

Abstract
Vaccination against human papillomavirus (HPV) has been introduced as a public health initiative in many countries, including Denmark since October 2008. It is important to monitor postimplementation effectiveness of HPV‐vaccination at the population‐level. We studied HPV‐prevalence after first invitation to screening at age 23 years in women offered the quadrivalent HPV‐vaccine at the age of 14 years. Randomly selected screening samples from women born in 1994 in four out of five Danish regions were subjected to analysis for HPV in addition to routine cytology. Cobas4800 was used in all participating pathology departments. Data from a Danish prevaccination cross‐sectional study using Hybrid Capture 2, and a Danish split‐sample study using Cobas4800 were used for comparison. In the period from February 2017 to April 2019, 6233 screening samples from women born in 1994 were selected for HPV‐analysis; 27 samples had no HPV‐test and 3 samples had no HPV‐diagnosis, leaving 6203 samples with an HPV‐diagnosis. Prevalence of any high‐risk (HR) HPV was 35%; only 0.9% were positive for vaccine HPV types 16/18 while the remaining 34% were positive for other HR HPV. When comparing with prevaccination prevalence data, HPV‐16/18 decreased by 95%; RR = 0.05 (95% CI 0.04‐0.06), while other HR HPV remained fairly constant; RR = 0.88 (95% CI 0.82‐0.94) and RR = 0.95 (95% CI 0.88‐1.03), respectively. One‐third of women vaccinated as girls with the quadrivalent HPV‐vaccine were HR HPV‐positive at time of first invitation to screening. Vaccine HPV‐types 16 and 18 were almost eliminated, while the prevalence of nonvaccine HR HPV‐types remained constant.
Keywords: cervical screening, HPV‐vaccination, human papillomavirus, prevalence
Short abstract
What's new?
Vaccination against human papillomavirus (HPV) has been introduced as a public health initiative in many countries. However, data on HPV infection prevalence at screening age in HPV‐vaccinated birth cohorts remain scarce. This study found that HPV‐16 and 18 were almost eliminated in a population aged 23‐24 years where 92% of women received quadrivalent HPV vaccination at age 14. Prevalence of HPV 16 and 18 was lower in non‐vaccinated women than in previous birth cohorts not offered HPV‐vaccination. Nonetheless, one third of vaccinated women were positive for high‐risk HPV other than 16/18, with potential implications for cervical cancer prevention and screening programs.
Abbreviations
- CI
confidence interval
- DNA
deoxyribonucleic acid
- HC2
hybrid capture 2
- HPV
human papillomavirus
- HR
high risk
- LBC
liquid‐based cytology
- LiPa
line probe array
- NR
not reported
- RR
relative risk
- U.K.
United Kingdom
1. INTRODUCTION
Persistent infection with human papillomavirus (HPV) is a necessary step in cervical cancer pathogenesis. 1 All three HPV‐vaccines protect against the high‐risk (HR) types 16 and 18, accounting for 70% of cervical cancers. 2 The nine‐valent HPV‐vaccine protects against an additional five HR HPV‐types (31, 33, 45, 52 and 58), and is expected to prevent 90% of cervical cancers. 3
HPV‐vaccination is widely disseminated in high‐income countries and vaccinated women have been shown systematically to have a lower prevalence of HPV‐16 and HPV‐18 than nonvaccinated women; indicating effectiveness of the vaccine in real‐life. 4 Many countries have furthermore changed from cytology to HPV‐testing in primary cervical screening. Data on prevalence of HPV‐infection at screening age in birth cohorts HPV‐vaccinated as girls are, however, still scarce. Insight into HPV‐prevalence after vaccination is crucial from a public health point of view as quality assurance of the HPV immunization programs, and for determining the future combination of HPV‐vaccination and screening in control of cervical cancer.
