

The content is available as a PDF (426.2 KB).

Recommendations for post-colonoscopy follow-up in average risk adults
Recommendations for second surveillance stratified by adenoma findings at baseline and first surveillance.

*Normal colonoacopy is defined as colonoscopy where no adenoma, SSR, or CRC is found.
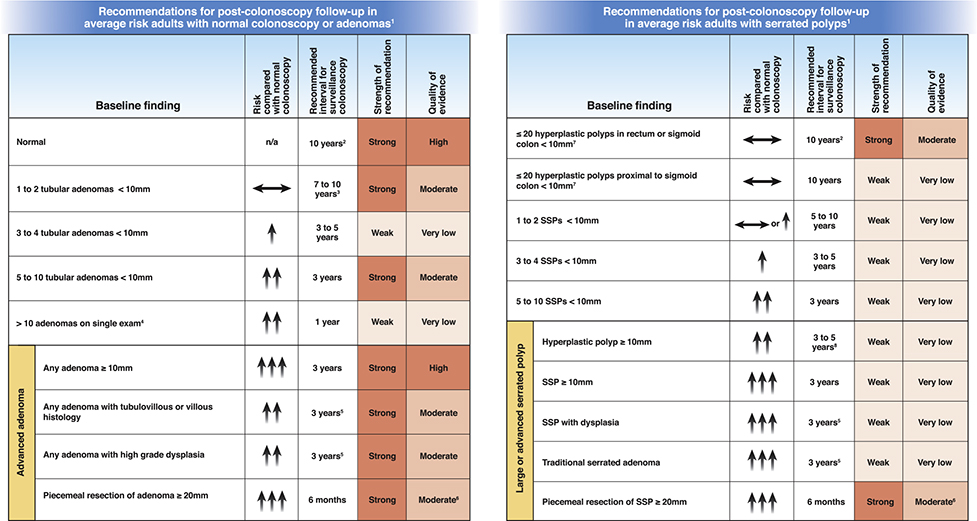 |
All recommendations assume exam complete to cecum with bowel preparation adequate to detect lesions > 5mm in size; recommendations do not apply to individuals with a hereditary CRC syndrome, personal history of inflammatory bowel disease, personal history of hereditary cancer syndrome, serrated polyposis syndrome, malignant polyp, personal history of CRC, or family history of CRC, and must be judiciously applied to such individuals, favoring the shortest indicated interval based on either history or polyp findings.
Follow up may be with colonoscopy or other screening modality for average risk individuals.
Patients with recommendations issued prior to 2020 for shorter than 7 to 10 year follow up after diagnosis of 1 to 2 tubular adenomas may follow original recommendations. If feasible, physicians may re-evaluate patients previously recommended an interval shorter than 10 years and reasonably choose to provide an updated recommendation for 7 to 10 year follow up, taking into account factors such as quality of baseline exam, prior polyp history, and patient preferences.
Patients with > 10 adenomas or lifetime > 10 cumulative adenomas may need to be considered for genetic testing based on absolute/cumulative adenoma number, patient age, and other factors such as family history of CRC (see text).
Assumes high confidence of complete resection.
See USMSTF recommendations for endoscopic removal of colorectal lesions (Kaltenbach TA et al., Endoscopic Removal of Colorectal Lesions–Recommendations by the US Multi-Society Task Force on Colorectal Cancer. At press 2020).
If cumulative more than 20 serrated polyps distributed throughout the colon, with at least 5 being proximal to the rectum, or 5 or more serrated polyps proximal to the rectum, all being 5mm or more in size, with 2 or more being 10mm or larger in size, consider a diagnosis of Serrated Polyposis Syndrome and alternate management (World Health Organisation. Classification of Tumours of the Digestive Tract. IARC Press, Lyon; 2019)
A 3-year follow up interval is favored if concern about consistency in distinction between SSP and HP locally, bowel preparation, or complete excision, whereas a 5-year interval is favored if low concerns for consistency in distinction between SSP and HP locally, adequate bowel preparation, and confident complete excision.
HP, hyperplastic polyp; SSP, sessile serrated adenoma/polyp/lesion