicity and cardiovascular risk in a population in transition in Nakuru, Kenya: a population-based survey. BMC Public Health 2010;10:569. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 18.Hugo G. New forms of urbanization: beyond the urban-rural dichotomy. London: Routledge; 2017. [Google Scholar]
- 19.Riha J, Karabarinde A, Ssenyomo G, et al. Urbanicity and lifestyle risk factors for cardiometabolic diseases in rural Uganda: a cross-sectional study. PLoS Med 2014;11: e1001683. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Prescott E. Prognostic factors and risk scores in heart failure. Dorobanţu M., Ruschitzka F., Metra M., editors. Current approach to heart failure. Cham: Springer; 2016. p. 575-602. [Google Scholar]
- 21.DeFilippis AP, Young R, Carrubba CJ, et al. An analysis of calibration and discrimination among multiple cardiovascular risk scores in a modern multiethnic cohort. Ann Intern Med 2015;162:266-75. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.WHO. Noncommunicable diseases country profiles 2014. Available from: https://www.who.int/nmh/publications/ncdprofiles-2014/en [Google Scholar]
- 23.Hair JF, Black WC, Babin B, et al. Multivariate data analysis: A global perspective. London: Pearson Education; 2010. [Google Scholar]
- 24.UN. World urbanization prospects: The 2011 revision. Available from: https://www.un.org/en/development/desa/publications/world-urbanization-prospects-the-2011-revision.html [Google Scholar]
- 25.Satterthwaite D, McGranahan G, Tacoli C. Urbanization and its implications for food and farming. P Philos Trans R Soc Lond B Biol Sci 2010;365:2809-20. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.UN. World population prospects: the 2017 revision. Available from: https://www.un.org/development/desa/publications/world-population-prospects-the-2017-revision.html [Google Scholar]
- 27.The World Bank [Internet]. World Development Indicators. Available from: http://datatopics.worldbank.org/world-development-indicators/ [Google Scholar]
- 28.Barquera S, Pedroza-Tobias A, Medina C, et al. Global overview of the epidemiology of atherosclerotic cardiovascular disease. Arch Med Res 2015;46:328-38. [DOI] [PubMed] [Google Scholar]
- 29.Chen M, Zhang H, Liu W, Zhang W. The global pattern of urbanization and economic growth: evidence from the last three decades. PloS One 2014;9:e103799. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 30.Turok I, McGranahan G. Urbanization and economic growth: the arguments and evidence for Africa and Asia. Environ Urban 2013;25:465-82. [Google Scholar]
- 31.Preacher KJ, Hayes AF. Contemporary approaches to assessing mediation in communication research. Hayes A.F., Slater M.D., Snyder L.B., editors. The Sage sourcebook of advanced data analysis methods for communication research. Thousand Oaks: Sage Publications; 2008. p. 13-54. [Google Scholar]
- 32.Lewington S, Lacey B, Clarke R, et al. The burden of hypertension and associated risk for cardiovascular mortality in China. JAMA Intern Med 2016;176:524-32. [DOI] [PubMed] [Google Scholar]
- 33.Sahakyan KR, Somers VK, Rodriguez-Escudero JP, et al. Normal-weight central obesity: implications for total and cardiovascular mortality. Ann Intern Med 2015;163:827-35. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 34.Lavie CJ, De Schutter A, Parto P, et al. Obesity and prevalence of cardiovascular diseases and prognosis—the obesity paradox updated. Prog Cardiovasc Dis 2016;58:537-47. [DOI] [PubMed] [Google Scholar]
- 35.Sajid MR, Muhammad N, Zakaria R, et al. Associated Factors of cardiovascular diseases in Pakistan: Assessment of Path analyses using warp partial least squares estimation. Pak J Stat Operat Resa 2020:265-77. [Google Scholar]
- 36.Smyth A, Teo KK, Rangarajan S, et al. Alcohol consumption and cardiovascular disease, cancer, injury, admission to hospital, and mortality: a prospective cohort study. Lancet 2015;386:1945-54. [DOI] [PubMed] [Google Scholar]
- 37.Malik VS, Willett WC, Hu FB. Global obesity: trends, risk factors and policy implications. Nat Rev Endocrinol 2013;9:13. [DOI] [PubMed] [Google Scholar]
- 38.Bullettin of the World Health Organization. Urbanization and health. B World Health Organ 2010;88:245-6. [Google Scholar]
- 39.Khatib R, McKee M, Shannon H, et al. Availability and affordability of cardiovascular disease medicines and their effect on use in high-income, middle-income, and low-income countries: an analysis of the PURE study data. Lancet 2016;387:61-9. [DOI] [PubMed] [Google Scholar]
- 40.Singh AR, Singh SA. Diseases of poverty and lifestyle, wellbeing and human development. Mens Sana Monogr 2008;6:187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 41.WHO. Global action plan for the prevention and control of noncommunicable diseases 2013-2020. Available from: https://www.who.int/nmh/publications/ncd-action-plan/en [Google Scholar]