Here we report on the prevalence of HPV‐infection at screening in a birth cohort offered the quadrivalent HPV‐vaccination at the age of 14 years, and personally invited to screening with cytology at the age of 23 years in the Danish national screening program. For comparison, we used data on HPV‐prevalence in young Danish women collected prior to the implementation of HPV‐vaccination. 5 , 6
2. MATERIALS AND METHODS
2.1. Cervical cancer prevention in Denmark
In October 2008, 13‐ to 15‐year‐old girls born in 1993 to 1995 were offered free HPV‐vaccination, and since January 2009 HPV‐vaccination has been offered to 12‐year‐old girls. 7 The quadrivalent HPV‐vaccine was used until 2015, and the bivalent HPV‐vaccine until 2017, when it was replaced by the nine‐valent HPV‐vaccine. 8 , 9
Cervical screening in Denmark targets women aged 23 to 64 years. At the age of 23 years, all women are personally invited to have a sample taken by their general practitioner, unless they are registered already with a cytology sample, which is the case for a minority only. At age 23 to 49 screening is offered every third year, and at age 50 to 64 every fifth year. 7 , 10 All laboratories in Denmark use liquid‐based cytology (LBC). In 2020, primary HPV‐DNA testing will be piloted for half of women aged 30 to 59 years, while LBC screening will be retained for the other half and for all women aged 23 to 29 years. Women aged 60 to 64 are offered an HPV‐DNA exit test. 11
2.2. Study population
Residual material from cervical screening samples was analyzed for HPV as part of a method study on the possible use of primary HPV‐testing in young, HPV‐vaccinated women. 12 The study population included a random sample of women born in 1994; offered quadrivalent HPV‐vaccination at the age of 14 years in 2008, and invited for cervical cytology screening, when they turned 23 years in 2017. According to national vaccine surveillance, 83% of women born in 1994 had at least one HPV‐vaccine dose. 13
2.3. Procedures
Pathology departments responsible for cervical screening in three and a half out of five Danish regions, covering half of Denmark, were involved in the study (Aalborg, Randers, Esbjerg, Soenderborg and Naestved) which started in February 2017. The selection of samples for HPV‐analysis was based on randomization of women born in 1994 present in Denmark in January 2017, so that samples from half of the women would be subjected to HPV‐analysis in addition to the routine cytology examination. At the scanning of the bar code of a newly received sample at the pathology department, a “pop‐up” message told that (a) the sample should be included in the study, and (b) whether an HPV‐test should be performed or not. Cobas 4800 HPV‐DNA test (Roche Diagnostics, Indianapolis, Indiana), already in clinical use in the participating laboratories, was used according to the manufacture's guidelines. Samples were clinician collected in SurePath liquid‐based medium (BD, Franklin Lakes, New Jersey) with the detachable head of the device placed in a vial containing preservative fluid. SurePath collected samples were handled in accordance with the manufacturer's protocols. Residual LBC material was utilized for HPV‐DNA testing. Then, 500 μL of diluted material were transferred to test tubes for analysis. Our study was embedded in the routine work at the labs, and Cobas4800 was used in the labs in advance for triage of ASCUS in women aged 30 and above. Before HPV‐testing, most labs performed pretreatment in accordance with the manufacturer's protocol. Cobas 4800 is based on real‐time PCR and can detect 14 HR HPV‐types (16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68) with four channels; HPV‐16, HPV‐18, a joined channel for the remaining 12 HR HPV‐types henceforth called “other HPV‐types”, and a β‐globin channel as control. 14
2.4. Prevaccine data used for comparison
In 2002 to 2005, a Danish cross‐sectional study examined HPV‐prevalence in a screened population of 40 382 women aged 14 to 95 years before implementation of HPV‐vaccination. 5 The study took place in the Capital Region of Denmark. In the age group 20 to 23 years, 2045 screening samples were analyzed for HPV using Hybrid Capture 2 (HC2) and Line Probe Array for genotyping of HC2‐positive samples 5 (Louise Thomsen and Susanne Krüger Kjær, personal communication, March 5, 2020). In 2011, a Danish split‐sample study, Horizon, was conducted in the Capital Region of Denmark. 6 In the study, 5072 cervical screening samples were tested for HPV using different assays. The study included 1522 cervical samples from women aged 23‐29 years tested with Cobas4800 6 (Jesper Bonde, personal communication, February 21, 2020). We used data from these two studies for comparison with our findings. Daily smoking in girls had decreased over time, but otherwise, the three study bases were fairly equal in demographics and behavior (Table S1).
2.5. Statistical analysis
Only the first screening sample for a given woman was included in the analysis. We assessed prevalence of any HR HPV, and of the following subgroups: (a) any 14 HR HPV; (b) all HPV‐16/18 including samples also with other types; (c) all HPV‐16 including samples also with other types, but excluding HPV‐18; (d) all HPV‐18 including samples also with other types, but excluding HPV‐16; (e) all 12 HR HPV Other including also samples with HPV‐16 or HPV‐18; and (f) HPV‐negative. Henceforth HR HPV is referred to as HPV. We did not have a specific code for unsatisfactory HPV‐test, but estimated that this was an issue for less than 20 samples. Prevalence proportions and relative risks (RR), together with corresponding 95% confidence intervals (CI), have been calculated using the binomial exact method and Wald method, respectively. Calculations and plots have been made using SAS statistical software version 9.4 and R version 3.6.2, with ggplot2 package.
3. RESULTS
Out of 18 924 women born in 1994 and living in the study area, 15 12 277 women; 65%, participated in the screening and were assigned a project code between February 1, 2017, and April 2019 (Figure 1). Of these, 6220 women were allocated to have an HPV‐test in addition to the routine cytology, 6065 women were allocated to cytology alone, while allocation missed for seven women. An additional 13 women had a project HPV‐test without a project code; they were included in the HPV‐group increasing the number to 6233 women; of whom 27 women did not have a HPV‐test recorded, and three women did not have a proper HPV‐diagnosis, leaving 6203 women to be included in the study (Figure 1).
FIGURE 1.
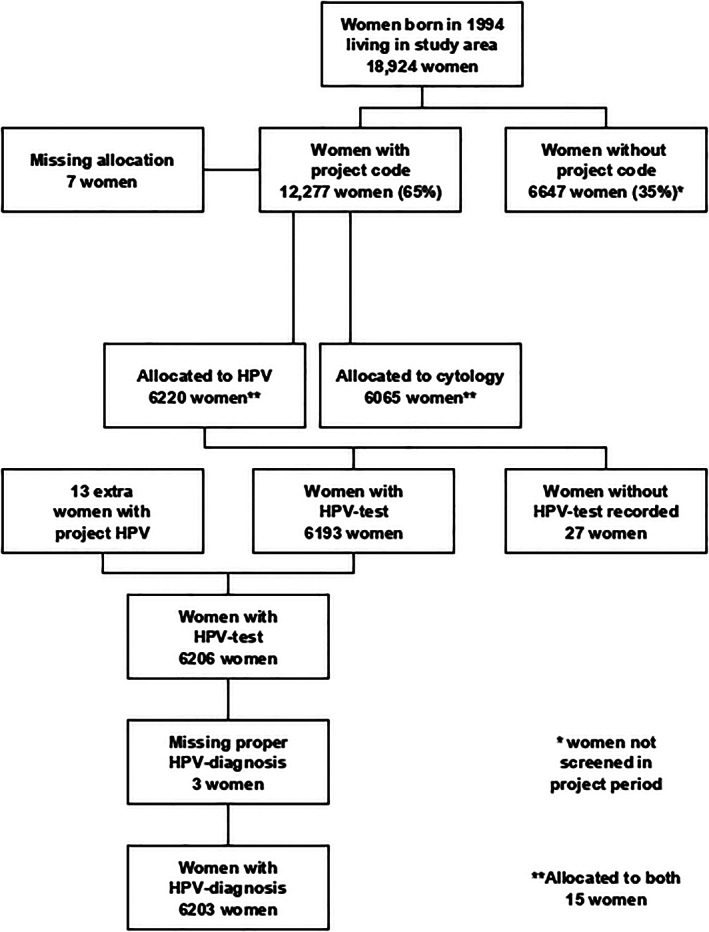
Study population, allocation to HPV‐testing and the presence of test results
Of the 6203 samples with an HPV‐diagnosis, 35% (95% CI 33.7‐36.1) were HPV‐positive (Table 1). Only 0.9% (95% CI 0.7‐1.1) of women were infected with the vaccine types HPV‐16 or 18 with the majority positive for HPV‐16 but not for HPV‐18, 0.7% (95% CI 0.7‐1.1), and 0.2% (95% CI 0.5‐1.0) positive for HPV‐18 but not for HPV‐16. No woman was positive for both HPV‐16 and HPV‐18. In total, 34.4% (95% CI 33.2‐35.6) of women were positive on the channel in the Cobas4800 assay measuring infection with at least one of the other 12 HPV‐types (31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66 and 68).
TABLE 1.
Prevalence of HR HPV in 6203 cervical screening samples from women born in 1994, from 2045 women aged 20 to 23 and screened in 2002 to 2005 5 , and from 1522 women aged 23 to 29 and screened in 2011 6
| Study | Present study | Kjær et al, 2014 5 | Preisler et al, 2013 6 | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Data collected | 2017‐2019 | 2002‐2005 | 2011 | ||||||
| Women aged, years | 23‐24 | 20‐23 | 23‐29 | ||||||
| Women born | 1994 | App. 1978‐1985 | App. 1981‐1989 | ||||||
| HPV‐vaccination | 1994: Offered at age 14 |
1978‐1984: not offered 1985: offered at age 26/27 |
1981‐1984: not offered 1985‐1989: offered at age 23/24‐26/27 |
||||||
| Sample media | Sure Path | Sure Path | Sure Path | ||||||
| HPV‐assay | Cobas4800 | HC2, positive genotyped with LiPA | Cobas4800 | ||||||
| HPV‐diagnosis | Number a | Prevalence a | 95% CI | Number a | Prevalence a | 95% CI | Number a | Prevalence a | 95% CI |
| Number studied | 6203 | — | — | 2045 | — | — | 1522 | — | — |
| Any 14 HR HPV‐positive | 2164 | 34.9% | 33.7‐36.1 | [940] | 46.0% | 43.8‐48.2 | 654 | 43.0% | 40.5‐45.5 |
| All HPV‐16/18 (including samples with other HR‐types) | 54 | 0.9% | 0.7‐1.1 | [380] | [18.6%] | [16.9‐20.3] | 253 | 16.6% | 14.8‐18.6 |
| All HPV‐16 (including samples with HR‐types other than 18) | 45 | 0.7% | 0.5‐1.0 | [241] | 11.8% | 10.4‐13.3 | 185 | 12.2% | 10.6‐13.9 |
| All HPV‐18 (including samples with HR‐types other than 16) | 9 | 0.2% | 0.1‐0.3 | [100] | 4.9% | 4.0‐5.9 | 55 | 3.6% | 2.7‐4.7 |
| All 12 HPV‐Other (including samples with HPV‐16/18) | 2132 | 34.4% | 33.2‐35.6 | 801 | 39.2% | 37.0‐41.3 | 549 | 36.1% | 33.7‐38.5 |
| HPV‐Negative | 4039 | 65.1% | 63.9‐66.3 | [1105] | [54.0%] | [51.6‐56.2] | 868 | 57.0% | 54.5‐59.5 |
Abbreviations: CI, confidence interval; NR, not reported; RR, relative risk; [ ] Calculated by authors.
Categories are partly overlapping.
In the first comparison study 5 with samples collected from 2002 to 2005, 46% (95% CI 43.8‐48.2) of women aged 20 to 23 years were HPV‐positive, with 18.6% being positive for the vaccine types HPV‐16 or HPV‐18 alone or in combination with other HPV‐types. Positivity for HPV16 but not for 18 was found in 11.8% (95% CI 10.4‐13.3) of women, and positivity for HPV18 but not for 16 was found in 4.9% (95% CI 4.0‐5.9) of women. The proportion of women positive for other HPV‐types, including those positive for HPV‐16/18, was 39.2% (95% CI 37.0‐41.3).
In the second comparison study with samples collected in 2011, 43% (95% CI 40.5‐45.5) of women aged 23 to 29 years were HPV‐positive; with 16.6% (95% CI 14.8‐18.6) being positive for at least one of the vaccine types HPV‐16 and HPV‐18. In total, 36.1% (95% CI 33.7‐38.5) of the women were infected with at least one of the other HPV‐types.
Comparing our findings with the 2002 to 2005 data, the prevalence of HPV decreased from 46% to 34.9%, RR = 0.76 (95% CI 0.72‐0.80) from before to after HPV‐vaccination. The prevalence of vaccine types HPV‐16 and HPV‐18 decreased dramatically by 95%, from 18.6% to 0.9%, RR = 0.05 (95% CI 0.04‐0.06). Comparing our findings with the 2011 data, the prevalence of HPV decreased from 43% to 34.9%, RR = 0.81 (95% CI 0.76‐0.87). Also here, the prevalence of the vaccine types HPV‐16 and HPV‐18 decreased by 95%, from 16.6% to 0.9%, RR = 0.05 (95% CI 0.04‐0.07). In contrast, the prevalence of the other HPV‐types remained fairly constant changing from 39.2% to 34.4% in comparison with the 2020 to 2005 data, RR 0.88 (95% CI 0.82‐0.94), and from 36.1% and 34.4% in comparison with the 2011 data, RR = 0.95 (95% CI 0.88‐1.03, Figure 2).
FIGURE 2.

Comparison of HPV‐prevalence data in the era before and after HPV‐vaccination
Vaccination coverage was 92% for at least one dose of the quadrivalent HPV‐vaccine in the cohort of 6203 women in the present study, of whom 97% were vaccinated at age 15 years at the latest. While the prevalence of the vaccine HPV types 16 and 18 was 0.4% in vaccinated women it was 6.6% in nonvaccinated women, RR = 0.05 (95% CI 0.03‐0.09; Table 2). The prevalence of other HPV‐types was slightly higher in vaccinated than in nonvaccinated women; 34.8% vs 30.1%, RR = 1.15 (95% CI 1.01‐1.32).
TABLE 2.
Prevalence of HPV in 6203 cervical screening samples from women born in 1994 stratified by HPV‐vaccination status
| Vaccinated (%) | Nonvaccinated (%) | RR (95% CI) | |
|---|---|---|---|
| Number of women | 5685 | 518 | NR |
| HPV‐positive | 1987 (34.9%) | 177 (34.2%) | 1.02 (0.90‐1.16) |
| HPV‐16/18 (including samples with other HPV‐types) | 20 (0.4%) | 34 (6.6%) | 0.05 (0.03‐0.09) |
| HPV‐other (including samples with HPV‐16/18) | 1976 (34.8%) | 156 (30.1%) | 1.15 (1.01‐1.32) |
| HPV‐negative | 3698 (65.1) | 341 (65.8) | 0.99 (0.93‐1.05) |
Abbreviations: CI, confidence interval; NR not relevant; RR, relative risk.
4. DISCUSSION
4.1. Main findings
The prevalence of high‐risk HPV‐infection around the age of 23 years, when women in Denmark are first invited to screening, was 35% in the 1994 birth cohort where almost all had been HPV‐vaccinated as girls. In comparison, 43% to 46% were HPV‐positive in birth cohorts where no one had been HPV‐vaccinated as girls. Infection with the vaccine HPV types 16 and 18 was almost eliminated in the vaccinated cohort, while it constituted an infection burden of 17% to 19% in the nonvaccinated cohorts.
In the 1994 birth cohort, a small number, less than half a percent, of the actually vaccinated women were positive for HPV‐16 or HPV‐18. It should be stressed that these cases cannot be considered as vaccine breakthrough infections, as not all the girls were HPV‐naïve at the time of vaccination. The HPV‐16 and HPV‐18 prevalence in actually nonvaccinated women born in 1994 was less than half of that found in the comparison groups not offered childhood HPV‐vaccination. This could indicate a herd immunity effect; which could be enhanced also by the fact that all birth cohorts born from 1993 onwards have been offered childhood HPV‐vaccination.
Our data indicated that vaccination with the quadrivalent HPV‐vaccine affected the risk of infection with high‐risk HPV‐types other than 16 and 18 only slightly. The proportion of women testing positive on other high‐risk HPV‐types was almost the same in the 1994 birth cohort as in the older birth cohorts not HPV‐vaccinated as girls.
4.2. Findings in perspective of other studies
In a recently published meta‐analysis on real‐life impact of HPV‐vaccination, 4 the prevalence of HPV‐16 and HPV‐18 was found to have decreased by 83% 5 to 8 years after vaccination among girls aged 13 to 19 years, and by 66% among women aged 20 to 24 years. The endpoints in the meta‐analysis were estimated from different types of studies. In our cohort study, where we had a longer follow‐up of 8 to 10 years after HPV‐vaccination, which took place at the age of 14 to 15 years, we found an even larger decrease of 95% in the prevalence of HPV‐16 and HPV‐18. The meta‐analysis indicated an increase in the prevalence of the nonvaccine HPV‐types. For this finding, three possible explanations were suggested: (a) a change in the background risk of HPV‐infection due to changes in sexual behavior; (b) unmasking, because HPV‐16 and HPV‐18 could previously have masked detection of these other HPV‐types; and (c) type replacement where other HPV types will fill the niche left after HPV‐16 and HPV‐18.
In contrast to changes reported from for instance the UK, 16 sexual habits have been fairly stable in Denmark, where the average age at first intercourse has remained at the age of 16 years, 17 , 18 and the median number of sexual partners for women aged 18 to 24 years was 4 in 2005 and 5 in 2012. 17 Changes in sexual behavior are therefore not likely to have biased the comparison of HPV‐data between for the generations of young women screened in 2002 to 2005, 2011 and 2017 to 2019, respectively.
We used Cobas4800 for HPV‐testing. In the studies we used for comparison, the samples were tested on HC2 5 and Cobas4800, 6 respectively, but due to cross‐reaction with HPV 66 in HC2, the two assays essentially detect the same 14 HPV‐types. In the Danish split‐sample study, 6 the HPV‐positivity rate for women aged 23 to 29 years was 33% with HC2 and 43% with Cobas4800. Changes from use of the first generation HC2‐assay to the second generation Cobas4800 assay could then have contributed to the increase in nonvaccine HPV‐types indicated in the meta‐analysis. 4 The fact that the HPV‐positivity rate was slightly higher in our comparison study using the HC2‐assay than in the one using the Cobas4800‐assay can probably be ascribed to the fact that the first study group was slightly younger than the second, 20 to 23 years and 23 to 29 years, respectively. For the comparison of positivity on other high‐risk HPV types than 16 and 18, it should be taken into account that while this group in our, and the 2011 data, was identified based on the other‐HPV‐signal in the Cobas4800, it was in the 2002 to 2005 data identified based on HC2‐positivity in combination with the Line Probe Array for genotyping.
The stability in the proportion of women positive for the nonvaccine high‐risk HPV‐types could indicate that neither cross‐protection nor unmasking, or type‐replacement took place. Due to the limitation in the Cobas4800 assay, we were, however, not able to reveal possible opposite changes behind the overall stability.
4.3. Strengths and limitations
This study was population‐based including randomly selected women living in well‐defined parts of Denmark, and with a cervical sample taken after first invitation to screening at Age 23 years. The screening coverage was 65%. All samples were tested with Cobas4800. The women had been offered HPV‐vaccination at age 14 years, and the vaccination coverage in the screened women was 92%. Between 8 and 10 years had passed between time of vaccination and time of screening. Due to partial genotyping, it was not possible to examine possible cross‐protection and/or possible unmasking and/or type replacement.
HPV‐vaccination coverage was quite high in the study, and practically all women were vaccinated at young age. While we can assume that the majority of vaccinated women were HPV‐naïve at the time of vaccination, this will not have been the case for all, as 24% of girls in this generation reported to have been sexually active at the age of 14 years. 19
4.4. Clinical implications
HPV‐16 and HPV‐18 have been found to be responsible for 70% of cervical cancers. The fact that we found HPV‐16 and HPV‐18 to be almost eliminated at age 23 to 24 years in women HPV‐vaccinated with the quadrivalent vaccine at age 14 to 15 years, therefore, pointed to a considerably improved protection against cervical cancer in women HPV‐vaccinated as girls. Nevertheless, still, 35% of the women were high‐risk HPV‐positive strongly indicating that primary HPV‐screening of women in this age group would have to be combined with triage to avoid referral to colposcopy of too many women with no underlying histological lesion. In 2017, Denmark changed to the nine‐valent HPV‐vaccine, which provides a better protection against cervical cancer than the quadrivalent vaccine, and the HPV‐positivity rate in young women is therefore expected to decrease when these younger birth cohorts will reach screening age.
5. CONCLUSION
The prevalence of the vaccine HPV‐types 16 and 18 was less than 1% when in young, Danish women offered quadrivalent HPV‐vaccination as girls attended cervical screening at the age of 23 to 24 years. This corresponded to a 95% decrease in comparison with the prevalence from the prevaccination era. Despite this impressive reduction, 35% of women were still HPV‐positive.
CLINICAL TRIALS REGISTRATION
ClinicalTrials NCT03049553.
CONFLICT OF INTEREST
Roche provided HPV‐DNA test‐kits for the method study but had no role in the data analysis, interpretation of results or writing of the paper. E. L.: Received HPV‐DNA test kits from Roche for the present study. B. A.: Received HPV kits from Roche and HPV self‐sampling kits from Axlab for other studies. L. T., L. G. L., J. C., T. J., J. H., S. C. and C. R.: No conflict of interest.
6.
ETHICS STATEMENT
The study was deemed a method study by the Ethical Committee of the Capital Region of Denmark (H‐16022292) and approved by the Danish Data Protection Agency under the University of Copenhagen (SUND‐2016‐22). Permission for data extraction was obtained from the Danish Patient Safety Authority (3‐3013‐2328/1). HPV‐DNA test‐kits for the study were provided free of charge by Roche.
Supporting information
Data S1 Supporting Information
ACKNOWLEDGEMENTS
A sincere thank to the bio‐technicians at the participating pathology departments. Thank you to George Napolitano for statistical support, thank you to Louise Thomsen and Susanne Krüger Kjær for providing data from the 2002 to 2005 study, and to Jesper Bonde for providing data from the 2011 study. The study was supported by the Independent Research Fund Denmark (grant no. 4183‐00315) and the Danish Health Foundation (grant no. 16‐8‐0227). The funders did not take part in the study.
Lynge E, Thamsborg L, Larsen LG, et al. Prevalence of high‐risk human papillomavirus after HPV‐vaccination in Denmark. Int. J. Cancer. 2020;147:3446–3452. 10.1002/ijc.33157
Funding information Danish Health Foundation, Grant/Award Number: 16‐8‐0227; Det Frie Forskningsråd, Grant/Award Number: 4183‐00315
DATA AVAILABILITY STATEMENT
Data from the study can be made available via the research service of Statistics Denmark and following the Danish Data Protection Regulation.
REFERENCES
- 1. Walboomers J, Jacobs M, Manos M, et al. Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol. 1999;189:12‐19. [DOI] [PubMed] [Google Scholar]
- 2. de Sanjose S, Quint WG, Alemany L, et al. Human papillomavirus genotype attribution in invasive cervical cancer: a retrospective cross‐sectional worldwide study. Lancet Oncol. 2010;11:1048‐1056. [DOI] [PubMed] [Google Scholar]
- 3. Joura EA, Giuliano AR, Iversen O‐E, et al. A 9‐valent HPV vaccine against infection and intraepithelial neoplasia in women. N Engl J Med. 2015;372:711‐723. [DOI] [PubMed] [Google Scholar]
- 4. Drolet M, Bénard É, Pérez N, et al. Population‐level impact and herd effects following the introduction of human papillomavirus vaccination programmes: updated systematic review and meta‐analysis. Lancet. 2019;394:497‐509. 10.1016/S0140-6736(19)30298-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5. Kjær SK, Munk C, Junge J, Iftner T. Carcinogenic HPV prevalence and age‐specific type distribution in 40,382 women with normal cervical cytology, ASCUS/LSIL, HSIL, or cervical cancer: what is the potential for prevention? Cancer Causes Control. 2014;25:179‐189. 10.1007/s10552-013-0320-z. [DOI] [PubMed] [Google Scholar]
- 6. Preisler S, Rebolj M, Untermann A, et al. Prevalence of human papillomavirus in 5,072 consecutive cervical SurePath samples evaluated with the Roche cobas HPV real‐time PCR assay. PLoS One. 2013;8:e59765 10.1371/journal.pone.0059765. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7. Lynge E, Rygaard C, Baillet MV‐P, et al. Cervical cancer screening at crossroads. APMIS. 2014;122:667‐673. 10.1111/apm.12279. [DOI] [PubMed] [Google Scholar]
- 8. Statens Serum Institut . Newsletter, Week 2. 2016. (In Danish). https://www.ssi.dk/Aktuelt/Nyhedsbreve/EPI‐NYT/2016/Uge%202%20‐%202016.aspx. Accessed 20 June 2019.
- 9. Statens Serum Institut . Newsletter, Week 42–43. 2017. (In Danish). https://www.ssi.dk/Aktuelt/Nyhedsbreve/EPI‐NYT/2017/Uge%2042‐43%20‐%202017.aspx. Accessed 20 June 2019.
- 10. Statens Serum Institut . Cervical cancer screening—national recommendations. 2012. (In Danish, summary in English). 2012.https://www.sst.dk/~/media/B1211EAFEDFB47C5822E883205F99B79.ashx. Accessed 20 August 2019.
- 11. Statens Serum Institut . Danish Health Authority. Cervical cancer screening guidelines. 2018. (In Danish, Summary in English). https://www.sst.dk/da/sygdom‐og‐behandling/screening/~/media/5466AB0B06184ED0969BC31DA397610D.ashx. Accessed 4 October 2019.
- 12. Thamsborg LH, Andersen B, Larsen LG, et al. Danish method study on cervical screening in women offered HPV vaccination as girls (Trial23): a study protocol. BMJ Open. 2018;8:e020294 10.1136/bmjopen-2017-020294. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 13. Statens Serum Institut . National vaccination coverage statistics. https://statistik.ssi.dk/. Accessed 17 September 2019.
- 14. Rao A, Young S, Erlich H, et al. Development and characterization of the cobas human papillomavirus test. J Clin Microbiol. 2013;51:1478‐1484. 10.1128/JCM.03386-12. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Population count (FOLK1A), statistikbanken.dk (In Danish). https://www.statistikbanken.dk/statbank5a/default.asp?w=1920. Accessed 6 January 2020.
- 16. Mercer CH, Tanton C, Prah P, et al. Changes in sexual attitudes and lifestyles in Britain through the life course and over time: findings from the National Surveys of sexual attitudes and lifestyles (Natsal). Lancet. 2013;382:1781‐1794. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 17. Hansen BE, Kjæe SK, Arnheim‐Dahlström L, et al. Age at first intercourse, number of partners and sexually transmitted infection prevalence among Danish, Norwegian and Swedish women: estimates and trends from nationally representative cross‐sectional surveys of more then 100,000 women. Acta Obstet Gynecol Scand. 2019;00:1‐11. [DOI] [PubMed] [Google Scholar]
- 18. Stryhn JG, Graugaard C. The age at first intercourse has been stable since the 1960s, and early coital debut is linked to sexual risk situations. Ugeskr Laeger. 2014;176(37):V01140063. [PubMed] [Google Scholar]
- 19. Rasmussen M, Due P. School survey 2010 (In Danish). 2011. https://www.hbsc.dk/downcount/HBSC-Rapport-2010.pdf. Accessed 26 June 2019.
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.
Supplementary Materials
Data S1 Supporting Information
Data Availability Statement
Data from the study can be made available via the research service of Statistics Denmark and following the Danish Data Protection Regulation.